This book is dedicated to all those who never found out what

This book is dedicated to all those who never found out what affected them.
THE AMALGAM WARS
A SOURCEBOOK ON AMALGAM POISONING
1844-1943
Mats Hanson
Many amalgam did I make,
Wenyng to fix these to grett avayle
And thereto sulphur dyd I take
Tartar, eggs whyts and the oyl of the snayle.
But ever of my purpose dyd I fayle,
For what for the more and what for the lesse,
Evermore something wanting there was.
George Ripley: The Compound of Alchymie 1475
Contents:
First Amalgam war
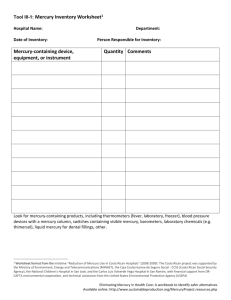
Report of the Onondaga County Medical Society on "Mineral Paste" Westcott A The
American Journal of Dental Science IV no3 1844 175-193
On the dangers of using Silver-Amalgams, called Succedaneum minerale, to fill teeth.
Talma, Dentist at the Belgian Royal Court in Brussels Der Zahnarzt 1(1) 1846
23-28
Letter. prof. Slack, Am J Dent Sci VIII 1847-8 172-8
Amalgam. Proceedings of Dental Societies The Dental Cosmos 1861 548-58
Amalgam. Editorial Dental Cosmos IV jan 1863 312-13
Poisoned by mercury from a tooth filling The Dental register XXVI 1872 47-8
Poisoning from corrosive sublimate generated in the mouth from amalgam plugs in the teeth Payne J The Dental Cosmos XVI 1874 213-4
Proceedings of the New York Odontological Society Dental Cosmos 17 1875 236
On teeth in health and disease and about their care Ulmgren O Samson & Wallin
Stockholm 1881
The chemistry and physiological action of mercury as used in amalgam fillings Talbot ES
Ohio State J Dent Sci II 1882 1-12; Editorial: The amalgam question again 51-54
The amalgam question Flagg JF Dental Cosmos 24 1882 237
Amalgam Fletcher T Amalgam Dental Items Interest 6 1884 171
The influence of amalgam fillings and red rubber plates upon the origin and growth of tumors Crutcher H Med Adv 35 1896 489
A few suggestions about mercurial fillings for teeth Wesselhaeft WP Proc Int
Hahnemannian Assoc 16 1896 200
Mercurial neurosis resulting from amalgam fillings Tuthill JY Brooklyn Med J 12 1898
725
Galvanism, gold, amalgam and the Hahnemanian theory Grant RC The Dental Digest 8
1902 1110-1122 (AD55)
Some things dentists know little about Morrison MA Dominion Dent J 14 1902 84-93
Second Amalgam War
The hazard of mercury vapor Stock A Zeitschr Angew Chem 39 1926 461
Faraday's laboratory. Louis Lewin
Discussion: On the question of the hazard of mercury vapor; Z Angew Chem 39 1926
786-790; Stock A; Schmidt A. Pinkus G; Reihlen H; Gradenwitz F; Sterner-Rainer;
Wolf L; Ruska J; Comments: A Stock
On the question of the hazards of amalgam fillings. A dental rebuttal. Haber G. Z Angew
Chem 39 1926 905
Amalgam fillings and mercury poisoning Kleinsorgen F Umschau der Wissensch 30
1926 476; Windmüller P 479
The hazards of mercury vapor and amalgam Stock A Z Angew Chem 39 1926 984
Die Amalgamfrage: Quousque tandem Fenchel Z angew Chem 41 1928 1182; Stock A
Comment to the contribution by Dr Fenchel p 1183; Fenchel: Rebuttal to prof. Stock's
Mercury poisonings from dental fillings Meyer E Med Welt 4 1930 703
On the question of the hazards of small amounts of mercury Fleischmann P. Verein für
Innere Medizin Z Angew Chem 41 1928 66; Dtsch Med Wschr 8 1928 304
The hazards of mercury and amalgam dental fillings Stock A Z Angew Chem 41 1928
663
Risks of poisoning during work with mercury Stelling O Sv. Kemisk Tidskr 41 1929 80
Presentation of the discussion, initiated by Stock, on the problem of the hazards of amalgam fillings according to literature Huber CD. Dissertation München 1957: from the Klin. f. Zahn-, Mund- und Kieferkrankheiten. (abstracts)
Mayer, E. (Prof. Breslau) Investigations of amalgam regarding release of metallic mercury. Dtsch. Monatschr f. Zahnheilk. 1927 p..226.
Rohrer, L. Does chronic mercury poisoning from amalgam dental fillings exist? Münch.
Med. Wochenschr 1927, p. 1346.
Werkenthin, A. Copper amalgam overbord, Zahnärztl. Rundschau 1929, p. 451.
Witzel, A. The question of mercury poisoning from dental fillings Münch. Med.
Wochenschr. 1926, 1021
Schoenbeck, F. (Prof. Biesenthal) The amalgam hazard. Zahnärztl. Rundschau 1926,
415; The hazards with amalgam fillings, Zahnärztl. Rundschau 1926, 449; Amalgam fillnings and mercury poisoning Dtsch. Monatschr. Zahnheilk. 1926, 435; The amalgam issue, Münchn. Med. Wschr. 1927, 1694; Investigation of mercury excretion in amalgam bearers and persons handling amalgam fillings Dtsch. Monatschr.
Zahnheilk. 1927, 208; The harmfulness of amalgam fillings Zahnärztl Mitteil 1928, 390;
On the amalgam question Dtsch Zahnärztl Wschr 1928, 151.
Feiler, R. A contribution to the amalgam issue, Zahnärztl. Rundschau 1927, 797-98.
Seifert, K. Regarding the controversy on mercury release from amalgam fillings.
Zahnärztl. Rundschau 1926, 516.
Joachimoglu, G, The hazards of mercury vapor. Med. Klin 1926, 1275.
Ritter, P. The hazard of mercury vapor, Med. klin. 1926, 1279; The hazard of amalgam fillings, Zahnarztl. Rundshau 1926, 415; The hazards of amalgam plombs Zahnärztl.
Rundshau 1926, 449; Objections against Stock in the amalgam issue, Zahnärztl.
Rundshau 1926, 553; On the amalgam issue, Zahnarztl. Rundshau 1929, 1471; The toxicity of copper amalgam, Med Welt 1930 no.51.
Maschke, A. Experimental-psychological studies on the effect of amalgam dental fillings on intellectual ability. Zahnärztl. Rundschau 1930, 990.
Borgzinner, U. The toxicity of amalgam fillings, Münch. Med. Wochenschr. 1927,
1346.
Müller, O. Description of a patient with cured mercury poisoning from amalgam plombs.
Münch. Med. Wochenschr. 1929, 651.
Wannenmacher, E. (Prof. Zahnärztl. inst. Univ. Tübingen) The amalgam issue, Münch.
Med. Wochenschr. 1927, 1694; A contribution to the amalgam issue Dtsch
Zahnärztl. Wochenschr. 1928, 152; The harmfulness of amalgam dental fillings
Zahnärztl. Mitteil. 1928, 390. comment p 1183; Stock A Final word p 1184
Fühner, H. Chonic mercury poisoning and danger from amalgam. Gesellsch. f. Natur- u. Heilkunde, 1927.
Rebel, H. Report from Zentralvereins deutscher Zahnärzte in Düsseldorf, Dtsch.
Zahnärztl. Wchschr. 1926, 485.
Krüger, R. Does chronic mercury poisoning from amalgam fillings exist? Münch. Med.
Wochenschr. 1927, 1346; Lewinski, E. A death sentence over copper amalgam?
Zahnärztl. Rundshau 1926, 517; The amalgam issue Dtsch Monatschr. Zahnheilk. 1926,
208.,
German Ministry of Health, jan. 1932
Amalgam fillings as a possible source of mercurial poisoning Bodecker CF Dent Items
Inter 48 1926 637
On chronic mercury poisoning caused by dental fillings Steffensen K Ugeskr f Laeger 96
1934 855
On "nervous" phenomena and amalgam plombs Schmidt-Phiseldeck K Tandlaegebladet
1936 598-603; Comments Schou H p604-6
The mercury content of the human excreta and the human blood Stock A & Cucuel F Z
Angew Chem 47 1934 641
On evaporation, solubility and oxidation of metallic mercury Stock A Z Anorg Allgem
Chem 217 1934 241
The effect of mercury vapor on the upper respiratory tract Stock A Naturwissensch 26/28
1934 453
Galvanic burns of the oral mucosa Hollander L JAMA 99 1932 383
Electrogalvanic phenomena of the oral cavity caused by dissimilar metallic restorations
Lain ES & Caughron GS JADA 23 1936 1641
Potential difference between various kinds of metals applied in oral cavity and their physiologic effects Wakai E JADA 23 1936 1000 (E3)
The mercury content of the human organism Stock A Biochem Z 304 1940 73
The mercury content of the human organism II. Stock A Biochem Z 316 1943 108
The calomel rebellion Leonard RB South Med J 80 1987 638
Calomel and the American medical sects during the nineteenth century Risse GB Mayo
Clin Proc 48 1973 57
Experiences on chronic mercury poisonings Burgener P & Burgener A Schw Med
Wochenschr 8 1952 204
Acrodynia or how to fail to recognize mercury poisoning for more than 100 years Hanson M. Tf-bladet, Bull of the Ass of Swedish Dental Mercury Patients no. 3, 1987, 4-5; Dental & Health Facts, Foundation for Toxic Free Dentistry 3:3, 1990, 1-4
Report of the Onondaga County Medical Society, on "Mineral Paste."
By A. Westcott, M.D. of Syracuse. N.Y.
The Americal Journal of Dental Science 4:3 1844, 175-193
Syracuse, Feb. 1, l844. To the New York Editor:-
My DEAR Sir:- Agreeably to your request, I embrace the earliest opportunity to forward you the report of the committee appointed by the Onondaga County Medical Society, to investigate the merits of "mineral paste" as an article for filling teeth. I transmit, also, some other facts and considerations, relating to this subject, which should you regard of sufficient interest, you may insert in the forthcoming number of the Journal. It may be deemed by those from whose territory this pernicious article has been already banished, by the perservering effort of a few individuals, too late in the day, to write exposes of this species of quackery. I would it were so in this region, but when I assure you that not more than a year since, at least one-half of all the teeth filled in this village,
(containing about eight thousand inhabitants) were filled with mineral paste, you may suppose that all the dental trowels are not yet gone into disuse. Nor has it been itinerant quacks alone, who have presumed to employ it and advocate its virtues.
About one year ago I caused to be published in one of our village papers, an article designed as an expose of this branch of empiricism, I will quote so much of that article, as is not already published in the Dental Journal, it is as follows:
DENTAL QUACKERY - Messrs. Editors - Dear Sirs:-Permit me through your columns to present to the public, the following expose.
Every practice either in medicine or surgery, if it be pernicious in its ultimate results, is the more dangerous to the community, as it is the more alluring, and of the many which are offered to the public, perhaps few so destitute of merit, present more apparent advantages, than that of filling teeth with "mineral paste," especially to those who are ignorant of its composition, and tendencies.
Indeed, who would not be induced to have their teeth filled when they are made to believe, that the operation may be performed "without pain" with little expense, and all this too with "royal mineral succedaneum," which, though a paste, when introduced, soon "becomes as hard as the tooth itself!"
Though this paste has at different times, received different appellations, changing with the fancy or policy of the operator, yet its composition has ever been the same. It uniformly contains as an essential, nay, as the chief ingredient, mercury or quicksilver, the other may be silver, tin or zinc.
From the mercury of this compound when oxydized or corroded, as it always is by the fluids of the mouth, there is formed a substance closely allied to calomel, indeed, judging from its effects, we might say it more nearly resembled corrosive sublimate which is but another compound of mercury.
The above facts will give an easy solution to the phenomena, described in the following letter from
Dr. J. Stearns, dated, Pompet, Dec. 15, 1842.
DEAR Sir: - Regarding as I do the profession of dentistry as a science, which ought to be ranked among the honorable professions, I therefore feel it my duty for the public good, and the honor of your laudable profession, to expose the vile quackery that is being practised on the community in this section, by an itinerant dentist, to the great injury of many individuals, and the success of the practice of dentistry. I wiIl here give a statement of a case or two, which have fallen under my observation. Miss R. S. called me to visit her. I found her with febrile symptoms; her tongue, gums and glands swollen; a free discharge of saliva; a fetid breath, &c. I asked her if she had ever been salivated- she said never, I was positive, however, that she was under the influence of mercury, and then found that two or three weeks before, she had several teeth filled with "royal mineral succedaneum." The teeth were very loose; the next day I removed one of the teeth, found it perfectly dead, and the alveolar process affected, which I have since removed, including almost the entire socket of the tooth. I have since been called to Mrs. W. who has been severely salivated by the use of the same compound.
Respectfully, yours, JEHIEL STEARNS
A. Westcott, M. D.
It is proper here to remark, that the effect as described by Dr. S. in the above letter, is not the same in all cases. I have seen several cases within the last year, nearly as strongly marked, yet perhaps with a majority of those who have had teeth filled with this article, the effect does not amount to salivation in the common acceptation of that term. This much, however, may be safely said, and is of universal application, that its tendency in this respect is always bad, and in no case where any considerable amount of it is used, does it fail to vitiate the secretions of the mouth to a greater or less extent. The influence it is capable of exerting, and time elapsing before it is rendered perceptible, will depend on the following circumstances:
1st. The susceptibility of the individual to the effects of mercury, it being well known that while some others are badly salivated by comparatively a trivial amount.
2d. The quantity of cement used.
3d. Age and health of the subject.
The remainder was made up of quotations from the different authors who had written on this topic in the Journal and the report of the committee of American Society, July, 1841. No sooner had this article made its appearance than it was construed by the oldest dental practitioner in this village, (Dr.
Bliss,) into a personal assault, and that too aimed exclusively at himself! He sought redress by applying to the County Medical Society, of which he claimed to be a member, and entreated its interference in his behalf, pledging himself moreover that he would convince them that the cement he used was not only efficient in arresting caries, but entirely harmless. The society very reluctantly recognised the subject of complaint as coming within its province, but at length, as the easiest method of disposing of it, appointed a committee of three, to whom the investigation was referred, and who were to report at the next meeting of the society. I was soon after summoned by this committee to appear before them, and answer the arguments, which Dr. B. had pledged himself to give in support of his grand dental catholicon.
At the meeting of the American Society of Dental Surgeons, convened at Baltimore, in July last, I brought this subject up for consideration, asking such action upon it as might be deemed proper.
This request was responded to by the following resolution, which was unanimously passed,
On motion of Dr: Harris, Resolved, That this society regards the use of mineral paste in plugging carious teeth as malpractice, and that a committee of three be appointed to receive information and facts on that subject to be transmitted to Dr. Westcott of Syracuse, in the state of New York, to be by him laid before the Medical Society of the county of Onondaga, in that state, before which the subject aforesaid is now pending.
This report was duly made, by the able gentleman to whom it was referred, and laid before the committee of the Onondaga Medical Society which, together with the report from that society, I place at your disposal. So much for the history.
On the discussion of this subject, which has been done frequently and efficiently, in the Journal, and elsewhere, the chief arguments against its use have been founded on its pernicious tendency in vitiating the fluids of the mouth, producing salivation, &c. Though this, independent of all other objections, is sufficient to condemn its use, there are other considerations which have not been fully weighed. I propose to offer some suggestions under the following heads in their order
1st. It is uniformly and necessarily inefficient in arresting caries.
2d. It is in every case dangerous.
3d. It is destructive to gold in the mouth either in the form of fillings or plate.
4th. It is never called for.
First. Inefficiency, no question is now more clearly settled than that dental caries, is chiefly, if not wholly owing to the chemical action of the acrid fluids upon the calcareous portion of the tooth, and hence the only object gained by any filling, is the protection of the exposed bone from such attack. It follows, therefore, that any attempt failing to accomplish this end, must be futile. Is this end attained by amalgam fillings? I answer promptly, no. Before giving any special attention to this subject, that such fillings did not hinder ingress to fluids into the cavity. The first was from observing that the plug when removed, appeared in all cases much more thoroughly oxydized on its posterior, than on its anterior surface.
And second, in all cases where the filling had remained any considerable length of time, the tooth was soft behind it, its earthy matter having been absorbed; to put this question to the test, I instituted the following simple experiment:
After preparing a quantity of the amalgam very carefully, I filled with it a strong glass tube, making it as compact as possible, and then suffered it to congeal undisturbed, after which I immersed it in a tincture of red sanders. In a very few hours the colored fluid penetrated entirely around it, absolutely hiding the cement from view. Now if this was the result in the case just described, and that too before any oxydation of its sides had taken place, what must be the result in the tooth, where the advantages for perlectly packing must be much less than in the tube. I may be permitted here to state, that, among the evidences furnished by Dr. B. to the committee upon this subject was a tooth which contained a very large cement filling; this was immersed in the same fluid. On breaking the tooth, the coloring matter was found covering the entire surface of the filling. This point being an important one to settle definitely, both on account of its rendering these fillings inefficient, and also giving a greater oxydating surface. I was induced to test its specific gravity as corroborating evidence, which alone would have settled clearly this point; upon this subject I need not repeat my own experiments, as we have ample testimony from good authority. In a treatise on chemistry by
Wm. Henry, M.D., F.R.S., with additions by Prof. Silliman, in speaking of alloys, he makes the following remarks:
"The specific gravity of an alloy is seldom the mean of its component parts. An alloy of silver with mercury, though the former metal is specifically lighter than the latter, possesses so much acquired density as to sink in quicksilver." Now, if the above observation be correct, the actual shrinkage in the process of hardening cannot be less than two twenty-fifths.
To make the absurdity apparent of using the compound, with the hope of arresting decay in teeth, no comment is needed.
Second. it is, in every case, dangerous. ln order to substantiate this position, it is by no means necessary to prove that this compound does, in every instance, produce salivation; indeed, so far from this, if it can be shown that a single case has ever occurred from its use, the point is gained.
This conclusion rests upon the fact that no man, however skilful, can judge, a priori, either of the natural or acquired susceptibility of an individual, in respect to the effect of mercury upon the system. Hence, whoever places this amalgam in the mouth, does so at the risk of the worst consequences, which are ever liable to result. This, I say, would be true, had there occurred but a single case of the kind. But since we have ample testimony of salivation being a very common result, and, moreover, that a vitiation of the secretions of the mouth a uniform one, the culpableness of this practice stands out in bold relief. Next let us lay aside, for a moment, the evidence founded on an observation of the result, and examine the properties of this paste, to see whether, by such examination, we should be led to anticipate what observation has shown to be true. To put this to the test, the only conditions necessary to be established are,
1st. That the mercury of the amalgam would become oxydized, and, 2d. That the amount of oxyd formed would, either as oxyd or as salts, by combination with the various acids with which it is liable to be brought in contact in the mouth or stomach, produce salivation.
Under what circumstances, then, is mercury oxydized? "Mercury is oxydized by agitation in a bottle, half filled with air, and is converted into a black powder" (Henry's chemistry, p.40). Now it is clear that any metal which would be thus affected by simple contact of air, would be far more liable to oxydation in the mouth. For example, tin and silver will retain a polish when exposed to air and moisture; but either of them is very soon corroded in the mouth.
The next question to settle is, whether this susceptibility of oxydation is enhanced by its union with silver as an amalgam? The following testimony, from Dr. Turner, is in point (Turner's Elements of
Chemistry, 6th Am. ed. p.309): The tendency of metals to unite with oxygen is considerably augmented by being alloyed. This effect is particularly conspicuous when dense metals are liquifled by combination with quicksilver. Lead and tin, for instance, when united with mercury, are soon oxydized by exposure to the atmosphere, and even gold and silver combine with oxygen, when the amalgams of these metals are agitated with air! The oxydability of one metal in an alloy appears, in some instances, to be increased in consequence of galvanic action. Thus, Mr. Faraday observes, that an alloy of steel with one-hundredth of its weight of platinum, was dissolved with effervescence in diluted sulphuric acid, which was so weak that it scarcely acted on common steel; an effect which he ascribed to the steel in the alloy being rendered positive by the presence of the platinum (Turner, p.89). (Alloy is a generic term, and includes all the various combinations formed by the union of one metal with another, while the amalgam is specific, and applies only to such metallic compounds as have mercury as one of the Constituents.)
If a similar galvanic action results from the union of silver and mercury in mineral paste, the mercury would, of course, bear the relation to the silver as did the steel to the platinum, in the case cited by Mr. Faraday. These two metals, together with the fluids of the mouth, would constitute all the essentials to a galvanic pile. If we add to these considerations the fact, that while "the current formed by the contact of two metals gives increased effect to the affinity of one of them for some element of the solution, the ability of the other metal to undergo the same change is proportionally diminished," we have at once a clear idea of the changes which occur, and the successive steps in the process. By the galvanic agency exerted betwen these two metals by the fluids of the mouth, the natural affinity of the amalgam for oxygen is so increased as to make the decomposition comparatively rapid. But the most important conclusion which may be drawn from these premises, is
the obvious fact, that the mercury (the most oxydable metal) would undergo much the most important, if not the entire change (Turner, p.89). For "when plates of zinc and copper touch each other in dilute acid, the zinc oxydizes more, and the copper less, rapidly than without contact." On the same principle, precisely, is the silver of this compound protected at the expense of the mercury.
It follows, hence, that while the presence of the silver greatly facilitates the oxydation of the mercury, the latter metal is principally acted upon, and the result must be a copious formation of a mercurial oxyd, corresponding to the amount shown by observation to be formed.
The only remaining question is as to whether the amount thus formed is capable of affecting the system in the way complained of. Of this, after presenting the following facts and considerations, I leave all to judge, who will lay aside prejudice. The amount of calomel, and other preparations of mercury, required to produce salivation, may be seen from the following quotations from the
London Lancet, and the British Foreign Medical Review:
"Very lately, a man who was taking sulphuric acid for epistaxis, was severely salivated by two grains of calomel, in a dose of cathartic pills. The acids naturally contained in the stomach were the muriatic and acetic, and the mercury contained in two grains of calomel, or a few grains of blue pill, would of course be sufficient to produce the most serious consequences, if changed into the bichloride, or corrosire sublimate."-Dr. Snow.
The following is the testimony of Mr. Streeter; "The fact of the action of blue pill being much more powerful at one time than another, might be accounted for by the conserve of roses, with which the mercury was triturated, being occasionally mixed with sulphuric acid, for the purpose of restoring its lost color. hence, instead of the simple oxyd, the sulphate of mercury was producing its effect on the patient. He had no doubt, however, that some constitutions were remarkably susceptible of the influence of mercury in its mildest forms. He had seen severe salivation produced by the administration of nine grains of blue pill, although it had been given in only one grain doses, three times a day, and its effects watched with the greatest care?" (Lancet jan.18, 1840, p.625)
We give the following quotation from Dr. Law, in corroboration of the above:
"We directed one grain of calomel to be mixed up with a sufficient quantity of extract of gentian to make a mass, to he divided into twelve pills, one of which was to be taken every hour. We found, in some cases, salivation to be produced by twenty-four of these pills, or two grains of calomel, and seldom were forty-eight pills, or four grains, required to produce this effect. We exhibited the blue pill in the same way, and found the mouth to become sore from six grains (It will be recollected that the blue pill is essentially the same as the oxyd formed in the mouth before acted upon by acids). We have found one drachm in every night sufficient to produce salivation."
Dr. Law accounts for salivation by such minute doses of mercury, on the supposition that a succession of impressions is thus kept up by the frequency of their administration. Nothing is more clear than that a very small quantity of mercury is capable of producing salivation, much less, I propose to show, than would result from a single cement filling.
I have one of these fillings in my possession which weighs sixty- three grains. Now this amount of amalgam would he sufficient to produce from the mercury it contains, thirty-seven grains of calomel, and about thirty-eight and one-half grains of corrosive sublimate. On the supposition that the whole of this was administered as calomel, in the way described above, it would be more than sufficient to salivate eighteen persons!
What are the real facts in the case? It has been shown that by the contraction of the mass in the act of congelation oxydizing fluids, have free access to the entire surface of the filling. A large oxydating surface, is hence constantly exposed to the perpetual action of these fluids. This oxyd, while it remains such, would get into the system only from the outer surface of the filling, and hence it accumulates, and would continue to do so till either some extrinsic acid, or the acid of the saliva, which frequently occurs under peculiar states of the system, unite with this oxyd, and convert the whole into a salt of mercury. It is a fact, moreover, that the mildest salt of mercury, which could be formed under any circumstances, is calomel, and inasmuch as the principal acids, prevailing both in the fluids of the stomach, and mouth are muriatic, with a small quantity of acetic, the presumption is, that corrosive sublimate, would be quite as likely to be the result, as calomel. Not only so, the mode of administration in respect to succession of doses, corresponds almost exactly with that above pointed out, in order to produce salivation with the least possible quantity of mercury. But while it'is true, that in most instances, the mercurial action would thus be got up only at intervals, alternating with changes of health, and natural fluids of the mouth, it is also true, that in many mouths, this oxyd of mercury, would be constantly changing into salts, from the uniform acidity of the saliva, and hence such persons would be constantly receiving the impressions from the oxyd of the entire surface of all the fillings in the teeth, and in no case would a person be freed from the amount of constant effect, which would follow from that portion of oxyd which accumulated on the outer surface of the filling. From the above facts and considerations, we make the following deductions:
1st. That every person wearing in the teeth any considerable Iquantity of this cement, is liable to salivation, from the accumulation of the oxyd shown above to take place.
2d. Every person is subject to so much of the constant effects, as would accrue from all the oxyd formed on the outer surface of these fillings, and which would be easily carried into the stomach.
3d. Those persons whose saliva is very generally more or less acid, would be subject to the constant impressions from the entire oxyd formed on the whole surface. In either of the last two cases, the effect would be sufficient to keep up an unhealthy action of the secretions of the mouth, if it did not amount to salivation.
4th. The constant oxydation and solution of the surfaces of these fillings, renders them less and less perfect, in respect to preserving the tooth, by giving more free access to those fluids which are the chief sources of decay.
Third. This amalgam is destructive to gold fillings and plate. The strong affinity of gold for mercury, renders this amalgam destructive to gold fillings or plate. I have seen in several instances the teeth which were clasped to secure the plate, filled with mercurial paste, and in each instance the clasp was literally eaten off at this point. To demonstrate this effect, we need only rub a piece of gold with the amalgam, when the surface will immediately become white to the extent that the amalgam of gold is formed. This amalgam like that of silver is oxydable and easily removed; gold plugs and plate are not only subject to this destructive process, from actual contact of the amalgam in its primitive form, but several salts formed from the oxydation of these cement fillings, and which are held in solution by the saliva, are also destructive to gold.
The fourth position we took in relation to this amalgam, was that its use is never called for. Though this position rests mainly on the ground, both of its inefficiency and hurtful tendency, yet were each of these qualities susceptible of remedy, it might easily be dispensed with. In substantiating this ground, we will briefly analyze the claims to confidence, which are set forth by its advocates, and which are offered as excuses for using it, the principal are the following:
1st. "Teeth so frail as cannot be filled with gold, may be filled with this amalgam."
2d. "A filling of this paste may be made to remain permanently, where one of gold could not."
3d. "The operation causes little or no pain," and
4th. "It is less expensive to the patient."
We remark in relation to the above reasons for employing "metallic cement," that they are so plausible without a careful examination, and such an one as few are enabled to give this subject, that its allurements are so strong, that we by no means wonder that so many unsuspecting people, have consented to have their teeth ruined with this worse than quack remedy, which unexamined, promised fair to shield them from one of the greatest ills which, at least bone, "is heir to."
It may be remarked also, that its claim is enhanced, not unfrequetitly by the former standing of those who recommend it were its use confined to itinerant quacks, the case would be different, but when we find for example, a man who claims to have practised dentistry in the same village for fifteen years, and that he has read and practised medicine for several years; when we find such a man, though stooping to this low degree of empiricism, claiming that he has successfully filled within the last twenty-two months, at least three hundred teeth with this mercurial paste, we need not be astonished at the number who would be thus inclined to try its virtues. But we will examine each of the above asserted virtues of this paste.
1st. What is the fact in relation to saving by its use, these "frail teeth" referred to, or inasmuch as it has been clearly shown that the paste is incapable of saving any tooth, we may inquire more properly whether gold cannot be used in all teeth, ~apable under any circumstances of being successfully filled. lf we are allowed to introduce testimony on this subject, we have it amply given in a resolution of the American Society of Dental Surgeons, in a convention held at Philadelphia,
August, 1841. In this resolution, unanimously passed by said society, it is declared, that "there is no tooth in which caries in it may be arrested, and the organ rendered serviceable by being filled, in which gold cannot be employed."
It is well understood by all who are conversant with dental operations, that caries frequently occurs where it is impossible to retain the entire shape of the tooth, but I would inquire, what would he gained by either making up for lost substance, with an article which can serve only to disfigure, or by undertakiug to fill beneath a portion of enamel, which would be fractured with the slightest pressure, with a material entirely incapable of preserving such delicate portion, or indeed any other part of the tooth. The fact is, that almost any tooth in which the nerve is not actually exposed, may be filled by a sufficient loss of substance, properly to shape the cavity. Under what circumstances then is it objectionable to sacrifice any of the substance of a tooth? The necessary loss would be almost exclusively confined to front teeth, and here the question again arises, what can be gained by filling under a portion of transparent frail enamel, with a substance which by its immediate oxydation and consequent discoloration, can only serve to disfigure, infinitely more than the actual loss of that portion of the teeth - to say nothing of the inefficiency or evil tendency of such fillings.
On the supposition that this paste was not objectionable in itself considered, its use would very rarely be indicated for such reasons, in the hand of a skilful operator, who uses instruments of sufficient delicacy, and foil of a proper pliancy.
I venture to assert that an exception to the rule, that gold may be generally used, would not occur in one case of a thousand, and in this case, paste could not be made to stay. Query- would three hundred such cases occur in twenly-two months to a person in a very sparse practice?
It is asserted, 2dly, that cement can be made to stay, where gold could not. This assertion shaped a little differently, is doubtless literally true. In other words it is doubtless true, that those who employ cement could make it more permanent, at least in many instances, than they could, a gold filling.
Were I under the necessity of charging my patients not to eat molasses candy, I certainly would resort to the use of cement, or abandon my profession. But the question is not whether gold would remain in the very cavity which some tooth mason had prepared for his cement mortar, but whether in any case, the cavity in question, might not, if skilfully prepared, be filled successfully with gold.
This question is virtually answered by the American Society, in the resolution above quoted, where it is declared in substance, that gold may be employed in all those cases where it would be serviceable to fill a tooth, and so far as my own opinion can serve to substantiate this view of the subject, I give it without qualification, in concurrence with the society, as expressed in said resolution.
It is a very common impression by those who are unacquainted with the pathology of caries, that while a filling remains, the tooth is safe, but all who are at all conversant with this subject, know that this is far from being necessarily the case. I have often been called upon to extract a tooth, having in the very cavity which was the origin of the difficulty, a gold plug, which from the imperfect manner in which the operation was performed, had not arrested the caries, but which had been retained there, in a consequence of the aperture through which it was introduced, being much smaller than the cavity within. This remark is particularly applicable to cavities filled with cement. That these filiings frequently remain till the mass by oxydation becomes much lessened, or till the tooth requires extraction from Ilie ill effect of the paste, or from exposure of the nerve, I freely grant. The difficulty often is in removing them, and indeed this is the very thing complained of. Did they easily escape, it would break the charm, and fewer evils would result from this species of quackery. 3d. It is asserted, that the operation of filling with this paste, causes "little or no pain." In respect to this point, it is quite as well known to patients, as the operator, that the pain of the operation, is almost exclusively confined to the preparation of the cavity for receiving the filling, and if it is essential, as it certainly is, to remove entirely the carious portion, when the cavity is to be filled with gold, I would inquire, what makes it less essential, when it is to be filled with paste-and if the care in this respect, be the same in both cases, how can the operation be less painful? The only conclusion which can be drawn in relation to those operators who verify this promise to their patients, is, that they do not remove the diseased portion of bone, which no one denies to be essential. Few men have ever made a greater figure with mineral paste, than the famous or "infamous" Mons. Mallan, and in relation to him, it is a fact, that he caused no pain in the operation, and the secret lay behind the filling, which on being removed, the mystery was perfectly apparent.
It was, that not even the foreign matter, was removed. In a well attested case it was found, that on removing several of these fillings, immediately after they had been inserted, the cavities were partially filled with "pound cake," which had been purposely lodged there, but a few minutes before.
In relation to the cheapness of such fillings to these wearing them, I apprehend that little need be said, after demonstrating both their inefficiency and hurtful tendency. The idea of paying half the amount of a good article, for one much worse than nothing, is a policy easily understood. But this by no means is the extent of the evil. The money paid for the operation is not merely lost, but the tee!h are thus sacrificed while the patient is feeling that they are being saved. Add to this the danger, and perhaps the actual occurrence of salivation, a siege of the tooth-ache, and finally the extraction and loss of the tooth, and we have a fair representation of the cheapness of a very dear operation.
Having now analyzed the qualities which it is claimed by its advocates to possess, I beg leave to offer an opinion, at least, upon the real inducements, or rather temptations, in all cases where the operator is not culpably ignorant of its real character, to employing this compound for stopping carious teeth. The principal are the following: 1st. It requires much less skill. 2d. It requires much less time, hard labor, and perplexity. 3d. The expense to the dentist is comparatively trifling.
That no special skill is required in using this article, hardly needs a single comment to prove. The fact that it becomes hard would render it evident, on the least reflection, that it would not be easily removed, in any case where the inner portion of the cavity was much larger than the outer. If this was not true of the entire cavity, if there were only two opposite projecting points, the object might be gained for a time. But, as has already been suggested, though it might remain, the tooth would not be benefitted unless it excluded from the cavity the fluids of the mouth; and the skill required to perform the operation would be far less than that exercised by the mason in making mortar adhere to an upper ceiling.
In respect to the comparative time required, we will let one of the chiefs of this tribe of operators speak for himself, in his own language, as is sworn to by several respectable witnesses:-"I can fill a tooth in a few seconds, sir, without giving the least pain. I filled thirteen teeth, yesterday, for a young gentleman of this city, a solicitor in chancery, a very liberal young gentleman. We can put in this composition of ours in less than no time; I filled those thirteen teeth yesterday in less than five minutes."
Here Monsieur Mallan asserts that he filled thirteen teeth in less than five minutes, whereas it not unfrequently happens that the most skilful operators spend an entire day on a single gold filling, meeting, at every turn, such difficulties and perplexities as can be appreciated only by those who have met and contended with similar ones.
In relation to comparative expense to the dentist, the sum is very easily stated. On the supposition that this cement contains sixty-four parts of mercury to thirty-six of silver, and estimating the mercury at one dollar per pound, and the silver at twelve dollars per pound, an ounce of this cement would cost forty-one cents, whereas an ounce of gold cost not less than thirty dollars, or more than seventy-three times as much as the same weight of mineral paste. To say the least, this would be a convenient saving, could it be made safely.
Having now briefly reviewed both the real and alleged properties of this paste, I subjoin the report of the committee appointed by the Onondaga County Medical Society, in June last. The circumstances giving rise to this committee, have been sufficiently detailed in the former part of this article; it will be borne in mind that it was appointed at Dr. B's earnest solicitation.
The report is as follows, viz.
The Committee to whom was assigned the duty of reporting to this Society upon the utility and safety of the royal succedaneum, in reference to its use in filling decayed teeth,
Observe - that there is a difficulty appertaining to the investigation of the subject, arising from the fact that the more intricate dental operations have been but in a limited degree the subjects of medical investigation.
Since dental surgery has been professed as a distinct branch of the healing art, there has been a disposition, (and we think a commendable one,) on the part of the medical profession, to confide both the investigation of the principles, as well as the practice of dentistry, to those who make that study and practice their exclusive object. And the Committee would have been quite willing that the diseases incident to, and arising from, dental practice, should also have been confided to the professors of the dental art, not doubting that they are fully competent to the task, although, from the acknowledged modesty and professional diffidence which characterize most of that profession, they might disclaim the possession of the requisite skill. But as the subject has been brought formally before the Medical Society, we observe, that cases have come to our knowledge, through one of the members of this Society, of serious injury resulting to a nujuber of individuals from the use of the royal succedaneum. We have also learned, from other sources, that in many instances bad effects have been produced, and, in some cases, that not only severe and distressing local disease has ensued from the use of the mineral paste, but the lives of patients have been endangered. On the other hand, we have the testimony of many persons who have had their teeth filled with the mineral paste, without experiencing any unpleasant effects; on the contrary, the ease, facility, and cheapness of the operation, and the fact that in these instances it has apparently answered all the purposes which could have been attained by the use of any other material, and has been used when, in the opinion of some dcntists, it would have been difficult, perhaps impracticable, to have used gold or tin foil, - all seems to imply some value in the practice. The testimony of an experienced dentist, upon whose representation of facts the Committee can rely, is, that within ihe last two years he has filled about three hundred teeth with the mineral paste, and that, to his knowledge, in no case has the specific effects of mercury been developed. To this statement it has been objected, that in a few instances the effects of mercury upon the mouth, from the use of the mineral paste, have been noticed in this village.
The Committee have no means of ascertaining the proportion of cases in which the mineral paste has produced the specific effects of mercury. As regards the utility of the paste, as a filling for carious teeth, the Committee have examined some cases in which the cavity seemed to be accurately filled, some months after the operation. To test this matter, however, by accurate experiment, a small vial was accurately filled with the amalgam, from which the free mercury had been pressed out by the application of great force. The vial was plunged into a colored liquid; in a few hours the fluid was found to have entered the vial by the sides of the amalgam proving conclusively that the amalgam diminishes its volume in the process of solidification.
That form of the paste which contains the smallest proportin of mercury becomes the hardest. It would apparently then, be the object of the dentist to diminish the quantity of mercury to the lowest point necessary to form the amalgam, so that, in the hands of the operator who would give to the article such proportions as would make the most eligible compound for use, the royal succedaneum would be less likely to produce injurious effects.
But it should be observed that the mercury and silver unite in but one proportion, and that any excess of mercury in the compound is in a free state; that when the mixture is subjected to the greatest degree of pressure to remove the free mercury, the amalgam then contains a proportion of sixty-four of mercury to thirty-six of silver.
To account for the activity of so small a portion of mercury, as the ordinary filling of a tooth would contain, the Committee refer to the admitted chemical principle, that "the tendeny of metals to oxydation is much increased by being alloyed." We find this fact so strongly stated and exemplified, by the standard chemical authorities, that the question has arisen in the mind of the committee, whether the presence of an equal quantity of free mercury, would probably be more pernicious, than the presence of the amalgam of mercury and silver. On this head the Committee also refer to recent published statements of interesting experiments, in proof of the occasional highly acid state of the saliva, not only in active disease, but in some instances, where there are but slight apparent deviations from health.
If it were admitted that the bad effects of the amalgam have resulted from an undue proportion of mercury, reasoning from the effects of even minute doses of mercury, internally administered, upon some constitutions of peculiar susceptibility to its action, the committee observe, that if the mineral
paste containing the largest proportion of mercury, has produced ptyalism, in numerous instances, that it cannot be so combined as not to produce its specific effects in some.
The occasional evil effects of mercury, even when clearly indicated, and used with care and discrimination, have been so often noticed and described by medical practitioners, that the
Committee need not enlarge on this point. In most cases, however, in which the local effects of mercury are injurious, some important benefit has been obtained to compensate the patient for his sufferings. If a patient were laboring under hepatitis or syphilis, he would have no good grounds of complaint, if his general malady were relieved, though the local effects of the remedy were severe.
It has been urged, that if the occasional bad effects of mercury -used in dentistry, are to preclude its use, by parity of reasoning, it should also preclude its use by the practitioner in all cases.
But the difference in the cases arises, not so much from the nature and effects of the article in question, as from the relative importance of the object to be attained. To incur the risk of ptyalism for the preservation of a carious tooth, would be one thing to take the same risk for the probable preservation of life, or for the removal of a serious malady, would be quite another. The first would he a matter of taste, or of probable convenience, the latter would involve the most important consequences.
The Committee enter into no discussion of the modus operandi of mercury in these cases. It would, however, be an interesting subject of inquiry and experiment, whether its peculiar effects are produced by the absorption and direct application of the mercurial oxyd to the parts involved, or whether it does pass into the general circulation, before its local effects can be evolved. Whether it is possible under any circumstances, and by any management to produce ptyalism, independent of the general circulation.
The Committee have thus endeavored to place before the Medical Society the leading facts in the case, and have added such reflections as naturally arise from the subject. That the mineral paste has produced, in many instances, the peculiar effects of mercury, though in diffcrent degrees of intensity, in some slight, in others severe and alarming, there can be no doubt. The Committee believe that the proportion of such cases is small compared with the whole number operated upon, but that no care in the combination or use of the paste will prevent its occasional bad effects. In view, however, of the apparently favorable cases, the question arises in regard to the probable effects upon some constitutions from the gradual absorption of the oxydized mercury, even when no palpable local effects are induced.
But we leave these points to the consideration of the society, referring the whole subject to it, for such action as it may choose to take, and for the expression of such an opinion of the merits or demerits of the mineral paste, as its regard to the interests of medical science, and its duty to the public may demand.
P.C. SAMPSON, Chairman of Committee.
I certify, that at the semiannual meeting of the Onondaga County Medical Society, held on the 30th
January, 1844, at the Temperance House, in the village of Syracuse, the above report was read and unanimously accepted by the Society. N.R. Tefft, Secretary.
Von den Gefahren der Anwendung des Silber-Amalgams, genannt
Succedaneum minerale, zum Plombiren der Zähne, von Talma,
Dentisten des Königs der Belgier in Brüssel.
On the hazards of using silver-amalgam, called Succedaneum minerale, for filling teeth.
Der Zahnarzt 1(1), 1846, 23-28
A substance which is to be used to fill cavities in teeth with any advantage, must be hard and impermeable, should attach to the tooth and form a uniform mass, and should not be mechanically or chemically attacked by foods or saliva, since only under these circumstances will it fulfill its purpose of protecting the inner of the tooth from air, degradation, contact with food and drink, contact with tools of various kinds and from the patient's use of tooth-picks. The tooth will not always heal from this but when the affected parts which still give opportunity for inflammation and pains are isolated and armed with a permanent harness, then the progress of the harmful processes will be disturbed and arrested. Manys teeth which appear to be almost completely destroyed can be retained for many years in this way.
If this hypothesis is correct, then it is clear that only a very plastic mass which easily can be placed in firm layers in the carious tooth, will resist chemical compounds and has no harmful effect on the tooth tissue, has any advantage. Substances which combine these properties are rather expensive; their proper use requires patience, skill and caution - circumstances which not everyone understands.
Under these circumstances it has appeared easier for some people, and especially for our collegues in England, to invent certain doughs which are placed in the prepared tooth in a soft condition, harden there and should fill the empty places.
Among these doughs there are several which have got used too much but which have damaging effects and we think it is our duty to focus attention to these. I think especially of those doughs which have mercury as a component and which, because of the characteristics of this metal, has the strange property of first becoming soft and then to harden when it takes up and releases the softening substance.
Thin, colored, dissolved compounds which are applied in the liquid state in a tooth which is damaged close to the pulp and which is still in the mouth or just extracted, will rather quickly penetrate not only the bone structure of the tooth but also partially the enamel - an experiment which is easy to do. Mercury especially has to a high degree the property of penetrating and saturating anything which comes into contact with it. Therefore, teeth which are filled with silver-amalgam, called Succedaneum minerale, will rather soon become black or bluish- black.
The metal is apparently not protected from oxidation by the the influence of the acid secretions of the oral cavity and which penetrate between the putty and the cavity walls; this oxide will be saturated with hydrogen sulphide and take on a very black color. The oxide is dissolved by the same liquids which caused its formation, penetrates and fills gradually all tissues of the tooth.
From numerous observations, I have come to the conclusion that the mercury which is brought into the tooth to be repaired with the amalgam can separate from it by the heat of the mouth, migrates into the dental tissues and there cause the same signs of irritation and disease which are produced when mercury is swallowed or rubbed into the skin. I have witnessed severe cases which were the consequences of filling teeth.
Baron v.P. from Lüttich, had seven or eight teeth filled with Succedaneum minerale; The day after the operation he developed severe pains in his whole head, accompanied by cramps in the cheeks, profuse, thick salivation, unbearable metallic taste in mouth and nervous pains which continued for most of the day and did not disappear until the teeth were liberated from the mass.
Count v. A. in Brussels, had a tooth filled with an amalgam of silver and mercury, used by some dentists. The operation seemed at first to be a complete success. But on the third day he got headache and ache in the jaws connected with rich salivation which was so profuse that the, at the same time loosening tooth, could not be kept.
The investigation showed that the roots in some places were colored black, in other places green.
The latter coloring appeared to have come from copper which contaminated the not enough purified silver. Quickly after the extraction of the tooth, all problems disappeared and did not return.
Dr. Th. in Brussels had several teeth filled with Succedaneum minerale. On the fourth day after the operation he was seized by violent pains in his teeth and in his whole head and a violent fever developed.
Mr. v. O. in Brussels, who was to leave fo a military campaign and who could not wait until I could replace a several year old but lost gold filling from a non-painful tooth, turned, as he thought whithout risk, to another dentist who filled in Succedaneum minerale. Already the following night he felt generally sick, got intense pain radiating from the tooth over the chin, profuse salivation with clear metallic taste, nervousness, fever, unintentional contractions of the jaw muscles etc. Mr. v.O. returned to Brussels; he said he felt like an insane since 48 hours. I removed the paste, still soft, from the tooth and the attacks diminished without delay. A few days later I again filled the tooth with tin foil and for three years this has kept the tooth free from pains.
It is common that the pains appear first five, six or even fourteen or twenty days after the application of Succedaneum. However, then the paste is hard like silver, the tooth is impregnated with mercury and since the foreign substance in the tooth can not be removed, the only remaining action is to extract the tooth. If some other filling material had been used the tooth might have been retained.
A young lady from Mons, who visited Brussels, was persuaded by a friend to fill some pinheadsized holes in the upper incisors with Succedaneum. A few days later the lady noticed that the paste had become black and looked like a piece of shale. Since the color became darker and darker and spread out, the lady came to me in desperation and told me about her adventure. I succeded, not without trouble, to remove the paste and to scratch away the black color from the cavity walls; but the affected teeth remained grey and without lustre and had such unpleasant effect since all other teeth were beautiful and white. Since the caries only had a limited extent, both my patient and myself hesitated for the the pains and trouble to remove the stained crowns and replace them with artificial ones. We had to be satisfied with gold-foil fillings. These had to be renewed twice in a year since the gold was attacked by the stubborningly remaining mercury but then no further problems have appeared.
It would be easy to present innumerable examples of the harmful effects which were caused by the filling with mixtures of silver and mercury, but such repetitions would not increase the weight of the
facts just presented. My intention is preventive and to make my fellow practitioners aware of the dangers and damaging effects which are connected with any filling material which contains mercury; this metal is a true poison for the teeth.
Relating to the operation of filling, regretfully the method in question has such harmful consequences since it is rapid to perform, can be understood by anyone, requires no special skillful handiwork and requires no learning of special placement methods to avoid pains which often might be violent.
Really, regarding myself, I was in the beginning uncertain and needed facts which were provided by doctors; later I acquired own alarming experience which made me decide not to use this filling method.
I have followed the various changes of this filling material since 1819 when it first was praised under the name Bell's paste. It is the same material which was presented under the name Taveau's silver paste a few years ago and which in recent times has been given the proud name Succedaneum minerale. I admit that it at first caught my interest. Just like many others who, at the first moment, were deceived by its simplicity, I made some experiments with it. I hoped that gold would render it more long- lasting than silver and made an amalgam from gold and mercury, just as white as silver, but the mentioned properties made me abandon it.
The english method has in the meantime spread too much on the continent, where some persons, shameful to their profession, try to make a secret of it, pretend it is a new method or even their own invention. By this and by a number of other methods of all kinds, the number of misled practitioners are increasing and these will undoubtedly cause futher damage since the public will only learn from bad experience.
I must also add that the method described does not at all arrest caries, even if the other described and miserable consequences do not appear. The latter problems might start slowly and insidiously, however, and perhaps quickly and more apparent, get worse. The paste will become fragile from loss of mercury which partly evaporates from the heat of the mouth, partly is deposited in the tooth structures. As a consequence, the moisture of the mouth will again have access to the cavity of the tooth, will remain between the walls of the tooth and the filling and dissolve the latter and cause it to fall out. Simultaneously the cavity will enlarge. These processes will be accelerated by stagnant moisture and remains of food which decompose, produce bad smell, become acidic and consequently increase the degradation of both the paste and the tooth tissues.
To sum up: the least degradable substances which completely adapt to the the hollow parts of the tooth, is most oxidation-resistant and which forms a firm mass which is impermeable to liquids is best suited for filling teeth. So far, gold and tin in the form of thin foils are the only known metals which dentistry with certainty can use for this purpose.
Letter from Professor SLACK, to JAMES TAYLOR, M. D., D.D.S.,
Professor of Practical Dentistry and Pharmacy, in the Ohio College, of
Dental Surgery, Cincinnati.
The Americal Journal of Dental Science Vol 8 1848 172-178
DEAR Sir:
I perceive, by the February No. of the "New York Dental Recorder," which you were so good as to allow me to read, a considerable controversy has been raised in New York, by action of a dental society, in regard to a quack and most reprehensible method of filling carious teeth with an amalgam of gold or silver, and we presume, more frequently, tin or lead.
I would here remark, that it behoves us, who live far over the mountains, to see that our practice in the only dental school in the west, be regulated by sound principles; let others do as they may.
In an examination of the subject before us, it becomes, in the first place, to attend to a few elementary particulars, which some may call small things, but to my mind, are, at the very foundation of the investigation.
The composition of the tooth, consisting of more than one-third cellular tissue, one-half phosphate of lime, one-tenth carbonate of lime, and a small fraction of fluoride of calcium, is an item to be remembered. The enamel differs from the body of the tooth only in the amount of phosphate of lime, which, on careful decomposition, is found to be 75 per cent.
It is a fact tolerably well decided, that the silicious coating of the wheat straw, Indian corn stalk, various grasses - of the cane, ratan, bamboo, &c, is reticulated. Also, that the enamel of various oceanic and fluviatile shells possess the same form of structure. The microscope examination of the exterior of a well conditioned tooth leads to the same result, i.e. a smooth reticulated or net-work coating.
Secondly. Eremacansis is slow combustion or gradual decay, and has been ably investigated by
Liebig, and confirmed by Dumas Gregory, and all chemists, who endeavor to keep pace with the rapid march of this noble science. This process of decay, slow combustion or oxydation, so important to the dental practitioner requires certain conditions to promote it. There must be moisture; a certain temperature above 32°, a blood heat 98°; or even higher, as in hot tea or coffee, or other heated articles of diet. There must be oxygen either from the atmosphere, or some other source, for eremacansis decay, or slow oxydation cannot proceed without this latter, which the atmosphere must, in 99 cases out of 100 furnish. Decay, or slow oxydation, then must begin in the external part of the tooth. In the interior oxygen could not be furnished, unless by some potent disease a passage be opened to the atmosphere. Eremacansis is the action of a substance in a state of decomposition, the particles of which are in intestine motion - placed in contact with another substance, whose chemical affinities are easily overturned, so as to produce the same change in the latter substance: ego, suppose decaying matter, with the circumstance above detailed, be brought in contact with the external of a promising tooth, and continued for some time, what, in living tooth is lilkely to be first affected? I have already spoken of the reticulated form of the enamel and of the cellular tissue, which contains nitrogen, and which all chemists admit to be held by the feeblest affinities. The substance in decomposition operates, in my view, first, on the nitrogen of the cellular tissue through the small openings of the enamel, and thus produces the same motion and decomposition in a fraction of the living tooth tissue. I am aware that sometimes the caries seem to attack the phosphate of lime, while the tissue remains, but careful examination, will, I am persuaded, from the very first, disclose in all such cases, a deceidedly unhealthy state in the tissue, though the greatest ravage may appear in the phosphate salt. It is my design to be concise, if practicable, and must thirdly consider the chemical action of substances employed in filling carious teeth on the organism in question, and on the general system. I have no objection to the employment of one metal such as gold, silver, or platina, if in the state of delicate foil. I will not object to tin foil, if it be pure or free from lead, with which it is, in 9 cases out of 10, adulterated in the tin foil commerce.
The filling ought always to be with one metal, and only one to avoid galvanic action, which will result where two metals are employed together. A certain amount of electricity is incident to every substance, whether organic or the contrary, and this is necessary in the organised to a healthy condition; but augument the amount and you invariably have unnatural action, which, if continued, will end in certain, and sometimes, fearful disease.
It may be said there are few metals which produce galvanic action. I deny the position, and my denial is confirmed by the gold plate and solder producing galvanic salivation, as reported in the
February No. of the "New York Dental Recorder".
Tin and copper vessels always are oxydizing and corroding, where the solder join the parts furnish a decided effect, produced by small quantities of galvanic electricity. The principle of delicate galvanic action is shown in Davy's beautiful contrivance for preserving the copper sheeting of vessels in oceanic waters, by small substratum of zinc or iron nails - changing by induction the electrical state of the copper. On the same law a copper kettle in boiling cider or pickles, is rendered measurably innoxious by immersing in the liquid a piece of pure metallic tin; without the tin it will be most certainly poisonous. The law of induction is illustrated by the practice of packing razors or surgical instruments in zinc cases to prevent rust; the electrical state of the steel instruments is changed to the same with the oxygen of the air; of course, union does not take place - even animal matter, as slices of brain and muscle, and vegetable - as sections of beet root and walnut tree furnish an example of distinct galvanic action where no metal is concerned - but to return to the amalgams noticed above, as used for filling carious teeth. Is it not true that the mercury miners at Idria in
Austria, Almeden in Spain, or Guaneavilica in Peru, are frequently affected injuriously by the crude article in which they work? Is it not true that sailors carrying cargoes of metallic mercury are sometimes salivated? These facts show that mercury is easily changed so as to produce the effects noticed; I say changed, for few pure metals are poisonous. Copper, while clean, is inert, but let it be oxydized, i.e. changed, and it becomes poisonous. Lead, when pure, I may affirm, is inoxious, but let it be oxydized, which it must be before combining with carbonic acid, and it is changed; carbonate of lead results, which produces painter's colic, and many other forms of poisoning.
Amalgams are but another name for alloys. In alloys it is a principle that the compound is more changeable than the simples forming the combination. Alloys universally attract oxygen more energetically than the metals of which they are composed. Is not an alloy more inclined to oxydation, i.e. to chemical action, and of course, to galvanic action than its simples?
Does not galvanic action, even in the common battery, primary result from the oxydation of one metal in the series? Is not this the laws of the battery? Mercury and gold, mercury and silver, mercury and tin, are peculiar combinations or alloys called amalgams, and these are most strikingly sensible to oxydation, and is not this, of itself, prima facie evidence that galvanic action, to no small extent, results. I speak theoretically but I have little doubt of the fact, that a few combinations, an
amalgam of gold, or silver, or of tin, (I will not mention bismuth or lead) arranged in order, would produce the effects an imperfect battery. Is it not true, that an amalgam of zinc, tin and mercury
(though the tin may be emitted) is considered necessary to the full excitation of the common electrical machine on which the friction of the amalgamated rubber is employed. I admit, with Davy, that the action of this amalgam is unexplained, but I have often thought that posibly the metals combined, evolve by friction, galvanic elctricity, which is identical with that of the common glass machines that from this source and the neighbouring bodies a large supply of electricity is regularly furnished. this is not more extraordinary than other facts. I have known considerable electricity collected from a piece of dry wood, moved swiftly in a turning lathe, another dry stick being applied to the former, to maintain friction. Fire is easily produced by such friction. Hence Count Rumford's wind-fall of continued friction, producing caloric as long as the motion was kept up, is not so strange after all. In the new hydro-electrical machine, the wonderful evolution of the electrical fluid, from which sparks 20 inches long were drawn by Faraday, he inferred arose from the friction of the steam against the orifices of the tubes from which it issuing.
The examples of the electrical amalgam, the dyed wood the hydro- electrical machine, are introduced to show the wonderful variety and delicacy in electrical action, which no philosopher has satisfactorily explained. Why may not galvanic action be promoted by friction as well as acids? How do we know that an amalgamed rubber mechanically pumps up the electrical fluid? The accumulation of the fluid is known, but the why and wherefore we know not. The delicate galvanometer affected by the movement of the hand on the slightest friction, clearly showing that the electrical or galvanic fluid is present. If a plate of zinc and a plate of copper, each with an insulated handle, be brought together and suddenly separated by a delicate electrometer, the zinc will be found in a positive state and the copper in a negative. Without this expedient they are both said to be positive. Whence the change? It will be answered by induction. Then one plate before the contact must have held more of the fluid than the other. May not the simple contact, producing friction, have generated or excited galvanic action? The subject is curious and recondite, but not probed to the bottom. It may be (a supposition) that friction on the amalgamed rubber, the dry wood, or in the hydro-electrical machine, is one means of promoting galvanic action.
The galvanic and electrical fluids are for the most part identical, except in the common machine, the fluid is more dense, in the other more rare, but in larger quantity. They both decompose; they both effect the living subject with as much similarity as their different circumstances and modifications permit. Galvanic action is so variant that it becomes the dentist lo look well to its laws, if he expect to excel in his profession, or be, as he professes, a benefactor of mankind.
Again, the amalgams so extensively employed in filling carious teeth before employed in such a service, ought to be subjected to the most rigid chemical examination, that the beauty of the face and the general health of the patient may be promoted - if these important points be not reached, the practice ought to be, must be abandoned, as wholly improper. if eremacansis be promoted by the absorption or action of oxygen - a chemical principle well established - I say, theoretically, but, as I believe, truly, the usual amalgam fillings above noticed, must promote decay. And in Dr. Allen's communication referring to the practice, which he seems somewhat to condemn, the fact is abundantly confirmed; and on inquiry, I find a considerable amount of facts, in the west, fully establishing my previous reasonings.
I laid it down above, as a principle somewhat certainly established, that a pure metal, with few exceptions, is innoxious, but one, or especially a compound, easily attracting oxygen, in general, deleterious. Will not this remark, based on principles apply most pointedly to the practice in question?
Again: The cellular tissue of the tooth is filled with minute arteries, veins, absorbents and nerves; - leaving out of view galvanic actions - what must be the effect from the oxydation of the inserted amalgam? Will not the deleterious ide compound be absorbed? And can a substance certainly poisonous, be any advantage to nerve, artery, veins, blood, &c? It will be thrown into the circulation, and through the poison may move slowly at first, it will most certainly, unless arrested, perform its work of destruction. Health must be prostrated, and an early grave will be the portion of the victim. Let chemists of experience, or physiologists who understand the chemistry of the system
(which the great Liebig unfolded, and which by others has been most triumphantly confirmed) speak out, and they will, for the most part, confirm what I have advanced. No other rational conclusion can be drawn from the premises.
PROCEEDINGS OF DENTAL SOCIETIES.
The Dental Cosmos 1861, 548-558
PENNSYLYANIA ASSOCIATION OF DENTAL SURGEONS. REPORTED BY GEO. T. Barker,
D.D.S.
A monthly meeting of the Association was held on the evening of April 9th, 1861, at eight o'clock.
President, Dr. Dillingham, in the Chair. Present, Drs. Buckingham, Flagg, Fitch, Garretson,
McQuillen, Roberts, Peiree, McGrath, Ellis and Barker.
The subject for discussion stated by the President to be
AMALGAM was opened by Dr. Peirce, who said, in opening this discussion he was not unmindful of the liability to misrepresentation one incurred in speaking favorably of amalgam. First, on the part of those who, purposely ignorant of the material so far as their own experience is concerned, are constantly attributing results to it that are due not to the amalgam, but to its improper use. Second, by those who, unable to perform a successful operation with gold, are eager to seize upon any remark in favor of a plastic material as an apology for their own empirical conduct. But fully indorsing a remark made some weeks since by Dr. Flagg, "that the mission of the true dentist is not merely to be able to put in a solid gold filling, regardless of consequences, but to operate in such a manner as would best subserve the interest of the patient, all things being considered," he was willing to give it such defense as it deserved. That there are teeth that can be saved for a much longer period and with greater advantage to the possessor, with amalgam than with a foil, no unprejudiced practitioner can deny; such teeth are the third molars that have been neglected until their pulp are nearly exposed, or would be quite, if all the disintegrated dentine was removed; these can be filled and preserved for years with a material such as amalgam offers, while to destroy the pulp and fill with gold from the necessarily frequent imperfect manner in which the operation is performed, the tooth in a few months at most must be sacrificed in consequence of severe periostitis; nor are wisdom teeth the only ones in which it can at times be advantageously used - both the first and second molars may be in a condition where it would be successful. In the anterior teeth, under no circumstances would he use it, believing that the preservation of their beauty is as essential as subserving the purpose of nutrition. The objections which have been urged from time to time by the most radical opponents of amalgam are, that it produces periostitis, alveolar abscess, exostosis, necrosis, and that it might occasion ptyalism.
The last and doubtful result is the only one that we do not frequently find where teeth are filled exclusively with gold, and it is of so rare an occurrence, that he believed the profession had never heard of but one practitioner who thought that that result was produced by amalgam. With the cause and treatment of the other difficulties complained of, we are all familiar, and that they should he more frequent proportionately or attended with a higher degree of inflammation than good gold fillings, is not surprising, inasmuch as the amalgam is used to such an extent by incompetent practitioners.
He would ask, who has not relieved periodotititis where there was an approximal filling by the proper application of a file to the ragged and protruding edges, whether it be gold, tin, or amalgam?
Who has not, time and again, removed both gold and amalgam fillings, and successfully treated fangs for alveolar abscess? Who has not extracted exostosed and necrosed teeth, filled as well with gold as amalgam?
The fault is not in the material but in the manipulation, and with the same care in performing the operation, the evil results mentioned are as little likely to follow with the one as with the other. But amalgam has faults, and grievous ones; in the largest proportion of teeth that are filled with it, their good appearance is completely sacrificed, and for that reason he would never, as remarked before, place it in an anterior tooth, nor considered it in any respect adapted to a small cavity, where either gold or tin could be used.
In defense of amalgam, he would state that the cavities in which he should deem it advisable to use it are proportionately very few, but that must be left with the judgment of the operator, and that judgutent must be based upon a proper appreciation of his professonal duties, a thorough knowledge of the tooth upon which he is to operate, and the relation it bears to the animal economy.
Of the materials which have from time to time been used in making the amalgam, none, be thought, have any advantages over the silver and tin, or what is known as Townsend's Amalgam. If it were desirable to insert a temporary filling having more durability than gutta-percha or Hill's stopping, an excess of tin used in the preparation of the filling would make it more easily removed.
Dr. Buckingham said. he had been using amalgam sparingly for a number of years, and thought a dentist, to do justice to his patients, should use it in certain cases. He knew that some writers said that any tooth that was worth filling could be filled with gold, but believed he had made teeth useful for a number of years that could not have been filled with anything but some plastic material, either amalgam or other substance similar to it.
He had never seen a case of salivation from its use, and had doubts about its ever having produced ptyalism. If he understood the action of mercury on the system when it was used either externally or internally, the effects were the same, viz., an increased action of the secreting organs, particularly of the salivary glands; the next effect in the mouth was the swelling of the gums, the teeth becoming loose, and sloughing and necrosis of the parts the final result. These were influences produced through the general system, but he did not think amalgam filliings would produee these effects.
As for the permanency of amalgam fillings, he had seen several that had been in for fifteen year, which appeared good; in other cases he had known them to give out in a very short time; but he was not surprised at this when he considered the class of teeth it was generally used in.
The amalgam composed of silver, tin, and as little mercury as could be used, was the kind he preferred. He melted pure silver and pure tin as he could get together, in the proportion of four of silver to five of tin, and kept it in the ingot form and filed it as he wanted it for use. When kept in this way, he thought it did not oxidize as much as it did when it was kept filed.
Dr. McQuillen remarked that no material employed for filling teeth has been a more prolific cause of controversy among dental practitioners than the subject under consideration this evening. In former days controversialits of an hour of both sides, gained for themselves an unenviable reputation, by the manner in which they opposed or defended the use of sense would employ or respond to, and which, when used, are ever the surest test by which to judge not only the breeding of scribblers, but also the shallow pretensions of the charlatans of science, were used in the most liberal manner.
Introduced into the American Association of Surgeon Dentists, the controversy was carried on with so much spirit and animosity, that a majority of the members forced a resolution upon that body, making it obligatory opon all, either to sign a pledge promising never to use the material, or else tender their resignation. Many of the members preferred the latter alternative, and the Association emerged from the struggle weakened rather than strengthened by the conflict.
The agitation of the subject (which was not confined to the professional journals, but to a great extent carried on in the daily press) attracted the attention of the community and aroused a strong feeling of prejudice against its use on the part of patients.
In this prejudice Dr. MeQuillen had shared, and believed that he never should be able to entirely free himself from it. And when the late Dr. Townsend advocated in this Association, about six years back, the use of amalgam prepared with greater care and in a different manner from former preparations, influenced by this feeling, and to a great extent by the opinions and positive assertion of those in whose judgment and veracity he then had every confidence, he opposed the use of this agent. Since that period, candor compelled the acknowledgment titat his views had changed, and he does not now regard amalgam as the unquestioned cause of all the difficulties that have been ascribed to it; for in an experience of fourteen years he could not recall a single instance of necrosis of the jaws, ptyalism, etc., of which others assert that they have seen so many. Recognizing the fact that idiosyncrasies sometimes exist in which the employment of the smallest quantitity of certain medicinal agents is followed by the most untoward results, he would not pretend, however, to offer this negative evidence as positive proof that such things never have occurred, but his own experience had made him look upon those who assert that they have seen so many cases, with considerable doubts as to the value of their judgement or opinions, as reliable diagnosticians.
Asserting that there are teeth which it would be impossible to fill with gold foil, and yet too valuable to sacrifice, be stated that under such circumstances, and such alone, would he feel justified in using this agent; for, notwithstanding the fact that he believed that it had been much belied, he could not, as already stated, entirely free himself from such prejudice so as to use it indiscriminately. Again, it not only required more skill but also afforded one more satisfaction to introduce a good gold filling, and such practice was by far better calculated to enable one to establish a high reputation as an operator.
As evidence of the value and durability of amalgam fillings. he had seen many teeth which had been filled for more than twenty years, as good as the day the operations were performed. An opportonity had been afforded him that afternoon of examining a number of amalgam fillings introduced by Dr.
Flagg to prove that one of the great objections urged against them (discoloration of the teeth) can be obviated. In all of these cases, which had been in from eighteen months to two years, there was not the slightest appearance of discoloration, and there was no doubt that the teeth were as fully indemnified against decay as if they had been filled with gold foil.
Dr. Fitch was well aware that he was stepping upon controverted ground. Many eminent dentists had used and still use amalgam occasionally for filling certain classes of teeth in particular stages of decomposition, and others of equal celebrity had wholly condemned its use. He thought it quite possible, at least with some, that early prejudices may have had not a little influence in producing their wholesale verdict of condemnation. In some repects should have to plead guilty to this charge, as prejudices, early imbibed, had led him to look with considerable suspicion upon amalgam as being, in any sense, a proper material for filling all classes of teeth; and did his observations extend no further than to those sad and deplorable results witnessed in some mouths, where its use had been general and indiscriminate, presenting teeth in all stages of decomposition and of all shades and hues of color, from inky blackness to that but little removed from their natural complexion, he too, most assuredly, would condemn its use and consign it to a region far removed from dental practice; but when remembering to have seen teeth claimed to have been filled fifteen or twenty years, in a good state of preservation, but somewhat discolored, and after having used it for plugging certain classes of teeth, with variable success, for the last sixteen years, he was disposed to give it its appropriate place in the list of materials to be used in special cases, after a definite formula of manipulation, even at the risk of incurring the charge of encouraging empirism and cheap dentistry. Regards the arguments which are often urged, as to its cheapness, and the great facility with which it may be manipulated, as demanding not even a pasing notice, really amounting to nothing if these be its only claims upon our attention as a material for the preservation of teeth. The considerations of a very few points will exhaust the entire question. Its susceptibility of being made adherent, or its nice adaptiveness to the walls of the tooth; its coloring effects; its toxical nature; and its expansion or contraction in crystallization. If it be found faulty in either of the above particulars, it must militate very much against its use. He believed, with careful manipulation, that it could be so adapted to the sides and angles of the cavity as to exclude all foreign destructive agencies, unless this adjustment be interfered with by its contraction while setting.
One of the maIn argumeuts urged by the opposers to its use is, that it imparts to the tooth its coloring properties, disfiguring and destroying the beauty of their texture. This, indeed, is a very serious objection, and is sufficient of itself to condemn it, if the argument be founded on truth and justice; but may not this result be due more to the impurity of the materials, or to the presence of their oxides, or the manner of their combination, rather than to any action directly upon the materials themselves?
That teeth are, and have been shamefully discolored by it, is a fact, and from this its use has been abandoned by some, and by others, whenever employed, restricted to molar teeth and those very far gone in decomposition.
He thought much of the discoloration arose from the impurity or degeneracy of the materials, as he found no free or combined acids In the secretions of the mouth that would act to any extent upon pure mercury or silver. These articles, especially the mercury of commerce, is found quite impure, and the silver usually very much oxidized at the time of using, consequently entertained the idea that the coloration was very much due to these circumstances. While the secretions of the mouth do not act readily upon pure mercury or silver separate or combined, the action must be very considerable upon their oxides, and was of the opinion that could something be employed to remove these oxides at the time and after mixing the materials, the coloring properties of the mixture would be mostly if not entirely removed. He was satistied that alcohol would not entirely do this, yet it removes much that is impure. Nitric acid is the only acid that acts to any extent, either upon pure mercury or silver, at a temperature at all permissible with the safety of the oral structure, and not being found in the sercetions of the mouth, therefore coloration is not due to acid reaction. Strong acetic acid used with articles of food, by its constant repetition may slightly tarnish their surfaces, but nothing further.
Coloration may be due to galvanic action induced by the saline secretions of the mouth, in the oxidation of one of the baser metals, or to the presence of sulphocyanuret of potassium in the salivary secretions.
In regard to its toxical or injurious effects upon the system, was inclined to question if not wholly doubt any such influence, and concurred in views advanced by Dr. McQuillen, that he had yet to see the first case of alveolar abcess, ptyalism, etc., due to the presence of mercury in the amalgam. It is well known that mercury uncombined is inert, and equally so must it be when combined with silver or tin. The proto-chloride of mercury (calomel) and deuto-chloride of mercury (corrosive sublimate)
are formed from the sulphate of mercury and muriate of soda, triturated and sublimated. As this process cannot very well be carried on in the mouth, it is hardly supposable that they are elaborated to any extent.
He thought that mercury and the crystals of silver expanded a trifle in setting, and had wittnessed a few instances where the tooth, being thin had checked after its use; yet could not speak with any certainty in reference to it. It was thought by some to contract; he this as it may, if either result followed to any extent, it should not be used.
But seldom used amalgam, and then never in any but molar teeth that were very much decayed. He considered equal care as necessary, in preparing the cavity and introducing the filling, as where gold or other materials were made use of, but much preferred gold for these particular cases, even where there is danger of breaking the tooth. Recently had seen some very fine amalgam fillings introduced by Dr. J. F. Flagg, where the teeth, after having been filled eighteen months, were in a state of perfect preservation and entirely free from coloration. This was due, as was claimed, to some peculiar manipulation or washing of the material, instituted by the doctor, and which he doubted not that gentleman would explain. Was shown others of five years' standing, performed by Dr. Flagg without having subjected the material to this peculiar process of cleansing, where the teeth were preserved but somewhat discolored.
Dr. J.M. McGrath said, unlike the gentlemen who had preceded him, his mind had never been imbued with any prejudices against the use of amalgam for filling teeth. From the day he first entered the profession up to the present, he had never hesitated to use it whenever he thought it necessary, and as yet had never seen any bad effects resulting, such as have been ascribed to its use by many practitioners. He would also claim the privilege of adding the same testimony for his father,
(Dr. R. McGrath,) who had been in the habit of using it occasionally for the last ten or fifteen years.
He did not wish to be understood as asserting that amalgam fillings have not failed to arrest the progress of decay in teeth, and that no matter with how much care the filling may have been prepared and inserted, such teeth have not continued to decay, and in the due course of time the fillings have not fallen out; such instances, he knew, occasionally occurred, but did not believe these facts are any arguments against its use, for we find the same thing happening to gold fillings. An imperfect gold filling will no more arrest decay due to local causes than a badly prepared amalgam filling; and in those cases where the decay is due to constitutional causes, unless the patient receives constitutional treatment, the finest gold fillnig ever inserted will be of no permanent avail. As regards the discoloration, he rejected the theory of the formation of the chlorides within the mouth or in the preparation of the filling.
He then stated an instance, where, about two years ago, he introduced an amalgam filling consisting only of pure silver and mercury, and happening to see it to-day he found it as perfect as when it was first inserted, not even having discolored during the two years it had been in the mouth, in the slightest degree but retaining its original hue - of frosted silver.
Dr. Flagg said that he had shared strongly in the prevailing prejudiee in regard to amalgam which existed in the profession during the early years of his practice of dentistry, and recalled vividly his feeling of mingled sorrow and astonishment when almost after his return from California, some six years since, his father mentioned to him that he wished to call his attention to a plug of Townsend's amalgam, which had been recently inserted. From that time to the present, he had been experimenting as to the availability of the material and as to the validity of the objections which had been urged against it.
Had for some years noticed that, as a general rule, fillings upon approximal surfaces failed in a comparatively short time, while fillinga properly introduced into cavities properly prepared upon the articulating surfaces remained perfect, (with the exception of discoloration,) and saved the teeth.
Was compelled to oppose entirely the statements which had been made regnrding constitutionally injurious effects from the use of amalgam. Had seen many cases of irritated gums looking terribly enough to afford ample opportunity for learned dissertations from operators to patients upon the effects of mercury upon the gums. But would say that he had never met with such a condition which was not dependent eitherr upon mechanical irritation, and which would have resulted just as soon from an equally bad gold plug, or froto constitutional causes entirely foreign to the abused amalgam, and which yielded to proper constitutional and local treatment.
Would be explicit in the opinion that it was barely possibIe that an idiosyncrasy could exist in which amalgam, per se, might be injurious, but wished distictly to state that, during a period of six years, had seen amalgam plugs in many hundred mouths, and had yet to meet with the first deleterious indications resulting therefrom. Had again and again treated teeth suffering from periostitis, abscess, etc., attributed to amalgam, and refiIIed them with amalgam for the sole purpose of proving to patients that the material used had nothing to do with the trouble existing. Had for some time regarded the discoloring of teeth and the failure to preserve teeth in plugging certain cavities the only valid objections to amalgam. The latter he had not as yet been able to overcome; but the former, through the instrumentality of his friend, Dr. J.E. Garretson, he had been able in a great measure to do away with. About two years since, Dr. Garretson had mentioned to him, as result of the admixture of chloride of zinc with the mercury and filings, and then washing with water, that the plug retained a purity of color and beauty which was at once surprising and gratifying. Dr. G. requested him to experiment in this direction. He (Dr. F.) had obtained equally satisfactory results, but finding the difficulty of manipulating so as to leave the fingers, instruments, etc. free from the chloride of zinc, he had tested Labarraque's solution (Liq. sodae chlo.) with the same results. This fluid being objectionable on account of its odor, he had tried chloride of sodium (common salt) and still with equal effect. This being agreeable, cleanly, and thus far free from any objection, he continued using it as he had been doing for eighteen months. He had, but a few hours previous, presented quite a number of plugs of from one to eighteen months duration, for the inspection of several of his professional friends, to prove that thus far they alike remained as bright as when first introduced, and preserved the teth in which they were inserted without the slightest particle of discoloration.
He described the method of preparation to be as follows: Into a small-sized wedgewood mortar he placed a quantity of mercury about equal in size to the cavity he was about to fill, then added three or four times that bulk of the ordinary Townsend's filings, and next, about twice the bulk of both mercury and filings, of chloride of sodium. These he rubbed well together until he obtained a dark, gray powder; to this he added a few drops of water, and then, upon further rubbing, obtained a very dark, almost black, paste; this he washed freely by pouring water upon it and mulling once or twice until the amalgam, which was now formed, presented a beautifully clean appearance; he then squeezed the mass in buckskin with plyers, rather more forcibly than was usual in preparing ordinary amalgam. This made the material too hard to work, but by holding it in the hand a few seconds, it was gradually softened sufficiently to introduce, after being properly and thoroughly manipulated, into the cavity; he allowed it to remain comparatively unfinished about fifteen minutes (sometimes more) until it was somewhat hard, and then smoothed it carefully with a burnisher; finally, arming a pair of thumb forceps with a piece of spunk, such as is used for drying cavities, he rubbed the plug evenly toward the edge of the cavity; this left an unburnished surface, which was allowed to remain. ln this condition the plug hardened, assuming the appearance of "frosted silver", maintaining its integrity, and upon the articulating faces of molar teeth doing better service than anything except the very best gold plugs, and equaling even these, as far as six years proving could testify.
He does not use amalgam, from choice, in any teeth except molars, as thus far he has been unable to insure against discoloration in the bicuspids and anterior teeth. Remarked that the discoloration of amalgam was superficial, and that it was oftentimes possible to restore the beauty of a tooth by simply removing the amalgam plug and excavating the darkened portion of dentine which it had been in contiguity with. He used the amalgam sometimes in lower bicuspids which were much decayed, and which it was desirable to retain for the purpose of occlusion with upper natural or artificial teeth to aid in mastication. These sometimes became discolored and sometimes retained their color, but as yet his observations had not disclosed the reason for this.
In conclusion, he stated that in comparing amalgam with gold for filling such cavities as he had indicated, especially when they were of large size, he thought the argument was decidedly in favor of amalgam; for while it saved teeth as permaneotly as the very best gold plugs, it was introduced with much less of disagreeable manipulation, less irritation, less consumption of time, less expense, and was so nearly the color of the tooth as to be scarcely noticeable. If these were not arguments in its favor to the minds of some, his own opinion was based upon them, and years of experience had, as yet, only served to strengthen it.
Dr. Fitch had recently subjected amalgam washed with alcohol to a microscopic test, and found the crystalline structure exceedingly close and compact. He expected to find the minute particles of silver coated with free mercury, but was disappointed. The crystals were very fine and the structure was apparently homogeneous.
Considered that the manipulation, suggested by Dr. Flagg, in the use of chloride of sodium, simply removed the oxides present or rendered them soluble and left the metals pure; for if chlorine was in this process liberated, we should have more or less of the chlorides of the different metals entering into the amalgam. But there is no chlorine set free. It cannot be due to any bleaching process, for we should have more or less coloration produced in the formation of the chlorides. The only way to test this matter would be to subject this highly colored saline solution, derived from the trituration and washing of the amalgam with chloride of sodium and water, to a strict chemical analysis, and this would show apparently the residuum, if not the process, of its removal from the amalgam.
Dr. McQuillen suggested that the discoloration of amalgam fillings was due to the formation of sulphurets rather than oxides of silver. In illustration of this, referred to the tarnishing of silver, exposed to the atmosphere, which chemists account for by attributing it to the affinity existing between the sulphur in the atmosphere and the silver; and, agan, to the blacking of silver spoons when used in eating eggs, which, like all albuminious food, containing a large proportion of sulphur.
As this discoloration was due to the affinities existing between elementary substances, he could not see how washing the amalgam in any way could destroy that affinity. It was, without doubt advisable that the material should be as free from discoloration as possible before introducing it into the tooth, and according to the plan described this evening, it can be made to resemble frosted silver. He had reason to believe, however, that the absence of discoloration in fillings that have been in some time, was more apparent than real. The surface exposed may be kept bright by the friction it is sujected to in mastication, but that which is in contact with the purietes of the cavity would, if exposed, be found to present a blackened appearance. This may be so slight that it would not affect the appearance of a tooth where the walls were thick, but if they were thin, it would be quite evident. He did not wish to be understood, in offering these views, as objecting to the method advocated, for he believed it to be a good one, and worthy of a fair trial.
Dr. Garretson was not prepared to discard the chloride of zinc as a material for cleansing the amalgam, even with the objections mentioned by Dr. Flagg; on the other hand, preferred it to the chloride of sodium, and would ask members to give both a fair trial.
He uses a drop or two of the chloride in the amalgam and then washes the mixture, and the result will he a beautiful silver-colored material. In using amalgam, is guided by his judgment alone, and not by auy fear of what the profession will say.
EDITORIAL
The Dental Cosmos vol IV Jan 1863 312-13
J.D. White
AMALGAM
It was my intention never to have said anything more on the snbject of amalgam, but at the urgent solicitation of some of my friends I am disposed to make an article on the subject. I do not wish to be understood as complaining about its use, but merely reporting matter upon the subject so that those who employ it may have some means of judging when and why it may produce unfavorable and unsatisfactory resuIts. I operated for an intelligent gentleman a few days since who had a number of his back teeth plugged with amalgam many years ago; the work seemed to do very well but his dentist left the city, and for other operations be came into my hands. I discovered that the teeth which had been plugged with the amalgam were decaying under and around the plugs; it is not unfrequent to see this the case, while the plug remains apparently firm in the tooth, that decay is going on around and below the plugs.
I removed all the amalgam and plugged with gold but the teeth were mere shells. I filled the roots well; the teeth are breaking and mouldering away but not decaying. He remarked to me a few days since that if he had not had the amalgam put in his teeth when they were first plugged he would have had a good set of back teeth, as he had lost a great deal of the strength of the teeth between the time of plugging with amalgam and the plugging with gold; besides, during the time that the amalgam was in his teeth he had suffered constantly with sore throat and sometimes it ran into ulcerations; he has been entirely free from every such difficulty ever since the amalgam has been removed. He said be knew of a great many patients of the same operator who had been injured by its use.
A case occurred a few years since of a young man about twenty years of age, of delicate temperament, a student at Yale College but a resident of this city, and son of a distinguished physician. He had a very large cavity plugged in the left inferior-first molar nerve dead- by an eminent dentist of our city. On a visit home from college, in the absence of his dentist he called to consult me about his teeth generally. I observed this large plug, and inquired if he had ever suffered any inconvenience from it; he answered he had not. I saw that the submaxillary gland of that side was very much enlarged, and remarked to him that in all probabilIty it was caused by the amalgam plug, and advised him to consult his father about it; he did so, but his father said he did not think there was any connection between the two, or that the amalgam plug caused the enlargement of the gland. He went back to college and returned in a few months when he called upon me again and I observed that he had a bad case of ranula; I advised him again to say to his father that it was probable that the case was due to the amalgam plug.
His father called in an eminent medical friend in consultation and they came to the conclusion that the plug had nothing to do with the case. He returned to college but the case grew so much worse that he went to New York to consult a surgeon, who told him that he must get the tooth extracted, that it was the amalgam which caused the disease; he came on to this city, had it extracted; he then returned to New York, the surgeon performed the usual operation for ranula, and the case recovered.
About two years since an intelligent lady called to see me from Norristown, Montgomery County, under a great state of excitement, to get some amalgam plugs removed from her teeth. She had lost a sister, the wife of a medical man, at Wahegan, Illinois, by salivation from two amalgam plugs; the plugs had been removed when it was found that she was under the influence of ptyalism but it did not arrest the progress of the case, and she died as it was believed, solely from that cause. I report this case to put those who use amalgam on their guard, and that when it unusually impress a patient in any way it ought to be removed as the prolonged action of mercury, however small in quantity, impresses some temperaments very strangely. At my request Prof. W. J. Taylor some time since made an analysis of the amalgam ready prepared for plugging and of plugs which had been taken from teeth after they had been worn for some time to determine whether it was probable that any mercury was lost while a plug was in a tooth; his communication will answer for itself.
***
I have made approximative analyses of the amalgam plugs and the freshly prepared amalgam ready for use, which you sent to me. The following are the results: I first selected a plug which had the appearance of having been considerably acted upon. Whether this appearance was owing to a partial decomposition I cannot say positively; were the same appearance in a mineral, I should not hesitate so to attribute it. The weight of it in grammes was 0.3973. I found that in this there was 37.5 per cent of mercury still in combination with the silver. I next selected a larger and fresher looking plug, which did not exhibit the same kind of surface, being without that appearance of partial decomposition such as I observed in the plug first examined. This weighted 0.9445 grammes, which contained about 55.43 per cent of mercury.
Now, whether this variation of composition in these two plugs is owing to loss of mercury after the plug was in the mouth, is a question which others are better able to decide. The great difficulty is in even obtaining an original composition for the amalgam; some may be made with a less quantity of mercury and a greater quantity of silver while others may have a composition exactly the reverse.
W.J. Taylor
POISONED BY MERCURY FROM A TOOTH FILLING
The Dental Register, XXVI, 1872, 47 8
The following. from a Nebraska paper, shows that the "amalgam quustion" receives some attention in the West: "Last Wednesday evening the intelligence was noised about that Mr. John C. Smith, a middle-aged man, unmarried, who lived in a small house next west of the residence of S.W. Allen, was dead. It was known in town that be had been suffering for some days with a swelled face and neck, coming from a tooth, which Dr. Keef, of Marysville, had lately filled, but his death was not thought possible. Dr. Sprague attended the deceased at first, but afterwards called Drs. Davis and
Buffon, all of whom agreed that he was suffering from the effects of mercury, present in the amalgam used in filling one of his teeth. The filling had salivated the unfortunate man, and as the inside of his mouth, throat and windpipe swelled, respiration was hindered, and it finally ceased altogether.
"Poultices were applied, and other means used to reduce the swelling, but all to no purpose. Mr
Smith died about 7 o'clock Wednesday evening.
"By request of a number of the citizens, Coroner Buchanan next day ordered a post mortem examination to be made of the remains and an inquest to be held. Dr. Davis made the examination, opening the chest and taking out the lung, and also extracting the filled tooth. No signs of any other disease were found except that caused by the mercury, and it was made clear to the jury by the
Doctor that this caused the death.
"The jury was composed of the following persons: L.Y. Coffin, C. F. Buchanan, Joseph Saunders,
James Charles, W.J. Dunn, 0.M. Enlow.
"S.W. Allen testified that Mr. S. had asked him to see a dentist for him; that Mr. S. afterwards told him that he had been to see Dr. Keef, who had filled the tooth: that he had filled it without killing the nerve, and that he (Smith) thought the dentist was intoxicated when he did the work.
"Drs. Spraguc and Buffin both testified that they believed the deceased came to his death from the effects of the mercury used in the filling of the tooth.
"In accordance with the facts elicited, the jury returned a verdict that the decased came to his death by suffocation, caused by inflammation of the glands and infiltration of the tissues of the neck, producing closure of the trachea by prcssure thereon; and we further believe that the above causes were brought about by the action of mercury, used in the filling of the second molar tooth of the right of the lower jaw, by Dr. E. D. Keef, of Marysville, Kansas.
Payne J Poisoning from corrosive sublimate generated in the mouth from amalgam plugs in the teeth The Dental Cosmos XVI 1874 213-4
(reprinted from Chicago Medical Journal)
Having been invited by an eminent gentleman of the medical profession to attend a convention of the State Medical Society to submit to its consideration a matter of vital importance to the human family, and being unable to comply with the invitation, I have written this article to lay the matter before the medical profession and ask its co-operation.
The matter which I wished to bring to the notice of the profession is the poisoning of thousands of people all over the world from corrosive sublimate generated in the mouth from amalgam plugs in the teeth.
Neither Asiatic cholera, nor smallpox, nor any malarious disease, is doing half the mischief in the world that is being done by this poisoning. Every medical man of any considerable practice has undoubtedly had numerous cases of it, but never knew what it was. The symptoms are so numerous and varied in different cases that it would be impossible to give them all in this short article, but I will say that a person poisoned in this way is liable to be treated for dyspepsia, neuralgia, paralysis, consumption, and numerous throat-diseases. The patient gradually wastes away as if going into a decline, and no medicine will afford any relief. In many cases the difficulty steals on so gently as not to excite the least alarm, and continues very gradually for a number of years till the patient becomes a total wreck; while in others the attack comes on violently, and the friends and attending physician think the patient is dying; but he will again rally, and again be prostrated.
There is such a resemblance in the symptoms to nearly all the diseases to which human flesh is heir that the physician is led to treat the patient for some disease which seems to be a very clear case, but his patient gets worse. In more than twenty cases that I have had, nearly all had been pronounced by some physician as having consumption. In nearly all the cases there are at times a very bad cough, eyes sunken, and haggard expression and deep blue or dark color under the eyes, invariably a metallic taste in the mouth, water flowing from the mouth in the night while asleep so as to wet the pillow, and in most cases extreme prostration.
I have not time now to detail the manner in which the corrosive sublimate is formed in the mouth, further than to say that the quicksilver in the plugs is driven off by the heat of the mouth in very minute particles, and, combining with the chlorine in the fluids of the mouth, or any saline substance, such as our food, passes into the stomach, and produces slow poisoning. If the State
Medical Society will appoint a committee to visit this place, I will show them several cases that place the matter beyond controversy.
There are some twelve thousand dentists in the United States doing a wholesale business at this poisoning, and I ask the co- operation of the State Medical Society, as guardians of the public health, to assist in getting an act of Congress passed making it a penitentiary offense to place any poisonous substance in teeth that will injure the people.
PROCEEDINGS OF DENTAL SOCIETIES. NEW YORK
ODONTOLOGlOAL SOClETY.
The Dental Cosmos XVII, 1875, 236-257
This society held a special meeting December 14th, 15th, and 16th, 1874. By arrangement, the usual routine business was omitted, and the sessions were devoted to the reading of papers and the discussion of professional and scientific matters.
Tuesday morning the secretary read a paper by S.P. Cutler, M.D., D.D.S., of Memphis, Tennessee, entitled "Amalgam Experiments." The author had made and described in detail the results of various experiments with silver, tin, platinum, brass, copper, gold, nickel, cadmium, etc., with a view to ascertain what metals, and in what proportion, make the best alloy. The following extracts show his conclusions:
"Filings of platinum and mercury rubbed together in the palm of the hand do not amalgamate readily, not even if moistened with alcohol; they do not form a metallic mass at all, but remain in the form of a dark powder. There appears to be no affinity between the two.
"I combined platinum with silver and tin in small proportion, and found that just in proportion to the amount of platinum was the amalgamation retarded, and just in proportion to the variation of the relative amount of platinum to the other ingredients, was the process of amalgamation varied. So long as there was any platinum present, so long, was the process retarded.
"The next experiment was with platinum and gold, one equivalent of platinum and two of gold; amalgamation was very slow, requiring considerable rubbing. After the lapse of two weeks, it was not firm, but was easily picked to pieces with the finger nail; in fact, it did not harden to any extent."
"Copper filings, rubbed with mercury do not easily amalgamate"; moistening with alcohol facilitates the process; it makes a white mass, but does not harden at all.
"Brass filings, after considerable rubbing, amalgamate slowly, but quicker than copper, owing to the zinc in the brass. This specimen did not harden in the least.
"Nickel does not unite with mercury after long rubbing, hence could be of no use in amalgams.
"Cadmium, combined with common amalgam, would only injure the preparation, from the fact of its readiness to oxidize in the mouth, forming a soluble oxide, which would endanger the pulp of the tooth. Amalgam of this metal has been used by some in the profession, the consequences being destructive to the tooth, or teeth, so far as they have come under my own observation."
"Now, in relation to amalgam and its place in rank, as a filling, I unhesitatingly place it next to gold for permanent use ; many would, no doubt give tin-foil the preference.
Permit me to make a statement. Take any mouth, or any number of mouths, with decayed teeth in every and all stages of decay, and let any first class operator fill all decayed teeth on one side of the mouth with gold. and all on the other side with best quality of amalgam, say all back of cuspids, the same skill and care being used in both; then turn loose the patient and await results.
"In my opinion, based upon observation, the side of the mouth filled with amalgam; in ten or twenty years, will be found to be ia a better condition than the other. Why this prejudice against the mercury, which is the demon in amalgam?
"Why is there so little prejudice against rubber plates, which contain mercury and make mouths more or less tender and sore in a majority of cases? ....
"When an excess of mercury is used in amalgam, it always comes to the surface, and an unequal plug is the result; moreover, the tendency to contract, or assume the spheroidal shape, is very largely increased. Mr. G.H. Makins, Lecturer on Metallurgy in the London School of Dental Surgery, well states the case as follows:
"Amalgams, as a rule, are compounded of a metal with mercury, which compound is further dissolved in an excess of mercury; and although, when subjected to pressure, this excess is largely squeezed out, as in larger ore operations for gold or silver separating, yet it is very difficult to do this to such an extent that no free mercury is retained. And, indeed, by much the same action as when one squeczes a sponge containing a fluid, you get the mercury forced to the whole surface, and thus, in your operations, what is so forced between the sides of the cavity and the plug, by slow and gradual vapor exhalation, is liable to leave a minute interspace."
"For when too much has once been added, any pressure to which we can subject it with the chamois skin and plyers will fail to remove all the excess. The best results will only be obtained with a very much less amount than will remain after any attempt to remove the surplus by pressure.
"The use of only a proper amount of mercury precludes the washing of the amalgam. With whom the idea of washing amalgams originated I am unable to say; but it seems to be practiced to a large extent. Many of the manufacturers recommend it. If they had taken the trouhie to properly test plugs made of amalgam which had been washed, they would have been less ready to advice it.
"If only the proper quantity of mercury is used in making the amalgam, there is but a very small amount of oxides present, and consequently less necessity exists for their removal. By an excess of mercury we get just what the washing is designed to remove.
"Even if it were possible to remove all the excess of mercury after washing, the amalgam would still contain more or less water, which can only be removed after much trouble.
"Tests made by Mr. Fletcher witb amalgam plugs containing an excess of mercury, and with amalgam which had been washed, gave the following results, viz.:
"The plugs mixed with an excess of mercury are distinctly more imperfect, and have a decidely greater shrinkage in every case. The proportion of mercury left in after thorough compression with powerful plyers is ahout double what is necessary to make a good amalgam, and the excess of nercury cannot be squeezed out without making the amalgam so hard as to be unworkable; also, in packing, tbe mercury comes to the surface of the filling, making an unequal alloy. As regards washing, when once wet, I have never in any single case been able to get the amalgam properly dry without an amount of trouble such as would not be taken by ninety nine operators out of a hundred, and the water works to the face in packing. Several plugs put in smooth parallel tubes, with an amalgam which had been washed, slipped out after hardening, on the slightest force being applied.
With amalgams which had not been washed, this was most decidedly never the case under any possible circumstances with amalgams of moderate shrinkage. ...
With regard to amalgam, viewed in the light of these researches, I have almost come to the conclusion that wherever we can make a perfect amalgam filling we can make a perfect gold filling.
There are a thousand little things that defeat us in the operation; mercury working to the surface, not only the outer surface under our pluggers, but the surface between the filling and the tooth. Mercury going there leaves a film, which, being afterwards reabeorbed into the filling, leaves a space or crevice.
Again, in reference to washing or wetting; it is next to impossible to get water out, if it once gets into amalgam. We think, perhaps, we can hurry up matters, and if there is a little moisture round the edge of a filling, it is no great matter, we can pack until we squeeze it out; but we cannot do it.
There are many difficult places about the mouth where we cannot use amalgam and be sure of the best results, simply because it is impossible to keep the tooth dry. In these cases we cannot make perfect amalgam fillings, no matter how good the amalgam may be. Hence, If a moisture-tight plug he essential to the preservation of the tooth, we may about as well attempt to use gold as amalgam.
...
The action in relation to amalgam, so far as the American Society of Dental Surgeons was concerned, commenced in 1841, and reached its height in 1847, when several of its members were expelled because they would not sign a pledge not to use it in their practice. Dr. Parmly was, at that time, the president of that society, and a large majority of its members took sides with him against its use; and the subject occupied the time and attention of that body, almost to the exclusion of any other business, for several years. The debates in relation to it were at length carried on with a great degree of feeling. Those opposed to it being in the majority, were determined that the society should be purged of those members who would not take sides with them against it, and many members resigned rather than be subjected to such discipline; while others stood up and fought against such action on principle, although they did not want to use it, and were eventually expelled from membership.
The result of this action on the part of the majority was most unfortunate. Men who had been friends for years became bitter enemies, and the usefulness of the society was at an end. And yet I believe now, from what I have known of those who so arrayed themselves against the use of amalgam, that they were entirely honest in what they said and did in this matter, and that they truly believed their action was for the best interest of their profession. ...
Dr. A.H. Brockway. I am under lasting obligation, as every one present must also be, to those gentlemen who have submitted papers on this occasion. I think the value of them can scarcely be overestimated, for they have given us information that we greatly needed.
There has been an impression in the community, which has been shared largely by the proression, that amalgam was a dangerous article to use; I was so taught by my preceptor, the late Dr. Westcott, and for many years refused to use it, but I have done so occasionally for the past fifteen years, and I never yet have seen a case of injury produced by it. I never have seen a case of mischief in the mouth which has been attributed to amalgam that would not have been produced by the use of any other material used in the same way. We must bear in mind that amalgam has not had as fair a test as other materials, in that it has, as a rule, been used only in the most difficult and doubtful cases. And here I wish to dissent from the statement which has been made, that where amalgam can be used gold might be used about as well. The semi-plastic quality of amalgam and the manner of its working are such as to permit its use in many cases where it would be impossible to make a good gold filling, or, if not impossible so extremely difficult as to render it unwise to subject the patient to the necessary fatigue and expense for what must, in the nature of things. be at best but a doubtful operation.
But there are some operators who use amalgam occasionally in simple cavities, on the score of economy, either of time or material; this I think is a mistake, because gold or tin foil can in such cases be as easily used, and, as amalgam is objectionable on account of the color, it is decidedly better to use gold.
THE CHEMISTRY AND PHYSIOLOGICAL ACTION OF
MERCURY AS USED IN AMALGAM FILLINGS.
BY E.S. TALBOT, M.D., D.D.S., OF CHICAGO
OHIO STATE JOURNAL OF DENTAL SCIENCE. Vol. II. JANUARY 1, 1882. No. 1.
"A word fitly spoken is like apples of gold" -Solomon
(Read before the Illinois State Dental Society, held at Rock Island, May 10, 1881)
The name Mercury was given by the ancients in honor of Mercurius, the messenger of the gods, whose volatile character mercury is supposed to typify. It is seldom found in the native state, but is usually combined. The most important as well as the most abundant combination is the sulphide of mercury, or cinnabar. It is found united with silver, forming an amalgam. The largest and richest mines are found in California. The process of obtaining pure mercury from the sulphide is very simple. Tbe ore is mixed with one-half its weight of lime and then distilled in iron retorts. The mercury is extracted and the lime remainns in the retort. It is a heavy fluid metal, odorless, tasteless, of a whitish color, and when free from other metals it does not tarnish, and its globules roll freely over white paper without leaving a streak or losing their form. It is liquid at ordinary temperatures. It boils at 662° F., and solidifies at -40o F. into a malleable mass of octahedral crystals. It is volatile at all temperatures, evaporation being much accelerated by the application of heat. The symbol is Hg, atomic weight 200. Mercury combines with other elements and radicals in two proportions. Those compounds in which the lesser acidulous radicals are united are termed mercurous. The higher mercuric - thus, calomel (HgCl) is mercurous chloride; while corrosive sublimate (HgCl2) is mercuric chloride. Mercury combines with chlorine, iodine, bromine, lead, oxygen, phosphorous, sulphur, arsenic, bismuth etc., forming compounds, some of which are used medicinally. The metal itself, rubbed up in confection of roses, licorice or suet until globules are not visible to the unaided eye, is used in medicine.
Amalgams were introduced into this country as filligs for decayed teeth in 1833. Since that time unlimited discussion has arisen among the general practitioners of medicine as well as the dentists, in regard to the practicability of utilizing this material in dentistry. The first amalgams were composed of pure silver and mercury, manufactured by M. Taveau. Later, Dr. Evans combined pure tin with a small quantity of cadmium, and Dr. Townsend formed an amalgam with four parts of silver to five parts of tin. Following these compositions came numerous others made from gold, silver, platinum and tin, until today we have more than a hundred varieties in the market, varying slightly in metals and proportions, that each manufacturer may rightly claim an original preparation.
These different metals are melted in a crucible in their proper proportions by weight, and poured into ingots. These are filed or cut into minute particles, ready for use. When the cavity in the tooth is prepared, a sufficient quantity of filings is rubbed up with mercury into a paste, the surplus mercury squeezed out, and the filling is inserted into the tooth.
From its first application as a filling, the better class of dental practitioners waged war against it on general principles; not alone on account of the deleterious effects of the mercury in its composition, but because of its unsightly appearance and demoralizing effects upon the dental profession. The manner in which it was introduced into the country called forth the censure of all having a regard for professional etiquette: "Two adventurers, without skill or any claim to the title of dentist, suddenly appeared in New York and began dental practice amid such a shower of advertisments, a profusion of display, and a metaphorical flourish of trumpets, as caused our staid and dignified dental ancestry to bound with surprise and indignation." (History of American Dentistry). From that time onward the use of amalgam has increased, until now tons are consumed yearly in filling teeth. Dr. Harris, in his opening address to the first class of the Baltimore College of Dental Surgery, in 1840, says: "It is one of the most objectionable articles for filling teeth that can be employed, and yet from the wonderful virtues ascribed to this pernicious compound by those wvho used it, thousands were induced to try its efficacy."
At the meetings of the dental societies this subject was spiritedly discussed with strong arguments against its use. The first official act in the matter was the appointment in 1841 of a committee by the
American Society of Dental Surgeons to report on the use of lithodeon - mineral paste, and all other substances of which mercury is an ingredient, for stopping teeth. They reported in substance that the use of all such articles was hurtful - to the teeth and every part of the mouth, and that there was no tooth in which caries in it could be arrested and the organ rendered serviceable by being filled, in which gold could not be employed. This report was unanimously adopted. (American Journal of
Dental science).
At a meeting of the same society July 20, 1843, the use of amalgams was declared to be malpractice, and a committee appointed to further investigate the subject. They referred the matter to the Medical
Society of the County of Onondaga, New York. The report of the medical committee was to the effect that no care in the combination or use of the paste will prevent its occasional bad effects. In
1845, the Mississippi Valley Association of Dental Surgeons resolved that the use of amalgam fillings was unprofessional and injurious, and would not be countenanced by its members. The actions of the various societies had very little effect; amalgam forced its way into the offices of the majority of dentists in the country. Many excellent practitioners were expelled, and others resgned from the societies to which they belonged. In 1850, a resolution was passed unanimously by the
American Society of Dental Surgeons to rescind the pledge made by the same society previously.
Thus ended the so-called amalgam war. It will be observed that no scientific researches were made to ascertain whether deleterious effects were produced by mercury; the chief object of the disturbance was, apparently, to rid the profession of charlatans and their obnoxious materials. These
These discussions, which have caused so much bitterness and enmity among the members of societies, have latterly aroused a feeling of enquiry into the scientific analysis of this filling for teeth, resulting in the discovery of a quality in its composition capable of producing salivation, and all other symptoms of poisoning. Many able practitioners of dentistry have experimented with all the different acids with no satisfactory results. When we consider that nitric acid dissolves mercury only when heated; concentrated sulphuric acid dissolves mercury only when heated; hydrochloric acid does not affect it at all - how can we expect the weaker acids of the mouth, diluted by saliva, to cause a chemical change?
If past experiments have proved unsatisfactory, it does not discourage me in the attempt to discover, if possible, by experiment and by the careful study of the subject of mercury in its every particular, some clue to this perplexing question. Having satisfied myself that the poisonous effects are not produced by the chemical changes in the mouth, I have entirely ignored this theory, and have looked about for a more simple and direct cause. In commenting upon mercurial poisoning, the idea has been advanced that the vaporization of mercury takes place only during the hardening process, and, that being consummated so quickly, no deleterious effects can occur.
In the construction of an amalgam two changes take place, the first being the mechanical, or mixing together of the ingredients, the second the chemical, or hardening of the composition. My first experiment was to place metallic mercury in a four ounce glass-stoppered bottle, and submit it to the gold test, by suspending a piece of gold foil in the centre of the bottle, taking care that it did not
come in contact with the sides, and cementing the stopperr. I placced it under different temperatures, of from 20 to 130° F. In about thirty-six hours the surface of the gold became coated with mercury, giving it a gray color. This proved the evaporation of the metal. I then mixed a quantity of the
Chicago Refining Co.'s amalgam, according to their formula, three parts of mercury to eight parts of filings, and subjected it to the same test. The reagent was not sufficiently delicate to produce any perceptible change. Wishing to bring the highest chemical skill to bear upon the experiments, I consulted Prof. Haines, of Rush Medical College, who kindly assisted me. At his suggestion, I procured two delicate reagents, the ammonio-nitrate of silver, and the chloride of platinum. In preparing the ammonio-nitrate of silver, I allowed thirty grains of nitrate of silver to the ounce of water, and put a small quantity of the solution in the test tube. This was heated, and aqua ammonia added until a precipitate formed. Increasing the aqua ammonia until the precipitate cleared up, I took a quill and, with this liquid wrote upon white paper. After putting the substance to be tested in the bottle, the strip of paper was placed across the mouth of the bottle, and the stopper cemented.
Should a vapor arise, the liquid would become black. Leaving the bottle for ten minutes, I examined it again, and found the writing in plain black coloring. The chloride of platinum produced the same results, but required more time to accomplish it. The rapidity with which the evaporation of mercury takes place depends upon the amount of heat and the surface exposed, and not upon the quantity of mercury contained in the fillings. Thus a jar containing one quart of water would evaporate the same quantity as a jar of like surface containing a gallon, the latter taking four times longer to empty.
In the following experiments, I attached a thermometer to a water bath, and heated to the temperature of the body, 98° to 100° F., to maintain an even temperature. I conducted these experiments in the dark, as the rays of light decompose the ammonio-nitrate of silver. The strips of paper containing the reagent were placed in the mouths of all the bottles, including an empty bottle, which was used in each experiment, to prove there was no mistatke.
Experiment No. 2 -Three bottles were prepared. In the first was placed an amalgam filling made from Chicago Refining Company's amalgam, according to their formula. In the second was placed an amalgam filling of the like size, containing five grains more of mercury. In the third bottle there was nothting. After a lapse of ten minutes I examined the bottles and found the writing on the paper across the mouth of bottles Nos. 1 and 2 was black, while there was no discoloration of paper in the third bottle.
Experiment No. 3 - A repetition of No. 2, with the exception of the reagent chloride of platinum being substituted for the ammonio-nitrate of silver. The results were the same in both. The time required for the latter being ten hours, while but ten minutes were required for the ammonio-nitrate of silver. In conducting the remainder of the experiments the ammonio-nitrate of silver was employed, it being the more delicate reagent, consequently producing a more marked impression, and also consuming less time than chloride of platinum.
Experiment No. 4 - Two bottles were prepared. In the first bottle were placed Scraps of amalgam six months old. In the second there was nothing. In ten minutes the writing on the paper was black in the first bottle, and uncolored in the second.
Experiment No. 5 - Bottle No. 1 contained amalgam fillings which had remained in the teeth from two to ten years. BottIe No. 2 was empty. The resuIts in both being the same as in experiment No. 4.
Experiment No. 6 - In bottle No. 1 I put an amalgam filling which had been in the mouth sixteen years. In bottle No. 2 there was nothing. At the end of twenty-four hours I found the paper discolored in the first, and not in the second.
Experiment No. 7 - To demonstrate that nothing in the composition of the fresh fillings could cause the discoloration I allowed some fillings to remain sealed in the bottle for twenty-four hours. At the end of that time discovered no signs of color on the paper.
Experiment No. 8 - I procured four preparations of mercurious vivus.
No. 1 contained 1/10 gr. mercury to 1 gr. of sugar of milk.
No. 2 " 1/100 " "
No. 3 " 1/1000 " "
No. 6 " 1/1000000 " "
A small quantity of each of these preparations was placed in bottles marked 1, 2, 3, 4. In No. 5 there was nothing save the reagent. The effect was alike in each of the four bottles containing the mixture.
Those having the greatest quantity of mercury caused the deepest color to the paper and required less time. As before, No. 5 was unaffected.
In order to determine the difference, if any, in weight after evaporation, I obtained strong glass tubes one-half inch in length, and one-fourth inch in diameter, and packed them carefully with amalgam fillings. Allowing twenty-four hours for hardening, I wighted them, and at the end of three months I again weighted them, finding in some no change at all, and in others an increase of weight. This is accounted for by the fact that oxydation and accumulation of moisture on the amalgam equaled in some and exceeded in others the loss of weight by evaporation. I am in possession of numberless cases of poisoning from mercury in amalgam fillings. I will mention but one, and report one case from my practice.
The Dental Register, January, 1872, has the following case of poisoning from mercury in a tooth filling: "John T. Smith died from salivation, caused from having a tooth filled with amalgam. Dr.
Sprague attended the case, and afterwards called Drs. Davis and Buffin, all of whom agreed that he was suffering from the effects of mercury present in the amalgam used in filling one of his teeth. The filling had salivated the unfortunate man, and, as the inside of his mouth, throat and windpipe swelled, respiration was hindered, and finally ceased altogether. Dr. Davis made the post-mortem examination in the presence of the coroner and jury of inquest, opening the chest, taking out the lungs, and extracting the filled tooth. No signs of any other diseases were found, except that caused by the mercury, and it was made clear to the jury by the Doctor that this caused his death. The jury returned a verdict that the deceased came to his death by suffocation, caused by inflammation of the glands and infiltration of the tissues of the neck, producing closing of the trachea by pressure thereon; "and we further believe that the above causes were brought about by the action of mercury, used in filling the second molar tooth of the right side of the lower jaw, by Dr. E. D. Keef,
Marysville, Kansas."
A case in practice: A lady from one of the towns in Illinois came to Chicago for treatment, having been troubled with dyspepsia and nervous debility for two years. While under the physicians care she complained constantly of a peculiar feeling and taste in her mouth. The doctor suspected the trouble might arise from a rubber plate which she had worn for four years, and advised her to consult me. Upon examination, I found a full upper plate, composed of of rubber, and on the lower jaw the molars were gone, except the second and third upon the left side. In the crown of the wisdom tooth was a large amalgam filling, and also one in the crown and posterior approximal surface extending to the free margin of the gum in the second molar: These had been inserted about two years previous. I noticed that the gums and the mucous lining of the mouth and salivary glands were quite
tender. There was a strong metallic taste in the mouth, and a metallic odor to the breath. She had a peculiar paralyzed sensation in the left side of the tongue which she had experienced for two years.
She also informed me that the saliva flowed so freely that at night her clothing and pillow were saturated, and estimated the loss of saliva each night to equal one pint. I suggested the removal of the amalgam fillings and the rubber plate, and substitution of gold. She assented to the proposition, and as early as possible I undertook the operations. Upon removing the amalgam fillings and applying the rubber dam, the saliva flowed in streams, completely saturating several towels. After refilling the teeth, and inserting a gold plate, the unpleasant sensation in the tongue and metallic taste disappeared. At the end of two weeks the glands were greatly improved, and the soreness under the tongue (of which she had complained at her first visit) was healed. lt is the accepted opinion of physicians generally, that mercury uncombined has no constitutional effect. Dr. Atkinson said before the meeting of the American Dental Association in Boston, August,
1880: "You must comoine the molecules of mercury with some other agent before they can have any affinity for the body at all. One who is familiar with the old method of making looking-glasses, with tin foil and mercury, knows that the workman would be literally satturated with it, so that he could not be capable of handling a gold or silver watch without its becoming amalgamated, and all this, too, without his health being compromised by the mercury so long as it remains in a metallic state."
The correctness of this theory may be questioned as it has been proven that these workmen have been affected by the vapor of mercury, when not protected by a veil over the mouth and the nose.
Dr. Bartholow, in his work on Therapeutics, p. 177, says: "As used in the mechanical arts, by gilders and others, the fumes of mercury cause wasting, ptyalism, necrosis of bones, trembling, impaired intellect, and, in women, abortion." "Walter Pope mentions a workman who for six months had not handled mercury; yet he rendered a piece of copper as white as silver by rubbing it between his fingers." Parish says that long trituration of calomel increases its power to salivate. This is also applicable to all preparations of mercury used with an excipient, medicinally. The homeopaths divide and subdivide particles, according to the required preparations, some of the radical members of the school claiming best results from the highest potencies, while the more conservative practitioners prefer a middle ground. They rub up pure mercury with sugar of milk into six different grades, the first containing one-tenth gr. of mercury to one gr. sugar of milk; the second, one onehundredth gr. mercury to one gr. sugar of milk, etc., as before mentioned in this paper. These are the finest forms in which mercury is prescribed, and yet the severest cases of salivation and constitutional symptonms have been produced by these agents, on account of their being so readily taken up by the blood. Is it not a reasonable supposition that, if poisonous symptoms are produced in proportion with the subdivision of the particles of mercury, that the system will be more severely affected by the vapor of mercury, which is finer than any mechanical subdivision can be? Dr.
Somers recalls an instance of a lady patient becoming completely salivated, the gums and mucous linings of the mouth inflamed and teeth loosened, by taking a second bath, in which forty grains of the black oxide of mercury were used. He thinks she could not have absorbed one-twentieth of the amount in the form of vapor.
As a forcible illustration, I quote the experience of the sailors on board the man-of-war "Triumph," which, in April, 1810, took from the wreck of a Spanish ship thirty tons of quicksilver, contained in bags of fifty pounds each. In the course of a fortnight some of the bags decayed and burst, the quicksilver mixing with the bilge water, the emanations from which coated all the metal about the ship.
Nearly all the crew were salivated.
In order to ascertain the effect of the vapor of mercury, I have employed it in a series of experiments upon plants and animals.
Experiment No. 1 - While conducting my experiments in the laboratory I was frequently visited by a family of roaches, who appeared to take interest in my operations. Suddenly they all disappeared, and it immediatedly suggested itself to my mind that their sudden departure argued favorably in the question of utilizing them in my experiments.
I took four two-ounce bottles and put in No. 1 pure mercury; No. 2 amalgam scraps six months old;
No. 3 fillings from two to ten years old; No. 4 fillings sixteen years old. After placing a roach in each bottle, I tied a piece of cloth over the mouth in order that the air might circulate. Evidently the bugs were not fond of mercury, for they clung to the tops of the bottles as long as life lasted. Roach in No 1, containing pure mercury, died in three days; roach in No. 2 was next to follow; roach in No.
3 lived a few days longer; and in No. 4 outlived them all by several days.
Experiment No. 2. - I prepared three bottles. The No. 1 contained ten grains of pure mercury; No. 2 contained an amalgam filling three months old; No. 3 was an empty bottle. In each of the bottles I put two roaches. In two days one in the bottle containing pure mercury died; the remaining one in the same bottle lived nine days from the time it was put in. In the bottle containing the amalgam filling one roach died in four days, while the other one died in eleven days; while those in the empty bottle lived fifteen and sixteen days.
Experiment No. 3 - On February 9th I placed an amalgam filling at the base of a sensitive plant. On examination, about the fourth day, I discovered that the extremities of the leaves had changed color and were dry and brittle, like the leaves in early Autumn; gradually the whole leaf was affected, and at the end of ten days the plant was dead, notwithstanding the care and nourishment it received.
Experiment No. 4 - In a four-quart glass jar I put about four ounces of mercury, and made a platform of wire gauze, fastening it two inches from the bottom of the jar. I placed a Guinea pig in the jar, and covered the top with gauze. Twice each day I removed him for exercise and nourishment. He thrived well for ten days, but at the end of that time he commenced to droop, and refused food and water. He became emaciated and trembling; the body and limbs were cold. He lingered along for two weeks and died.
Experiment No. 5 - I administered six grains of mercurius vivus, first trituration, to a dog with his supper, and repeated the dose next morning with hios breakfast. The blood and liver were examined under the microscope in the evening and found to contain globules of mercury.
It is the opinion of many eminent scientists that mercury inhaled into the lungs produces a greater effect than when taken into the stomach. Among this number Prof. Stille in his Therapeutics, Vol. 2, page 789, says: "Of the several modes hy which mercury is made to enter the body, inhalation most speedily produces the specific influence of the medicine." Claude Bernard, late Professor in "Le
College de France," makes the same statement in one of his lectures. This is readily understood when we consider that the drug taken into the lungs in the form of vapor is distributed over a large surface and brought in direct contact with oxygenated blood, and thus carried directly to all parts of the body.
Mercury taken into the system in small quantities, long continued, manifests itself in a variety of ways. One of the first symptoms noticeable is an increased flow of the secretions of the body - salivation being the most striking - the glands becoming inflamedand the mucous membranes tender.
The gums tumefy and change in color to a dark rose tint; the tongue is swollen; the patient not only experiences an unpleasant metallic taste, but the breath becomes impregnated also. Sometimes extensive ulcers attack the throat, gums and cheeks; aedema of the glottis, with difficulty in breathing and swallowing. The digestive apparatus is involved, with loss of appetite, nausea and vomiting, and frequently pain and tenderness of the stomach; the bowels loose, and often bloody stools. The fatty constituents are removed, aud the patient becomes emaciated; no part of the body is more affected by mercury than the nervous system; the body trembles; sometimes one limb, and again both limbs contract. A sense of coldness and occasional chills are experienced; often neuralgic pains are felt, particularly around the motor nerves; mental debility and loss of memory. These are some of the many symptoms caused by the inhalation of thc vapor of mercury.
RESUME'
There are in the market many varieties of amalgams. Evaporation does not depend upon quality or age, but all amalgams will send off the vapor of mercury. This has been proved conclusively by its destruction of animal and vegetable life, and by chemical tests. Evaporation is facilitated by an increase of surface, consequently a greater amount of vapor would arise from several small fillings than from one large filling. The facility with which mercury is taken into the lungs by continued inhalations and the rapidity with which it enters the blood, requires less mercury to produce systemic effects than when taken into the stomach. In order to produce systemic effects from metalllc mercury, it must be rubbed up with an excipient, to reduce the particles to a size capable of entering the capillary system, or it must be taken iuto the lungs in the form of vapor.
***********
Editorial; Ohio State Jornal of Dental Science
THE AMALGAM QUESTION AGAIN.
Though we find little or nothing that is new in Dr. Talbot's article on this subject, we still consider it timely and appropriate. That mercury vaporizes at common temperatures is so well known by men of science that it seems like a waste of time to prove it, as does Dr. Talbot, yet his experiments are instructive and profitable; for only a few years ago, prominent and active members of our profession were claiming that mercury vaporizes only at 662° and upward, that being its boiling point. They might with equal propriety, set up the claim that water does not evaporate below 212°; and then it would be hard to account for the drying of the ground after a shower.
That the vapor of mercury is poisonous is beyond dispute. No one can know it much better than the writer, who has been repeatedly poisoned thus when redeeming mercury from its oxides-once till the tongue protruded beyond the teeth for several days. It matters not practically whether or not this vapor must be combined with another element in order to work its mischief; for the other elenients, oxygen, chlorine, sulphur, etc., are ready to pounce upon it at the earliest opportunity.
But, after all, it is not probable that the vaporization of the mercury of amalgam fillings in the teeth is the only or even the chief source of poisoning; for every close observer will recognize the fact that patients in whose mouths the soluble chlorides abound, other things being equal, suffer most, while those who stink with sulphuretted hydrogen suffer least. The worst cases of poisoning we have witnessed are those in which the amalgams retatin their original bright color; and in these, whenever tested, we have found mercuric chloride, or corrosive sublimate. The bright surfaces, it is true, are favorable to the vaporization of the mercury, and the two sources of poisoning acting together are able to cause the most serious disaster. This brings to mind a case which we have had opportunity to watch since 1868. At that date the family physician of Mr. H. brought him to our office for consultation. He was suffering from profuse ptyalism.
All the salivary glands and his tongue were much swollen. The mercurial fetor was sickening, and so intense that it was noticed on the stairway by parties who followed him to the office. He was suffering from tremor mercurialis, and complained of a nearly universal aching of bones. His physician diagnosed mercurial disease; but his patient persisted that he had never taken mercury in any form. He had not been sick before; and the family physician, till now, had been an eclectic, who discarded mercury.
As the man owned but six hundred acres of land, and it was worth only a hundred dollars an acre, and he had nine or ten teeth to fill, he could not afford gold, and he had amalgam put in, but not in our office. The teeth had been filled some weeks before we saw the case. We told the physician the composition of the amalgam plugs, and he at once urged their removal, but the poor man could not afford it. The physician abandoned the case in disgust. The poor man has endured years of agony, but has, in the last few years, had most of the amalgam taken out. He is gradually improving. A few years ago we treated him to a mild course of iodide of potassium, which had to be frequent]y interrupted on account of a return of ptyalism. He was a giant in development and strength; but is now a broken-down, prematurely old man.
Before we had turned our attention toward dental surgery, we had a case of paralysis agitans. The patient was a young lady of eighteen years. She continued to grow worse under our treatment, till becoming desperate, we began a more thorough investigation. Looking carefully into the mouth we found a mass of blackness. There was no dentist accessible, so we went to gunsmith shop, made two or three excavators, and by a series of operations, we removed seventeen large and small amalgam fillings from her mouth. She recovered rapidly without other treatment. She had suffered from ptyalism at an earlier stage of the case, and before coming under our care.
This case had baffled the leading physicians of the community, ans we doubt not it is a type of numerous cases having the same etiology. Not that even recognized mercurial poisoning often manifests the form of tremor; but when we know that amalgam is used in filling teeth to the extent of tons each year, we should not be surprised at the great prevalence of nervous diseases. Physicians should wake up to the importance of this subject; for it is evident that many obscure diseases especially of the nervous and glandular systems, originate from this source. In the case Mr. H. of the six hundred acres, the family physician referred to, and we are all of many physicians who suspected the influence of mercury, and yet he got better only in proportion to the removal of the mercury. And not only is his own constitution ruined, but, though he has a healthy wife, his offspring are puny, neuralgic - in short, total failures.
Some strange thoughts found utterance in the discussion of Dr. Talbot's paper. One thought there could be no danger of mercurialization from rubbing mercury in the hands, because the particles are not sufficiently minute to be absorbed till the metal is vaporized. But the particles of mercury are as small when it is liquid as when it is vapor; and, space for space, more of its particles are in contact with the skin. And all who read ought to be familiar with Scheele's case, detailed by Pereira and others, in which a small quantity of mercury in a leathern bag, left hanging against the breast produced fatal merurial poisoning.
It is very fortunate, in view of the fact that so much amalgam is used, that sulphuretted hydrogen is present in so many breaths, and cyanide of sulphur in the saliva of so many patients. In either case
the mercury is sulphidized, and as the sulphide is less soluble than the oxides or chlorides of the metal, bad results are less likely to follow. In a mouth destitute of the compounds of sulphur, the chloride, (corrosive sublimate) is more likely to be formed than either of the oxides of mercury, when amalgam fillings are inserted. It requires but a small amalgam filling to contain twenty grains of mereury, which, if chloridized, will yield twenty-three grains of corrosive sublimate. Were this formed suddenly in the mouth, of course the consequences would prove promptly fatal, yet it is the very slowness of introduction that insures those fearful results sometimes seen in consequence of the administration of mercury, and which are acknowledged and detailed as minutely by its friends as by its enemies, as in the celebrated fatal case of Scheele already alluded to. Some persons are much more readily poisoned by mercury than others. We have seen severe ptyalism caused by a single three grain pill of blue mass; and we killed a little girl of twelve years by the administration of six grains of calomel, even though followed by an infusion of senna, so as to induce early and prompt purgation. And when a dentist uses amalgam, he never knows but that he is inserting it into the mouth of one of those patients so easily poisoned with mercury, unless he has previously found by experiment that the reverse is true.
We do not hope to see the use of amaIgam fillings abandoned. They come too handy for feeble men and lazy men; and, oh! the poor quacks! Like Micah, in the book of Judges, they would cry with an exceedingly bitter wail, "Ye have taken my gods, and what have I more?" But, just in proportion as the profession make attainments in chemistry and pathology, will be the decline in the use of amalgam.
We shall close as we began, stating that the paper of Dr. Talbot is both conclusive and timely. When associated with Professor J. Taft we tried all these experiments, substantially, more than a quarter of a century ago, and they were to us so conclusive that we declined then, as we had done before, to use amalgam fillings, and notwithstanding slanderous statements to the contrary, we have declined ever since, and neither of us has ever found occasion to use, and neither has used amalgam fillings in practice.
This late discussion of amalgam shows how little close thought exists on the subject. They talk of the way Dr. Townsend made his amalgam when they ought to remember that Dr. T. didn't make it, and always so stated, telling all the while that he got the formula and the amalgam from Dr. Wm.
Hunter, of Cincinnati.
THE AMALGAM QUESTION.
J.FOSTER FLAGG, D.D.S.
The Dental Cosmos Vol XXIV 1882 237-242; 313-318;364-370
That two such remarkable papers as the leader and editorial of the Ohio Sate Journal of Dental
Science for January, I882, should have been seriously presented for the consideration of dentists is, to say the least, surprising; but when it is recognized that, in the face of an accumulation of facts which have proved so irresistible as to have practically swept away all the enunciations antagonistic to the filling-material known as amalgam, the antiquated blasts of forty years ago are repeated, what must we think of it? It is retrograde metamorphosis, surely!
The "leader" is a paper by Dr. Talbot, of Chicago, and is a statement of a line of work to prove that mercury is "volatile at all temperatures" - a position which, I believe, is not disputed - together with a series of experiments, which rival the celebrated work of Prof. Westcott, with diluted acids, which were accredited with the power to cause dental caries, because they "softened the enamel so that it could be scraped off with the finger-nail!"
The experiments really do not bear as much actual relation to the filling of teeth as did these strange expositions to the decay of the teeth.
The paper opens with the old garbled statements in regard to the early doings about amalgam.
It is noteworthy that it seems impossible for the opponents of amalgam to make other than unfair and partial statement of these things, and this, too, when it is so easy for anyone to see that this is so.
The advocates of amalgam, in giving the history of these matters, tell "the truth, the whole truth, and nothing but the truth." Its opponents reiterate statements which were made, and which are now known to be false, and, taking parts of statements which favor their views, leave out that which is damaging even to destruction.
It is stated that, from the first, "the better class of dentists waged war against it" -amalgam- "on general principles" The present condition of things would seem to render it a matter of doubt as to whether the warriors were entitled to the distinction of "better", if so, it seems a pity that the "better" men should have been so badly beaten!
It is quoted from the "History of American Dentistry" that the performance of the adventurous introducers of amalgam "caused our staid and dignified dental ancestry to bound with surprise and indignation," when the truth of the matter is that the filling and saving of hundreds of teeth which had been pronounced by the "staid and dignified" as impossible to fill and unworthy to save was the real cause of the bounding!
The next sentence in the paper speaks volumes. "From that time onward the use of amalgam has increased, until now tons are consumed yearly in filling teeth." A hundred such papers as Dr. Talbot s would only weigh as the dust in the balance against this one overwhelming fact.
It is then given as the report of the committee of 1841 that "there was no tooth in which caries in it could be arrested and the organ rendered serviceable by being filled, in which gold could not be employed. This report was unanimously adopted." Such statements as this, given without comment, are used to shed their portion of the general air of condemnation to amalgam which pervades the paper - and this, too, with the knowledge that thousands of excellent dentists, together with a large majority of the best informed, most skillful, and most successful practitioners of the present day. know and assert that this position is absurdly fallacious, and that the fact of the "unanimous" adoption of such a report is simply a sad commentary upon the foolish ignorance and prejudice of those days.
The report of the Medical Committee of the County of Onondaga, New York, is spoken of; and it is stated that "the report of the Medical Committee was to the effect that no care in the combination or use of the paste will prevent its occasional bad effects."
In the midst of the excessive luminosity which medicine has shed upon dental effort, this work of the
Onondaga gentlemen stands preeminent! No mention is made of the fact that amalgam was given to this committee as a mineral compound - that it was received as such, and reported upon as such in these words: "That the mineral paste has produced, in many instances, the peculiar effects of mercury, though in different degrees of intensity - in some slight, in others severe and alarming - there can be no doubt. The committee believe that the proportion of such cases is small, compared with the whole number operated upon, but that no care in the combintion or use of the paste will prevent its occasional bad effects."
This report truly reminds us of some of the reports of committees, and discussions thereupon, more nearly connected with our speciality than is the Onondaga effort. They are reporting upon an exclusively metallic compound, and call it a "mineral paste." This compound has always been
"combined" and "used" in but one manner and in but one way - whether it is soft or hard, plastic or powdery, washed or unwashed, it is practically the same combination, and is practically "used" the same. But of all these things the Onondagaians were uninformed. It might then be pertinently questioned, What business had they to "believe?"
The summing up of this portion of the paper is a reference to the resolution of the American Society of Dental Surgeons to rescind the "amalgam pledge," a pledge not to use any amalgam, which enforced expulsion of all members refusing to sign it, and under which a number were expelled, and it is stated in the paper, "Thus ended the amalgam war." No mention is made of the little closing paragraph of the rescinding resolution; that disgraceful avowal; that stench in the nostrils of all honest men, which gave to dental history the statement that the ama]gam pledge was rescinded because "the resolutions had accomplished the object for which they were designed, and there no longer existed any necessity for their enforcement." Who would be found fighting for a cause which required such abominations for its support?
Next follows in the paper a series of experiments which may possess some value as indicative of a deviation from the beaten tracks of the advocates of gold foil in experimentation, and as possibly demonstrative of an eventual emergence into the light of the broad scientific surroundings of the advocates of amalgam.
These seem conclusively to re-prove a position which has been so well proved that, as Prof. Watt very appropriately remarks, "it seems like a waste of time" to have done it. And yet so important was it thought to be that this undisputed fact should be incontestably established that the "highest chemical skill" was brought to bear upon the experiments."
Among the many who may justly be regarded as eminent authority in matters pertaining to chemical research, it seems invidious to designate anyone as preeminently superior, but it is well to know, in
view of possible future experimentation in behalf of dental chemistry, that the highest skill is to be found at Rush Medical College, of Chicago.
But must it not have been amusing to one so erudite, that his immense resources should have been enlisted in a work so palpably unworthy of such gigantic grasp!
If good reasons for doubt as to the truth of the position that mercury vaporizes at ordinary temperatures had been thought to have been discovered, then, indeed, high authority might well have been consulted as to the value of the reasoning, but for the further proving of the accepted fact additional authority seems as little requisite as it would be to prove that the earth is spheroidal, or that it makes diurnal revolutions.
After the disposal of this vaporization of mercury, then begin the wonders of the paper. Such a peculiar line of work (?) and such very peculiar deductions therefrom, such attempts to prove a theorizing which "all the rest of mankind" know has no foundation in facts, is wonderful, almost beyond comprehension, and certainly extraordinary beyond parallel.
The first case given is that of John T. Smith, rather an equivocal name, but who is reported as having died a vastly more equivocal death. John Smith had a lower molar filled with amalgam; a subsequent swelling occurred, which, by its magnitude and extent, hindered respiration. Finally respiration ceased altogether and, as a consequence, the "unfortunate man" died. It was made clear to the jury by the attending doctor that the mercury in the amalgam filling caused the death.
First Query. - If the jury had been composed of well-educated dentists, is it probable that "the doctor" could have made the same thing clear to them?
Second Query. - Would it not be in order that the several hundred John Smiths who have had lower molars filled with amalgam, and whose respiration has not yet been "hindered" should be called upon to offer "rebutting testimony?"
The next case is that of a lady who suffered "debility," "dyspepsia," "paralyzed sensation in the tongue," "strong metallic taste", "metallic odor to breath," "free flow of saliva" - estimated at a pint each night - "together with tenderness of gums and salivary glands." The patient wore a piece of rubber work and had two amalgam fillings. Upon the removal of the fillings, and the substitution of gold work for rubber, all unpleasant symptoms passed away and the soreness of the tongue was healed.
I had a case which was sufficiently similar to this one to be a "parallel" - the symptoms were as like as those of one patient could be to those of another; the difference was only in length of time, my case being more acute. The whole trouble was caused by a gold plate! - even a coin gold was tried, but it was proven to "vaporize" too much. The peculiar "coppery" taste and odor of mercurial ptyalism were too apparent to admit of a doubt as to the gold being the cause! he plate was abandoned, and the patient promptly recovered.
A "forcible illustration" of the effects of vapor of mercury is given in the paper as having occurred on board the man of war "Triumph." This seems rather a mal-a-propos name for a man-of-war fighting as an opponent of amalgam, as the neccessity for renaming the ship "Defeat" is too inevitable, but "nearly all the crew were salivated" from the vapor arising from only thirty tons of quicksilver!
As it would seem proper that I should have a ship story, I would direct attention to the no less
"forcible illustration" of the marked benefit arising from exposure to mercurial vapor which will be found recorded in "Ziemssen's Cyclopaedia of Practical Medicine," Vol. I., p. 512 "The efficacy of prophylactic medicine is very doubtful, although quinine is highly recommended for this purpose by
Cummings, and mercury by Walker, of Jamaica.
"The latter gained its reputation through a peculiar incident. On the occasion of the capture of Fort
Omra, the yellow fever broke out among the land forecs as well as on the fleet, and decimated the men. One of the captured ships was struck by a shot in such a way that the quicksiler with which it was loaded ran out of the vessels containing it. The sailors who were ordered to gather up the valuable cargo did so, using their bare hands; and all who were employed in this way during their stay in that region remained perfectly well, although surrounded by sickness and death." (La Roche, loc. cit. Vol. II., p. 762.)
But now we come to the serious portion of the conflict. In order to ascertain the effect of vapor of mercury, it was en employed in a series of experiments upon living things, and the first suggestin, which is impressed, if it proves to be successful, is a boon, indeed, to infested humanity. It almost rivals the boon of amalgam itself as a filling material.
This suggestion is the employment of mercury as an anti-roach remedy. Its vapor is supposed to have caused the sudden disappearance of roaches from the experimenter's laboratory, and if this supposition should be verified by experiment, from the domestic standpoint the knowledge thus imparted would be of incalculably more value to man - or, at least, to woman - than have been all the thirty dollar gold-fillings that have ever been inserted.
The apparent antagonism existing between cock-roaches and mercurial vapor having been noticed, these insects were placed in bottles, which were either empty or contained mercury or amalgam filings. in every case the cock-roaches died much sooner when exposed to mercurial vapor than when placed in empty bottles. Ergo, amalgam is not a good material with which to fill teeth.
A guinea pig was put in a four-quart jar with four ounces of mercury; he was taken out twice a day for exercise and nourishment; he lingered for two weeks, became emaciated and trembling, and finally died. Ergo, amalgam is not a good material with which to fill teeth.
An amalgam filling was placed at the base of a sensitive plant; in four days the extremities of the leaves were dry and brittle, and at the end of ten days, notwithstanding care and nourishment, the plant died.
These are certainly curious and interesting results from the entomological, the zoological, and the botanical aspect; but recognizing little similarity between cock-roaches and guinea- pigs, and the patients for whom I operate, and yet, perceiving some little analogy between the most delicate among them and the sensitive plant, while I cannot accept the ergo in any case, epecially in view of
FACTS established by an experience of twenty-five years using of amalgam as a filling material, I would nevertheless call attention to the results of an experiment which has now stood the test of nearly four successive years.
In the year 1879 a favorite cat died. It was placed at the "base" of an unpromising Concord grapevine, which has since been plentifully supplied with manure water. The result is gratifying in the extreme; luxuriant growth has been attained, with bountiful return of fruit, which, though grown on Concord stem, has a delicious Catawba flavor; nothing could be finer or more satisfactory. Ergo,
dead cat, either soft or cohesive, is a good material with which to fill teeth; and, for the assuring of continuously satisfatory results, the mouth should be rinsed frequently with manure-water.
It now remains for us to inquire into the object of such papers as that of Dr. Talbot and such editorials as that of Prof. Watt, and the "ways and means" by which this object is sought to be attained.
For twenty or thirty years past dentistry has been divided into two factions, the one, a large one, claiming prominence, and indeed preeminence, upon the ground of a demonstration of superior manipulative skill. To be an "elegant filler of teeth with gold was to be an eminent" dentist. This position has its peculiar strength, and certainly is entitled to all it deserves, but another faction, a smaller, and a constantly growing one, has been restless under this jeweler-like presentation of a profession which they believed, under broader view, held at its bestowal an untold amount of relief to suffering humanity. As I have said, and as is well known, the opponents to the according of
"eminence" to mere manipulation are now so numerous that the "balance of power" is beginning to be a question of much moment, and it can therefore be only in the interest of the weakening cause that such efforts are made.
Why must thls he so? It must be so because at the earliest date of inquiry into the plain question of the "saving of teeth" it was at once recognized that the opinion of the committee of 1841, as to the possibility of filling with gold all teeth that were capable of being rendered serviceable in any way or by any material, was the most unmitigated nonsense, for there were then monuments of nearly ten years duration in the shape of "hopeless," "worthless" teeth saved by amalgam. Thus it was shown that teeth could be saved by amalgam which even the "most eminent" manipulators could not save with gold. It was this fact which placed amalgam solidly as the antagonist of gold; it was this fact which has made those who have rested their claim to "eminence" upon their ability to work gold fear amalgam. They have affected to despise it, but no one who truly despises a thing heaps upon it constant invective; nothing which is despised is persistently defamed and decried; nothing which is despised is maligned and abused intolerantly. All this has been done and is yet done to amalgam, and the result is that "the use of amalgam has increased until now tons are consumed yearly in filling teeth!" It is well worth the strongest effort of the antagonists to amalgam that this tidal wave should be stayed in its progress, for it truly threatens their annihilation!
That gold will be "abandoned" as a fllling-material is not and never has been the idea of the advocates of amalgam, but that it is unwisely and disadvantageously used, even yet, with all the marked modification which is now manifest, is the opinion of the advocates of amalgam. Why is this antagonism especially against amalgam? It is because no other filling-material possesses the resistant characteristics which pertain to amalgam - nothing else can compete with gold - nothing else can successfully compare with gold - nothing else can do, as amalgam can, MORE than gold! This is why the narratives of "debility," "dyspepsia, "ptyalism," "paraIysis, and "broken-down, prematurely old men" are periodically dispensed at society meetings and in the dental journals. If it were not for this, cock-roaches, guinea-pigs, and sensitive plants would live on in peace and quiet.
Who ever heard of such calumniation of gutta-percha? - even of red base-plate full of the sulphuret of mercury! It is promptly eaten out from articulating cavities; it cannot restore contour to teeth; and therefore, although in protected cavities in soft teeth it has repeatedly outlasted the best gold efforts of the best gold-workers, it is quietly alluded to as a "temporary material." Who ever heard of such calumniation of oxychloride of zinc? Nay, more, who does not know of the wholesale acceptance and laudation of this wonderful (!) filling-material? So easy to mix; so easy to introduce; so easy to finish; so like the teeth in color! so desirable in every way; so fortunate a possession in cases of frail teeth!
Was it the "feeble" men, who said all this? Was it the "lazy" men, who periodically discussed this boon to humanity? Was it the "poor quacks," who were so well satisfied with the "Diamond" and the
"Adamant" cements? Diamond! Adamant! Names which none but the most unscrupulous would affix to such evanescent compounds - materials which no worker of amalgam would ever indorse.
And yet, the strong men, the energetic men, the skillful manipulators, the hard workers, the eminent men, the reputable practitioners, all who hated amalgam and who worshipped gold, have cried out with a loud voice, "Great is oxychloride of zinc!" So also has it been with the oxyphosphates and the nitrophosphates, and, judging from precedents, we have the right to assume that it would ever be so with any and all materials which truly could not compete with gold.
None such as these have ever been denounced as "demoralizing" to the profession; the use of materials such as these has never been regarded as "degrading" even by the "most respectable." They have been "plastered" in far more like plastering than has been amalgam, but the term "plasterers" has never been thought applicable, much less appropriate, for bestowal upon these "elegant operators." They have never for a moment thought of regarding the use of such materials as infringing, even distantly, upon the domain of gold, or as in the least degree comparing with it in value, beauty, or permanence. Gold-work has had no fear of such competition, and experience has proved that if it had had, all such fears would have been utterly groundless.
With amalgam all is different; it has been found to be a compound singularly adapted to the requirements. It is easy to mix, as much so as the zinc plastics; it is easy to introduce, as much so as the zinc plastics; it is easy to finish, as much so as the zinc plastics - and so far, reasoning from analogy, all would be well. But now come serious difficulties! It can not only be introduced with facility, without the necessity for rubber-dam infliction, without the consumption of very much time, without the pain and irritation incident to prolonged malleting or hand- pressure, without the subsequent tedious and disagreeable filing, pumicing, tape-finishing, and burnishing (all of which might still be well enough), but, unfortunately, it is very durable, very tooth-saving, and, worst of all, not very expensive. From these three considerations, it is very "demoralizing!"
A few trials of amalgam by those, who have vainly expended a vast amount of patience, strength, and skill, in years of honest, faithful endeavor to save soft, sensitive teeth with gold, give results which force the experimenters to indulge in serious thinking as to their duty towards those who place themselves in their professional keeping.
A few trials of amalgam by those who have given time, endurance, and money, without stint, to that which has proved a series of unsuccessful experiments in the endeavor to stay the ravages of caries and the frequent loss of teeth, shows them, so conclusively, the folly of continuing in the old way, that amid satisfaction, contentment, and outspoken joy at the demonstration of prospective comfort, they indulge in sarcastic comments, upon the elegant efforts of "eminents," and cover with bitter invectives the memory of the useless torture and the wasted time and money which has, until now, been their ideal of dentistry!
It is strange, indeed, but no less strange than true, that all the power which the acknowledged
"leaders" in the dental profession could bring to bear for the prevention of a fair, open, honorable, and unbiased trial of amalgam has been essayed. Sneers as to incapacity on the part of men who were daily saving just such teeth as the scoffers were extracting have been liberally indulged in by those whose highest dental ability was that of sticking gold together piece by piece. lnvidious
comments, refusal of recognition, denial of respectability, and absolute proscription, are the weapons which have been used against such as arrogated to themselves the right to try experiments which seemed to promise comfort, satisfaction and reasonably permanent tooth-salvation, even in most desperate cases!
It seems hard to credit this; it might seem harder yet to give a reason for it; but that it has been so is indisputable.
And for patients, that they might not indulge, it has been deemed advisably professional that fearful tales of dyspepsia, nervous prostration, mercurial ptyalism, and paralysis should be related to them, ad nauseam!
What is the result of all this powerful, systematic, official antagonism? What is the result of all these horrible bug-bear narrations? I will take the answer to these questions fom Dr. Talbot's paper: "The use of amalgam has increased until now tons are consumed yearly in filling teeth!"
Dr. Talbot quotes Professor Chapin A. Harris, who in his opening address to the first class of the
Baltimore College of Dental Surgery in 1840 said of amalgam, "It is one of the most objectionable articles for filling teeth that can be employed, and yet, from the wonderful virtues ascribed to this pernicious compound by those who used it, thousands were induced to try its efficacy."
And now, after forty years of additional experience, what is the result of this earnest, faithful, scientific teaching?
It has proven so eminently objectionable and so diabolically pernicious that, at first, the thousands who were induced to try its efficacy were only able to induce some tens of thousands to accept the benefits of its "wonderful virtues," but, as years rolled on, and the solidity of Prof. Harris's teachings became more incontestably established, the recipients of the benefit to be derived from this "most objectionable" and "pernicious" compound came to be counted by the hundreds of thousands!
By this time, as might reasonably have been expected, the cases of nervous prostration, mercurial ptyalism, paralysis, and death, had become so alarmingly numerous and so well authenticated that millions have rushed forward to immolate themselves before this dental Juggernaut, and "tons of amalgam are now consumed yearly in filling teeth!"
And now, in truth, who has seen all, or any, of the direful sequences which have been ascribed to this "objectionable," "pernicious" compound?
Dr. Talbot states that he is "in possession of numberless cases of poisoning from mercury in amalgam fillings."
To old experimenters, experienced observers, and statisticians this seems, at first, a peculiarly loose and unscientific statement, but, upon slight reflection, it becomes far less unreasonable, for, if Dr.
Talbot had been posessed of only 1000 cases - a very large number for any one record - it would have been easy to have so stated it, and the cases would have been by no means "numberless." If he had been informed of 100 cases, that rceord would have been larger, by far, than any other observer has collected, and ought to have been regarded with favor - and yet a hundred would have been even less "numberless." It is hardly to be assumed that he would have regarded 10 cases as "numberless," and we are therefore left with only 0 cases, which may, with perfect propriety, be regarded as
"numberless," and which, indeed, is the only number of cases which any statistician could accept as
"numberless."
From this stand-point I, too, can say that after an experience of twenty five years extended use of amalgam fillings I am in possession ofjust exactly "0" cases of complicated mercurial, dyspeptic, ptyalistic poisoning or paralysis and " 0" cases even of death from mercury in any form.
From analogy we might reason that a like experience with mine at the hands of several thousand dental practitioners may have had something to do with the increase of the use of amalgam, for it is hardly fair to assume that so large a proportion of the members of so progressive a profession as dentistry has proved itself to be, ought to be ranked as "feeble, lazy quacks."
When the sewing-machine was invented it was inveighed against most bitterly as ruinous to the poor women and injurious to the rich purchasers, but as year after year developed the truth in regard to them the sale and the utilization of them increased "until now tons of them are consumed yearly" in response to the demand.
When coal-oil was offered as an illuminator, ruin was proclaimed alike for whalers, lard-oil makers, and camphene manufacturers, and it was held up in holy horror as dangerous to limb and life, and as not even a good material with which to kindle fires! But truth developed "until now tons of it are consumed yearly" in response to such varied demands in the behests of comfort that it has come to be one of the largest interests.
Even "envelopes" - so mild and placid in their exterior and general physical characteristics - were antagonized as detrimental to prosperity and "ruinous" to seal-makers and sealing-wax manufacturers, but the former and the latter alike continue their elegant and useful occupations, while the sale of envelopes has steadily increased "until now tons are consumed yearly" in their manifest aid to celerity and comfort in the routine of social and business duties.
So has it been with amalgam, as year by year it has defiantly, and with greater solidity, put under foot the vague assumptions and false assertions of its antagonists. Steadily has it maintained its onward and upward march, vindicating its capabilities, asserting its claims, and demonstrating its merits "until now tons are consumed yearly in filling teeth," and imbecility, laziness and quackery labor with increasing cheerfulness in the Christian like work of comfortably and satisfactorily saving the human teeth.
But, peculiar as are the thoughts which are engendered by perusal of Dr. Tatlbot's paper, those which are suggested by a conjoined study of it and the editorial upon it by Professor Watt are, naturally, doubly so.
The very first proposition of this powerful, industrious, scientific editorial suggests thoughts which are at least twice as peculiar as any suggested by the perusal of Dr. Talbot's paper aIone. The editorial commences, "Though we find little or nothing that is new in Dr. Talbot's article on this subject, we still consider it timely and appropriate." Now, why is it "timely and appropriate?" Is it because articles which do contain some little that is new are generally regarded as untimely and inappropriate to dental literature? Or, is it that the propositions, though old and hackneyed, are worthy, from their weight and importance, of being always regarded as "timely and appropriate?"
This can hardly be so, for Professor Watt, after stating, in defiance of authority, that "the vapor of mercury" (without any reference as to quantity) "is poisonous beyond dispute," also states, in the
next paragraph, that, "after all, it is not probable that the vaporization of the mercury of amalgam fillings in the teeth is the only or even the chief source of poisoning."
If this is so, why should a paper the whole power of which is expended to prove that this
"vaporization" is the "more direct and simple cause" of all the trouble (?) be regarded as in any way
"timely and appropriate?"
Again, Professor Watt says that the vaporization of mercury at common temperature is "so well known by men of science that it seems like a waste of time to prove it, as does Dr. Talbot, yet his experiments are instructive and profitable."
How are they "instructive," if all that they prove was well known before? And how are they
"profitable," if they tend to give chief prominence to a cause which is "probably" not the chief cause?
Professor Watt says the experiments of Dr. Talbot are "instructive and profitable, for only a few years ago prominent and active members of our profession were claiming that mercury vaporizes only at 622° and upward, that being its boiling point." Now, this seems to prove inaccuracy and ignorance among "prominent and active members" at that time, raither than the possibility of anything instructive or profitable being derived from Dr. Talbot's paper at the present time, for it would be markedly discreditable if any of the "prominent and active" were to advance such doctrines at this late date. For these reasons I cannot see that Dr. Talbot's paper can properly be regarded as either "timely" or "appropriate" and I most certainly cannot find that it is possessed of any points which can be regarded as, in the least degree, "instructive" or "profitable." The next participants in
Professor Watt's parade are a series of horriblyl disgusting swollen tongues and glands, universal aching of bones, suffering from tremor mercurialis, years of agony, and one broke- down, prmaturely-old giant. These are found in company with a female case of paralysis agitans, aged eighteen years, from which, through the intervention of some gunsmith-shop excavators, no less than seventeen amaIgam fillings were removed.
The broken-down giant's case was a very sad one, for, although he had a healthy wife, his offspring are "puny, neuralgic, total failures," showing how very much more powerful for evil to posterity are
"nine or ten" amalgam fllling than is one healty woman powerful for good; and yet, the paraysis agitans result must be viewed as one of the mostt favorable among the direful possibilities of amalgam, for, we are informed, in her mouth was "found a mass of blackness," while we are told that where this "blackness" exists "bad results are less likely to follow." On the other hand, it is stated, editorially, that "the worst cases of poisoning we have witnessed are those in which the amalgams retain their bright color;" so it may be possible that the dark cloud of the broken-down giant's case had this "silver lining."
It is nothing less than amusing to follow the reasoning (?) by which chemically fearful results are imaginatively produced by amalgam fillings. In some mouths it is said that "the mercury is sulphidized," and in such cases "bad results are less likely to follow." In other mouths "the chloride
(corrosive sublimate) is more likely to be formed when amalgam fillings are inserted;" and then we are gravely and innocently informed that "it requires but a small amalgam filling to contain twenty grains of mercury, which, if chloridized, will yield twenty-three grains of corrosive sublimate."
Now I ask, seriously, is there a more absurd proposition than this on reeord for the thoughtful consideration of the members of the dental profession? I ask that it shall be remembered that this statement is made by one who has long been regarded as a teacher, who occupies an editorial chair, and who is, professedly, a dental chemist. "If chloridized!" - I should say if chloridized! But suppose that it is chloridized, what becomes of the amalgam filling? And suppose that the amalgam filling remains, practically, as it is introduced, and the mercury continues as mercury and only
"vaporizes," while, "after all, it is not probable that the vaporization of the mercury of amalgam fillings in the teeth is the only or even the chief source of poisoning," what then? It seems to me that it becomes a matter of little moment, so far as amalgam fillings are concerned, whether twenty grains" of mercury would make twenty-three grains or two hundred and twenty-three grains of corrosive sublimate, so long as the eorrosive sublimate is not made. "If chloridized," indeed!
And what does Dr. Talbot say of this loss of mercury even by evaporation? He says that he made amalgam fillings and weighted them, and after three months he weighted them again, "finding in some no change at all, and in others an increase of weight;" he tben continues, "This is accounted for by the fact that oxidation and accumulation of moisture on the amalgam equalled in some and exceeded in others the loss of weight by evaporation." The explanation may be or may not be entirely satisfactory, but the fact remains, and in relation to that I would say that, so far as those who have had the most extensive experience in amalgam-work are able to observe, the condition of amalgam fillings in the direction of change in which Dr. Talbot's experiments of weighing would be of any value would remain practically the same at the end of three months, three years, or thirty years, for the condition, relative quantity and effect of the mercury in an amalgam filling are regarded as having been proved to be always the same. It is from this fact that different proportions of mercury and alloy are combined for the specific purpose of making a softer or a harder filling of amalgam, and the desired softness or hardness is a condition which is found to be equally in existence, whether the filling is examined a few months or many years after its insertion.
The only noticeable change which ever occurs is actual loss of amalgam from attrition, and even this result is remarkably trivial in comparison with what might be expected; and this, too, in fillings composed of an unduly large proportion of mercury, and, in consequence, unnecessarily soft.
In this loss of amalgam both mercury and alloy metals are naturally lost in the proportions of amalgamation, and it cannot, with any reason, be supposed that vaporization chloridizing have any especial connection with the loss of the mercury.
We now reach a portion of this remarkable editorial at whieh it becomes a serious question as to how it shall be regarded; I refer to the naive narration of advanced infanticide, or child- murder, contained in the following brief but striking paragraph:
"Some persons are much more readily poisoned by mercury than others. We have seen severe ptyalism caused by a single three- grain pill of blue mass, and we killed a little girl of twelve years by the administration of six grains of calomel, even though foIlowed by an infusion of senna so as to induce early and prompt purgation."
As with Dr. Talbot and his cockroaches and guinea-pigs, so it is with Professor Watt and his blue mass and calomel and from this dire mishap in his practice of medicine he deduces the inexplicable, irrelevant, and illogical conclusion that, ergo! amalgam is not a good material with which to fill teeth! Truly, this line of argument could only be equalled by assuming that the pilula ferri carbonalis must be an exceedingly dangerous medicament because a man would probably die if struck fairly in the abdomen by the iron ball shot from a cannon!
It is only another illustration of the usual appearance of things presented to those eyes which for "a quarter of a century" have been kept persistently at the "big end."
Professor Watt does "not hope to see the use of amalgam fillings abandoned." I regard that as very fortunate, for it certainly would be a "forlorn hope", indeed, if he did hope it; but after another slur at the "feeble-minded," "lazy men" and "poor quacks," following which charitable epithets is, very appropriately, a quotation from Holy Scripture, he concludes the paragraph thus: "But just in proportion as the profession makes attainments in chemistry and pathology will be the decline in the use of amalgams."
What shall I say to this? Can it be possible that dental chemistry and dental pathology have so ignominiously retrograded that in fifty years the consumption of amalgam has increased several thousandfold, "until now tons are consnmed yearly in filling teeth?"
If this be so it must be regarded as fully time that effort in these two important directions shall be radically changed in its eharacter, or else, for a season at least, be stopped altogether. If the position of Professor Watt be correct, the result is eminently discouraging, and work upon dental chemistry and dental pathology cannot be too quickly abandoned.
But is this so? Is it true that dental chemistry has done naught else but retrograde? Is it true that we know far, far less of dental pathology now than we did fifty years ago? And if these positions are not true, the reverse, absolutely exactly the reverse of Professor Watt's position is the only tenable ground.
Dental chemistry and dental pathology have both kept pace with the almost unparalleled progress of both operative and mechanical dentistry. They are in no wise in the rear, and just in proportion as the profession has made attainments in chemistry and pathology has been the increase in the use of amalgam!
Next in order in the editorial we find that the author has never "found occasion to use" and has never
"used amalgam fillings in practice." Truly, he is the one who should certainly tell us all about them.
The time has gone by when such enunciations as the editor here makes have the desired effect of placing him a little higher than the other brethren. The thoughts of those who read are not as they would have been in days of yore, but now they pass, in mental review, the hundreds of teeth which must have been lost that could easily have been saved; the hours of infliction that must have been given which could easily have been spared; the thousands of dollars that must have been taken which could easily have been left; the scores of cases which must have been failures that could easily have been successes; and they bless the progress which has been made in dental chemistry and dental pathology, and continue giving satisfaction - comfort and SATISFACTION - to the timid, semi-edentolous sufferers who come to them for relief, by doing their share in using a part of the tons of amalgam which are now consumed yearly in the filling and saving of teeth!
A fitting "snapper" - because it will not crack! - to this editorial lash is the finally-offered proof (?) as to the absence of close thinking on the subject by those who discuss amalgam. The concluding paragraph is worthy of quotation as an evidence of what is regarded as "close thought" by an authoritative opponent of amalgam:
"This late discussion of amalgam" (referring to that of the Illinois State Society, May, 1881) "shows how little close thought exists on the subject. They talk of the way Dr. Townsend made his amalgam, when they ought to remember that Dr. Townsend did not make it, and always so stated, telling, all the while, that he got the formula and the amalgam from Dr. Wm. Hunter, of Cincinnati."
In my work on "Plastics and Plastic Filling" - adopted as one of the text-books of the Philadelphia
Dental College, without my request and without my knowledge - it is stated, on page 30, that
"Professor Elisha Townsend, one of the best gold-workers of his day, gave dentistry his sanction to the first formula for the making of an alloy of amalgam that ever had the least pretention to respectability." On page 35 it is written, "It was not suspected that the "shrinkage" of the so-called
Townsend's amalgam exceeded, enormously, that of the silver-coin amalgam." On page 37, "but it was also due, in part, to my gradual change of formula from that of the so called Townsend's". On page 84 it is said, "It is now about twetity-five or thirty years since the mode of making which has been referred to and described as the "mortar" and "washing" was brought to the general notice of the profession by Professor Townsend. It is not claimed that the ideas originated with him, but, on the contrary, it is admitted that the formula for alloy and the process of "washing" were both given
Professor Townsend by Dr. Hunter, of Cincinnati."
These numerous extracts are given to show, conclusively, what a tremendous amount of intensely
"close thinking" must have been given to this momentous matter, - and yet, this was all bestowed without the knowledge that anything was being done except the making of a plain statement of facts.
Whatever may be the laziness, the imbecility, or the quackery of the advocates of amalgam, they are, naturally, and without conscious effort, very powerful on facts.
But what an idea of close thinking is given by the editorial paragraph last quoted! If it requres "close thought" to "remember" that Professor Townsend obtained his formula for amalgam alloy from Dr.
Wm. Hunter, of Cicinnati, what kind of thought must have been required to work out the possible change of twenty grains of mercury from an amalgam filling into twenty-three grains of corrosive sublimate, to be gradually introduced into the system of a patient?
Such brain-racking effort would surely demoralize even a "giant."
And now, if, "after all", it is not probable that the vaporization of the mercury of amalgam fillings in the teeth is the only or even the chief source ot poisoning" (Watt); and if, in their search for a quality in the composition of amalgam capable of producing salivation and all other symptoms of poisoning,
"many able practitioners of dentistry have experimented with all the different acids with no satisfactory results" (Talbot); and if the statement "that the vapor mercury is poisonous is beyond dispute" (Watt), is so far antagonized by authority that in one case quoted it salivates near all of a crew, and in another case quoted it proved a safeguard against contagion from yellow fever to all who had been subjected to it, keeping them "perfectly well, although surrounded by sickness and death" (La Roche, vol. ii., p. 762); and if, in the experience of a tremendously overwhelming majority of those who have extensively used amalgam for ten, twenty, or thirty years, the reputed cases of ptyalism, dyspepsia, paralysis, and death from its mercurial composition are literally
"number-less," - is it not about time that the labor of dental investigators should be no longer
"wasted" (Watt) in the endeavor to find out how these imaginary results are occasioned; that the pages of dental journals should be no longer burdened by such contributions and editorials as those found on this subject in the January number of the "Ohio State Journal of Dental Science; and that the futile attempts to clog that inevitable increase in the use of amalgam, which has been so persistently and so signally demonstrated to be one of the natural results of the struggle for the saving of the frail, soft teeth, should be no Ionger essayed?
AMALGAM.
THOMAS FLETCHER, F.C.S., WARRINGTON, ENGLAND.
Dental Items of Interest Vol 6, 1884, 171 3
Dr. I.P. Meredith says: "There is a compound ...which goes by the gentle name of amalgam. I pause upon the threshold of this subject, as I feel my utter incompetency to do the subject justice." If he had, after giving so good a reason, left the subject alone, one could not have well found fault, but unfortunately he is not satisfied with the simple statement, but goes on to prove it in the most thorough manner possible. He begins: "the mischievous agent is mercury, which causes soreness, swelling and ulceration of gums and tongue, profuse salivary flow, coppery taste, loosening, blackening and decay of the teeth, gangrene, etc., etc." In answer to this I can only say, that in twenty years I have not seen a single case such as he states caused by amalgams in the mouth, although I have seen thousands of amalgam fillings; that the experiments of Dr. Bogue prove most conclusively that mercury is not absorhed in the most minute traces from amalgam fillings under the conditions found in the mouth in any degree. I see plugs of these materials which have been in the mouth from twenty to thirty years, which are invariably as satisfactory as fillings could be in every respect, except as regards surface discoloration, and any operator, who has had much experience with these, speaks most positively as to the uniform success and satisfaction he has with their use, with the one exceptional point of discoloration of the surface of the plug.
He says: "And now we will consider another of the evil effects caused by amalgams, and that is galvanic action. (We are astonished that a man of Dr. Meredith's reputed attainments should not reflect that for the amalgam in a tooth to act as a battery, there must be two pieces of dissimilar electric metals. In the case of the amalgam filling, therefore, where are the opposing poles? Even if the silver and the tin of the amalgam were separate they would not be such metals as to produce opposite poles, neither would they if there were a multitude of such fillings in the same mouth.
Besides, if there were some fillings of positive and some of negative metals in the same mouth, where is the connection? The teeth are non-conductors, and the fluid of the mouth is not sufficient of itself. Then where is the battery ? Ed. ITEMS.). He rerers to the coppery taste caused by plates of dissimilar metals, being apparently ignorant of the fact that these plates of dissimilar metals are necessary to cause galvanic action, and that alloys act as single metals when used as battery plates, notably brass, which will replace copper in Wallaston's battery, platinized silvcr, which acts as platinum alone would in Smees' battery, and last, but not least, the alloy of mercury and zinc which offers a resistance to acid solutions incomparably greater than zinc alone, the zinc becoming soluble only when in contact with a plate of a dissimilar and less soluble metal. He refers to "every-day schoolboys' experiments" to attempt to prove his assertions. I would suggest his attention to these
"every-day schoolboys' experiments, the value and force of which he apparently does not appreciate.
If they were not amply sufficient to upset the galvanic action theory, amalgam of palladium and mercury, two most dissimilar metals in every respect, would in itself be sufficient to do so - as it is known by every operator who has used it not to discolor the dentine or to cause the slightest change in any number of years. Further than this, my own experiments have proved beyond doubt that the failure of amalgam discoloration of dentine, etc., are caused simply and solely by the alteration of form of amalgam plugs by the mechanical interference of moisture by capillary action, and that the discoloration, under ordinary conditions, is in precise inverse proportion to the power of the amalgam to retain its form under water. He then details the "chemical action set up by the galvanic action." "The electrical current decomposes the water of the mouth; the hydrogen set free combines with the chlorine of the chloride of sodium present! The oxygen combines with the nitrogen form, decomposing food, etc., and form nitric acid! The union of the two giving us aqua regia." Now we want to know where the sodium is all this time, and why it does not take up the oxygen, as it certainly would if it had a ghost of a chance. Surely the schoolmaster is abroad who teaches elementary chemistry.
Dr. Meredith again says: "It is useless to attempt to answer these indictments against amalgam by advancing occasional instances of persons who have had considerable amounts of it in their mouths for years and yet enjoy good health, and have retained their teeth in fair condition. It may be that isolated cases exist which we do not understand." Here he has at least hit the nail on the head with vengeance. The isolated cases are those which occur in the practice of the few dentists who have taken the trouble to understand the material they use and to use it in a proper manner. Some dentists object to blame themselves when they fail, and therefore do not understand the success of others.
Again, "certain it is, at least, in all cases that amalgam plugs become unsightly, that there is always more or less shrinkage around them, etc." As regards shrinkage, a plug of precipitated silver expands so much as to visibly lift above the level of the tooth and to burst it open if weak and much undercut; palladium amalgam and precipitated copper amalgam cannot be found with a probe, if inserted with moderate care; an alloy of two equivalents silver, one equivalent tin, with ten percent gold, expands in hardening, (although from other causes it is unfit for amalgams) as do many other alloys. Shrinkage therefore does not always occur. "Besides, alveolar abscess occurs much more commonly associated with amalgam fillings than with any others."
This is easily explained by the simple fact that amalgam is used frequently as a last resource, and its use is in most cases accompanied by carelessness on the part of the operator. With equal care, knowledge and judgment, the failures with amalgam would be more rare, taking every case which presents itself, than with any other known filling. As a grand climax he condudes: "I would not be understood to say that amalgams should never be used amalgam, which, unfortunately, are precisely those which the whole of the experiments ever published go to prove as the very worst possible, and which entail certain ultimate failure. I should recommend Dr. Meredith a little quiet study of the
"Transactions of the New York 0dontological Society," a little private careful experimenting, and a little careful work in the mouth with this material which he states is the cause of so many of the evils flesh is heir to, but which he has still the audacity to recommend shall still be used, notwithstanding the fact that if his statements be true, the operator would be pretty nearly committing murder. After his study and experience he would perhaps not feel so fully his "utter incompetency to do the subject justice," which he has so clearly and fully proved. Missouri Dental Journal
A FEW SUGGESTIONS ABOUT MERCURIAL FILLINGS FOR
TEETH.
Wm. P. Wesselhaeft, M.D., Boston, Mass.
Proceedings of the International Hahnemannian Association 16, 1896, 200-209
Early in the sixties I had my first practical experience with these fillings. A middle aged woman doing housework in a neighbors family asked me to cure a sore tongue from which she had been suffering several months. On examination I found a gouged out ulcer on the left side of the tongue, which lay against, and partially around a molar tooth. This tooth had been filled and built up with a grayish, glistening mass and had done good service for nearly eight months. In those days lunar caustic was the proper thing to touch all ulcers with, which would not heal, and she had been cauterized several times, each time leaving the ulcer in a worse, and more painful condition than before. I treated her as carefully as I knew how at that early period of my professional experience, but without any apparent change in the very sore tongue. After six weeks of treatment I persuaded her to have the tooth drawn, which she very reluctantly consented to, and I accompanied her to the dentist's chair the same day.
The tongue was thickened, the edges of the ulcer felt very hard to the fingers, and the pains were often sharp darting, but she complained chiefly of soreness which made eating, and talking even, painful. I suspected malignant disease. The removal of the tooth was soon followed by improvement, and in a very few weeks the tongue was healed.
I firmly believe the ulcer was caused by the contact with the filling. Some people may disagree with me and exclaim post hoc ergo propter hoc. The woman, however, got well after the removal of the cause whatever that may have been in the minds of other people.
The second instructive case occurred in 1883. A young man twenty- four years old had to leave his studies on account of inveterate dyspepsia. He was taken to Europe after finished with all sorts of drugging in this country, and went through the usual Carlsbad cure, where he only grew worse, and then was sent to Ragatz "to build up on the waters and the Swiss altitudes." He did not build up at all, but his instead his stomach caused him more and more pain. When he came to me the main symptoms were as folows: Dull aching pains in pit of stomach, extremely sensitive to touch and pressure of clothing. Is usually relieved for a short time after eating; continual raising of gas, which gives only temporary relief; worse sitting up, better lying flat on back. General times of aggravation between 10 and 12 A.M. and again after 4 P.M. Great aggravation from cold drinks.
This case I treated for over a year with what is usually called success, so that he could take up his studies again after a few months. Nevertheless, there remained constant recurrences of the old symptoms. One day he came in and asked me to look at his throat, as he had felt alternatively cold and hot with intense pain on swallowing. When I looked into his throat I saw a very decided follicular tonsillitis, but what interested me more, was about two square inches of mercurial fillings staring me in the face. I gave him a remedy for his tonsillitis, and told him that I should decline to treat him after this unless he had every mercurial filling removed. This he did immediately, and I think he spent the most of three weeks in the dentist's chair.The fillings had been put in when he was about fourteen years old. The result of the removal of the fillings was a perfect and permanent cure of his chronic gastritis.
In Dec. 1885, a young lady of twenty-seven years presented herself for a throat affection, which had existed for three or four months, for which she had been locally treated by a specialist without relief.
She had a fine voice, and came to the city to pursue her musical studies. Her voice had so entirely failed her that she was on the point of abandoning her studies, and the specialist gave her little encouragement of a cure.
The symptoms were as follows. Sensation of a foreign body in the larynx, much aggravated by attempts at singing. After singing a few notes voice grows so hoarse that she cannot produce a tone.
Has a constant desire to swallow this lump down. All symptoms of throat aggravated by any attempt to use the voice in singing. Is always much worse during damp weather. Has a slight post-nasal catarrh, with hawking up and drawing down of clear mucus. Is always better while eating, and then the sensation of lump entirely disappears. Has had much grief during the last two years. All functions normal, and she looks the picture of health.
On examining throat I found four molar teeth filled with mercurials. I decided to try two remedies and if they acted palliatively or not at all, I should decline to go on with the treatment till the fillings were substituted by gold. Ignatia helped her wonderfully for a week, then everything returned.
Spongia relieved her for a few days only.
The fillings were removed, and one dose of Ignatia took away the lump and it has never returned. I observed this case from December till May. From January 15 to May 14 she was able to sing, and had no more hoarseness, and made very satisfactory progress in her art.
A case of Menie`re's disease treated by me during the last ten years is also instructive. I am fully aware what a vague term Meniere's disease is, and that it can convey no concise idea of the terrible misery this young school teacher was suffering from, till she fortunately came within the blessing of
Hahnemann's teachings. It would be too long a story to relate here in detail. She had been a sufferer from intense vertigo, nausea and tinnitus, which came in paroxysms obliging her to give up her occupation for weeks. During intervals of freedom from vertigo etc., she was comparatively comfortable except a constant tinnitus, and dullness of hearing.
She improved very much after Silicea, which was very surely indicated. Still occasional occurrences of entire incapacity to perform her duties recurred year after year during which time she reported every six to eight weeks without thoroughly eradicating these attacks. At one time she obtained almost two months of freedom after a dose Kobaltum given after the symptom of stinging pains from soft palate into left ear. The tinnitus, however, remained. Two years ago I had over a dozen amalgam fillings removed. When one of these fillings was opened to the base, a horrible odor came from the cavity; her dentist told her he had never smelt anything more foul, and dentists ought to know what a foul smell is.
Her health has markedly improved during the two years. The tinnitus she says is now "so far off" that she scarcely hears it. A ptosis of both eyelids has entirely disappeared during the last year. A chronic post-nasal catarrh gives her no more inconvenience. She told me a few days ago that she should never regret the inconvenience and expense of the removal of the old fillings, even if her head and ears had not improved, because she now felt that her teeth belonged to her and she could use them with real comfort, which was a new sensation to her. These fillings had been in her teeth since her girlhood.
I have several more cases, but I will only report one more. A young gentleman of twenty-five years appealed to me for the cure of an eczema which appeared chiefly on scrotum, pubis, and legs. As he
lived in Brooklyn I advised him to consult one of our honored members, who I knew would take the case into careful consideration.. The young man was tortured by the most intense itching especially at night, so that frequently he was kept awake three to four hours. After nearly a year of treatment he derived no benefit whatever, and appealed to me again. After an examination of his case I came to the remedy which I thought surely indicated, but I knew that my astute friend in Brooklyn must have given it to him. Among other indications there was a fearful thickening and deformity of the nails of fingers and toes. Besides the eczema of scrotum, crotch and legs, he had a thick, crusty eruption on left ear, which was so disfiguring that he was obliged to throw up a lucrative occupation. On the left side of head above the ear a large crust had formed and the hair was closely matted down into this crust. The itching was intolerable in all parts of the body affected.
By the merest chance my attention was drawn to his throat, as he complained of some catarrhal irritation there. On examination I found a whole battery of mercurial fillings which he told me had rested there since his boyhood.
I knew the eczema was inherited as I had treated and helped his father of a similar eruption on the scrotum several years before. I knew also that my colleague in Brooklyn could recognize an indicated remedy far better than I could. I knew that the mercurial fillings were not inherited, and their existence had escaped the attention of my colleague who had treated him for months without benefit. I sent him home to Brooklyn with the order to remove every amalgam filling. I think he had sixteen removed. Then he came to our hospital as a private patient, as his appearance made it impossible for him to get into any other quarters, so repulsive was his condition. He remained here four months and I have the gratification to say that he is so nearly cured that he has resumed his work. The thick crust on ear has vanished. He sleeps eight hours every night. His finger and toe nails have improved wonderfully, and his mother sent me this message: "The Lord be praised that our son is again presentable through your ministrations."
Now this is all very fine and satisfactory. But I have something to offer per contra. A young woman whom I have been treating for over a year for intense headaches, and an offensive ozaena, derived great benefit for the latter affection, but the headaches persisted although the remedies given were carefully chosen. She had a mouthful of amalgam fillings, which were removed at my advice six months ago. So far the removal has not in the slightest degree aided me in overcoming the headaches. She is still under treatment, but no better. I am, however, much more confident of ultimately healing her now that the amalgam fillings are removed.
Per contra, another case: A man of forty has had continual canker in his mouth, on tongue, gums, and cheeks since his boyhood. They have been especially persistent since a suppression of eczema fifteen years ago, since which time he has rarely been without one or two large ulcers in his mouth. I found he had a mouthful of amalgam fillings which he had carried since boyhood. They were all removed last October. I have treated him ever since and he is not one whit better since the removal and the treatment. Nevertheless I feel that I have removed a possible hindrance to his case, and if he
"sticks" I hope to eradicate this psora from his system, which would probably be doubtful with the amalgams remaining.
The use of amalgam fillings dates back a great many years. No two are prepared under exactly the same formulas, but they are generally composed of silver, tin, zinc mixed with mercury. Some of them have platinum or copper also mixed with them to give them greater hardness, and to prevent their shrinking away from the margins of the cavity. Some are entirely of copper mixed with mercury, which gives the hardest kind of filling so far as saving tooth substance is concerned.
This paper is merely offered as a stimulus for further investigations. However, I advise you to look into patients mouths if the indicated remedy fails, or acts only palliatively.
DISCUSSION.
Dr. H.C. Allen - That is a very instructive paper and one from which we may learn a good deal. In my practice I am in the habit once or twice, or some times oftener every month, of sending patients to the dentist to have mercurial fillings removed. I have found that a great many cases of follicular pharyngitis, and many other affections of the throat, post nasal catarrh, etc., are practically incurable until these amalgam fillings are removed. I have relieved chronic rheumatism many times after having the mercurial amalgams removed, and I think this is the experience of a great many in our profession.
I remember one case last winter, a lady about forty-five, a large, apparently healthy looking woman, came into my clinic with a very peculiar report, What she wanted to get rid of most was a tumor in the left side of the middle of the tongue, about as large as a walnut and hard as a piece of lead. On the upper portion of this was an ulcer, about as large as a dime; sharp, shooting, pricking, stabbing pains; profuse salivation; swelling of the carotid and submaxillary glands and, also, the cervical glands on that side. She had, I think, thirteen large amalgam fillings in her teeth and one tooth, a molar on this side of the mouth, almost entirely built up, the entire crown being of mercurial amalgam.
The first thing to be done was to send her to the dentist and, after two or three weeks, she returned with the amalgam fillings removed. Her case was then very carefully taken, and one peculiar factor in it, one peculiar symptom, was that for a number of years since these fillings had been put in her teeth, she had only menstruated once a year. Psorinum was given her and pretty soon an improvement began, and within a month menstruation occurred, profuse, long lasting, painless, dark, offensive and clotted. This was followed by a decided improvement, and in another month the tumor was nearly gone, and the ulcer, or whatever it was, healed up. She is still under treatment and far from well.
Dr. Clark - The experience of Doctor Wesselhaeft goes to confirm the experience of all others who have given any attention to this subject. Doctor Gregg, of Buffalo, has given, or did give, more aftention to it than anyone of whom I know, and some time before his death I wrote him regarding the subject, and he sent me a lot of literature on the subject including some of his writings. He had attempted to educate the public in Buffalo up to the point of avoiding amalgam fillings. He had written to the daily papers; there were quite a number of articles over his signature that he sent me. It is an important subject, and, as I said a moment ago, anyone who has given any attention to it will be able to confirm what Doctor Wesselhaeft has had in his experience.
I had numerous instances of it. I remember particularly one young lady who was subject to attacks of pharyngitis. Ulcers would form; the medicine would help, and again another attack would come on.
She had quite a number of amalgam fillings, and until they were removed she continued to have the attacks. So soon as they were removed the attacks disappeared and she has had none since. The dificulty is not confined to the throat, but there are symptoms in other parts, and it is always important to get rid of the amalgam before we will be able to do anything for the permanent relief of these cases.
Dr. W.L. Morgan - This discussion brings to mind an experience I had when I was practicing dentistry. There was a lady complaining of rheumatism or something else, didn't know what; had complained several years. She was limping a part of the time, walking on a crutch for a pain in the
ankle without swelling, a simple pain, and described symptoms like headache. Finally she came to me to give some little attention to her teeth. I found three large amalgam fillings in the lower molars of the same side. She then told me about her trouble with the ankle, and after carefully investigating the symptoms all around I told her I thought those fillings were having a great deal to do with her ill health. Well, she said, take them out, then, and it did not take much persuasion till I took them out, and put in gutta percha filling. In about six weeks her ankle was well, and her headaches were well, and for three, four years afterward she had good health and no trouble. Since that time I have always made it a habit to watch the mouth, when symptoms would appear that I could not get relieved by the remedies that seemed to be indicated, and I have always told them to go to a dentist and get the amalgam fillings taken out. I have found, in a large majority of cases, that it rendered the case curable, if it did not cure it without any other treatment. Only last week I directed one of my patients to have an amalgam filling taken out, on account of an earache and tonsilitis, with a swelling under the ear that resisted all treatment. I found a large amalgam filling on the lower second molar. I directed her to go and have it taken out and she did so just the day before I came away, so I don t know what the result has been.
MERCURIAL NEUROSIS RESULTING FROM AMALGAM
FILLINGS.
by J. Y. TUTHILL, M.D., Brooklyn, N. Y.
THE BROOKLYN MEDICAL JOURNAL, vol. XII, dec. 1898, 725-742
Read before the Medical Society of the County of Kings.
Mercurial neurosis is a field of pathology which has not received the investigation it deserves by the medical profession. While the poisonous effects of mercury have so long been recognized that I need take no time in rehearsing them, yet there are certain causes affecting the nerve-centers which demand more thorough investigation than has yet been given.
In presenting this subject to the Society for consideration I want to show that by the use of amalgam in filling teeth there is a possibility of mercurial poisoning, which seriously affects the nerve centers, impairs locomotion by heaviness of limb and stiffness of joint, gives rise to obstinate diseases of the skin, and makes a mental wreck of its victim, whose imaginations and hallucinations are more than my pen can describe.
Physical examination reveals nothing to assist the physician in making a diagnosis of his case, as all the functions are usually well performed. There is, however, nervous depression, irritability, unreasonableness, an inability to overcome and throw off feelings of oppression which settle upon the patient and hold him as in the clutches of despair until his ambition is broken, his energy is gone, his purpose is lost, and he drifts for lack of power to concentrate his actions and assert himself as a force in the world. There are shifting, shooting pains here and there from head to foot, affecting sometimes one part and then another; numbness of hand, foot, orjaw, heaviness of leg, arm, or head, with an almost inability to move them, and a feeling as though one would fall or lose consciousness.
Again there is a light, floating sensation as though moving in air. There is mental excitatbility as well as mental depression; Perplexing events cause the highest degree of excitement, ordinary conversation sometimes causes, complete confusion, headache, palpitation, intense solicitude, and anxiety, without reason for it. Such are some of the symptoms attending these cases.
To bring this pathological condition more clearly to your thought, allow me to cite a few cases which have come under my observation during the past few years, and you will pardon me for alluding to my own individual case which first opened my eyes to this subject.
During the winter of 1884 and 1885, when working far beyond the limits of good judgement and averaging from October 15th to April 27th, not more than from 4 to 4 1/2 hours sleep per night, I was attacked February fist with neuralgic and rheumatic pains, usually short in duration, lasting from
10 to 15 minutes to 3 or 4 hours, affecting chest, back, arms, and legs. My work was ardous, and the professional demands upon my time and strength prevented my getting adequate rest. With failing strength and energ, I continued my daily routine of work until April 27th, when I was in a state of physical and mental collapse. I sought a quiet place for rest, and April 28th went to Saratoga
Springs. Arrived there at 3 P.M., and in half an hour was in bed. I had a good nights rest; and after breakfast the following morning took a stroll through the village, which at this season of the year is the sleepiest place of its size that I know of. Then, thought I would write home news of my safe arrival and a good nights rest. But never was I more surprised than to find that I could not write more than two or three words when my hand would be so numb that I could not hold the pen, until I had rubbed it for some minutes. The same processes were repeated over and over again until I succeeded in writing a short letter. This condition continued, with some abatement, for many weeks and, in much less degree, for years following. I remained in Saratoga for 10 days sleeping 13 and 14 hours in every 24, then returned home and resumed practice fee]ing much improved.
An eruption which appeared like psoriasis, and had troubled me for several years, became more troublesome and refused to heal, much to my annoyance and chagrin. All the foregoing conditions continued up to the spring of 1889, when a persistent headache, often of neuralgic character, continued for 2 or 3 months, which was relieved by taking a 4-months trip abroad.
Since that time I have had average health, with occasional numbness of hands. The handling of steel would almost paralyze my hands for some minutes to come. The eruption continued the same, resisting all treatment that my own ingenuity could devise or that my professional brethern, who took a kindly interest in my case, suggested.
The numbness attended with pain in the fingers, was thought to be a form of gouty neuritis.
Following their advice, I took such remedies as they prescribed, sometimes it seemed for the better, but with no permanent improvement.
In the summer of 1895, spending the month of August on the Shawangunk mountains, I was applying to the eruption several times a day, a lotion of bichloride of mercury, which accomplished more for healing than anything I had ever used; but while the eruption was first getting better, my hands were rapidly losing their power and I could not rely on holding anything, nor could I pick up small things like pins, needles, or twine, because of the numbness. At this juncture, it occurred to inc that I was absorbing mercury, and that mine was a case of mercurial neuritis or paralysis, the result of this absorption, and that the eruption was a mercurial psoriasis. Returning to the city I laid the matter before several physicians, who thought I was mistaken as my gums showed no evidence of mercurial poisoning, and on their advice resumed the use of the bichlorid lotion, but was compelled to abandon it in a few days because of the numbness which followed. I reported my condition. They then agreed with me that the mercury affected my sysiem in an unusual manner, but thought that I had an idiosyncrasy, and that it would probably not affect more than one in a thousand under the same circumstances.
Being thoroughly aroused as to my state, and having several amalgam fillings in my teeth, I soon came to believe that my entire condition, the numbness, the rheumatic pains, and the eruptions were all due to the action of mercury absorbed from those fillings. So I decided to have them removed, and the work was done in May, 1896. In two weeks I felt like another man; it seemed as though a great weight had been lifted, and I was once more free from an oppression whch had hung over me like one long nightmare for years, handicapping, restricting, and restraining me on every hand.
My improvement has continued from that time to the present, the numbness growing less and less, the eruption disappearing until there is less of it than at any time in 15 years.
I do not imagine that all the mercury that I absorbed from those fillings which I carried for thirtyeight years, is out of my system, but from my general improvement, believe it is growing less all the time, and I am feeling better than at any time since the spring of 1885. Having lived for eleven years on the ragged edge of hope and dispair, and thus secured my freedom from a bondage worse than human slavery, I could appreciate the sufferings of others when they rehearsed experiences which I had realized. As a natural consequence, I readily recognized the same enemy to their peace and happiness which had shattered my own.
In December, 1896, I was called to see Miss F., aged thirty-three years, who had been in excellent health previous to an attack of la grippe in december, 1892. Since then her nervous system had been much disturbed, and she had come to be melanclolic and to withdraw herself from her family and friends, seeking the seclusion of her room - refusing to go out or to associate with others, or eve with the members of her own household. When I was called she had been treated by five different physicians with no improvement. I treated her for indigestion, torpid liver, constipation, etc., for ten weeks, with no improvement in her mental condition. Then numbness of hands and stiffness of jaws led me to examine her teeth, when I found five amalgam fillings which I believed, had produced a mercurial neurosis. I gave it as my opinion that her condition was due to the effect of mercury upon her nervous system absorbed from those fillings and advised their removal. She was stubborn and for some time refused, but yielded in May, 1897, and had the work done. She has steadily improved since that time, and her family say that she has not been so well in five years as now.
In the early part of last September, Miss F., aged eighteen, was brought home from a three months' sojourn in the country, with all the indications of typhoid fever. I Intestinal antiseptics, tonics, etc., arrested the progress of the case, but an unaccountable languor, debility, loss and flabbiness of flesh with drowsiness, continued for several weeks, she sleeping 18 and 20 hours out of 24. My case otherwise appearing well, her sluggish gait, heaviness of limbs, and stiffness of jaws led me to examine her teeth, in which I found 9 amalgam filings. Being convinced that these were retarding her recovery, I advised their removal and the substitution of gold. When the fillings were taken out she became more wakeful and animated, and has continued to improve although still suffering from the effects of the absorbed mercury.
Miss K., a young lady of culture and refinement, was brought to my office December 1 1887, surffering from extreme nervousness, which had continued for 3 years. She was restless and could not appIy herself for any length of time to any one thing, sleepless, irritable, hysterical etc. Having maade a thorough examination of her case and being assured that all her functions were normal, I examined her teeth and found sixteen amalgam fillings, several of them in teeth containing gold fillings. Believing this to be a case of mercurial neurosis I told her, and her mother who accompanied her, that her case put me in mind of what I had read in "Ziemssen's Cyclopaedia" a day or two previous on mercurial poisoning, and I read to them, viz.: "Essentially the condition is characterized by great mental excitability of the patient to external impressions. Every unexpected or perplexing event excites him in the highest degree. The visit and the conversation of the physician put him into a state of complete bewilderment, even to syncope; the adult patient grows pale and stammers in answering the simplest questions. To perform his allotted task requires the greatest effort, or is even impossible if he sees or thinks he is being watched. There is also great solicitude and a feeling of anxiety without any reason for it. There is sleeplessness, or sleep which is restless, frequently broken and disturbed by frightful dreams, headache and palpitation. In the severer forms there are frequently hallucinations, usually of a frightful nature. When perplexed or excited, traces of tremor are often perceptible in a slight twitching of the muscles of the face at the corners of the mouth." Having heard this, she remarked that it was a perfect description of her case in every particular, except she had not had the hallucinations there mentioned. Following my advice the fillins were removed and the young lady has improved very rapidly to the present time, all her nervous feelings having disappeared. Indeed, her mother tells me that she has manifested none of her nervous troubles since the removal of the fillings.
In February, 1897, was called to see Mrs. N., who was extremely nervous, with neuralgic pains in the chest and palpitation of the heart. Upon looking up she felt as though she were falling backward.
Had heaviness of limbs. loss of memory, and found it difficult to think and harder still to put her thoughts into words. Numbness of hand or foot, a sensation of floating, and a feeling that she would die, were common experiences. I did not see her many times before I examined her teeth and found one large amalgam filling in a lower molar, which I advised her to have removed, but doubting its necessity she kept it until November. Here I wish to read a letter sent me several weeks ago:
"DEAR DR. TUTHILL: "I wonder if there is another woman in this world who has had all the peculiar feeling that I have had within the past two years? You know that I am one of the healthiest- looking mortals, have good appetite, sleep fairly well, etc., yet for all this time I have suffered from such awful feelings. I was afraid to go out alone, or be alone, and in constant fear that something dreadful was about to happen. I suffered much from palpitation. Sometimes, when sitting in a streetcar, the people would suddenly begin to look queer, the car crooked, and I would look around at each one to see if any one realized the dreadful condition of things. I had also light, floating sensations, and at times it was hard to talk, to think, and speak in sentences. When lifting my eyes upward I felt as though I were falling backward. Then my limbs were so heavy, my memory seemed to be gone, and I often felt dazed. Even when conversing with friends, or sitting at the dining-table, such a horrible feeling would suddenly seize me and I thought that in a moment I might fall down dead. I became hot and cold and sick, and would have to rise and walk about till it passed over. The feeling that I was just about to die often came to me with sensations that I cannot describe, but such as I should imagine a person dying would have. It began at my feet, a numb, cold, creeping feeling, and I seemed to to be hardening all over. Two or three of these spells I would have in a day, lasting from ten minutes to half an hour.
"You told me last spring that if I would have an amalgam filling in one of my teeth removed, a large part and perhaps all of these nervous troubles would disappear. But it seemed so absurd to me that I hardly gave it a thought till you urged it again this fall. While my husband was in one of the Western citie he happened to be in a large Dental Association and asked the President if he had ever heard of amalgam fillings causing nervous troubles. He replied, 'Yes, we have. It is not common, but some people are poisoned by the mercury, as I can prove,' and then he cited the case of a man in that city who was a nervous wreck, given up by several physicians. At last one doctor said he believed him to be surffering from mercurial poisoning, and, upon examination, found seven amalgam fillings in his teeth. They were removed and from that day the man began to improve, and is a strong, well man today, scarcely knowing what a nerve is.
"So my husband wrote to me to take your advice and have the filling removed. I did so about two months ago. Immediately I felt better and coming home felt as though I could have walked to
Beersheba and not have fallen. My buoyant feelings have not lasted, however, and some days I am almost discouraged. But I know that I am better. I have not have one of those awful dying sensations, nor do I have nearly so much of my nervous troubles. I can go downtown and to New
York and do many things that I could not do before I had the amalgam filling out. Still I do have days of some of the old feelings and fears, but they pass away more quickly. I am living in hopes that it will be as you said, 'They will all be gone to stay away, in time.' But as the filling was in two and a half years, I could not expect to be cured in two months.
"Oh, Doctor, how I wish that I had taken your advice last spring and saved myself the sufferings of the summer and fall! I wish I had never had it put in my mouth. No dentist could put in another for any amount of money. I want to thank you with all my heart for insisting upon my having that filling removed and bringing brightness again into my life. Days when I feel well I am the happiest woman living. I only long to feel entirely well, and trust as the poison passes off that I shall. "Very gratefully yours, Mrs. N."
In July last I was called to see Mrs. H., aged twenty-six, who was in a very excitable condition, afraid to go out alone in the street or stores lest she become unconscious and be taken to some hospital. Upon looking up she felt as though she were falling backward; when looking down, as though falling forward; when standing still, as though she were going to pieces; when lying in bed, as though floating toward the side wall; when sitting in a chair she often felt as though she were dead all over, and that it would require the greatest effort to make any movement. Her troublcs began in the fall of 1895, with pains in the back of her neck and about the lumbar regions followed by pains in her left thigh and arm, which would last from a minute to one or two hours and then pass off to reappear there or elsewhere at irregular intervals. In the spring of 1896 she complained of stiffness of the jaws, of her left hand foot going to sleep, with continued numbness of the third finger of the left hand. The left side of her head and the left ear would often become numb. The large toe on the right foot would be numb for weeks at a time. She also complained of her limbs being heavy, like lead, and at times it was difficult for her to raise them.
There was loss of memory, the eyes looked dull and heavy, the skin had a dingy look which washing did not improve. Feelings of dread and fear lest some calamity might befall her, made her afraid to stay in or go out alone, which she had ceased to do for more than a year. I treated this lady for several weeks without making any progress on the case. Then I examined her teeth and found nine amalgam fillings, which I believed had more to do with her conditien than anything else. I therefore advised the removal of the fillings and that they be replaced with gold or bone. The work was done.
In less than a week she began to improve; in three weeks you would hardly have believed her to be the same woman. All her symptoms have abated; the numbness, the heviness of limbs, the constant fear, the falling tendencies, the stiffness of jaws, have disappeared, and she goes out alone. There is a buoyancy and vivacity in her manner which shows that her hopes and anticipations are bright. Her skin looks clear and healthy, her eyes sparkle with expression, while her memory is true to her as in forer days. Since the removal of the amalgam she has gained twenty pounds in weight. I might say in passing that nine physicians had treated this case before it came to me.
I might describe several other cases, in one of which the fillings were in between twenty-five and thirty years, and the toxic effects mainifest for a dozen years; but those already given are a sufficient illustration.
Members of the dental profession who are so freely using amalgam tell us that over the surface of each filling there is an oxidation which prevents any possible absorption of the mercury. Fillings which have been removed are bright, where in contact with the cavity, indicating that this oxidation occurs only to the exposed surface and not to that which comes in contact with the structural parts of the teeth. The circulation in the teeth, is continually in contact with the unoxidized surfaces of the amalgam and constantly receiving some mercurial taint which is carried throughout the system. As the nerve-centers are most impressionable to its toxic effects, we find neurasthenic conditions chiefly resulting.
It is not my purpose at this time to indulge in theories as to how these results follow the use of amalgam, but to merely state the facts. While many having these fillings seem to be exempt, others suffer from the subtle effects of the mercury. This is clearly proven by the cases I have cited, which have come to my knowledge during the past two years. So long as the system keeps in vigorous condition many feel no ill effects of the poison, but when from any cause it falls below par, either from over-tax or from disease, the toxic effect of the mercury becomes dominant, with those susceptible to it, and gets the mastery of the nervous system, to be followed in many cases by the tram of symptoms mentioned above.
Although the number of cases may be comparatively few, they deserve as thoughtful consideration as would be given the subject if mercurial neurosis were more common. I doubt not that our insane asylums have many an inmate because of a mental state developed by amalgam fillings, which produces excitation or sluggishness of brain, impairs thought, destroys memory, blunts perception, and relegates to despair what otherwise might be a bright and brilliant career.
To insist upon a patient's enduring the agony, torture, and expense of having these fillings changed for gold, requires considerable nerve, with positive assurance of a correct diagnosis, for in case no improvement should follow the physician would be a subject for wholesale condemnation, and branded as a crank. Fortunately for the writer, in no instance has he advised the removal of these fillings where a marked improvement has not followed in a few days. It would be unreasonable to expect the relief to be complete and immediate, for the removal of the fillings does not remove the mercury which has been gradually absorbed into the system during months and years of contact with the amalgam, and which has seriously affected the nerve centers. But it does stop the supply, and when that is cut off there is an abatement of all the more prominent symptoms, followed by a marvelous improvement, and the patient realizes that he is living under new conditions, with hopes and aspirations he has not known for long months and perhaps for years past.
For the conscientious physician the obscure and unsuspected causes of disease have a peculiar interest, and he will not allow prejudice to prevent a careful investigation of the facts which may reveal such causes.
If this paper shall but stimulate some present to a more earnest study of this subject it will have fulfilled its mission and put into motion a train of thought which must eventually secure to many a now hopeless sufferer a relief so great as to be almost the beginning of a new life.
Discussion.
R.C. Brewster, D.D.S.: When our President asked me to take part in this discussion, and told me that
I would be allowed ten minutes, I determined I could cover more of the enormous ground involved, and in a more connected manner, if I should read what I had to say.
History. - About the year 1826 M. Traveau of Paris, France, advocated the use of what he called
"Silver Paste" for permanent fillings in teeth. This metallic preparation was first brought to the notice of the dental profession in the United States about seventy years ago through the advertisements of two Frenchmen by the name of Crawcour.
It was called by them the "Royal Mineral Succedaneum"; succedaneum, a replacer or substitute, a name which is indicative of fraud and which, consequently stamps the adventurers as unworthy of professional respect.
It was soon proven that instead of being a mineral compound it was purely metallic, and consisted of silver and copper rendered temporarily plastic by the addition of mercury. It was easily manipulated and they were enabled to fill a class of largely decayed teeth with frail and broken cavity walls such as had never been attempted by the most skilful surgeons.
Scientific investigation at last was imperative, and, as a result, the foremost men who had been arrayed against it now became its ardent supporters. Professor Elisha Townsend, one of the best gold workers of his day, and President of the American Society of Dental Surgeons, found that the cry of mercurial ptyalism was not supported by fact.
This investigation gave birth to an organization called "The New Departure Corps," and was composed of the following gentlemen: Professors Henry Morton and M.B. Snyder, scientists;
Messrs. Jacob B. Eckfeldt and Patterson Dubois, assayers of the Philadelphia Mint, metallurgists;
Drs. S.B. Palmer, Henry S. Chase, and J. Foster Flagg, dentists. The work of this organization gave to our profession what is known as the new- departure creed, the most important deduction of their work being expressed in the following statement: "In proportion as teeth need saving, gold is the worst material to use."
These gentlemen did much to improve the formula for amalgam alloys and it has gone through successive changes until now we recognize the following to be as good in all respects as we can get:
Silver, from 60 to 70; tin, from 30 to 35; and gold and zinc from 5 to 10. These are about the proportions. These metals are melted in a crucible and thoroughly stirred while in a molten condition, and then poured into a mold. After the mass has become cold it is cut into filing with a file and we then have the alloy.
To make an amalgam for fllling a cavity the required amount of alloy is placed in one side of a pair of weighing scales, and an amount of mercury in the other sufficient to balance the scales. Both the alloy and mercury are now put into a mortar and very thoroughly mixed, after which all possible mercury is squeezed out through chamois with heavy pliers, and the amalgam is now ready for insertion into a properly prepared cavity.
An ordinary sized cavity will require 5 grains of alloy. After adding 5 grains of mercury and thoroughly mixing, 1 1/2 grains of mercury can be expressed through the chamois, leaving 3 1/2 grains of mercury in a filling of 8 1/2 grains. This is in a cavity with entire walls. In cavities where contour fillings are required the amount of mercury will be slightly increased.
The object of putting an excess of mercury in the mixing, and then expressing the surplus, is to facilitate a complete and thorough amalgamation, while expressing of the surplus removes only the mercury, no portion of the other metals passing through the chamois.
Such a filling placed in a properly prepared cavity makes what all dentists recognize as a good filling, and from which no mercury can be removed so long as it remains in the mouth. This, I believe to be the consensus of opinion of all scientific practitioners of dentistry throughout the world.
It is claimed, however, that the mercury does get out and is absorbed into the system, producing mercurial neuroses, ptyalism, etc.
If any of the mercury could be removed from such a filling it would no longer be a fit stopping for a tooth. It would be disintegrated, soft, and fall out, either by mastication or the tooth brush. We do not, however, find amalgam fillings acted upon in this way. Fillings that have done good service for thirty years are always as hard as the day they were inserted. The mercury can be removed by heat and by chemical affinity, neither of which can be produced so long as they remain in the mouth. The boiling-point will not eliminate it, and as the tissues of the mouth will not tolerate anything approaching that temperature, heat is excluded.
Chemical Affinity. - I am reminded here of a letter recently received from Dr. Bogus in which he says, in reply to my question about the action of iodids on amalgam: "I did not make any experiments at all relative to the systemic effects of iodin upon mercury which had entered the system from amalgam fillings in the teeth - perhaps because most of the patients for whom I had the honor of operating have not during my time been subjected to a dull red heat, which is about the temperature required to produce either of the two poisonous salts of mercury."
Messrs. Woodman and Tidy, in their work on "Forensic Medicine and Toxicology," make the statement that the following medicines have sometimes produced salivation. Bromin, arsenic, prussic acid, nux vomica, cantharides, digitalis, conium, opium, and particularly iodid of potassium; and in the face of all this the mercury in amalgam fil]ings is made to bear so great a burden.
Professor A. Winter Blythe, in his work says, in speaking of amalgam, that the mercury is in too powerful a state of combination to be attacked by the fluids of the mouth.
That serious consequences will sometimes follow the insertion of any filling material placed in the cavity of a tooth, I will admit, but such results are not due to the nature of the filling material, but to the condition of the tooth at the time of filling. The first of these are caused by the pressure of the filling on an exposed pulp; the second is where a filling is inserted over a devitalized pulp; and the third is where the pulp has been removed and the canals not properly sterilized.
The results from this method of fillings are facial neuralgia, shock from thermal changes, pain on percussion, pericementitis, alveolar abscess and great cellulitis, elevated temprature, fetid breath, and excessive flow of saliva, with corresponding constitutional depression. When amalgam had been used in a filling of this kind, all these conditions were said to be caused by the mercury in the amalgam, but anything that will hermetically seal a cavity containing septic material, will, on true surgical principles, elevate the temperaturu, the same as an abscess without a drainage-tube or any cavity in any part of the body containing septic material with no outlet.
The question that is constantly asked of me is, "How great a loss of mercury is sustained by an old amalgam filling?" This is most thoroughly exemplified by a wonderful series of scientific experiments, in a masterly work on that subject, and as the author of that book is in the room he will explain it far better than I can.
In a letter recently received from Dr. Jarvie he says, "I have practised dentistry for thirty-five years, and have yet to see the first case where injurious results have attended the intelligent use of amalgam."
Far greater than any series of scientific experiments can possibly be, is the fact that tons and tons of amalgam are used every year, and no injury has ever been proven to be caused by it. In J. Foster
Flagg's work on "Plastics and Plastis Filling," in looking for some scientific experiments, he says:
"I found reference made to the practical experiments of Messrs. John and Charles Tomes, in 1861 to
1872, which I had regarded as conclusive and had accepted as such. I found the term 'oxidization' as almost invariably applied to the discolorization of amalgam fillings, corrected by the acceptance of the long before urged, and much more reasonable hypothesis of 'sulphuretting.' I found a long list of elaborate experimentation with filled teeth and amalgam pellets, weighed with marvelous accuracy, placed in little bottles containing saliva acidulated with nitric, acetic, citric, or hydrochloric acid, and kept in a water bath inside another water bath at a uniform temperature - blood heat - for a period of three months, in order to prove by analysis of the saliva whether or not amalgam fillings would be capable of producing, mercurial ptyalism. I could not reasonably doubt the certificate of the Professor of Analytical and Applied Chemistry that the saliva contained no mercury in solution."
In speaking of the systemic effects, the author quotes from a discussion held in the Pennsylvania
Association of Dental Surgeons as follows:
"Dr. C.N. Pierce, one of the professors of the Dental College of Pennsylvania, who opened the discussion, said in regard to amalgam ptyalism, that it was a thing of so rare occurrence that he believed the profession, had never heard of but one practitioner who thought that that result was produced by amalgam."
Professor T.L. Buckingham said, "he had never seen a case of salivation and had doubts about its ever having produced ptyalism"; that MERCURIAL EFFECTS were "influences produced through the general system and he did not think amalgam fillings would, produce thoese effects."
Dr. J.H. McQuillen said that "in an experience of fourteen years he could not recall a single instance of necrosis of the jaws, ptyalism, etc., of which others assert they have seen so many"; and that while he recognized the fact of idiosyncrasies in which the smallest quantity of certain medicinal agencies is followed by untoward results, and would not, therefore, offer his negative testimony as positive proof, yet "his own experience had made him look upon those who assert that they have seen so many cases with considerable doubt as to the value of their judgement or opinions as reliable diagnosticians."
Dr. C.P. Fitch said, "in regard to its toxical or injurious effects upon the system, he was inclined to question, if not wholly doubt, any such influence, and concurred in the views advanced by Dr.
McQuillen, that he had yet to see the first case of alveolar abscess, ptyalism, etc., due to the presence of mercury in the amalgam.
Dr. J.M. McGrath testified for himself and for his father, who had had an amalgam experience of ten or fifteen years, that as yet "they had never seen any bad effects resulting, such as had been ascribed to its use by many practitioners."
Dr. Flagg says: "Thus it was that I was fortified by the combined testimony of gentlemen whom I could esteem as conscientious observers, and for whom I had much regard, both socially and professionally. It now remained for me to add the testimony of almost thirty years more of increasingly acute scrutiny (this book was written ten years ago), with the assertion that during all of my amalgam experience I have never seen one case of mercurial ptyalism, mercurial periostitis, mercurial necrosis, or of the slightest symptom which could reasonably be ascribed to mercurial action. I have had cases of asserted mercurialization brought to me by the score. I have treated them experimentally with chlorate of potassium to demonstrate its utter impotency, and have then cured every case without the use of any antimercurials and have left the teeth refilled with amalgam. If anything more convincing than this is required, I have it not to offer."
The President: I have before me a very elaborate series of experiments on "The Physical Properties and Physical Actions of Dental Amalgam," by E.A. Bogue, M.D., D.D.S., of New York, now known as Manhattan. if Dr. Bogue is present we should be very glad to hear from him.
Dr. Bogue: In the first place, the dentine of the tooth has a circulation like a vegetable, and only that; the cementum of the tooth has a circulation like bone; the enamel, I need scarcely say, is akin to crystal. It is plainly stated in "Wood's Therapeutics" that minute doses of mercury increase the weight and increase the number of red blood corpuscles. So far, therefore, from being detrimental, it would seem that a thirty eight years wearing of amalgam fillings ought to have helped him. Perhaps it is that that enabled him to work eighteen hours a day! I do not see that such a supposition on my part would not be quite as susceptible of proof as the assumptions of Dr. Tuthill's part that these neuroses of which he speaks arose from amalgam fillings.
Then as to the power of mercury from amalgam to penetrate into the system. In the first place, the amalgam filling should be a chemical combination. It should not be a mere loose mechanical mixture. If it be a chemical combination it is impossible to separate the mercury from the mass short of a heat very nearly approaching redness, excepting it be a dry-heat. I did go through a series of experiments, which I have looked over to-night for the first time in twenty years, and I am ashamed of their elementary character, but at that time in 1873 we knew very little of amalgam fillings. It so happened that two gentlemen then connected with Harvard University, and a third connected with the University of New Orleans, had written certain papers which were read and discussed. In the course of my experimentation I kept a whole handful of amalgam fillings at 100° F. for three months, in saliva, for the purpose of making not only the test as to whether it were possibe for mercury to be injurous systemically, but also for the purpose of finding out what the effects of certain chemicals were upon the teeth in connection with amalgam fillings. Perhaps, if I might be allowed, I will tell the reason that caused me to commence these experiments. A gentleman of great prominence in the now Greater New York placed his son in my hands for treatment and for a curious reason, as I supposed, declined to pay my bill. He sent him to some one else to have the amalgam fillings which I had put in taken out. This is history. It so happened I had not put any in. He then sent a letter from Dr. Metcalf, Professor of Theory and Practice at the College of Physicians and
Surgeons, New York, to me, with the statement that the probability was that his son was suffering from mercurialism from the presence of amalgam fillings. That boy had but one amalgam filling in his mouth, which had been there a number of years - a tiny thing, about as large as a pin's head. I replied to Dr. Metcalf that the boy was not suffering from mercurialization but from chronic dyspepsia due to his inability to masticate properly - rather a saucy thing to say to a Professor of
Theory and Practice. Dr. Metcalf took it kindly, however, and in a letter inquired of me whether it would not be possible for the emanations from amalgam fillings to produce systemic results.
Thinking the question easy to answer I laid it by to the next day, and the next week, and in fact it was unanswered for twelve months, all of which time it took me, besides four or five hundred dollars in cash, before I was able to satisfy myself with an answer to that question. Then came the analysis made by Professor Chandler of Columbia College, in which, as has been stated, he certifies that there was no mercury to be found in any of the bottles of saliva, which for three months had been kept at 100° F. and contained, as I said before, a handful of amalgam such as dentists use. That report was made just after a little extract from the Chicago Medical Journal for July, 1873, had been put into my hands, in which was an article by Dr. Paine, in which he speaks of "the poisoning of thousands of people all over the world from corrosive sublimate generated in the mouth from amalgam plugs in the teeth; neither cholera, smallpox, or any malarious disease doing more injury in the world than this poison." That is broader and stronger than any statement that has been made this evening, and it was in answer to that and to Dr. Metcalf's very kindly question that these experiments were undertaken. I would only add that it is quite possible to eliminate mercury from amalgam fillings when they are dry, but when they are under saliva, or under water it has not been found so in three months time.
Dr. F. H. Babcock:, I have been in practice for a number of years and have been looking for these cases of salivation. I saw last October a case that I thought was a typical one, but every filling in his mouth was gold. I saw another case only last month and that man did not have a singlc filIing in his mouth; so I hardly think that can be charged to the amalgam. The statement was made that amalgam fillings when removed are found to be bright on the side which comes in contact with the walls of
the cavity. I think you will find they are as perfectly oxidized there, or sulphuretted, as they are on the outside.
Dr. A. C. Brush: Mr. President, either mercury produces, when absorbed from the teeth, an entirely different clinical picture than when absorbed from the other parts of the system, or there is a discrepancy in Dr. TuthiIl's cases. As he read them off they reminded me more of miscellaneous cases of neurasthenia and hysteria than anything else, and the rapidity with which they changed their character from time to time; the variability of the symptoms and the extreme rapidity with which they got well, even after existing for years. A mercurial poison which has existed for years almost invariably produces a continuous tremor, due to the deposit in the nervous system and accompanying sclerosis. Had these cases lasted for so many years there would have been the production of some organic change there and the condition would not have cleared up so quickly. I think the last speaker is quite correct regarding the element of mind-cure. I think that was the potent element which produced the cure in those cases.
Dr. Tuthill: We all admit that there is a circulation in the teeth which may be the means of carrying the poison through the system, and this kept up for weeks, months, years, and decades, the system will feel the effect of this poison. I tell you, gentlemen, no one knows the direful consequences if he has not been there himself. Of course I am more interested in this subject, for it came near costing me my life.
I have often thought how the fathers in dentistry wrought well when they fought to the bitter end this subject of amalgam fillings; how they wrestled on the one side to prove it harmless, and on the other to expose its treachery and condemn its use. The struggle lasted from 1841 to 1847, when in the
New York Dental Society all who had not pledged themselves not to use amalgam were obliged to resign or were expelled. Those who had been the best of friends became bitter enemies. I hope that the same conscientious feeling which prevailed then will prevail again.
Dr. Brockaway.: I would like to say a word on that point. I think at present there is hardly a dentist in practice in the entire world but habitually uses amalgam; they have all overcome their prejudice to it. There is no more danger of that fight being renewed than of any other absurd thing.
Dr. Tuthill: I do not claim for this peculiar effect of mercury that you get salivation. There is no ptyalism present; I never saw it in one case, but, as I said in my paper, there is a peculiar action upon the nervous system. The theory that, recovery was due to mind-cure is too absurd for consideration in connection with the cases I have cited. I have seen people who would get well on that theory, but
I am sure that does not hold in these cases.
**********
GALVANISM GOLD AMALGAM AND THE HAHNEMANIAN THEORY
By R C GRANT M D
Read BEF0RE THE ROCHESTER DENTAL SOCIETY APRIL 8 1902
The Dental Digest, 8, 1902, 1110-1122
It seems to me the great mistake has been made by the gentlemen of your profession arraying themselves irrevocably on one side or the other for or against amalgam fillings; seeing on the one hand nothing that was bad or dangerous in them and on the other nothing but harm and suffering from their use. I do not suppose there are many to-day who would attempt to deny that a galvanic current may be and generally is produced where there are metallic fillings of different kinds in a mouth; that is, if a gold filling be placed in a mouth with amalgam fillings, the saliva acts as the exciting fluid and galvanic action occurs. If the secretions have become acid from decomposition of any particles of food that have adhered to the teeth, this galvanic current is greatly increased but even in the normal alkaline secretions it is readily detected.
Up to a certain point galvanism may produce a beneficial effect and by its stimulating property actually assist tissue growth or building, but if long continued the inevitable reaction, which pervades the whole domain of drug action, is sure to set in, and hyperesthesia and tissue degeneration occur, and we have that most deplorable of all patients, the neurasthenic. The galvanic current produced by the precence of gold and amalgam fillings in the same mouth may not be of sufficient intensity to produce this effect in all or in many cases but those who are susceptible to this kind of action will surely be affected, and the greater the susceptibility the more pronounced and lasting will be the symptoms. Then there is another effect which is produced by galvanism in the mouth that is still more serious.
One of the commonest elements found in the mouth is salt or sodium chlorid. This chemical combination is broken up by the electric current and the chlorin may form with the mercury of the amalgam chlorid of mercury, which is one of the most active forms of mercury known, and is a drug that has a cumulative effect in the system, so that the most minute quantity if repeatedly (not to say constantly) absorbed into the organism will be almost sure to exert in time a profound systemic poisoning. Then where there is a wearing surface of any size and number of amalgam fillings there must be some minute quantity of the metal worn away and of course absorbed by the system. Now do not imagine that I am insensible to the infinitesimal amount that this would be, but I mean to show later that the quantity has actually little to do with the effect produced; simply the susceptibility of the patient to the drug
Let me say here that the stock arguments against the theory of mercurial poisoning from amalgam and red rubber in the mouth are weak and unscientific. First it is said that there is only occasionally a man who fancies he sees these dire effects, where there are hundreds who do not. In answer I will say that the failure of any number of men through carelessness, lack of observation, or lack of opportunity to observe, to see these effects does not negative the facts that are seen and understood by even one honest observer.
Second. Salivation being a known symptom of mercurial pisoning, it is held to be a test, and the absence of salivation is a conclusive argument with these gentlemen that no mercurial absorption has taken place. Now be it known that salivation is only one symptom which may or may not be present, and is shown only in the poisoning by crude doses, except here and there a case where the patient is most susceptible to the action of mercury.
Third. It is claimed by the critics that the symptoms reported ar scarcely alike in any two cases, and are often at variance with the toxicological effect of mercury. Especially was this argument used by the editor of a dental journal in criticism of some cases reported by Dr. Tuthill of Brooklyn. I took the pains to compare the symptoms of those cases with the homeopathic provings of mercury, and found the pathogenesis of the drug to cover very nearly every symptom that he reported.
Furthermore, in poisoning by minute doses of any drug the symptoms produced will be modified by the idiosyncrasies of the patient, and no two victims will show the same set of symptoms.
I have referred repeatedly to the susceptibility of patients to drug action. This is a well known and indisputable fact and it is a further fact that one individual may resist disease action or drug action perfectly at one time and under certain conditious, and at another time or under other circumstances will succumb to the action of the same disease or to the same drug. It seems unnecessary to cite instances of extreme susceptibility, such as a well authenticated case of a lady who would become nauseated by even holding a bottle of ipecacuanha in the hand, experiments being tried in various ways and times to try to fool her, but in vain. We all know of people who will show violent symptoms of poisoning by being brought into near proximity to poison ivy, without in any way coming in contact with it except the emanations conveyed through the atmosphere.
Perhaps all of us have had cases of neurasthenia due to either galvanism or mercurial poisoning, that we relieved with more or less dispatch, and never realized the cause, for it is well known that if such patients relapse they are more likely to go to a new physician than back to the old one. Again there are others who may have been convinced in their own minds that the cause of the suffering was the fillings in the teeth, but who could not bring conviction to the mind of the patient with sufficient force to induce him to have the fillings removed, and so to prove or disprove the diagnosis.
Doubtless the methods of "proving" drugs and recording symptoms for the building up of the homeopathic materia medica is familiar to you all. Suffice it to say, that the homeopathist knows nothing of the value of a drug for therapeutic use except as he has learned of its action upon people in health. In order to get at the whole pathogenesis of a drug many provings are made on scores of observers, using doses ranging from the largest that can be borne by the system without fatal effect to the most minute doses possible to conceive, and it is an incontrovertable fact that the smallest doses will always bring out the greatest number of symptoms and the subtIest effects. This is a fact that has been observed by all of the best men of our school of medicine for the past hundred years, and it is not in dispute.
This, then, will account for the great variety of symptoms, and the lack of the grosser or cruder ones, in the cases of mercurial poisoning that have been so frequently reported by dentists and physicians. It is generally conceded by the masters in homeopathic materia medica that comparatively few people make good provers because of their lack of susceptibility to or observance of the symptoms produced by any except the crudest doses. I leave you to make the application of this fact to the question in hand
Personally I have observed but few cases where I felt sure the mercury in the mouth was very harmful to the patient, but I have observed repeatedly the peculiar mercury tongue - broad, flabby, with indented edges from the imprint of the teeth - in patients with amalgam fillings, and if this is a fact there are doubtless many other conditions which I should have attributed to this cause. In my own case I suffered for years with bleeding gums, which symptom disappeared on the removal of the amalgam fillings. There is a physician in the Hahnemann Society who had a case of typical skin disease which failed to yield to any other treatment, but got well after the removal of amalgam fillings from the teeth. But cases of this kind have been reported so frequently that it is unnecessary to multiply instances and unfair to deny their existence.
To sum up, if my postulates are accepted the deductions would be that there may be and frequently are patients who cannot bear amalgam fillings without great mental and physical sufferings; that there are many who carry them with impunity because of their lack of susceptibility; that no man can possibly tell before trial who can and who can not bear them; that it is far better where gold or bone fillings can be employed to never use the amalgam; but in those cases where nothing else will answer, either from the condition of the teeth or the financial aspect of the question, and amalgam is used, to be open-minded and fair and ready to acknowledge the deleterious effects of the same upon the system, if they should unfortunately appear, and remove the offending substance gracefully, graciously and without excuse or apology.
Discussion.
Dr. C.H. Nicholson read the following letter from Dr. S.B. Palmer: Gentlemen of the Rochester
Dental Society: It will be impossible for me to meet with you this evening. Not knowing the views that Dr. Grant may present, I cannot intelligently discuss his paper, so will give my own methods of practice, with the reasons therefor. The greatest trouble with amalgam fillings is occasioned by the galvanic action upon the exposed surfaces of the filling and those in contact with the dentin. Unlike single metals such as gold, tin, lead etc., amalgam is composed of an alloy and mercury. That is, the alloy is united or soldered by mercury, and presents minute elements both positive and negative. For this reason, amalgam fillings are never briht when in contact with the dentin, unless heavy varnish has been used before the plug was inserted.
Here we see a lesson relating to two conditions - one concerning the dentin, and the other the quality of the alloy. Oxidation tends to increase the size of the plug as rust does iron. Nornal dentin furnishes less moisture to increase circulation or cbemical action, and the density of the dentin confines the oxid, so amalgam fillings become cemented to the walls of the cavity. To increase oxidation, copper is used in alloys, giving better results in poorly calcified teeth, such as the deciduous set and the first molars. I rarely use copper in an alloy, but depend upon varnish as cement. Tbe latter is best for devitalized and badly decayed teeth, because it prevents galvanic action upon the surface of the plug, and at the same time fills the tubuli better than the oxid.
The next point to be considered is the location of amalgam fillings, either in conjunction with gold, or even with a filling of the same material. Not only when the plugs are in absolute contact in the same tooth or cavity, but in approximate cavities which represent two distinct conditions. It is safe and good practice to use gold and amalgam in conjunction, that is, to add amalgam to an old gold filling or vice versa, or to use amalgam for a guard filling at the gingival border. The effect is to oxidize the amalgam to such an extent that the local elements as already mentioned, consisting of alloy and mercury are obliterated. The amalgam surface is always black and smooth where exposed.
In short, the positive plate in the battery becomes polarized and no current passes into the dentin.
This is not so with approximate fillings, for after every precaution has been taken to avoid it, a galvanic current will be generated where a gold and amalgam filling are in close proximity.
The following authorative statement gives the amperage, or force of currents between the plates, relative to the distance of their separation - "The quantity of electricity traversing an acid solution of uniform strength varies inversely as the square root of the distance between the plates. The distance varying from four to one, the current will be as one to two. Thus it will be seen that very small exciting surfaces may produce vigorous chemical action when the distance between them is but trifling."
The most marked disturbances are noticed when a tooth thus filled has approached its approximate, until in masticaton or on becoming loosened the two fillings come in contact. Thus there is established a "make-and-break" current. The amalgam is the positive element from which the current enters into the gold. Should the dentine under the gold prove a conductor, the pulp manifests the presence of a circuit. Tbe remedy is to remove the most objectionable filling and replace with gutta-percha, perhaps temporarily. When both fillings can be made with gold all will be well. Some of our younger members may learn by experience that when a fresh amalgam filling is placed adjacent to one of years' standing, like effects upon the pulps are produced, though in less severe form.
I have had two cases for removal of fillings within a few months from the cause already mentioned. All new amalgam fillings undergo vigorous electric excitement from galvanic action occasioned by the elements of alloy and mercury. This excitement subsides when the surface by oxidation blends or polarizes the elements. At first an amalgam plug is in much the same condition as a filling of zinc would be, and we all know that a zinc plug would not be tolerated. It is well to use heavy varnish, or cement upon a coating of thin varnish, before inserting the filling.
The next disturbance is doubtless familiar to all, namely that caused by amalgam fillings coming in contact with gold crowns, especially when the latter are used as a support for a bridge. One case will illustrate the principle. About five years ago a man consulted me regarding alarming symptoms supposed to arise from facial neuralgia, which extended to the shoulder and down the arm. An examination showed the cause to be an amalgam filling in the superior third molar. The second molar was capped with gold and supported a bridge carrying three or four crowns. Wedging was necessary to make the filling accessible, so a thin, wide strip of rubber was drawn between the filling and crown and the patient instructed to return the next day. A cure was effected over night by the separation. The amalgam filling was removed and gutta-percha inserted, and no further trouble has ensued. In this case I do not hold the amalgam responsible for any pathological influence, other than an element that aided in generating an electric current. Two other cases have been relieved. The first, incipient deafness, was due to a second molar which seemed too remote to be considered. It had been filled with amalgam many years before. Removal of the fiIling showed the pulp chamber to be full of odorous septic matter. The tooth was treated, refilled, and hearing was restored. The second case presented symptoms of paralysis of neck and sholder. About the same conditions existed, and the same line of treatment was carried out. The tooth is still giving service and there is no more paralysis.
I am convinced that some patients are more susceptible to mercurial influences than the profession realize. Before drawing conclusions I always consider well the objection to amalgam as given by the patient. I remove amalgam fillings occasionally for the possible benefit of a patient, and generally find it the right thing to do. Complaint of a metallic taste in the mouth by patients who have amalgam fillings leads me to remove all the possible causes of such taste. While I am not prepared to believe as fully in the theory of Hahnemann as a late friend of mine, who believed that if mercury were hermetically sealed in a glass tube and carried in the pocket, it would affect the individual, there are grounds for believing that amalgam causes more injuries than general practitioners credit.
Discussion.
Dr. F.W. Proseus, Rochester: There is one thing upon which we all agree, and that is that amalgam does in some patients and under some circumstances give rise to widely varying troublesome symptoms. From my own experience, if two differeat metals are in a mouth I am certain that a galvanic current is set up which might affect the health, beside tending toward the destruction of the fillings themselves and the dentin where in contact with the fillings. I had a patient who complained of a constant metallic taste in her mouth, and pericementitis. Dr C. a homeopathic physician told the lady that the trouble was caused by the presence of amalgam fillings in her teeth. I objected to removing the fillings, but finally did replace the larger ones with gold, and the metallic taste and other trouble immediately ceased. Dr. C. charged the trouble to the mercury overlooking the galvanic action. Another case was a gentleman had recently had a bridge inserted. There was a very old amalgam filling in one tooth, and his teeth became so sore that he could not bring them together.
The filling was replaced with red gutta-percha and the soreness disappeared. A somewhat similar case was reported at the Columbian Dental Congress.
Dentists recognize that these troubles do occur, and as the homeopathic school teaches that if you get an action from a drug when a large dose is administered, it will also produce an effect if the dose is small, we must allow that if gold and amalgam are present in the same mouth there will be galvanic action which will eliminate a certain amount of mercury. In many cases sufficient will be set free to constitute the homeopathic dose. Dr Palmer says that a new amalgam filling will cause more of this galvanic action while it is bright and clean than after it becomes tarnished. For this reason it would probably be safer to use an amalgam that will tarnish quickly and thus limit this action. Dr Palmer has been studying amalgams for forty years and his experience should be received with respect. I think we will have to admit that such results are possible, and when we receive complaints from homeopathic physicians we should treat them courteously and remove the fillings.
Dr. J.H. Beebe, Rochester: Many present remember the antipathy to amalgam which my old partner,
Dr. Walter, had for so many years. The origin of his feeling arose in this way. He was doing some work for a homeopathic physician who, observing him cough frequently, pronounced it an amalgam cough, and told him to remove the amalgam fillings from his mouth and he would be rid of it. The fillings were removed and the cough left him. After that he used no more amalgam in his practice. The difference is in the people. Some will be affected by the presence of amalgam and others will not, and no one can tell until it is proven, who will feel it.
Let me read an extract from a letter from Dr. Barrett to Dr. Walter, written in 1888 - "You ask me why certain effects of nercury are sometimes seen in patients. Mercury is, with few exceptions, the most powerful of the metallic poisons. Its toxicological possibilities are wonderful. Combinations with other substances develop characteristics that are amazing. Analogous combinations develop the most diverse substances. For instance mercurous chlorid (Hg2 Cl2) is calomel, which is largely used as a medicine and is a very effective cathartic. Mercuric chloride (Hg Cl2) is corrosive sublimate, a poison so virulent that it has given its name to a whole class of toxicological agents, Now there is only this difference between the two substances - one proportion of mercury. In the mouth we meet with all manner of substances that are under the most favorable conditions for uniting with the mercury if it is present. The combinations of mercury are very unstable, and under the influence of heat, any free mercury especially is readily sublimated. So here we have, if mercury be present in the mouth, all the conditions that might form deleterious compounds. That free mercury is inert, as has been frequently asserted, is not so, for we all know what are the dangers to which workers in mercury, especially in the mines, are liable. Some persons are exceptionally sensitive to the action of mercury as some are to every poisonous article. Some will handle Rhus Tox (Poison ivy) without harm, others are violently affected by the merest contact.
About the use of mercury in the mouth, I believe it is too powerful an agent to be used without the most extreme care. Most persons will not be affected by a moderate amount of amalgam fillings, while others cannot bear even one such filling. It may be used in moderate amount in most cases, but the dentist should exercise care. Its effects, so far as I am aware, are constitutional and not very often local. It produces its characteristic periosteal effects in the mouth and upon the mucous membrane.
You know what they are. There may be cases where it produces local irritation and soreness, but I have never seen one in which the difficulty could not properly be attributed to something else.
Pharyngeal and laryngeal complications are quite possible. I have under treatment now a patient the most of whose teeth are well filled with gold but in some locations amalgam was inserted. In every one of the teeth so filled there is periosteal trouble and there has been ever since they were so filled.
Periosteal difficulty about the roots of the teeth in mouths in which there is a great deal of amalgam is often seen, as indicated by painless swellings of a hard character opposite the roots (indurations) which gradually increase, and unless the amalgam is removed will result in necrosis. You may ask why I ever use it. Chloroform and other anesthetics are useful in their way, but I would not use them
indiscriminately to everyone without examination. Chloroform and amalgam are both of great service if judiciously employed, but either is capable of great mischief if given to the wrong person."
Extract from a letter from one of Dr. Walter's patients - "I thank you for the comfort I now have.
You may remember my mentioning that in winter time I was troubled with eczema in the calf of my leg. Since the extraction of the soft fillings it has entirely disappeared."
Dr. Walter once said, "One of the most remarkable cases of mercurial action, not on the system, but on gold placed in close comtiguity to a large amalgam filling, was that seen in the mouth of C.M.W.
I placed a gold crown on a second lower right bicuspid, said crown being simply rolled from an
English crown piece, consequently 22K fine. Immediately in the rear of the crown was a large amalgam filling which composed the crown of the sixth year molar. Six months after the gold crown was set it commenced to turn dark, until it was the color of oxidized silver and nearly as black as the amalgam filling itself. I removed the amalgam and there has been no indication of a return of the color.
Another case: Rev. Dr. R. came to Dr. Walter some time in August 1888. Had been suffering for years, complained of dizziness and swimming vision. The least excitement caused "a darting up in front of face." Had for five years been unfitted for his profession. He was in the office Dec. 20,
1888, and mentioned voluntarily that he had not been so well in years. He would not say that it as the removal of the five amalgam fillings that had caused his convalescence, but he was certainly better and the mending commenced soon after the fillings were removed. Eyes at the former date had an uncertain and vague expression which had entirely disappeared.
Dr. Walter also had recorded cases of neuralgia, eye and throat trouble, and pimples on the face, which had been cured by the removal of amalgam fillings, the neuralgia in an hour.
Many think because the mercury is closely combined with the other metals in an amalgam that it can have no action on the system. I argued this way with a dentist who told me that at one time a patient, instead of spitting out a number of particles which became detached from an amalgam filling as he was inserting it, swallowed them, and next day had an active diarrhea. The dentist did not believe it was the mercury that affected him, however, but thought it was the irritation set up by the rough and sharp particles of metal. The same amount of sand would not have had the same effect. Amalgam does often have a deleterious effect on the system, and many patients have been benefitted by the removal of fillings. People of exceedingly nervous organisms are peculiarly susceptible.
Dr. W.W. Coon, Alfred: The coloring matter in base plate gutta- percha is red oxid of mercury, a preparation which is much more likely to be harmful than amalgam. Don't you use gutta percha?
Dr. Beebe: The coloring matter in red base plate gutta-percha is Armenian bole, an earth composed largely of oxid of iron, and even if it were sulphid of mercury we would get less mercury than from amalgam.
Dr. Johnson: Dr. Palmer struck the key-note in galvanic action, but failed to note the vital point.
The galvanic action breaks up mercury and forms oxid of mercury, which is a soluble salt and a powerful poison. When the fillngs are near each other in the mouth the effect is greater and more apt to affect the patient. I am not a crank on this subject, in fact, I have amalgam fillings in my own mouth, but I have had patients who suffered from their presence, also those who suffered from the wearing of red rubber plates. Some reported cases are hard to credit, such as the cure of a longstanding neuralgia in an hour by the removal of amalgam fillings. To report such a case lays the man open to the suspicion of being a crank, and brings up the idea of suggestive therapeutics, but in other cases the idea of cure by suggestion was not admissible.
Dr. Haydon: A lady of forty-five came to my office. She was under electro-magnetic treatment and had all the amalgam fillings removed to relieve her of a ringing in the ears, but it did not improve after their removal.
Dr. H.L. Belcher, Buffalo: A friend of mine had a metallic taste in his mouth which was caused by galvanic action between two gold fillings.
Dr. W.W. Belcher, Rochester: If the keynote of the situation is as Dr. Johnson states, that the soluble salt of mercury is released by galvanic action, it would eliminate all fear of danger when there were only amalgam fillings in the mouth. Some people have idiosyncracies and may be acted upon unfavorably by substances perfectly harmless to the vast majority of mankind. Some cannot eat strawberries, and I know a lady who is made violently ill if she eats the least bit of an apple, although she is exceedingly fond of them. Such persons would have only to look at amalgam to suffer from mercurial poisonings, and the removal of amalgam fillings from their mouths would probably cure them of almost anything.
Dr. G. Goode, Rochester: Mercury in alloys is in a chemical combination and not readily separable.
Dr. Black taught us that the change of form in amalgam fillings always, always thought to be due to oxidation, was due to flow of the amalgam or what is commonly called "stress". The amalgam is possibly changed by changing the chemical composition of the filling, and this change may drive the mercury to the side of the filling and thus allow of its escape.
Dr. Beebe: Amalgams, as any alloys made by a mixture of two or more metals in definite proportions, are mechanical combinations, but all amalgams are not alike, therefore galvanic action would be produced in a mouth having only amalgam fillings.
Dr. C.H. Nicholson, Rochester: I do not believe amalgam is a chemical compound, but simply a mechanical mixture, and mercury may be freed from it under certain conditions. That galvanic action may change mercury from the metallic state to a salt may be granted, but I do not believe it can be demonstrated, and if it does so, the amount of mercury so thrown into the system would not be sufficient to affect it. Those brought up in the homeopathic school no doubt think so, but the idiosyncrasy of the patient would explain any supposed effect in perhaps every case. I believe in the effect of suggestive therapeutics. A young man came to me with severe neuralgic pains in the side of his face, which he supposed were from a tooth he pointed out, which had an amalgam filling. This filling was removed but the tooth was found to be in good condition and the cavity was filled with gutta- percha. The neuralgia left him for a time, but after a few weeks he returned with the same trouble and this time he thought it was from the next tooth. This was opened up and found to contain a pulp stone. A cure of the neuralgia followed as before, but twice more it returned and the last time
I only pretended to do something to the tooth and discharged the patient. Some time afterwards a hypnotist was giving an exposition, and this same patient was made the subject and proved to be yery easily brought under hypnotic influence. At the end of the seance he suddenly had a severe attack of the neuralgia and called to me for help. I told the hypnotist that the man had no toothache or other pain but thought he had, and asked him to treat him by suggestion. He was thrown into a hypnotic sleep and told that the trouble and pain had left him, and when he awoke he was all right.
Amalgam has been used more than any other filling material, and with most excellent results in saving the teeth and building up the health of the patients, and unless there is a rare case where we know there is an idiosyncrasy against it, we should not hesitate to use it.
Dr. M. Rosenberg (M.D.): I do not believe that mercury could produce any poisonous effect in quantities so infinitesimal as would be derived from amalgam fillings in the mouth. I frequently precribe mercury and never get the results from much larger doses than are described in these cases.
The human system will withstand the action of poisons and eliminate them when in small quantities.
The galvanic current theoretically will produce chemical changes, but the current must be used in definite amounts, and that generated in the mouth would be too slight to produce appreciable results.
Dr I.C. Edington, Rochester: There is one phase of the subject that has not been considered. I had a patient who complained of neuralgia and metallic taste in her mouth from the effect of amalgam fillings. I replaced these with gold fillings and gold crowns. Some months later she returned complaining again of the metallic taste and suggesting that pure gold had not been used. I consulted
Dr. Palmer and he said galvanic action was possible between different qualities of gold. She had two or three 22K gold crowns soldered with somewhat lower carat and the fillings were of course pure gold. I concluded nothing could be done and the metallic taste continued, though it was not as bad as it was when the amalgam was present.
***********
SOME THINGS DENTISTS KNOW LITTLE ABOUT
M.A. Morrison, D.D.S., PETERBORO, ONT.
Dominion Dental Journal, 14, 1902, 84-93.
Read before the Ontario Dental Society, February 19th, 1902
Mr President and Gentlemen. No individual man or body of men are expected to know everything, not even all connected with their own particular caling or profession. But at the same time there are often things we neglect fo know because it may cause an effort or even a struggle to gain that knowledge, and in this paper I wish to call up a few things pertaining to the study and practice of dentistry that we as dentists appear to know little about.
I. Heredity, and its Relation to Diseases of the Dental Organs. - The American System of Dentistry says: "Through the law of inheritance, the teeth are the unfortunate recipients of a legacy of disease in many forms, the tendency of which is to intensify in the course of transmission." Dr. Williams, in a most excellent paper on "Pathology of Enamel," said: " I Believe that if the environing conditions of the teeth are such as to favor the development and activity of acid-producing bacteria, and if those bacteria are permitted to become attached to the surface of the enamel, it is doomed, although it may be the most perfect that was ever formed. On the other hand, if those environing conditions are not present, the worst enamel will not decay." And I think we have all accepted Dr. Williams' theory. If, then, we place these two statements side by side, and make the one conform to the other, where are we at? What has heredity to do with caries of the teeth? Or what part does it perform in forming that environment? It may be one of the greatest enemies of the human teeth. .....
2. Electric Circuits of the Oral Cavity. - We are just in the shallow waters of the great ocean of electric knowledge, but one of these days a great wave will carry us far seaward and we will all be our own wireless telegraphic station, central telephone office and dynamo combined. For the late Dr.
Relyea tells us that by wearing a partial aluminum upper denture and the metal articulating with a gold crown on lower molar so far as he himself was concerned he could regulate the electric lights of the town of Oswego. In other words, he generated such a current that it affected the optic nerve even to blindness. Our own experience is not so marked as that of the Doctor. But on one occasion where
I adjusted a gold cap, it occluded with a large amalgam filling. When the patient closed the teeth she got shock enough to cause severe pain. I gave her relief by grinding the amalgam filling so that there was no point of contact between the two metals. I also filled with gold mesial surface of first sup. bicuspid. There was already an amalgam filling in distal side of cuspid. When fillings were polished and separated and dam removed they came almost in contact. At once the patiet received severe electric shock, almost unbearable. I wedged the teeth, bringing fillings in contact when current ceased and no further trouble. These examples demonstrate that there are strong electric currents generated in the mouth. Do they affect our fillings? Our crowns? The nerves of the teeth they pass through, or the general health of the patient? In short, do we know what kind of a battery we are making when we have such an aggregation of metals as gold, silver, tin, copper, mercury, varbon, etc., all immersed in the acids of the saliva. It may be, gentlemen, that when we understand the electric currents of the mouth we will have solved many of the obscure things of dental science.
3. Amalgam, and its Relation to the Generral Health of the Body. - Amalgam is the most used and, I might add here, the most abuscd of the filling materials we have. Thousands of ounces of it are used every day, and many are the people that are lauding it as the preserver of their teeth and deliverer from pain. While some are calling the judgement of the gods upon it as the destroyer of their bodily health. We have had from time to time published in our journals instances of men and women who had been in ill health, and on removal of some amalgam fillings recovered their health. We have had it in our own practice and under our own observation.
Amalgam är det mest brukade och, kan man tillägga, det mest missbrukade, av de fyllningsmaterial vi har. Tusentals uns av det används varje dag och många är de personer som hyllar det som bevarare av deras tänder och som räddare från smärta. Andra däremot nedkallar gudarnas dom över det som förstörare av deras hälsa. ..... Jag talar enbart om silver amalgam. Vi kan ha våra egna ideer och åsikter i denna fråga, men kan vi stötta dem med goda auktoriteter? Detta är en fråga som kåren som yrkesområde har glömt. (M.A. Morrison, DDS, Peterboro', Ontario, 1902)
A lady was taken ill, treated by local physicians for several weeks without any improvement, went to an American sanatorium, was under care of several eminent doctors who treated her for general debility, then chronic indigestion for three or four months, also without improvement. Her friends then called in another physician who made a thorough examination, and finally diagnosed the case as systemic poisoning due to several amalgam fillings in her teeth. He ordered these replaced by other fillings which was done by gold and cement at a cost of $6o to patient, and the lady immediately began to get well aud made marked improvement in a few months, and after two years is comparatively well.
Another lady had me remove her amalgam fillings and put in gold because she was in poor bealth.
Needless to say, she got well at once. Are these cases of hysteria? Are they idiosyncrasies? Or are we putting into the teeth of our patients that which will cause some of them ill-health and probably death? Is it possible for a poisonous compound to be formed from a combination of the saliva and the amalgam without causing any disintegration of the filling? I am speaking entirely of silver amalgam. We may have our own ideas and beliefs on this question, but can we back them up by good authority? It is a question that the profession as a profession has overlooked.
DISCUSSION
G. M. Hermiston, B.A., D.D.S., Picton:
Dr. Miller, of Berlin, says there are electric currents in the mouth wherever there are teeth in which metallic fillings have been inserted, but unlike Dr. Palmer, of Syracuse, he does not think this current exits in such a way between the fillings and the tooth substance that the dentine could in any way be compared to the generating plate of a galvanic cell. If this be true, there can be no destruction of dentine substances underneath the filling material. The only possible dissolution of tooth substance would be at the margin of the filling, where the acids which are set free by these currents, electrolytically decomposing the liquids of the mouth, are deposited on the surface of the electro-positive metal and attacks the enamel at its margin. This action, even in the most marked cases is very slight, and ceases as soon as the surface of the electro-positive metal becomes oxidized.
Practically such effect is nil. These currents would hardly be produced were all metallic fillings homogeneous, but will be produced on the surface of every metallic filling even if of pure gold, provided the filling has not the same density throughout, and the current always flows in the direction of least resistance, that is, from the denser to the less dense parts of the filling. Bearing in mind the direction of these currents, their injurious effects must be at the minimum, since few of them would tend toward the margin of the filling.
There are three conditions, says Dr. Miller, when these currents may be produced: (a) When fillings have not the same density throughout; (b) When two fillings of different metals touch either in the same or adjacent teeth; (c) When a plate is composed of different alloys. He further says that since dentin is a non-conductor of electricity, these currents between a filling and the tooth substance can have only an imaginary existence.
3. AmaIgam, and its Relation to the General Health
I am quite ready to admit that amalgam is very much abused as a filling material but I am not so easily convinced that it has or does produce any injurious effects upon the human system. The ordinary amalgam filling contains silver, tin, perhaps a little gold, a little platinum, or a little copper.
Any one of these metals in the amount in which which we find it in patients teeth could in no way affect the patient's health. To what, then, can we ascribe any ill effects, if ill effects are any? It must be to the mercury alone. Authors, with unqualified assertion, state that mercury in the metallic condition is nonpoisonous, in fact has no therapeutic action on the human system, and that it is only in the form of vapor that its ill effects are produced. In a hardened metal filling there is no free mercury; all of this metal is in combination with the other metals of the alloy. In this condition, then, the mercury can do no harm. The condition of vaporized mercury is never attained in the human mouth. This would be absurd as mercury requires a little over 6oo degrees F. to sublime. Burchard says: "Amalgam fillings in contact with dentine in which putrefaction is in progress are frequently discolored by the formation of, presumably black sulphide of silver and perhaps salts of mercury, the dentine being stained black." Presuming that such were true, if the filling were to be removed and the disintegrating dentine thoroughly excavated, and a new and perfect amalgam filling inserted, would not the patient's health be ensured just as certainly as though we had inserted gold? When we meet with such cases of supposed mercurial poisoning are we not justified in concluding that they are hallucinations rather than idiosyncrasies? Hallucinations that, to the operator are a financial success, and yet such as we should seek, if possible, to dispel if we are to act honestly with our patients.
Were we to attempt to account for all the hallucinations - for such we prefer to call them - of humanity, we would have a neverending task. There are cases on record where diseases of prolonged duration have suddenly cured as if by magic. We cannot doubt the cure, but are inclined to think that the disease was wrongly diagnosed and that the disturbance was in the gray matter rather than in some of the other organs.
*********
THE INFLUENCE OF AMALGAM FILLINGS AND RED RUBBER PLATES UPON THE
ORIGIN AND GROWTH OF TUMORS Howard Crutcher, M.D. Chicago. Hahnemannian
Advocate, Chicago 35:8 1896 489-91 (Med. Adv., St. Louis)
In common with other writers, I have often directed attention to the pernicious effects of amalgam fillings. That they produce violent and intractable neuralgias, irregularities of vision, pernicious stomatitis, chronic saIivation, dyspepsia and melancholia, I have demonstrated beyond the shadow of doubt in repeated instances. I now report a case of a woman of thirty-three who had an aggravated nocturnal cough which had resisted all methods of tretment and a journey to the Rocky Mountains, and which was relieved at once and for all by the removal of a solitary "silver" filling which had been worn for six years.
In April of the present year, a man of forty-one came to consult me concerning a troublesome "ulcer" of the tongue. There was no syphilitic history, and no traces of tuberculosis or of cancer in his family. I told the patient that he was suffering from an epithelioma and this opinion was confirmed by two skilful surgeons of St. Louis who examined the case before it came into my hands. The growth had appeared three months before I saw it, and was abont the size of a silver dime, although not of regular outline. It was located on tbe right superior surface of the tongue, overlapping the border of the margin almost three quarters of an inch from the tip. A request for a microscopic section led to a firm refusal. The patient talked of the "cancer" continually and seemed to think that the epithelioma was a polite way of reading his death warrant to him.
There was no infection of the surrounding glands, so far as I could judge. For several years a red rubber plate had been worn. I advised its instant removal and gave order on the removal of some amalgam fillings occupying the molars. My directions were carried out without delay....and in June no traces of the growth could be detected. I think that the growth was an epithelioma; that it was produced by the red rubber plate; and that its cure would not have been possible without the removal of that dangerous appliance.
This opinion is expressed with increased confidence since the appearance of the last volume of
Dennis' System of Surgery (New York and Philadelphia, Lea Brothers & Company, l896), wherein is narrated a most interesting case (page 20, vol. 4), of epithelioma of the mouth resulting from the wearing of a red rubber plate. The report is as follows:
"Another patient suffered from an ulcer in the mouth, which proved, upon microscopical examination, to be an epithelioma. The submaxillary and sublingual salivary glands were infected.
The epithelioma with the glands were removed. The history revealed the interesting clinical fact that the patient had worn a red rubber plate of false teeth for many months. The question naturally arises in connection with this case as with similar ones: Did the red rubber plate cause the development of epithelioma? ... While the red rubber is not a cause of epithelioma, yet this material produces a longcontinued irritation which devitalizes and deteriorates the tissues, and thus produces a soil favorable by mal-nutrition and by lowered vitality to the development of carcinoma. At all events, it is not apt to occur in the mouth of a patient who uses a good plate. The question of mechanical friction must not be overlooked, though it is a notable fact that rarely if ever has an epithelioma been observed in a patient who wears a gold or aluminum plate."
The plate, then, does not of itself cause trouble, as a rule; it is therefore the material composing the plate that produces the irritation; it would seem to follow, if the rules of logic are to be adhered to, that the mercury in the plate is to blame for the disturbance. I do not see how any other conclusion is possible. It is earnestly hoped that this signal illustration from so eminent an authority will not be lost.
Mr. Sutton (Tumors, Innocent and Malignant, by J. Bland Sutton, Lea Bros. & Co., 1893), does not mention the red rubber plate as a factor in the causation of tumors.
Prof. Gross, whose Monumental Work on Surgery will endure as tbe pride of succeeding generations of Americans, has this to say concerning the influence of mercury (System of Surgery,
1882, vol. 1, p. 83):
"There are certain persons who, from idiosyncrasy, or the former use of mercury, cannot take this medicine, even in the smallest quantity, without being violently salivated."
The American Text-Book of Surgery says that "Mercurial Stomatitis and Mercurial Glossitis are not uncommon in the trades in which mercury is used," etc.
I find no other specific references than the one given from Dennis, but the testimony on this point is piling up high enough to command the thoughtful attention of pathologists. Certain dentists are themselves aware of the popular dread of mercury and hence the false term of "silver filling", which is a deliberate swindle and a disgrace to the dental occupation. Many honorable dentists have told me that they always advice against the use of mercury in any form in the mouth, but there are hundreds who are too stupid or too dishonest to abandon a practice which is profitable only to themselves.
It is not claimed that mercury worn in the mouth is universally detrimental to health; my own experience, which includes hundreds of observations, leads to the conclusion that injurious effects are detected in only a small per cent of those who wear red rubber and "silver" fillings. But the exceptions are frequent, and the results are no doubt often disastrous - so disastrous, in fact, as to warrant the absolute and unqualified condemnation of the practice.
THE HAZARDS OF MERCURY VAPOR
Alfred Stock
Kaiser-Wilhelm-Institut für Chemie, Berlin-Dahlem
Zeitschrift für angewandte Chemie vol. 39, 1926, 461-466
(Die Gefährlichkeit des Quecksilberdampfes)
When I decide to tell a wider audience everything about personal troubles, which in themselves do not concern others and therefore should not be worth publishing, it is because of an intense wish to spare others, who have anything to do with metallic mercury, the very bad experiences which have destroyed a major part of my life and to very emphatically warn against the volatile metal. I can freely tell about it today since it is fortunately enough in the past and a terminated matter.
The insidious dangers of mercury are not sufficiently known and are too little noticed just in the places where people are especially threatened, that is in the chemical and physical laboratories.
For nearly 25 years I experienced symptoms, in the beginning only weak and occasional, in time increasing up to being unbearable and which caused me to doubt if I could continue my scientific work. The cause was not known to me or to any of of many excellent doctors I visited to ask for advice. It was considered possible that my problems were caused by an especially narrow nasal passage and an unusual sensitivity of the nasal mucosa. My nose was therefore treated for decades by etching, burning, massage, electricity and bloody operations. Without results! Two years ago something happened - a few of my collaborators fell ill with similar symptoms - and it was revealed that the cause was an insidious mercury intoxication. Because of my chemical work; the study of volatile compounds with vacuum technique using vessels with mercury, mercury pumps, manometers and valves, I was for 25 years in constant contact with mercury.
It is not possible to doubt the casual connection since all symptoms, even if not yet completely, have disappeared (and a short time ago clearly reappeared when I for some time worked in mercurycontaining air because of a mishap with the ventilation of my laboratory) when I, for two years have protected myself from inhalation of mercury vapor.
I will give an account of my symptoms and how they developed with time. They agree, even in detail, with all insidious mercury vapor poisonings, something my collaborators and other chemists could confirm. They were and are, largely unknowingly, victims of mercury vapor poisoning and do not know the source of their troubles. Many essential symptoms have, until now, not been sufficiently described and the insidious mercury vapor poisoning has not received the attention it deserves.
The matter started with me as periodically occurring light headaches and weak dizziness which increased with the years to continous, nervous unrest and irritability, to a pressure on my head which made thinking difficult, to ever increasing headache, finally almost continous and tormenting
(mostly over the eyes), to intense vertigo which was connected with troubles of vision (dim and double vision). Soon also the upper airways were affected; in the beginning light an occasional nasal catarrh, then permanently tight nose, later almost continous catarrhs of the olfactory mucosa with often bloody mucus production and crust formation, violent throat inflammations and pains in my ears connected with impaired hearing and smell (for some substances like hydrogen cyanide it remained), distaste for tobacco smoke.
In the last years before the cause was recognized, other symptoms appeared: salivation, sour-stale taste in my mouth, eye inflammation, inflammation of the oral mucosa, vesicles and sensitive and ulcerating spots on my tongue, gums, gingiva, insides of lips and cheeks, redness of gums and slight bleeding during toothbrushing, toothache, withdrawal of gingiva from teeth and the appearance of pockets, occasional loose, single teeth. The mouth and teeth changes occurred late with me (the peak of these symptoms did not occur until months after the poisoning had been discovered) since I from childhood had been careful with my mouth hygiene (for instance every evening prolonged rinsing with 1.5 % hydrogen peroxide solution and then with sodium bicarbonate). If this had not been the case I might have discovered the cause of the symptoms earlier because of the mouth inflammations.
Further symptoms were: intellectual exhaustion and depression, lack of energy and ability for work, especially intellectual work, increased need for sleep, trembling of my stretched fingers, often also my eyelids, pains in various places, stabbing pains in my back and in limbs, pressure around the liver, sudden need for urination and diarrheas without special reasons. Slight vesicles on the inner sides of my arms and on the upper half of my legs.
The manifestation which was most severe for a person with intellectual work was the loss of memory. My originally very good memory got worse and worse so that I, two years ago, was near total amnesia. Only with the help of extensive notes and with considerable effort was it possible to write a paper or to hold a lecture. I would forget the phone number on my way from the telephone directory to the telephone; I would forget almost everything I had learnt by heart, the contents of books and theatre plays I had recently read and seen, the contents of my own papers I had published.
It was impossible for me to remember numbers or names. Often I could not remember the names of close friends. Especially the ability to calculate, to do matemathical thinking, also to play chess, was severely affected. The depressed ability to remember and the difficulties in calculating seem to be a special sign of insidious mercury vapor poisoning. This was also evident with my collaborators and with other persons, for a long time exposed to mercury vapors, cases which have now become known to me. Shortly after we had discovered what was wrong, I and two collaborators were trying to finish writing a paper which needed calculations. None of us had the ability to add 10-20 large numbers without errors!
In contrast to only a small effect on bodily strength, for instance during mountain climbing, the intellectual capacity was also in other ways depressed although not as severely as memory. In addition there was psychic depression, a painful inner unrest, with time also causing disturbed sleep.
By nature fond of company and full of enjoyment of life, I withdrew in misery into myself, avoided public relations, people and social contacts, lost love for art and nature. Humor rusted in.
Difficulties which I earlier had cleared with ease (and today again can clear with ease) appeared insurmountable. The scientific work required considerable efforts. I forced myself into my laboratory but could not produce anything of value despite all efforts. My thoughts were heavy and pedantic. I had to give up participating in matters which were not of immediate importance. The lectures, previously something I liked, became tormenting. The preparation of a lecture, the writing of a paper, even a simple letter, required immense efforts in handling the contents and language. Not seldom it happened that I wrote words wrongly or forgot letters. To be aware of these shortcomings, not to know their cause, to know no way of getting rid of them, to expect further deterioration - that was not nice.
All efforts to improve my condition failed. Several weeks in the mountains was of no use; I did not feel less miserable there than in Berlin. The nasal treatements and operations often gave short, not lasting improvements. It was remarcable that all psychic symptoms disappeared for hours when the doctor treated certain places of the upper nasal mucosa with cocain; if the correct spot was treated, headache and vertigo disappeared, often within a few minutes. Memory, ability to work and good
spirits reappeared, however, only as passing guests. I often used the method to recall my ability before a lecture, an important meeting etc.
As I have already mentioned, also my collaborators in the laboratory; assistants, Ph.D. students, technicians, had various symptoms: depression without apparent cause, bad memory, headaches and dizziness, now and then gastrointestinal troubles, limb pains, slight mouth inflammations, nasal catarrh etc. With one person some symptoms were worse, with another some other symptoms, apparently for each person at his weakest point. All showed tiredness and depression of intellectual capacity. However, nobody got the idea that there could be a common cause for all of us. Not until a happy-unhappy event finally opened our eyes.
In order to save money we had in 1921 disconnected the ventilation aggregates of the Kaiser-
Wilhelm Institute of Chemistry; aggregates which consumed much expensive electric current. Since the middle of 1923 two of my collaborators, an assistant and a spanish guest, were working on density measurements in a small room. The measurements required constant temperature and therefore windows and doors were kept closed. The work had to be finished before early 1924 since my assistant was to take up a post in industry and the spanish collegue had to go back to his home country. Therefore the work was rushed and the careful cleanliness we at other times kept, was neglected in this room and scattered mercury was left unattended in cracks and joints in the floor and under laboratory stands. Instead of an insidious mercury poisoning the conditions were given for a more acute and more easily recognizable mercury poisoning. The assistant fell severely ill, not just with headaches and intellectual depression but also with severe bodily deterioration, ulcers in his mouth etc. His brother, a doctor, thought that the condition reminded him of mercury poisoning. The renowned toxicologist L. Lewin whom we called for, examined the laboratory personell and declared, that according to his experience, we were all with certainty suffering from mercury poisoning.
Mercury was found in the air of the laboratories as well as in the urine of all affected persons. The mercury concentration in the air varied from room to room, from a few thousandths to a few hundredths of a milligram per cubic meter. That is only a small fraction of what air can contain when saturated with mercury vapor (about 12 mg/cubic meter). Since a human being breathes about 1/2 cubic meter each hour and the inhaled mercury, as it appears, is largely absorbed in the lungs, only a short visit in mercury saturated air is sufficient to elicit an acute mercury poisoning.
When air containing small amounts of mercury is inhaled, it will take a long time until the poisoning becomes apparent. For one to several years the symptoms can be restricted to tiredness and slow deterioration of the intellectual ability and memory. For instance with the spanish guest, inflammations in the mouth did not appear until at the end of the year he stayed with us and reached its peak a month after he had left us and was not exposed to mercury any more. The psychic effects he had felt earlier without knowing their cause. "It was as if I became more stupid in Germany." And similar observations I could make on my other collaborators. Almost all Ph.D. students in my laboratory had difficulty qualifying for the doctor degree. If the students and assistants left the laboratory after a few years, they recovered without knowledge of the mercury poisoning. On myself, the effects of the minimal amounts of mercury developed as I have described.
Especially significant for this type of insidious mercury poisoning are sudden changes in the condition. After a few weeks of better health follows, often quite suddenly, a time of worse conditions. This also holds true for the relapses during recovery. When my disease was at its peak, the general rule was: one or two days of endurable conditions, then increased salivation and nasal catarrh including catarrh in larynx and bronchi, inflammation around teeth, sewere weakness and dizziness, tormenting headache, often also joint pains and diarrhea. The headache, dizziness and weakness of memory are connected to the nerves in the upper part of the nose as the effects of the cocain treatment has shown.
The recovery from insidious mercury poisoning, after elimination of the poison source, is extremely slow and there are often relapses. Professor Lewin told us so and the development of our conditions has proved him right. The necessary time apparently depends on the length of the poisoning, maybe also on the person's age. My collaborators who left the laboratory fortunately recovered within one or two years from all symptoms and have recovered their powers of thinking and memory to the full extent. But also these persons had to endure relapses of psychical and physical character (especially mouth inflammations). Some of the assistants and technicians continue working here and we can unfortunately not avoid using mercury. They have now, nearly two years after the poisoning, clear but ever weaker symptoms. I was exposed to the damaging effects for more than 20 years and the complete recovery apparently takes the longest time; the capacity for work is almost back, only occasional relapses (headaches, dizziness and mouth inflammations) affect me slightly. Judging from the development of recovery so far, I do not doubt that all of my collaborators and myself will completely recover from all symptoms. It is likely that it takes years to excrete the mercury which has been taken up by the body for years.
It appears that from a mercury poisoning follows a special sensitivity towards a new exposure to mercury vapor. Some of us, who because of work or faults in the ventilation system, were again exposed to mercury, felt it immediately as an increasing number of relapses. That seems understandable since the long time for development of the disease shows that a certain threshold must be reached before symptoms appear. The threshold will certainly easily be reached again during recovery and any additional amount of mercury will worsen the condition.
We tried in various ways to enhance the recovery on advice from doctors; using diuretics and substances to promote fecal excretion, taking hot baths, eating small amounts of sodium iodide. I have not the impression that the recovery was substantially enhanced through these measures. Iodine is supposed to bring the metal into solution from insoluble organic mercury compounds, the form in which mercury probably is bound in the body. I could not demonstrate on myself that significantly higher amounts of mercury were excreted in the urine after iodine intake. We did not expect the diuretics to have any effect since we had shown that mercury excretion in the urine soon stopped.
The art of medicine unfortunately has no substance which can detoxify the body from mercury.
To be in the fresh air seems to be most useful for making subjective symptoms less felt. Novalgin has some effect on lighter headache and dizziness. In general one has to let time take away the disturbing influences on the body. Some weeks visit in the mountains and a voyage at southern latitudes brought me hardly any faster recovery than at home, although the psychic rest had a positive effect on my nerves.
Why was our disease not recognized as mercury poisoning earlier? I have often asked myself this question, not without reproach. The first symptoms of the slow mercury poisoning, before any oral symptoms appear, are hardly known to the medical world. They are tiredness, depression of thinking and memory, light headache and dizziness, occasional diarrhea. Neither was it known that the nose and the upper airways were affected. Just this started myself and my doctors on the false track and has also fooled others I know of. One of my assistants was for a long time teated for sinusitis until the true cause was found. Also the difficulties in thinking make it difficult for the affected person to make a correct diagnosis of his troubles: Quem Mercurius perdere vult, dementat prius!
It is appropriate in this context, to warn of another source of insidious mercury intoxication: dental amalgam fillings. Prof. Lewin advised me immediately he had diagnosed the mercury poisoning, to exchange for other materials the amalgam fillings I had in considerable numbers since early youth.
He called attention to a case he knew of, a university collegue who was on the border of psychical and physical collapse when the cause, in the nick of time, was found to be the numerous amalgam fillings he had since youth. After their removal he slowly recovered.
This collegue recently gave me a shaking account of his sufferings for several years until the cause was discovered.(transl. note: Z. angew. Chem. 39, 1926, 984).
The dentists formerly preferred copper and cadmium amalgam and today use silver amalgam for filling teeth since these amalgams are easy to manipulate and fill the cavities well. Silver amalgam is better than the other amalgams which corrode considerably with time. However, also silver amalgam gives off mercury vapor at oral temperatures, which the following experiments proved. (compare also G.Tammann & O.Dahl. Z. anorg. allgem. Chem. 144, 1925, 16).
We sealed silver amalgam pieces in glass tubes, bent into right angles, evacuated them and heated the horizontal part with the amalgam to 30-35o, cooled the other part in ice or liquid air and determined the amount of mercury which distilled over.
1. Amalgam piece, carefully prepared by a dentist from metal powder and mercury for this experiment. Weight 0.801 g, sealed into the glass tube 24 h after preparation, heated for 23 days, ice cooling. Amount distilled over: 11.2 mg mercury.
2. Similar, weight 0.810 g. Three weeks after preparation to obtain as complete hardening as possible and then sealed in a glass tube. Heated for 12 days, cooling with liquid air. Distilled over:
15.3 mg.
3. A piece of amalgam, carefully prepared with as little mercury as possible. weight 1.000 g, three weeks hardening, 9 days heating, cooling with ice: 8.2 mg mercury.
4. Amalgam filling which had been in a tooth for a year and had fallen out. Weight 0.894 g, 14 days heating, liquid air cooling: 29.4 mg mercury.
Undoubtedly fillings like these will also slowly give off mercury in the mouth and give the inhaled air a low level of mercury which must be harmful in the long run. The old copper and cadmium amalgams should be even more dangerous.
One of my faculty collegues suffered since a long time from occasional headaches and dizziness without obvious cause. After he had removed an old amalgam filling which caused slight in- flammation near the tooth, the problems disappeared after some time. The filling was fragile and full of mercury droplets after removal.
Dentistry should completely avoid the use of amalgam for fillings or at least not use it whenever that is possible. There is no doubt that many symptoms: tiredness, depression, irritability, vertigo, weak memory, mouth inflammations, diarrhea, loss of appetite, chronic catarrh often are caused by mercury which the body is exposed to from amalgam fillings, in small amounts but continously.
Doctors should give this fact their serious consideration. It will then likely be found that the thoughtless introduction of amalgam as a filling material for teeth was a severe sin against humanity.
Insidious mercury poisonings are certainly much more common than is generally thought. This is especially relevant for chemists and physicists who often have much to do with mercury. The danger gets too little attention, the real cause of troubles and diseases are often not recognized. In the literature almost nothing is reported on this (An exception from recent times is the report by A.
Blomquist, Ber. d. deutsch. Pharmaz. Ges. 23, 1923, 29, on a general mercury vapor poisoning at the institute of Physiology, Uppsala University). After the resolution of our unhappy fate, I have come to know about a dozen certain cases of insidious mercury poisoning among my aquaintances alone, almost always with the same symptoms, mostly with wrongly diagnosed causes and therefore falsely treated. A typical example is a collegue from another country who has worked a long time with mercury equipment. When he visited me and I asked him if he never had felt any symptoms of mercury poisoning, he definitely denied this. Further questions about his health was answered with:
"I am in a bad state of health; I have suffered from neurasthenia for several years, I have had to abandon my laboratory for long periods etc." The doctors had tried various treatments, had treated him for stomach-, intestinal- and chest-diseases, treated him with special food etc. In reality he had a pronounced mercury poisoning, something which has now been established without doubt.
Faraday was certainly a unsuspecting victim of mercury poisoning. In the late three to four decades of his life which ended after 76 years, he suffered more and more from troubles which made the scientific work harder and harder. He has described this in his letters and in his description of his life where it takes large space. By his doctors it was interpreted as neurasthenia and premature atheriosclerosis. It consisted of periodically pronounced exhaustion and intellectual depression, in irritable weakness, headaches, vertigo, "rheumatism" and primarily in ever increasing loss of memory (comp. E. Jentsch: Faraday's loss of memory. Naturwissch. 3, 1915, 625 & 637).
Spared serious "bodily" diseases; even at advanced age a hiker and a swimmer, Faraday avoided other people in the third part of his life. His scientific work and his lectures he continued, with long breaks, into his last year. One is deeply affected when reading the great scientist's letters where he describes how he often had to visit his medical friends to complain about vertigo and headache, how he could not remember any names, how he lost contact with his scientific collegues, how he forgot his own work and papers, his correspondance and did not know how to write words. "The affected organ is my head. The result is loss of memory, confusion and vertigo." All these symptoms makes it likely that Faraday suffered from an insidious poisoning because of the mercury which was used in his laboratory. It is a disturbing thought how apparently easily it could have been to rescue this gifted man from his sufferings and how much he could still have given science if the cause of the problems had been recognized and removed.
Perhaps was also the strange disease which the mathematician, physicist and philosopher Blaise
Pascal (1623-1661) suffered from in his younger days, a mercury poisoning. Prof. E. Jaensch,
Marburg, notified me about this. Pascal worked much with mercury during his well known barometer experiments. His problems (periodical headache, vertigo, pains in the teeth, loss of appetite, severe cholic) constitute a complete picture of an advanced, slow mercury poisoning.
Undoubtedly mercury, which research can not be without, caused science severe damage in the past as well as today since it depressed the ability of so many scientists. I hope this warning will help to more clearly recognize and avoid the hazards of this devious metal.
***
(In Faraday's laboratory, preserved until today, his experiments with the electrical motor and generator are on display. The apparatus consists of metal rods, immersed in open beakers with kilograms of liquid mercury)
***
Louis Lewin, 1850-1929, was the foremost toxicologist in Germany at the turn of the century. When
A. Stock suspected mercury poisoning he called for Lewin who also put him into contact with prof,
Jaensch, Marburg.
Lewin is considered to be one of the great names in the history of Science. There are still conferences held in his name. He published several books on toxicology, the best known is Gifte und Vergiftungen, 1928. The fifth, unchanged edition was printed in 1962. Few scientific books have such a long life. His most famous book, however, is Phantastica, 1924, "A book of extraordinary scientific depth" according to A. Hoffman, head of research at Sandoz and the discoverer of LSD (by mistake). This book laid the foundations for psychopharmacology and ethnopharmacology. These areas have, good and bad, resulted in a major part of today's drug industry and also use and abuse of drugs.
From Lewin's toxicology book (1928) we cite: "Mercury has a high toxic energy which often, also after medical use, manifests itself in an unpleasant way. In any form, mercury is a strange substance, harmful to tissues and life... From amalgam plombs, especially from copper amalgam, the metal can evaporate in the oral cavity or in any changed form be absorbed into the circulation from the cavity in the tooth and cause a chronic poisoning. This manifests, apart from local effects in the mouth, especially as an impaired function of normal brain- and nerve function. Such disturbances do not always depend on a special sensitivity towards mercury. I have lectured on this subject since the turn of the century and also informed people with such fillings, who have contacted me because of nervous symptoms. I have always arranged to have such fillings removed and in that way produced recovery, even among professors. Prof. Stock was informed about this matter by me and recovered.
ON THE QUESTION OF THE HAZARDS OF MERCURY VAPOR
Dipl. Ing. A. Schmidt, Charlottenburg
Z. Angew. Chem. 39, 1926, 786
In no 15 of this journal prof.Stock published a paper on the hazards of mercury vapor.
It is surprising how easily most chemists and not least prominent scholars and scientists have passed the question of the hazards of mercury. When prof Stock means that not enough has been published on the dangers of mercury I must refer to two books, appearing in the beginning of the 90ies: 1. Dr.
J. Hermann in Vienna: There is no constitutional syphilis. A comfort for all humanity. 2."Mercury treatment is a crime against humanity"; Hermann Risel & Co Publ. Hagen in Vienna. These books did not suit contemporary medicine and were silenced to death by all methods. In these books, however, the dangers of mercury are strongly emphasized and also described are the symptoms which mercury produces among workers who have a lasting exposure to mercury, e.g. in mercury mines, in mercury mirror factories and in the thermometer and barometer factories. If these publications had got a wider attention much bad health could have been avoided, at least during the latest 3 1/2 decades.
I was once suspicious about the amalgam fillings because of these publications, but all dentists I spoke to about this matter, declared that they were completely harmless.
After Stock's irreproachable experiments one can not doubt that they are very harmful. What has the
Minstry of Health to say on this matter? Will they, since no further investigation is needed, produce a document which strictly prohibits the further use of amalgam fillings, or will they, as is always the case in Germany, go into further evaluations?
When prof Stock writes that the unusually strong ventilation of the Kaiser Wilhelms-institut is not sufficient for removing mercury vapor from the air, this is not surprising for someone who has some experience with ventilation equipment. It is known that not only liquids with different densities, but also gases with varying densities often only partly mixes (Dog-cave on Capri); gases with high specific weight will stay beneath. If mercury vapor is to be removed effectively, air can not be removed upwards as usual but it has to be removed from the deepest places. Hempel demonstrated this more than 35 years ago and he constructed laboratory ventilation with evacuation at low sites. It is necessary, where mercury is used, to know what Hempel teached and to construct the ventilation accordingly.
It would be a blessing if prof. Stock not only published his results in Z. f. angew. Chemie, but also in the daily newspapers, so the public is made aware of the insidious hazard.
(Translators note: Mercury vapor is not heavier than air and does not flow along the floor. It apparently drifts in the air in the same way as tobacco smoke. If the source of the vapor is on the floor or in cracks in the floor, the vapor concentration will naturally be higher near the source. An excellent photographic demonstration of the evaporation of mercury can be found in National
Geographic Magazine, oct. 1972 p. 507, Quicksilver and slow death.)
Dr. Georg Pinkus, Berlin-Fridenau. Z. Angew. Chem. 39, 1926, 787
The warning by prof. Stock, based on his own disease story, will not appear without effect. A large number of chemists have similar symptoms as Stock have described them and since there is not a single chemists who not at some time comes into contact with mercury or at least has amalgam fillings in his mouth, many will find an explanation for their symptoms in a insidious mercury poisoning. One must hope a suggestion that such diseases are of any real importance among chemists will not have too much effect. This is in order to counteract any far reaching worry among lay people and to prevent premature conclusions. The removal of all amalgam fillings which Stock recommends, means an enormous task and concerns a much wider public than a small group of chemists. To prevent this it seems necessary to point out that there are also experiences showing that workers and chemists have worked in nearly mercury-impregnated rooms for decades without the slightest harm.
It is known that the vapor from metallic mercury is poisonous. Every student is made aware of the dangers with mercury distributed into cormers and cracks. Skin affections among doctors when they have broken a thermometer in their pocket are not rare and during the anti-luetic ointments, when the mercury has an especially large evaporation surface, salivation, mouth-, tooth- affections are even common. Even if it is known that mercury can pass the intestines without harm when it is swallowed in order to clear intestinal obstructions, it belongs to every chemists basic knowledge that the vapors are toxic.
One can imagine my surprise when I, with this knowledge, in 1923 entered a company where the owner since more than 30 years was occupied with the purification of mercury for dental purposes and with the manufacture of amalgam. I saw that in large, light, carefully cleaned but not ventilated rooms, relatively large amounts of mercury (up to 50 kg daily) were handled. It was not possible to completely avoid scattering of mercury. Not only in the corners of the floor but also on the working
tables were constantly mercury drops. Only when the mercury was heated did the work take place under an exhaust; as soon as it had cooled it was placed freely in the room.
The copper amalgam is rolled out in large sheets during manufacture and these square meter sheets were day and night open in the room. I must explain here that silver-amalgam, gold-amalgam and platinum-amalgam are mercury-free alloys and amalgamated with mercury by the dentist. They are not discussed here. Copper amalgam, however, is commercially delivered as a real amalgam, becomes softer by heating and can be filled into a tooth. Copper amalgam always contains an excess of mercury and the large surfaces have excellent opportunity to give off mercury to the air.
Despite these circumstances which, to the best of my knowledge, are similar in other such factories, not one of the chemists or workers have fallen ill with the symptoms described by Stock. All workers have been employed for many years, some more than 20 years and one of the managers, as already told, more than 30 years. Most of them are robust and appear to be in good health.
The same observation on the harmlessness of mercury have been made at the Hoechst Farbwerke where 70.000 kg have been used in 10 years (comp. Schardt, this journal 39, 1926, 668). Also
Loesch (Deutsche dentistische Wochenschr., München 1926, p.443) has made thousands of kilograms of sublimate tablets from metallic mercury in open vessels without any harm to himself or his collaborators.
I like to present these realistic and contrasting facts against the observations by Stock which presumably also are correct and I dare, respectfully, suggest an explanation: When a chemist - also
Stock - discusses medical matters, he can draw no better conclusions than any layman. He has, in addition to what the layman knows, his occupationally learned fright for real conditions he knows about but can only draw conclusions from his own experiences. The general survey and the possibility to compare are lacking. I will not, because of this, go further into the question, but will restrict myself to my own experience.
More than 20 years ago I fell ill with intestinal catarrh which was so severe that I had to give up my position in industry. Quite analogous to Stock who blames mercury for his disease, I was at that time of the opinion that a certain chemical compound was the cause. I will not mention its name in order to avoid another anxiety. But none of my collaborators, chemists or workers, became sick although the latter came into much closer contact with the material than I did. Only I was, because of coinciding psychic agitation, susceptible for the poison. The psychic problems were hardly alone sufficient to harm a healthy intestine, neither was the organic poison alone sufficient to harm, something the health of the others showed.
The symptoms of the disease was almost completely the same as those described by Stock as mercury poisoning: general neurasthenic problems, although mercury, disregarding a few amalgam fillings, was clearly not involved. This poses some doubts on the etiology of Stock's disease. As in
Stock's case it took years until everything was in order again. I can with certainty say that my condition during the latest three years, when I breathe mercury-containing air, has not become worse; my memory is neither better nor worse today. The ability for mental calculation and to add figures has in fact improved.
I conclude from all this that also for mercury poisoning another factor is necessary besides mercury; it could be a psychic or a physical one. In support of this I can mention the "Ärztlicher Merkblatter" which is published by the medical doctors of the German chemical industry (1925, J. Springer Verl p 8), that the disposition for occupational mercury poisoning is "individually very varying" and that its occurrence in Germany is very rare.
All this is, however, only possibilities, maybe at best only likely causes and an explanation can not be expected from publications by chemists, describing single cases. Now the medical doctor and the statistical scientist must intervene. I consider it to be false and premature and the suggestion of damage as a calamity, if because of a single case the daily press and the journals take up the question and cause unrest in wide circles before medical statistics are available. Before such wide reaching demands are made, i.e. removal of the amalgam fillings from the mouths, a statistical connection between these fillings and nasal-, intestinal- and nervous- problems as described by Stock must be established. It does not seem an exagerration if the number of persons with amalgam fillings is estimated to be 100 million. Then it must be possible, even if it means much work, to obtain statistics on 5000 or 10000 cases, maybe with the help of the insurance bureaus of the major factories, in order to compare the health of the amalgam carriers realted to number of fillings, age and occupation.
Only in this way can the value or lack of value of Stock's observations on himself be evaluated.
Summary:
1. It is known since a long time ago that mercury vapors are poisonous. To obtain intense effects
(ointments against lues) one has always used finely divided mercury and distributed it over the skin to enhance evaporation by the body heat. (however, all statements by Wassermann are in need of medical examination: before lues was known to produce paralysis, many direct luetic consequences were blamed on mercury).
2. Then most of the mercury enters the body through the lungs. Metallic mercury can pass the stomach and the intestines in large quantities without producing beneficial or harmful effects.
3. Stock has, for the first time, described the subjective conditions of an insidious mercury poisoning and blamed, not salts of mercury but evaporation of metallic mercury, and amalgam fillings.
4. Amalgam fillings, which might be present in 100 million persons, have so far been considered completely harmless (Witzel: Das füllen von Zähnen mit Amalgam, 1899, Berlinische Verl.). Stock's suggestions contradicts this and a careful study on the connection between health problems or lack of them and amalgam fillings is desirable. To cause anxiety before such statistics is available is premature.
Prof. Dr. H. Reihlen, Karlsruhe
Z. Angew. Chem. 39, 1926, 788.
After A. Stock recently with emphasis has pointed out the dangers of mercury vapor, many chemical laboratories have been searched for mercery and this with such a result that it is a small wonder that mercury poisoning is not a normal condition among laboratory chemists. It seems to me as if the finding of mercury in all laboratories which are carefully enough searched, could lead to an underestimate of the poisonous effects of this element.
I will report on some cases of light mercury poisoning and on a case where it did not happen, despite apparent danger.
In my laboratory the collaborators of my predecessors worked much with mercury; the laboratory was therefore, when we took over a year ago, carefully cleaned, at least in a manner I then thought sufficient; all tabletops were taken out and cleaned and about 200 g mercury was recovered. I found an even larger amount in the drains. The latter might not have been dangerous since it was always
covered with water. In the summer working period nobody working in the room had any problems with health. Today we consider that the open windows helped us since, at the end of the winter period, both of my collaborators, working in the room, fell ill with severe gastrointestinal problems.
I developed dry but intense dermatitis with small red vesicles on the inner side of my left arm and later on the inner and upper parts of my legs.
At the same time all three of us had constantly running noses, something I personally already had some predisposition for. We suffered from the manifestations which are generally called semester tiredness to a degree which was less than endurable.
The skin problems were diagnosed by the prof. of occupational medicine, Holzman, as side effects of medicines and were treated with zinc-containing cream without results. Dr. Wirz, dermatologist in
Munich, prescribed a tar-sulfur soap, containing bismuth and zinc oxide and promised a cure within a few months.
The semester has passed and I traveled with my ointments to Schwarzwald for a few days. Contrary to my expectations, the soap and a few days of sunbathing helped as if by magic; after a week the skin eruptions were not to be seen and only a light irritation remained.
Apparently two fortunate circumstances were present. Primarily the room is long and narrow and door and window are opposite each other facilitating ventilation. Secondly, the room next to the laboratory is the hydrogen sulfide room and the wall is porous and often hydrogen sulfide penetrates the wall. It is possible that the hydrogen sulfide reacts with the mercury vapor and precipitates the metal as harmless sulfide. This could also explain - the idea was communicated to me by prof Stock
- why mercury poisonings so far have not been reported from teaching laboratories.
Finally I must also remark that no disease of the oral soft tissues, something which is generally considered characteristic of mercury poisoning, did appear among any of us three. Two of us are heavy smokers, the third one does not smoke at all. His teeth are in a remarcably good condition, something which also is explained by a particular care and is also necessary for smokers because of the otherwise appearing bad-looking, yellow deposits which are formed. Also the gastrointestinal problems of my collaborators diseapperared during the holidays. It is likely that they must have been connected with the work in the laboratory.
Since we now only work with harmless compounds, we again thought about the possibility of a contamination of the laboratory and mercury poisoning. We again removed all tabletops, cleaned all drains etc. Then we discovered a few drops of mercury in a drawer which we had cleaned the day before. The table top above the drawer was used for all major destillations etc. and was covered with a large piece of slate , held in place with putty. We broke it off with force and really found a lake of
300 g mercury beneath it. It is noteworthy that you can hardly imagine a worse place for mercury spillage than beneath the cover of a table for experiments using heat. We did not wonder any more where the source of our mercury exposure was. However, I wonder why another collaborator, working with vacuum equipment in another room since two years and constantly in contact with mercury, has shown none of these disturbances.
Dr. F. Gradenwitz, Berlin
Z. Angew. Chem. 39, 1926, 788.
The results from the four experiments with dental amalgams can, according to my opinion, not be directly applied to oral conditions, something also prof. Stock has confirmed in a private communication. The experiments which will certainly be described in the dental journals, could be falsely interpreted; in the newspapers from Voss there has already been an extensive report and in this the attention was especially focussed on the dangers of dental amalgams. I do not exclude the possibility that scared patients will cause troubles for their dentists when amalgam filings are suggested.
If I have clearly undestood the experiments by prof. Stock and his collaborators, they have placed fillings in the form of cylinders or spheres in tubes, sealed by melting and then heated. Then the whole surface can give off mercury. In the mouth whole crowns of amalgam are seldom used (earlier this was common) and usually a small or large cavity is filled with amalgam. The free amalgam surface in the mouth is perhaps a fifth of that used in Stock's experiments. I also can not exclude that the saliva which wets the teeth and the fillings regularly, also will inhibit or reduce the evaporation of mercury. Primarily the small surface area will alter the conditions. Apparently a somewhat mercury- poor layer will form on the surface of the filling after some mercury has really evaporated and after a short time no noticable amounts of mercury will be released.
If my considerations can not be disputed, then the objections from prof. Stock and prof. Lewin will have less weight than it appears from the reported experiments.
One can not dismiss that amalgam fillings and especially copper amalgam are very easily worked and cheap materials which protect especially childrens teeth from premature deterioration. It can only be excluded from the stock of materials which the dentist uses if the latter can report harmful effects. The dentists will certainly now carefully watch their patients because of Stock's warnings.
One has especially to avoid placing amalgam fillings near metals (gold fillings, gold bridges and bridges and plates of alloyed gold). In such cases there wil be electrolytic currents which also destroy the deeper parts of the amalgam fillings and can cause evaporation of larger amounts of mercury in the mouth.
A note added to my previous rebuttal of prof. Stock's paper:
Shortly after sending my rebuttal I found in Zahnärztl. Rundschau no 19, may 9, a paper by the dentist Dr. Jarecki, "The hazards of mercury vapor" in which the paper by prof. Stock was reported in more detail and at the end is a request that control experiments should me made at the dental research institute "to evaluate the results" Jarecki recommends "that discussions which have already appeared in the daily press should be disregarded in the interest of the matter itself and the patients.".
In connection with the report by Jarecki, there is also in Z.R. no 9, a publication by the Berliner university professors Dr. Schroeder and Dr. Schoenbeck: "On the question whether amalgam filings are harmful." "From various places we have been asked to give a statement on the publication by prof. Stock in Z. angew. Chem. on the hazards of amalgam fillings. Immediately after its publication we decided to carefully study the dental side of the question with our own experiments. Primarily because Stock's experiments did not simulate real conditions in the mouth and therefore the results could not immediately be considered relevant. Above all, the evacuation of the tubes which he used in his experiments must be the subject of consideration since this is different from conditions in the oral cavity."
It should be valuable if also the readers of Z. Angew. Chem. were made aware of the opinions of these authorities on practical dentistry and dental filling materials.
On the question of the hazards of the amalgam plombs, we have received the following paper: THE
HAZARDS OF AMALGAM FILLINGS
A dental rebuttal to the paper by Alfred Stock. by dentist Dr. Gustav Haber, Berlin. Zeitschr. angew.
Chem. 39, 1926, 905
The statements by prof. Stock are of basic importance and the accusations against dentistry concerning the use of amalgam fillings have such wide implications that each dentist must ask himself if the further use of a filling material for which mercury is used can be allowed.
Prof. Stock and his collaborators approached with open eyes their psychical and physical destruction without being able to help themselves or to obtain help. A tragic picture which can only evoke anyone's compassion. We are happy and feel relief when we read that the art of medicine has succeeded to bring prof. Stock and his collaborators back to their full psychical and physical powers.
We have the task of evaluating if amalgam fillings could be responsible for a mercury poisoning.
Prof. Stock describes in every detail the insidious sufferings, discusses the causes and asks rightly why the mercury poisoning was not recognized earlier. One must agree with Jarecki when he writes
(Zahnärztl. Rundschau no 19) that it is completely incomprehensible that none of the doctors got the idea, considering the occupation of the patient, to analyze the urine for mercury and that it took nearly 25 years until finally the toxicologist L. Lewin found the correct diagnosis and then opened the way to recovery.
The observations which prof. Stock made on the causes of the mercury poisoning in connection with the description of his sufferings, must be critically examined from various points of view. In the centre is the warning for the amalgam dental fillings as a little recognized source of insidious mercury poisoning. To support this suggestion is the following: 1. Laboratory experi-ments with three pieces of amalgam and a filling which had been in a tooth for a year and then fallen out. 2. The clinical observations by Stock of his own body, the ones by prof. Lewin of another university professor and similar observations which a faculty collegue of Stock made on himself. This material only supports the suggestion of mercury poisoning from amalgam fillings. Prof. Stock concludes, based on the four laboratory experiments and the three clinical observations by the patients themselves (it is not known whether medical evaluations support the information from the patients) that: "Dentistry should completely avoid the use of amalgam for fillings or at least not use it whenever that is possible. There is no doubt that many symptoms: tiredness, depression, irritability, vertigo, weak memory, mouth inflammations, diarrhea, loss of appetite, chronic catarrh, often are caused by mercury which the body is exposed to from amalgam fillings in small amounts but continously. Doctors should give this fact their serious consideration. It will then likely be found that the thoughtless introduction of amalgam as a filling material for teeth was a severe sin against humanity."
Is then this annihilating accusation against amalgam as a dental filling material so securely based that it can be accepted without consideration? I first notice that Stock and his collaborators always used equipment with mercury like pumps, manometers etc and that the amounts of mercury which was scattered in the laboratory experiments could not at all be used for comparison. It should also be valuable to know how large the amounts of mercury were in the amalgam fillings in order to evaluate the amount distilled over and the relation between the used and the released amount of mercury. It appears completely possible to me that the amounts of mercury vapor released from the equipment during experiments could be several hundred times more than the minimal amounts released from excess mercury, even if all 32 teeth were filled with amalgam.
Apparently the evaporation from the mercury equipment will be very varying in relation to time, temperature and use. Tests showing the effects of these conditions on the release should be carried out before information in the literature can be simply dismissed as prof. Stock does. Prof. A. Witzel has, in his book "Das Füllen der Zähne mit Amalgam" p.232, listed the cases reported in the Berliner
Klin Wochenschr. 1895. He points out the danger for the dentist when he presses out mercury from the plastic amalgam through leather or between the finger tips, does not collect the mercury under water but lets it fall carelessly onto the floor of the clinic, he writes: "That the dangers are not imaginary but is something which surrounds every dentist who handles mercury carelessly, the following examples, reported by Lewin, can show: He describes the ointments where inhalation of vapors released from the body were a major factor; Gerhardt in Wurzburg had a piece of linen, impregnated with grey ointment, hanging in a room. The syphilitic symptoms reduced, one sick person even got a mercurial ulcerative stomatitis. - A girl, who had nothing to do with mercury but who lived together with a woman who worked in a mirror factory, got typical mercurial stomatitis from the vapor of the minimal amounts of mercury which had been trapped in the clothes of the woman. In two quite similar cases, completely healthy persons, living in the same rooms as persons treated for syphilis, fell ill with stomatitis and also had other symptoms of a mercurial intoxication.
Finally I like to mention the events on the english ship Triumf, known also from the literature.
Three large vessels with mercury broke and the vapors, despite all efforts to clean and ventilate the ship, poisoned the whole crew on the short trip between Cadiz and England. Several members of the crew even died. The same happened to animals which were onboard. Any dentist who has up to now been careless should learn from this to carefully collect any excess mercury from the preparation of amalgam in order to prevent it from being lost and evaporated in the clinic."
Concerning the laboratory experiments by prof Stock where it was shown that mercury releases mercury at mouth temperature, one has to note what prof Schroeder and Schoenbeck recently communicated in Zahnärztl. Rundschau no 19: "that Stocks experiments did not simulate real conditions in the mouth and therefore the results could not immediately be considered relevant.
Above all, the evacuation of the tubes which he used in his experiments must be the subject of consideration since this is different from conditions in the oral cavity". - But even if Stocks experiments were relevant for oral conditions, they could only be used for an evaluation whether amalgam fillings can cause mercury poisoning if shown that the mercury comes free, is absorbed into the body through the lungs or skin and its total excretion is not possible. I have already noted the information on this type of chronic mercury poisoning in the dental literature.
Stocks presumption that "amalgam as a dental filling material was a severe sin against humanity", is only relevant if it, without any possible objection, can be shown that mercury droplets in the amalgam filling are set free and are not excreted from the body and thus remain for ever in the body.
In contrast to that we have information from other well known authors. Stocks observations on four amalgam fillings is to be contrasted with the many thousand amalgam fillings and the many hundred diffrent materials which Witzel studied and presented already 30 years ago in his book: "Das Füllen der Zähne mit Amalgam".
The tables by Witzel comprise a material which is more than one hundred times larger and where all aspects have been studied in detail. It is too much to go into details here. I can only mention that
Witzel was not content with the simple determination of how much mercury was released in each case but that he noted in tables amalgamation and hardening experiments with pure metals, metal mixtures and metal alloys. Witzel did chemical- mechanical and chemical-electrolytic dissolution studies in acids and by abrasion of amalgam disks, also in acids and with contact with metals; chemical and electrolytic dissolution in lactic acid; he studied the chemical-electrolytic processes in sodium chloride solutions and in mixtures of sodium chloride and lactic acid. He did comparative
chemical-electrolytic experi-ments with different amalgams and solutions at various temperatures and he calculated how much was swallowed as lactic acid salts from an amalgam filling each day and during a year when different amalgam alloys were used.
Witzel has reported in detail on the simple and combined amalgams, also on the form changes of the hardened amalgam and the amalgam surfaces in the mouth. Witzel has carefully studied the electric currents which the teeth with amalgams and metals are exposed to. Besides other important chapters in this classical book there are experimental studies and practical experiences of copper amalgams and all other amalgam alloys and there is an additional chapter which is only devoted to the question: "Can metal- and especially mercury-poisonings be caused by amalgams as filling materials". Witzel arrives at the following result which I quote literally: "I have not, among thousands of patients, observed any symptoms of a chronic poisoning which could be ascribed abraded or dissolved parts of our copper amalgam fillings. I emphasize: although I have filled innumrable childrens teeth with copper amalgam, I have not seen any case similar to that published by Roussy. However, I will not state that this filling material never has caused such diseases of the gastrointestinal tract.
We must in any case consider that, when the saliva is very acid, the presence of large copper amalgam fillings might harm the patient. If this is also posible from a number of large, tin- containing copper amalgam fillings, is not yet possible to decide. That also this material can be markedly degraded by dilute acids and electrolytic processes in the mouth is clear from our experiments and the figures in our tables.
We know about the complex amalgams with platinum, gold and nickel which are much more resistant against the oral liquids and will be little degraded, hardly noticably abraded after several years because of chewing and that we never can find free mercury on the surfaces whether these are dark colored or polished. Our simple but very sensitive test with gold foil has demonstrated this.
The results of all these studies allow us to conclude that we, with the complex platinum- and goldcontaining silver amalgams, have an excellent filling material, completely harmless for health."
More recent research has confirmed the statements by Witzel. We find the following information in
"Dental Progress" by Misch: "Urine measurements of dentists and dental assistants have shown that these always have mercury in the urine, however, in very small amounts - 0.05 mg daily (Schulte).
The highest levels in urine were found in those who worked with large amounts of copper amalgam, irrespective of whether the amalgam was worked with the hands or contact with the body was avoided. It thus seems that the mercury did not enter the body because of direct contact but as vapor, inhaled through the airways."
This information contradicts the statements by prof. Stock, based on the scientific data from four amalgam fillings and simple excretion tests. The removal of the amalgam fillings from prof. Stock's mouth and the other two stories of disease can not be used to give a verdict on amalgam. Stock's public accusation that amalgam was a severe sin against humanity is only valid if he can offer an experimental material which is as large as that from Witzel. This material must then be tested in every way, just as Witzel's, and his results disproved. Since it has been shown that the poisoning is caused by mercury in vapor form and that Witzel's studies show that a poisoning from amalgam fillings is not possible, there is no doubt that the symptoms of poisoning which prof. Stock and his collaborators showed was exclusively caused by the mercury equipment and the use of mercury.
It should also be investigated whether the clinical observations by the professors Stock and Lewin and the information from the other university teacher could be considered proof or supporting evidence for the validity of Stock's laboratory experiments. Prof Stock, was adviced by prof Lewin and after recognition of the mercury poisoning to exchange the amalgam fillings he had in considerable numbers since early youth for other materials. We lack information without which a dentist can not properly evaluate the situation: 1. Was there immediately an improvement of the general health after the removal of the amalgam fillings? 2. Were there among Stock's mercury affected collaborators also persons without amalgam fillings and if so, how did this affect the types or severity of the symptoms? 3. Had the treatment of the mercury poisoning already started when the amalgam fillings were removed; had an improvement of the health already started before the fillings were removed? 4. The most important question: were the pulps and the root canals dead beneath the fillings. If this is confirmed, were the canals filled or infected? If only one root canal was infected, then the improvement can not be ascribed to the contemporary removal of the mercury in the amalgam fillings but with the opening of the root canal and the "airing". The airing is connected with a release of the putrefication gases which had caused an increasing pressure on the nervous system of the head in the region surrounding the root canal. When therefore prof Stock, to support his opinion on the hazards of the mercury droplets in the amalgam fillings, reports on the case of his faculty collegue, I am completely convinced, even if I do not know the case myself, that the troubles disappeared only because the root canal, filled with putrefication gases, was opened and treated. It is further reported that the filling, after removal, was brittle and full of mercury droplets. The fragility can have several causes, e.g. the amalgamation, the binding of the mercury to the powder was not sufficient or the quality of the "amalgam" was not good or the filling was exposed to the biting pressure before it was enough hardened, or the articulation and occlusion was not enough considered which could cause wrong loading and fracturing of the amalgam filling. We see that many causes can contribute to the fragility. However, rarely mercury droplets.
The case contributed by prof. Lewin: "a University collegue who was on the border of psychical and physical collapse when the cause, in the nick of time, was found to be the numerous amalgam fillings he had since youth. After their removal he slowly recovered. This collegue recently gave me a shaking account of his suffering for several years until the cause was recognized." Also concerning this case one must state that without an answer to the questions to prof. Stock, only part of the sufferings and their removal can be ascribed to the mercury in the dental fillings.
The verdict is quite different when one has to consider whether amalgam fillings should be placed into a mouth where there are already gold fillings or gold bridges. In this case one must, if possible, avoid any amalgam filling, also when they consist of platinum or gold amalgam. All amalgam fillings must also be removed from teeth which are to be filled with gold or have crowns of gold.
The amalgam fillings must also be removed from the neighbouring teeth and antagonists (however, not when platinum crowns are placed, something I will report on elsewhere). The same requirement for amalgam removal is also necessary for teeth which are in contact with the edges of a metal plate and which serve as support for the metal hooks of a protheses (also non-noble ones of e.g. steel). This must be rigorously adhered to, also if it means the removal of every faultless amalgam filling.
This rule is not at all because of fear of health disturbances, although there are possibilities for this because of electrolytic processes when gold and amalgam come into contact. When the mercury is not under pressure from the gold there is rarely a release of mercury into the gold. Howvever, when the gold in contact with amalgam is subjected to pressure or rubbing, its indifferent state ceases and there will be an amalgamization of the gold and a destruction of the latter. Witzel has shown that hardened amalgam is transformed into a ductile form when it is subjected to strong pressure, also biting forces.
The answer on the question what can be used as a substitute for amalgam as a filling material is more than can be answered in this communication; I have discussed it in the chapter "On the contact between amalgam and gold" in my book "The root as a support for protheses" by Dr. G. Haber. In the book I concentrated on showing that a general condemnation of the use of amalgam fillings is not substantiated. The removal of amalgam fillings and their replacement with tin-gold, silver alloys or gold something I have done for years, has other causes than the ones reported by Stock.
Summary: 1. The analyses and clinical observations, reported by Stock, are not sufficient to disprove the hundred and thousand times larger results by prof. Witzel.
2. The amalgam fillings are not harmful for the patients but their preparation constitutes a risk for the treating doctor. The danger increases with the number of fillings prepared and with neglect of precautions.
3. Amalgam fillings are no hazard for the human organism. - Infections in the body and other damage has in no case been proven to be caused by the mercury in the amalgam fillings.
4. The number of cases, reported in the literature, with damage because of mercury in amalgam fillings constitute a considerably smaller percentage than the damage caused by drugs and injections.
Then one has also to consider that in the latter cases there is mostly a clear connection, something which is seldom the case in presumed amalgam damage.
5. Just as the medicament or the injection solution can not be blamed for too strong doses which are given, the use of amalgam fillings can not be totally condemned because some compositions with increased mercury content and unsuitable alloys might cause damage if they are improperly made, something which still has to be proven.
When I, as a non-chemist, took up the task of opposing the views of one of our greatest scientists and reject his material as not sufficient proof, then it was because I, as a dentist, have been studying this question. I have rejected amalgam as a dental filling material only under certain conditions, namely in connection with gold and idiosyncrasies which people sometimes acquire if they have occupations which bring them into contact with mercury. These exceptions, however, can not form the basis of a general condemnation like that expressed by Stock.
On the question of the hazards of amalgam fillings.
L. Sterner-Rainer, Engineer, Wien. Z. angew. Chem. 39, 1926, 907
Concerning the discussion which the paper by prof. A. Stock in no 15 of this journal has started, Dr.
G. Pinkus writes in no 26, that now the medical doctors and the statistical scientists must have the word. Regarding the hazards of mercury vapor this does not at all seem to be necessary; in this respect we are all grateful to prof Stock that he has made us aware of an almost generally underestimated hazard. However, to find enough material to evaluate the hazards of amalgam fillings for carious teeth and to compile the results, doctors and statistic scientists will need more time. Also metallographic specialists must be allowed to illuminate the problem. Prof. G. Tammann, senior scientist in metallurgy, has together with O. Dahl at the inst. for physical chemistry, Univ. of
Göttingen, published an extensive study of the composition and properties of silver-tin-amalgams in
Z. anorg. allgem. Chem 144, 1925, no 1. These are the ones which are mainly used in dentistry. Prof
Stock also refer to this paper in a foot-note. Older studies by Ogg (Z. phys. Chem 285, 1898) and
Reinders (Z. phys. Chem 609, 1906) do not contradict the results by Tammann-Dahl. The experiments which have been carried out at the metallographic laboratory of G.A. Scheid's Affinery in Wien during the latest 3 years and which include amalgams with gold, platinum, palladium, copper, lead, zinc, cadmium etc, in addition to the basic silver-tin alloy, agree in all major respects with these results.
I notice, when I carefully read the paper by Stock, that when he warns of amalgam fillings on p.465, he always writes about silver amalgams. Such amalgams are, however, not used by dentistry and it should be silver-tin alloys he used to manufacture the amalgams for his experiments; The "amalgam manufacturers", whom prof Stock adresses in no 26 of this journal, produce no silver amalgam but alloys of pure silver with tin, with or without additions of small amounts of other metals. It is the dentist who, in the presence of the patient and after desinfection of the cavity in the tooth, places the amalgam he has just manufactured by mixing silver-tin chips with mercury and pressing out the mercury which was not absorbed. The amount of absorbed mercury varies according to composituion of the silver-tin alloy and the pre-treatment of the filings. Silver-rich alloys absorb more than tin-rich, "aged" ones, e.g filings which have been made a long time earlier and which have been placed in the sun or at 100 oC for an hour. These bind much less mercury, something which already Joyner and Knight (J. Chem. Soc. 1911, 1913 and 1914), G. Black in Chicago (Die Technik des Zahnfüllens 1914 bd II) determined. Tammann and Dahl have recently studied the ability of silver-tin alloys with various compositions to take up mercury and found that the alloy, especially recommended by Black, 73 parts silver + 27 parts tin, takes up 170 parts mercury if freshly prepared and in aged condition 78. The often used 60 parts silver + 40 parts tin alloy takes up 112 and 29 parts of mercury respectively and holds it with a pressure of 35 kg/cm2.
What happens then with the ternary alloys silver-tin-mercury in the few hours when it hardens and thus a profound change in properties occurs? Also on this the work by Tammann-Dahl gives a clear account. The alloy transforms into a mixture of the following crystals: Ag3Sn, Ag3Hg4 with a little
(about 2.5%) tin and the mixed crystal Sn-Hg. Free mercury is thus not present in a properly made and hardened amalgam dental filling but chemical compounds and a saturated solution of mercury in tin with the approximate composition 85 parts tin + 15 parts mercury. The amounts of this phase is less if the original alloy is silver- rich. The mercury which Stock distilled from amalgam in vacuum can only come from this solid solution since a decomposition of the chemical compound Ag3Hg4 at a temperature of 30 o is not to be expected. However, also the crystalline, solid solution Sn-Hg will not decompose under normal oral conditions since then gamma- tin must precipitate. The author of this communication has worked with the purification and reuse of metals from scrap for 42 years and has never been able to measure a loss of weight from hardened amalgam scrap, delivered from dentists and kept in open vessels.
That the equilibrium conditions of metals in alloys change, not only with temperature but also with pressure is known to every metallurgist (phase rule of J.W.Gibbs). It is no doubt that the large evaporations from amalgam fillings in extracted teeth which Stock demonstrated recently (no 26 this journal), was only produced by the vacuum. If three large fillings can give off 150 mg mercury in three days at 30 o, then a 3 g plomb, prepared from fresh 60 silver + 40 tin alloy, according to
Tammann-Dahl, containing 1.59 g mercury, should in one year become mercury-free and disintegrate. A similar one, prepared from aged alloy and containing 0.675 g mercury, should have given off all its mercury in less than five months. Such consequences are against all experience.
Amalgam fillings, properly prepared from silver-tin filings, with excess, not binding mercury pressed out before it is placed in the tooth cavity or to which no excess mercury has been added, can not be hazardous. With this confirmation, the anxiety which has affected not only dentists and
assistants, but also has been spread by the daily press to the carriers of the dental fillings, can again disappear.
Ludwig Wolf, Berlin
Chem. Inst. of the University
Z. angew. Chem. 39, 1926, 789
Recently a paper appeared in this journal in which the harmful effects of mercury vapor were described in detail. The symptoms were so appropriately described that any reader who like me has suffered from mercury poisoning will find his disease described in detail. Then it might appear superfluous to deal with the subject any more - however, I will anyhow do this.
The reason is that one can hardly often and strongly enough warn for the hazards of mercury vapor.
Anyone who has himself experienced this poisoning needs no further warning, - but others who work with mercury and not rarely consider it harmless, should once more with emphasis be reminded of the unhealthy effects caused by the drops which use to be scattered in most laboratories.
I had to suffer severely myself from the consequences of my thoughtlessness. Some years ago I was visited by prof. Pregl when he stayed in Berlin and he warned me sincerely when he saw the large amounts of mercury, not only in the equipment but also scattered as small drops everywhere in the room. If I had given my full attention to prof. Pregl's sincere warning, I could have been spared many bad conditions. However, I did not believe in such a danger from mercury vapor since I thought that such small amounts could not be harmful. Then I was already a constant guest at the medical clinics in order to have my completely unexplainable symptoms from throat and nose examined. In addition to this, I had just as prof. Stock, unbearable headaches, pains in my ears and nearly all symptoms which prof. Stock has described. Neither I nor my doctors got the idea that all these symptoms could be connected with mercury poisoning. Only when vesicles appeared in my mouth, something which was known by my doctors as characteristic for mercury poisoning, I got a correct diagnosis.
To me it seems that he signs of an insidious mercury poisoning are not enough known. For instance, a doctor friend of mine had the same symptoms as prof. Stock and did not know their cause. The paper by prof. Stock convinced him that he had mercury poisoning; some time later he got vesicles in his mouth and this confirmed his suspicions. His poisoning is without doubt caused by gas analytical work when he is constantly in contact with mercury.
My collaborators, who worked much with vacuum apparatus and mercury, also suffered from the symptoms prof. Stock has described. When they left this work their symptoms diseappeared with time. Mercury vapor appear to affect the kidneys of females especially. Two female collaborators fell ill with kidney inflammation, a third case outside our institute is known to me. All persons are not equally sensitive towards mercury vapor; it seems as if many are quite resistant.
However, also in such cases there is need for extreme caution. In winter one has to arrange an especially good ventilation and open mercury should always be covered. The heated mercury in the seals of mercury vapor pumps appear to be sources of contamination. If the pumps can not be placed under an exhaust, it is possible to cover the mercury seals with solid paraffin and other seals can be covered with liquid paraffin.
Just as prof. Stock, I have tried all sorts of healing methods without success. The most successfull ones are time and extreme caution during mercury work, especially in heated laboratories. A good prophylactic and antidote seems to be the well known method of daily drinking one litre of milk.
Observations on mercury poisonings by arabic alchemists and doctors.
J. Ruska, Heidelberg
Z. angew. Chem. 39, 1926, 790.
The observations on the symptoms of insidious mercury poisoning which prof. Stock has reported in this journal reminded me of arabic descriptions of mercury poisonings which I have published many years ago and also of an, up to now, unknown description by Gabir ibn Hajjan in his "Book of
Poisons".
The description has been collected by al Qazwini (dead 1283) in the mineralogical part of his cosmography. According to Avicienna (dead 1037), mercury vapor causes paralysis and tremor and the smoke destroys the ability to see and often causes watering eyes among chemists. It also takes away the ability to hear and causes foul smell from the mouth.
An unknown author has described the symptoms in even more detail: Heated mercury causes - if the vapors are inhaled - paralysis, numbness, unconsciousness, yellow color, tremor of arms and legs, foul smell from the mouth and dehydration of the brain. Mercury dust, mixed into dough and placed as a bait, kills mice. Ointments with mercury kills all parasites which are on the body. Snakes, scorpions and other animals leave the house or are killed when mercury vapors are inside.
I will relate the description by Gabir (dead about 820) completely. It can be found in a large work on poisons, up to now only known from a citation in a dissertation on famous alchemists by
Berthelot and it had been considered lost. It has, however, been rediscovered by M. Meyerhof in
Cairo and is in my posession as a handwritten text. The text is as follows:
Quicksilver: This element belongs to the major (strong) poisons and this is both when it is killed
(ashed, oxidized) and when it is sublimed (evaporates) or is treated in any way which is known to men who know the art (chemistry, alchemy). The killed quicksilver causes strong stomach pains and pains like knife- stabs in the abdomen, anxiety, then arrests the movement of the blood and finally kills; however, the killed quicksilver is less dangerous than the sublimed, this is because the sublimed quicksilver is deadly in several different ways.
If it is sublimed once, twice, up to seven times, it will attack the internal organs and heart however, in a way which can easily be cured and treated by medical methods. It will. in the beginning of the poisoning, cause much arrest of blood; one who swallows it will feel an unendurable pain in the abdomen and is rapidly killed.
Regarding the living (metallic) quicksilver, it is harmless; humans will only be frightened (by its coldness?). If it is harmful, it is only slightly and this is connected with the fright; only if some of it is poured into the ear or the nose will it kill or cause long-lasting disease.
The quicksilver which has been sublimed 30 times or more is a poison of great potency. A person who smells it (inhales) loses his memory and his wit, it causes the blood to stagnate, brings it to the pores of the body and will kill him rapidly. I do not doubt that it is more potent than aconit and the other strong, simple or combined poisons. It cuts the intestines and the stomach and throws them out in pieces. Recovery is possible, death more likely; if you do not hurry, no help is possible.
According to Lippmann (Origin and Extent of the Alccemy p 603), the story about poisoning through the ear is extremely old, also the use of mercury in the form of ointments against parasites.
It should be very valuable if persons who know middle age medicine could follow up the matters discussed above.
***
What killed Hamlet's father?
Hamlet, act I, scene V
Sleeping within my orchard,
My custom always of the afternoon,
Upon my secure hour thy uncle stole,
With juice of cursed hebenon in a vial,
And in the porches of my ears did pour
The leprous distilment, whose effect
Holds such an enmity with blood of man,
That swift as quicksilver it courses through
The natural gates and alleys of the body,
And with a sudden vigour it doth posset
And curd, like eager droppings into milk,
The thin and wholesome blood; so did it mine.
And a most instant tetter bark'd about,
Most Lazar-like, the vile and loathsome crust
All my smooth body.
Thus was I, sleeping, by a brothers hand,
Of life, of crown, of queen, at once dispatch'd.
What did he get into his ears? Hebenon extract or mercury? The symptoms described are those of mercury. Mercury has been used as a medicine against leprosy (and against almost every known disease, including mercury poisoning itself), but can cause skin eruptions and sensory loss, similar to leprosy. Hebenon extract (Henbane, Hyoscyamos niger) was probably used to induce a deep sleep before metallic mercury was poured into the ear, something which should be quite a noisy experience for the victim. It is certainly also possible that hebenon itself could cause death if it was poured into an ear. However, mercury in the metallic state in the ear was a known method of murder and probably Shakespeare knew about it. The first written record about this use of mercury comes from the arabian writer Gabir ibn Hajjan (dead about 820) in his "Book of Poisons". Gabir describes the effects of mercury: Quicksilver: This material belongs to the strong poisons, both when it is killed (oxidized, calomel?) and when it sublimes or is treated in any of the ways which are known to men with knowledge of the art (alchemy). The killed quicksilver causes strong stomach pains and pains like knife-cuts in the abdomen, anxiety, then arrests the movement of the blood and finally kills; however, the killed quicksilver is less dangerous than the sublimed, this is because the sublimed quicksilver is deadly in several different ways. If it is sublimed once, twice, up to seven times, it will attack the internal organs and heart, however, in a way which can easily be cured and treated by medical methods. It will, in the beginning of the poisoning, cause much arrest of blood; one who swallows it will feel an endurable pain in the abdomen and is rapidly killed. Regarding the living (metallic) quicksilver, it is harmless; humans will only be frightened (by its coldness). If it is harmful, it is only slightly and this is connected with the fright; only when some of it is poured into the ear or the nose will it kill or cause long-lasting disease. The quicksilver which has been sublimed
30 times or more is a poison of great potency. A person who smells it loses his memory and his wit, it causes the blood to stagnate, brings it to the pores of the body and will kill him rapidly. I do not doubt that that it is more potent than Aconit and the other strong, simple or combined poisons. It cuts the intestines and the stomach and throws them out in pieces. Recovery is possible, death more likely; if you do not hurry, no help is possible.
Rhazes (dead 925), another arabian alchemist, gives a description of mercury in the ear which indicates that they had really studied the effects: If quicksilver is poured into the ear there will be severe pains, followed by delirium and cramps. In addition it will feel like a heavy weight on the side quicksilver was poured. However, it is likely that there will be no severe effects if the quicksilver can flow out immediately. But if some mercury reaches the narrow passages in the ear, severe effects can be expected. Some doctors have told me that they have seen such patients get epilepsia followed by stroke.
A method to save victims of mercury in the ear was also described. Rhazes and later Gilbertus
Angelicus in Compendium Medicinae recommended that gold foil should be pushed into the ear to form gold amalgam which could be removed.
The Hazards of Mercury Vapor. Comments on the communications by Gradenwitz, Pinkus, Reihlen,
Ruska and Schmidt.
Alfred Stock, Berlin-Dahlem
Z. angew. Chem. 39, 1926, 790
I have, as Dr. Schmidt has written, not at all considered that "not enough has been published on the dangers of mercury" (the comments in my first paper only related to the hazards of mercury for chemists and physicists), but only that, as the communication by Ruska shows, also the oldest) is rich in papers on the damaging effects of mercury. I will only point out the very detailed work by A.
Kussmaul: "Studies on constitutional mercurialism and its relations to constitutional syphilis",
Wurzburg 1861. In this book several hundred cases are carefully described with all symptoms, nervous, catarrhic, those affecting the teeth and the gastrointestinal tract and several others. One obtains a thorough impression of the hell people had in the old amalgam mirror factories. The frank occupational mercury poisonings have become rarer after the mirror factories abandoned the use of amalgam; in wide circles one has forgotten what a dangerous and devoius poison mercury vapor is.
The former careful precautions have been neglected. Apparently not only in the scientific laboratories but also in the technical workshops! Reading the communication by Pinkus, one is amazed to find that amalgam for dental purposes can be manufactured without any special precautions. Pinkus is himself the owner of such a factory and must know the conditions. It is incomprehensible to me and certainly to anyone who knows the literature, that "there are also experiences which show that workers and chemists have worked in nearly mercury-impregnated rooms for decades without the slightest harm." A more careful study should lead to a less optimistic opinion. It must be noted that noticable damage from mercury vapor often might not appear for years
(therefore the case described by Reihlen that someone had worked for two years with mercury equipment, is not remarcable. Also in my laboratory some of the persons did not notice any consequences of a mercury exposure until years had passed.)
The symptoms can be restricted to nervous ones which the manual worker does not notice so much as far as they are endurable. To appear to be in good health means less; that can remain, as my own case showed, when mercury vapor already had caused pronounced nervous disturbances.
Mr. Pincus presumes that the problems in my laboratory were not caused by mercury but, at least partially, had a nervous origin. He mentions his own case which he blamed on a certain chemical
compound whereas his collaborators, working with the same compound, remained healthy. Our case is, however, different since all persons working in the laboratory, without exception, fell ill. In any case, neurasthenia does not produce salivation, mouth inflammations or loose teeth!
Mr Pincus refers to the "Arztlichen Merkblatter", which states that "mercury poisonings in Germany are rare." According to my experience, this is not true. I have received numerous letters and communications after the publication of my paper. They tell about many poisonings where the cause had been unknown.
And now to the objections on amalgam fillings by Gradenwitz:
It is certainly correct that the conditions for mercury evaporation from amalgam fillings are quite different from those in the laboratory experiments I described and where the amalgam was heated to
30-35 oC in vacuum. The smaller surface area, saliva, the lack of vacuum will reduce the mercury evaporation. Fortunately! If the fillings released mercury vapor that fast in the mouth they could be deadly! On the other hand, there are also conditions in the mouth which act to enhance the degradation of the amalgam fillings e.g. mechanical load on the fillings during chewing, chemical influence of the saliva etc.
However, even if the evaporation of mercury is far slower in the mouth, this can not cause the undisputable fact disappear from the world, that mercury in amalgam, even in the best silver amalgam, is volatile and has a noticable vapor pressure. Amalgam fillings must therefore evaporate mercury also in the mouth. How much and how fast is related to conditions in the individual case, to size and position of the filling, mechanical influence during chewing etc. Even if mercury evaporation in the mouth is only a hundredth or even a thousandth of that in the laboratory experiments, it must cause health disturbances during years and decades if the conditions are less favorable.
It is not at all, as Gradenwitz presumes, that the surface of an amalgam filling, after it has lost mercury, is poor in the metal and then does not give off any more mercury. On the contrary, the surfaces become rough, porous and fragile, mechanically more vulnerable (one can often clearly see scratches because of chewing), more easily abraded and new, mercury-rich layers are exposed. This can easily be seen on old fillings with the help of a microscope.
To add further data to our previous studies, we have measured how much mercury is released from silver amalgam fillings, still present in extracted teeth. They were placed in vacuum for 3 days at 30 oC, thus considerably below oral temperatures.
1. Three large fillings (surface area together 300 mm2) in two teeth (mainly chewing surfaces).
Evaporation: 150 mg mercury. A frightening amount!
2. A filling of relatively good appearance (70 mm2): 1.3 mg mercury.
Even a small, especially blank and smooth filling of only 25 mm2 surface area (not a chewing surface), released over 0.1 mg mercury in three days.
The damage caused by amalgam fillings should be of all degrees, realated to individual conditions.
From the most severe cases where there are a number of large copper amalgam fillings with a large surface area and which will lead to deterioration of body and mind, to slight, hardly noticable symptoms and to lack of noticable symptoms. I have not considered, as Pinkus writes "to recommend removal of all amalgam fillings". However, anyone who has symptoms which, without any other recognized cause, suggest a mercury poisoning, whether it is from his amalgam fillings, from occupational contact or from other causes (e.g. living in a room where a mercury thermometer has been broken), should as fast as possible have all amalgam fillings removed since he will be especialy sensitive towards even traces of mercury.
Amalgam fillings will always constitute a source of danger. Anyone who interprets my statements on amalgam fillings as a warning should interpret it as it was meant and not falsely. And when
"scared patients cause troubles for their dentists when amalgam fillings are suggested", it is for their own best and they have the right to have their very well founded suspicions taken into consideration.
It will certainly not be easy to find a good substitute for the easily manipulated, cheap and relatively long-lasting amalgam fillings. Maybe they can still be used, if they are small, in the milk teeth of children since they disappear again when the teeth are lost. The amalgam manufacturers should, however, be more concerned with the task of finding a harmless substitute for the amalgam than to fight against the well founded warning for mercury vapor.
In addition, one must point out that the removal of amalgam fillings must take place with extreme caution. When the amalgam fillings are drilled out, the inhalation of the fine amalgam dust which is produced, should be carefully avoided in order to prevent an even more pronounced damage by mercury.
I agree with Pinkus that it should be highly desirable to obtain the largest possible material, comparing the health status of amalgam carriers with the number, size, age and conditions of the fillings (which also recognizes the special hazards of neighbouring amalgam and gold fillings which
Gradenwitz pointed out). Such an investigation should as soon as possible be conducted by concerned authorities.
Amalgamfüllungen u. Quecksilbervergiftung
Umschau der Wissenschaft 30, 1926, 476-479
Dr. med. Fritz Kleinsorgen.
The publications by Professor Stock at the Kaiser-Wilhelm- lnstitut in Dahlem on mercury poisonings (Zeitschrift für angewandte Chemie Nr. 15, 1926), have caused considerable attention; especially the statements on the dangers of mercury poisoning by the use of amalgam fillings have caused considerable anxiety in a large parts of the population. Indeed, professor Stock states "that the thoughtless introduction of amalgam as a filling material for teeth was a severe sin against humanity."
If we consider that most persons in the population have amalgam fillings, often a dozen or more, we can understand the excitement which has been caused among all who have learnt about Stock's paper. Short reports in the daily press have made the widest dissemination certain. Just the renowned scientific place from which the warning for amalgam fillings has emanated makes it especially necessary for serious consideration.
Considering the ubiquitous distribution of amalgam fillings since decades, it is strange that the symptoms of chronic mercury poisoning has so completely escaped attention that they have remained undiscovered until now. One must therefore ask: Are the symptoms of poisoning so uncaracteristic that they could be overlooked by medical doctors or has professor Stock exaggerated with his warning?
If one reads the publications by Stock and studies his descriptions of his experiences of mercury on his own health, we certainly can understand that the slow, chronic poisoning by mercury vapor has a fluctuating course and can remain undiscovered. The symptoms of mercury poisoning, as they are described, is for a long time within the limits of general nervous symptoms as they appear in
neurasthenia or the nervous exhaustion which is characteristic of the stressed and overworked person in our civilization. It is therefore very difficult to distinguish between these diseases.
Memory disturbances, headache, dizziness, nervous unrest, vertigo, irritated mucosa, lack of initiative etc. were, according to Stock, present for 2 1/2 decades and worsened with time. However, these are also the typical symptoms of general nervousness in the population and offer nothing characteristic.
The characteristic symptoms of mercury poisoning like salivation, losened teeth etc. appeared first after 25 years of exposure to mercury vapor in the laboratories of the Kaiser-Wilhelm- Institute. This quickly led to the recognition of the true cause of the symptoms.
The development of the chronic mercury poisoning overlaps to a large degree with the development of nervousness caused by other conditions.
When now professor Stock, based on a series of experiments with amalgam fillings, states his conviction that they are harmful and constitute a sin against humanity, it is understandable that carriers of amalgam fillings with nervous tendencies (which should include the majority of persons with amalgam fillings), discover that they are mercury poisoned.
In relation to the anxiety which has been caused and already has resulted in the refusal to have amalgam fillings placed in dental clinics and the demand to have the already present ones removed, it is urgent for the involved circles to take a scientific stand to Stock's publications.
In this place one can add: amalgam are compounds of mercury and various metals like copper, tin, gold, silver. These compounds with metals are chemically labile and already strong heat will remove part of the mercury.
The experiments which professor Stock has made with both new fillings and old ones, were carried out in evacuated glass tubes where the amalgam-end wase heated to mouth temperature and the other end cooled to 0°C and partly even colder. After 8 to 14 days mercury was found in the cooled ends.
Such experiments do not prove the release of mercury in the mouth. Such pressure- and temperaturedifferences are not applicable to the mouth. Therefore it must be said that there is today no need to fear mercury poisoning from amalgam fillings under normal circumstances. However, this does not mean that they are completely nonexistent.
Under special circumstances mercury poisonings might occur. This depends both on the quality of the amalgam fillings and on special conditions in the mouth.
Amalgam fillings which have no defects do not have a risk of poisoning. However, earlier there were amalgam fillings which dissolved in the mouth. I do not know if they are still used. This relates to copper amalgam fillings. These were, and are if they are still used with the same composition, a constant risk for the carrier.
In addition, there might be circumstances which also make normal amalgam fillings risky.
When different metals in the mouth come into constant or intermittent contact, electrolytic processes can occur. Such processes are not rare when gold- and non-noble alloys are used for crowns and hooks for cautchuk dentures and these are in direct or intermittent contact with amalgam fillings.
Dentists should therefore be careful not to place crowns of gold or other metals on teeth which contain amalgam. One must then place a thick enough cement layer between the metals. One must also take care to prevent contact with fillings in neighbouring teeth. Dentures and hooks of metal must not come into contact with amalgam. It is also dangerous to the repair of old amalgam fillings.
New amalgam must not be placed close to old amalgam without a cement barrier; also one should avoid placing amalgams of different manufacture or composition close to each other.
Many dentists are ignorant and sin against these rules and they must especially have their eyes on these circumstances.
To reassure the public with amalgam and other materials one must state that there is no reason to fear any form of metal poisoning if the teeth are regularly carefully examined by a dentist.
Amalgam fillings and mercury poisoning
(Amalgamfüllungen u. Quecksilbervergiftung)
Umschau 30, 1926, 479
Dr. med. P. Windmüller
In dental circles, especially in America, there has been considerable argument whether amalgam dental fillings are acceptable or not. I have shown for over 20 years that it is possible to work without amalgam fillings and I have shown it in my own practice!
We are in the lucky position in dentistry to have materials available which can be incorporated in the body and teeth and which are not only neutral and biological, but which can have a health promoting effect on the cells in the tissues.
Scientific research and experience from clinical practice have confirmed this fact since several years.
Every alert doctor and especially dentist has without doubt noticed that the gingiva does not adhere closely to the teeth if it is in contact with amalgam. More or less dirt collects at these places and they will be inflamed. This is a proof that amalgam are foreign to the body and must be harmful, in contrast to fillings like cement, metal-cement, porcelain and especially gold-fillings.
When two metals touch each other, for example amalgam and gold in neighbouring teeth or opposing teeth which come into contact when biting, and the saliva har an acid reaction or acid food is eaten, then an electrogalvanic element is created. The more or less happy owner of such a battery experience an unpleasant taste, sometimes even electrical discharges with pain. The same happens with amalgam-filled teeth in contact with a denture hook of gold.
Gold has a yellowish color of its own. In the vicinity of a biting contact between an amalgam filling and gold or gold hook there will in most cases be a whitish discoloration of the gold together with a destruction of the noble metal. Every alert dentist can recognize it as a mercury deposit on the gold.
When a large number of amalgam fillings are present there will be a more or less strong evaporation of mercury which manifests physically as time goes by in the form of a contraction of every amalgam filling. This reduction in volume constitutes a certain hazard for the teeth and causes eventually "secondary caries", i.e. an empty space will form under the amalgam which will fill up with rests from food. The recurrence of caries is certain.
Certain diseases have to be treated with mercury. The patient will take on a pale color and the metallic poison leads through the saliva to severe gingivitis. Even if the amount of mercury from amalgam is much less than that used in the ointment treatments, it is completely certain that a reduction in the use of amalgam or the total abstaining of this questionable metal mixture for filling teeth will protect the patients from mercury damage.
Even if the majority of persons who have amalgam fillings do not have any health disturbances, such a negative finding is not proof of the neutrality of the amalgam filling material. If the dentist removes the amalgam fillings from a patient with many general health problems before these have become too severe, the problems will disappear within a relatively short time.
THE HAZARDS OF MERCURY VAPOR AND AMALGAM
(Die Gefährlichkeit des Quecksilberdampfes und der Amalgame)
Alfred Stock, Berlin-Dahlem
Zeitschrift fur angewandte Chemie, 39, 1926, 984-989
My warnings for mercury vapor and amalgam fillings have made a more than expected echo; in personal communications and letters, in papers in especially the dental journals and unfortunately often in erroneous desk products, published in the daily press.
I recently briefly reported at the Dental Society and at the Berlin Medical Association on the material I have received. The contents of these lectures will be published in "Medizinischen Klinik".
In addition and leaving out material which is already known by the readers of this journal, I will also publish it here since many collegues should be interested in the developments of this question.
Our experiences let us suspect that there should be many other victims of mercury poisoning besides us. Mercury is very much used in science and industry and is almost never treated with the absolutely necessary caution. Actually, conditions are much worse than we had expected. After the publication of my paper on the hazards of mercury vapor, I received a flood of written and oral communications, reporting of mercury poisonings of various severity, almost always with the same symptoms, all too well known by us and their cause not recognized. Often it was reported that the symptoms had slowly disappeared when mercury contact had ceased. The largest number of such reports were naturally from the circle of our own collegues, from chemical scientists and industrial chemists, people I was personally acquainted with or met at conferences. Today I know nearly 50 chemical scientists who suffer, or have suffered from chronic mercury poisonings; among these persons there are several well known scientific names. Also in the chemical industry the mercury poisoning turned out to be relatively common. Certainly I have only obtained reports on a small fraction of all poisonings. There must be many more cases also among physicists; these use in general even more mercury than the chemists and often handle it very carelessly. Also from other groups: technical, medical, dental, teachers, many letters told about mercury poisonings. The contents were nearly always the same: "When I read your paper, the scales fell from my eyes and I now finally know the cause of my problems; my doctors have not recognized the cause etc."
Sources of the mercury vapor poisonings were, in addition to scattered and in cracks of the floor discovered mercury, work with mercury switches, mercury retifiers, mercury seals of tube connections, ozone equipment, mercury air pumps and other mercury apparatus, use of alkaliamalgam for chemical reactions, prolonged stay in rooms where earlier a thermometer or a barometer had been broken etc. In most cases one could estimate that the mercury levels has been equally low as in our laboratory.
From many of the communications one could learn about the despair the affected persons felt in their condition which affected their work and the ability to carry out the tasks their position required.
As examples I will cite some passages from letters. They come from known scientists:
Dr. H wrote: "In november 1924 our institute bought an apparatus for exact gas analysis according to Ott; Mercury was used as a sealing liquid", and he reports of several mercury poisonings, both his own and his collaborators, because of this apparatus. For instance: "Dr. G, then scientist at our institute, suffered during the time we used mercury and also afterwords, from constant tiredness. He complained about loss of memory, had problems from his teeth (bleeding gingiva). I met Dr. G. at the Kiel meeting. His problems have now nearly disappeared. He left us a year ago."
Dr. S. now director of a research institute and earlier working in a chemical factory, reports on a mercury poisoning he acquired when mercury was used to seal tubing: In the beginning I had light headaches, then more severe and with shorter intervals. I had also a profound unrest which affected me more and more. As especially characteristic I find the sensitivity to colds, affecting the respiratory organs and causing inflammations of the nose and nasal mucosa. A doctor I asked for advive suggested that the symptoms were caused by a latent spanish flu. The formation of vesicles and inflammations of the tongue, especially at the lower end.. appeared about three years ago. These symptoms were especially painful. The doctor explained also these symptoms as caused by flu...
Bleeding of the teeth during the slightest brushing.. In addition to the above symptoms I had also an ever increasing tiredness, pains in various places and a profound need for sleep." Dr. S tells about another collegue in the factory who also suffered from mercury poisoning. "Concerning myself, I felt a clear improvement, apart from the bleeding gingiva and some dizziness, after I had left my work at... "
Dr. Kolle, director of the Inst of Experimental Therapy in Frankfurt, also reports on his own and others mercury poisonings. "I have suffered for years from the same symptoms you have described.
In addition to rather severe disturbances of the gastrointestinal tract, primarily the nervous disturbances were quite similar to those you have described. I was, for a long time, not aware of what the cause of my healt disturbances was.. later completely healthy although I, at the time, had the impression that I suffered from a rather severe disease.. Many of my collaborators had quite similar experiences."
From a letter by the laryngologist prof. G. in Berlin: "My patient, chemist at a large company here, suffered from general tiredness, severe inflammation of the mucosa near the teeth and severe catarrh of the upper airways. He complained less of headache but one could notice profound change in his appearance. In the beginning of the treatment he liked a glass of Moselwine but after some months he lost interest in life and became depressed. On my advice he visited a dental expert.. The patient was then sent to various resorts by us, however, when he came back to Berlin he became sick again.
Finally he himself got the idea to search his laboratory and found in the floor considerable amounts of mercury. After this adverse condition had been corrected, he recovered remarcably fast from both the symptoms in the upper airways and primarily in general health."
Compare the communication by L. Wolff (Z. angew. Chem 39, 1926, 789). This might be sufficient.
I could add considerably more material.
However, it has been demonstrated that prolonged inhalation of also very small amounts of mercury
(daily hundredths or thousandths of a milligam) cause health disturbances. These are in the beginning very non-specific and affect mainly the nervous system and the upper airways (primarily the nasal mucosa; this is repeatedly pointed out in the communications), usually without the mouth
inflammations, otherwise considered characteristic for mercury poisoning. The symptoms generally agree for all affected persons. If there is immunity against the effects of mercury, it is rare.
Metallic mercury is one of the most insidious of poisons because of its volatility, lack of smell and insidious effects with aftereffects for years. These can so far only be helplessly endured. In addition to the cases of certain mercury poisonings there is certainly an even larger number where the symptoms restrict themselves to the first stages, a depression of intellectual capacity without any other signs and the real cause is never known. If they are noticed, they are explained by overwork, nervous exhaustion, age etc.
However, the hazards of mercury are not only a matter for scientists. Also other groups are threatened by it. Consider e.g. mercury thermometers. Many mysterious disease cases might be caused by the breaking of a mercury thermometer in a living room and the scattering of its contents as dust in cracks and joints. The amount of mercury in a thermometer is quite sufficient to give the air a harmful level of mercury for years. What is sooner or later the fate of almost every fever thermometer? One day, when it is hurled to press down the mercury, it slips from the hand and is broken; this mostly even happens in a bedroom. The possible consequences can readily be imagined: tiredness, unrest, dizziness, headaches, catarrh, gastrointestinal troubles. The cause will hardly be recognized by anyone; the breaking of a thermometer can even have been done by someone who lived in the room earlier. If the problems in such cases are caused by mercury can only be clarified with an, unfortunately not so easy, air analysis or the finding of mercury droplets (magnifier) in the joints of the floor boards.
Much more important is the general use of mercury in the form of amalgams for dental fillings.
Originally the dentists only used copper amalgam. This is bought ready-made, is heated by the dentist and then softens; in the tooth it rapidly hardens. The later introduced, so-called silver amalgams, are prepared otherwise. The commercial metal alloy (a third to two thirds silver, a few hundredths of other components and the rest tin; if it contains platinum or gold it is called "platinum amalgam" or "gold amalgam") contains no mercury. It is mixed with mercury by the dentist; a plastic amalgam is formed, which also hardens after a short time. The amount of mercury used for the preparation varies within large margins according to the methods practiced by the dentist. He subsequently presses out excess mercury from the plastic mass. The mercury content of the final filling can therefore be very variable.
The filling with amalgam is also a hazard to the dentist himself since with common practice mercury evaporates and mixes with the air. The copper amalgam gives, when it is heated and especially when it is heated more than necessary, off considerable amounts of mercury as vapor, mercury which can precipitate as a fine dust in the surroundings. When silver amalgam is mixed and even if instructions are carefully followed, the pressed out excess mercury will often be left in the room for a considerable time or falls even on the floor. The dentists handle mercury very differently but are apparently often too careless. The beginning of chronic mercury poisonings are not rare among them, among older ones even rather common. This is shown to me by communications I have received. It can also be found in the literature. Before my own paper on the hazards of mercury appeared, Dr Lowy (Medizinische Klinik 1926 p 608), for instance, wrote in a paper on occupational diseases of doctors : "Also dentists are threatened by mercury.. even if they have not symptoms of an acute poisoning.. , general tiredness, loss of interest in work, easy exhaustion, irritability, anxiety, loss of sleep and general decrease in psychic ability is apparently caused by a latent, chronic mercury poisoning." And Dr. M. Jarecki, himself dentist, writes (Zahnärztliche
Rundschau 35, 1926, 327): According to the urine analysis by Schulte (who found considerable amounts of mercury in the urine from almost every examined dentist) it seems very likely that the considerable nervousness which many dentists show, has its cause in an insidious mercury vapor poisoning." Considering our own experience one must agree with this conclusion. If the dentists should use amalgam, they must be far more careful than now in order not to be endangered. A simple exhaust which leads to the outside must belong to the equipment of the operatory (it is easy to obtain one equipped with a small electric fan). All handling of mercury and amalgam should take place under this exhaust. Naturally, rests of mercury and amalgam scrap must be stored tightly sealed.
Concerning the hazards for the carriers of the amalgam fillings, there is certainly a large difference between copper and silver amalgam (and the varieties of these).
Copper amalgam is strongly degraded in the mouth. It will be generally degraded and fragile, gives of copper and copper compounds and simultaneously mercury is released, often in the form of visible drops. The copper amalgam is degraded and disapperars with time. As it appears today, copper amalgam has no defendant any more among the professionals, although it was highly praised when it was introduced, also because of its desinfecting properties! In a statement at the
Brandenburger Dental Society meeting, june 5 this year, a meeting which dealt with the amalgam question, I heard, to my astonishment, distinguished spokesmen of the dental profession say that
"copper amalgams should not even be discussed". The well known Wurzburger pharmacologist F.
Flury recently wrote (Münchener Medizin Wschr. 73, 1926, 1022) about the "old binary copper amalgams with their unsuitable composition and which can produce mercury droplets" and about the recognized defective copper amalgams". These "recognized defective" copper amalgams are, however, extensively used in Germany, in the insurance-paid practice they are even dominating dental filling materials only because they are cheap and very easy to manipulate. One can ask: How is something like this possible? and must sincerely wish that concerned authorities, e.g. the Ministry of Health, brings this question up to discussion as fast as possible.
The silver amalgams are more durable, more mechanically and chemically resistant. However, also these change slowly in the mouth and their surfaces become rough, scratched and fragile, something which can easily be seen by a microscopical examination of older fillings. New layers of amalgam will continously be exposed. Freshly prepared amalgam will even give off much mercury vapor. But also after long storage and after long use in the mouth they give off considerable amounts of mercury as vapor, at least such amalgams as are used in practice. We have published such laboratory experiments (Z. angew. Chem 39, 1926, 791). The results are confirmed by the following experiment which we made with one of our collaborators at our institute, Dr. D.:
D. has about a dozen fillings of good appearance in his teeth which always were kept in good order.
Most of them are silver amalgams; maybe one or two are copper amalgams. He held a glass tube between his closed lips and we let about 400 l air pass from his nose and out through the tube by suction. The air was led through liquid air and the condensed liquid was analyzed for mercury as previously described. Result: weak but clear mercury reaction. In a control experiment we of course determined that the air in the room was mercury-free. It should be emphasized that nothing had been done to Dr. D.'s fillings for three years. After this experiment Dr. D. had a new silver amalgam filling placed. When we repeated the experiment four days later, the mercury reaction was considerably stronger. Quantitatively such experiments tell little since of course only a small fraction of the air stream comes into contact with the dental fillings and since also the saliva flows especially much when you have a an unusual thing like a glass tube in your mouth. Qualitatively, however, the results are quite convincing.
In addition it is not at all stated that amalgam fillings are harmful because of evaporated and in the lungs inhaled mercury exclusively or even mainly. Also the mercury which enters the gastrointestinal tract because of the general destruction of the fillings and that in very finely divided and almost atomic condition should be absorbed in a similar way as the inhaled. The genrally known fact that large amounts of mercury in compact form can be swallowed and passes without harmful effects through the body, will not, because of the enormous difference of the mercury surface, contradict this presumption.
When I pointed out, in my first publication, the possibilities of harmful effects because of amalgam fillings, there was a storm of distrust and protests from wide dental circles (e.g. P. Ritter, Zahnärztl.
Rundschau 35, 1926, 415). Nobody had observed any mercury poisoning among millions of persons who had amalgam fillings! Others meant that that the very few cases of harmful effects because of mercury from amalgam were "idiosyncrasy". What is this idiosyncrasy? Nothing else than a high sensitivity towards mercury. Our observations now clearly demonstrate that many, apparently most, humans are sensitive towards mercury. Thus, mercury-"idiosyncrasy" can not be dismissed that simply.
The dentists are seldom in a position to recognize general effects of amalgam fillings or even to learn about them. When the patient suffers from nervousness, intellectual exhaustion, catarrhs etc. they do not go to the dentist whom they also usually do not tell about their problems since they are prevented from talking during the treatment. The family physician, nerve specialists, laryngologists, internists are the ones they discuss these problems with.
The dentists who try to give the impression that the amalgams are harmless also quite forget the strong opposition amalgam met from the beginning among physicians and dentists and still meets.
Just two recent voices:
Dr. P. Windmüller (Die Umschau 30, 1926, 479): "Every alert physician and especially dentist has undoubtedly in his practice had the opportunity to observe that the gingiva does not adhere firmly to places where it comes into contact with amalgam.. Even if most of the patients who have amalgam have no noticable disturbances in healt, such a non-demonstration is not at all a proof of the neutrality of the amalgam filling material. If the dentists remove the amalgam fillings from patients with many general problems and fill the teeth with neutral material, the problems disappear within a relatively short time."
Dr. Lichtwarck (Zahnärztl. Rundschau 35, 1926, 363): "I have, since a long time, observed the harmful effects of mercury from copper amalgam fillings. I do not place copper amalgam plombs since many years. I have in my practice recorded a considerable number of cases where I suspected them to cause headache, discomfort, indisposition, strong salivation, neurasthenic symptoms and stomach problems and where a spontaneous disappearance of the problems occurred when they were removed."
A German-American writes me from New York that dentists there do not use amalgam since years ago. He adds an objection to the german dentists views on the warnings for amalgam "this should reduce their reputation in the opinion of famous dentists here". Whether this information is correct I certainly do not know.
When one knows that already extremely small amounts of mercury are harmful to humans and that amalgam filling continously give off mercury to the body, one will be convinced that amalgam fillings are objectionable. This view has been supported by numerous communications which I obtained because of my paper.
I will describe one case in detail since it is important for judging in this question. It concerns the well known, today again healthy and working, professor of psychology at the University of Marburg,
Dr. E. Jaensch. From the report prof. Jaensch wrote about his experiences with amalgam fillings and which he generously allowed me to make public, I will cite some parts:
"You do humanity a favor when you take up the question about amalgam. At about the age of 15 my teeth were, as the saying is, put into order. I had fillings in a large number. Gradually persistent troubles appeared which first restricted themselves to the nervous system. The condition was diagnosed as "hypochondriac neurasthenia" since the symptoms were only of a nervous character and since I in general appeared to be in good health.
At the end of my student time I had again distinct nervous and also bodily symptoms. The troubles increased year by year. The beginning of the deterioration was clearly associated with an unusually large and especially unskillfull dental treatment. I had mostly so called contour fillings and a distinguished dentist now told me that "to prevent anything more from happening" he had to connect the adjacent fillings in the molars and he made these solid connections.
From 1909 my condition deteriorated... chronic, worse and worse diarrheas. 1912-16 I had to go to the toilet ten or more times each day and it is understandable that I lost much weight. In addition I had intense pains in all parts of my body.. I could sleep less and less, ..inflammations in my mouth with increased salivation.. worse inflammations in the upper airways, especially in my throat.. painful asthmatic condition, intense anxiety and deterioration of my physique so I could only leve my bed for short times.. complete impairment of my intellectual abilities.
I was on sick-leave since a year and my life was a futile wandering around to medical specialists in
Baden-Baden, in hopeless resignation, when I there in summer 1916 met my former aquaintance prof. Sommer from Giessen. I told him about my condition and also of a recent thought. Suffering from toothache I had, in front of the mirror, contemplated my set of teeth with its in part very large amalgam fillings (18 silver amalgam fillings). Then I had recalled a remark which I had often heard from my doctors. I had suggested also unusual causes, also that I had contracted lead poisoning because of work with accumulators. From the physicians I then got answers like: You have certainly not a lead poisoning, the symptoms are more similar to a mercury poisoning. But that's an impossibility - where should that have come from?
When I now contemplated the large amount of amalgam in my mouth I got the idea that might it not after all be a mercury poisoning? Sommer then told me that he had a significant number of similar cases where the puzzling disease state upon closer examination had turned out to be toxic polyneuritis.
My urine and saliva were tested for mercury. The clinical and chemical examination gave the results which are written in the records of prof. Sommer. (In these records from 1916 one can read: In the urine was mercury in considerable amounts. In the saliva mercury could not be detected with certainty. The source of the mercury seemed to be the many amalgam fillings the patient had in his mouth for many years. the previous history fits completely the assumption that it is a toxic disease caused by mercury).
Now, however, we faced the almost impossible task of finding a dentist who could be persuaded to take out and replace the fillings. Again and again I was dismissed. everywhere the dentists pointed out that the harmlessness of the amalgam plombs was proved, therefore the records from Sommer could not be believed and that no dentist from a dental standpoint could take the responsibility for such a large and "unnecessary" operation. Prof. X at the Emperors court, told me: "You can send me reports from all the medical specialists in the world - I do not believe it."
And all that only because Witzel was said to have proven the harmlessness of amalgam fillings, partly against a considerable resistance against the older dentists. When I had obtained Witzel's book
(Witzel: Das Füllen der Zähne mit Amalgam, 1899; Witzel played the same role as Black in the
USA, transl. note) I was shocked by the shallowness of these proofs..
It might not have been possible to find a dentist who could exchange the fillings if prof. Binswanger had not explicitly asked a relative of his who was a professor of dentistry. When the large plombs were drilled out I had increased troubles... when we sucked away the amalgam dust during the rest of the work the problems did not appear.
Immediately after the removal of the amalgam fillings a considerable improvement of especially the diarrheas started, at least compared to the previous condition. Even if the rest of the recovery was slow.. the time of the amalgam removal was a turning point after which all symptoms from the digestive and respiratory organs as well the nervous system, steadily decreased so that now, for the first time, I really know what it is to live.
Only time has really helped me, after the exchange of the amalgam fillings for gold, everything else only to a small extent.
How many people might suffer in the same way, even if it is to a lesser degree and how many such cases might forever remain undiscovered?
Prof. Jaensch deeply affecting story needs no comments. It generally agrees with the experiences we unfortunately had ourselves.
This severe case is not at all the only one. Dr W., chemist, wrote me: "When I read your paper in Z. angew. Chem....I found the symptoms of my wife described in every detail... strong catarrhs of the upper throat... headaches and vertigo up to being unbearable.. tight nose, pains over the eyes
(diagnosed as sinusitis by the physician)... the condition needed medical care during the latest two years because of psychic depression which added to the continously increasing bodily problems
(neuralgias in face and head, painful cramps in the liver area)... eleven amalgam fillings (the oldest and biggest ones of copper amalgam).. the fillings were immediately removed. Then they turned out to be i a very bad condition, especially the copper amalgam filling in the molar was fragile and with a completely changed color. ... Undoubtedly the most severe symptoms from the throat, the changes of the oral soft tissues, the neuralgias and the pains of the liver have disappeared. The psychic depression has also continously improved; there is no doubt about it although the improvements take longer time than with the above described symptoms."
A quite similar case with an elderly woman is described by Dr. Lichtwarck (Zahnärztl. Rundschau
35, 1926, 363): tiredness, loss of sleep, easily irritated, tinnitus, sick feeling etc. up to a suicide attempt. Treatments without results by stomach- and nerve-specialists until the removal of a large amalgam filling with a gold crown finally brought complete health. Amalgam and gold next to each other is, because of the electrolytic processes which then appear in the mouth, dangerous and should be avoided; compare also e.g. Dr. G. Haber, Zahnärztl. Rundschau 35, 1926, 395.
In the literature one can find descriptions of many similar cases. I also know several similar cases among my own aquaintances. We analyzed the urine of two of these and it did contain mercury.
The problems must certainly not always be so severe. The effects of amalgam will pass through all stages according to number, condition and position of the fillings; from the most severe cases of psychical and physical deterioration up weak, hardly noticable symptoms or from the affected himself not noticed effects (depression of intellectual functions). On each severe case there will be a hundred, maybe a thousand or ten thousand slight ones. Alert medical observations, directed at the connections between the amalgam fillings and the symptoms of chronic mercury poisonings, should soon produce important information. That such information really exists, apparently to an amazing extent, seems certain from the reports which voluntarily are sent to me. Again and again is reported, that after placement of amalgam fillings, symptoms which had not been present before, appeared: dizziness, vertigo, bleeding gingiva, chronically running noses and catarrhs (the location was almost always the connection between throat and nose) etc. In cases where the amalgam fillings, because of tooth extraction or falling out, had been removed, the problems had slowly again disappeared.
The recognition of the beginning of a chronic mercury poisoning is not simple since the first only psychic and nervous symptoms are so little specific (They appear, with the exception of mouth inflammations, also in other chronic poisonings, e.g. by arsenic or hydrogen sulfide). They are more reliable when also chronically irritated nose and catarrhs, oral symptoms (vesicles, bleeding gingiva, loose teeth), diarrhea etc appear. The most convincing fact is certainly the demonstration of mercury in saliva or urine; this requires a certain training and skill when the amounts are small (the chemical laboratory of Dr. A. Buss, Berlin SW 47, Grossbeerenstr. 31, has already declared that they can determine mercury according to our methods). As we have already demonstrated the excretions are often periodically mercury-free although mercury poisoning has been present and mercury is still in the body.
In most of the severe cases known to me, there have been copper amalgam fillings present. How extensive the damage because of silver amalgam is, must be determined on a larger study group. The possibility for such damage exists since also the silver amalgams give off mercury in amounts which are harmful because of the high sensitivity of many persons towards mercury.
These important questions demand the attention of all physicians. Perhaps it should be useful if the
Ministry of Health published a mercury bulletin, similar to the lead bulletin, where questions could be resolved. The fight against the copper amalgams as dental filling materials should immediately be taken up.
The dental profession, as told above, at first completely dismissed the matter but now quite other views can be heard from these circles. For instance, at the end of a recent paper by Dr. A.
Werkenthin (Zahnärztl. Rundshau 35, 1926, 451) one can read: "If this "amalgam-alarm" results in a prohibition of copper amalgam fillings (as lead fillings, plombs, once were prohibited), then we should be grateful for this sound scare (alias shaking-up)."
Fortunately the medical profession gives the question of chronic mercury poisoning their attention.
Dr. His reports in the Medizinischen Klinik: "The discussion of Stock's report in the the medical and dental profession has resulted in the desicion that it is necessary to clarify to what extent damage because of chronic mercury poisoning, especially from amalgam fillings, exists. Therefore a place must be organized where people, who think that they have mercury poisoning, can be carefully examined, both regarding their symptoms, the condition of their plombs and the presence of mercury
in the urine. Such an institute will be arranged at the 1st Medical Clinic where a physician and a dentist and it will also be arranged that the urine of the patients can be analyzed for mercury according to the methods which Stock has developed. The organization of this examination and councelling place will take a few weeks; according to our plans it will open in the middle of september and the medical profession will be notified about it in due time."
Then this question will be in the right hands and one can calmly wait for the results of this professional study without further involvement of the press.
Mercury poisoning, caused by amalgam fillings
Quecksilbervergiftungen, von Zahnfüllungen ausgehend
Prof. Dr. E. Meyer, Berlin
Die Medizinische Welt, 4, 1930, 703
In No. 9 of Med. Welt Arnoldi makes his collegues aware of mercury poisonings, caused by Hgcontaining air in laboratories. I would like to point out another source of poisonings - the amalgam fillings which, despite the publications by Stock and others, have not received enough attention in medical practice. Two recent similar observations makes me emphasize this type of etiology for Hgpoisonings.
Case 1. The 7th. of januar 1930 Mrs. R.F., 40 years old, came to my practice. She complained of burning tongue, especially in the mornings and evenings, not related to type of food, of mouth and throat dryness and of gingival inflammation. General health, sleep, appetite and gastrointestinal tract were disurbed, menstruations irregular. The patient is depressed, can not concentrate enough to read books. Earlier she was an intellectual and had several such interests. She complained ove pins and needles and numbness of her hands and feet. She had lost 10.5 kg in one year. The patient considers her illness caused by a gastrointestinal catarrh one year ago. Because of her oral problems she had been under dental treatment for a long time.
At examination I found a glossitis superficialis with rather unaffected margins of the tongue, some rest signs of a gingivitis and a chronic tonsillitis. Inner organs nothing notable, slightly exaggerated reflexes. The discrepancy between the few objective changes and the strength of her problems was remarcable. The blood examination by prof. Schilling showed an atypical picture with elevated leucocytes and low color index which indicated a toxic anaemia, originating in the gastrointestinal tract. Since no other changes other than hyperacidity were present in the gastrointestinal tract, I looked for other explanations to the blood changes and the clinical state. I found a number of old amalgam fillings in her teeth, something which made me suspect a Hg-poisoning. I therefore asked the treating dentist to remove the fillings which partly consisted of old, degraded copper amalgam fillings. At the same time I sent an urine sample for mercury analysis to the Hauptgesundheitsamt.
The result was 4/1000 mg Hg, calculated on a daily urinary volume of 1,5 liter urine.
The result of the removal of the fillings was rather remarcable. Within a few weeks the patient had recovered completely, she is again healty to body and soul. The depressive state has disappeared, the gingiva has healed; the only remaining symptoms is a lightly burning tongue, however much less than earlier.
From the clinical story the diagnosis is evident. The finding of Hg in urine explains the clinical picture and the blood changes completely. That the copper amalgam fillings were the sole cause of the mercury intoxication is evident from the lack of any other contact with mercury and from the improvement in health in direct connection with the removal of the fillings.
Case 2. Mrs. G.M., 32 years old, complains since a long time over burning mouth and throat, over tiredness, lack of appetite, gastrointestinal disturbances, poor sleep. She connected her problems with her pregnancy. However, since no improvement had occurred six weeks after delivery, Prof.
Paul Strassmann sent the patient to me. In addition to a light rhino-pharyngitis I found a swelling of the right margin of her tongue with clear impressions of her teeth, a thin mucosa. No changes in the gingiva or inner organs.
In the molars there were fillings of both copper- and silver amalgam. Since also in this case there was a remarcable discrepancy between the complaints and the objectively demonstrable changes and there was no other obvious cause, I thought about a Hg-poisoning from her amalgam fillings. I therefore had the copper amalgams removed. The urinary analysis at the Hauptgesundheitsamt showed 6.25/1000 mg Hg, calculated on a daily urine volume of 1500 ml. The effects of amalgam removal were not that remarcable as in case 1. According to a letter from the patient, who departed soon after the amalgam removal, the symptoms had diminished after 14 days, but not disappeared.
This is, however, not remarcable since it usually takes a long time to improve after a mercury poisoning.
Based on these observations I would like to stress that Hg- poisonings are more common than generally thought. In cases where a mercury poisoning might be suspected must, if no other cause is found, the amalgam fillings be considered. If such fillings are present, their immediate removal is absolutely necessary. A urine- and feces-analysis must support the diagnosis. Therapeutically, after the removal of the fillings, one must enhance elimination of mercury from the body by a healthy lifestyle and by medical treatment and to assist a general improvement in strength.
Discussions about the hazards of amalgam were also published in other journals than the chemical ones.
Some abstracts, mainly collected from: Huber CD, Darstellung der durch Stock ausgelösten
Diskussion um das Problem der Schädlichkeit von Amalgam-fullungen an Hand der Litteratur.
Dissertation from the Klin. f. Zahn-, Mund- und Kieferkrankheiten, Munchen 1957 (Report on the discussion, caused by Stock, on the problem of the hazards of amalgam fillings, according to literature, 54 pages). This seems to be a fairly accurate report on the discussion from 1926 to about
1931. Huber does not judge who was right or wrong but his recommendations are that copper amalgam (with or without additional metals) should never be used and silver amalgam very conservatively e.g. never on occlusal surfaces if it comes into contact with an antagonist tooth, never when the cavity borders on the gingiva etc. The removal of old amalgam should also be done very cautiously to prevent poisoning of patient and dentist.
Abstr: Mayer, E. (Prof. Breslau) Untersuchungen von Amalgam auf die Abgabe von metallischem
Quecksilber. Dtsch. Monatschr f. Zahnheilk. 1927 p226. Mayer used Stock's method with amalgam in closed glass tubes; the amalgam part heated to 37 degrees and the other cooled in ice. The experiments were conducted at atmospheric pressure in contrast to Stock's. Detection of mercury was by weighting any distilled mercury after three weeks. Results:
Copper amalgam 0.640 - 0.960 mg
Silver amalgam 0.130 - 0.265 mg
Conclusion by Mayer: Since every human, whether he has anything to do with mercury or not, daily excretes up to 0.5 mg mercury as something completely normal, then silver amalgam can be considered harmless, but copper amalgam, with its high release of mercury, must be considered
harmful. Copper amalgam should therefore not be used but only silver amalgam. (transl. note:
Whether the figure in the original paper really is 0.5 mg has not been controlled. The experiments confirm the results by Stock and that without vacuum).
Rohrer, L. Gibt es eine chronische Quecksilbervergiftung durch Amalgamzahnfullungen? Munch.
Med. Wochenschr 1927, p 1346: Can amalgam fillings cause a chronic poisoning? Rohrer finds that dental metallurgy has advanced so much because of its systematic studies of amalgam, that today there are amalgams on the market which are without objection. These can certainly not give off any free mercury if they are correctly prepared. This does not apply to all kinds of copper amalgams, with or without additions. These should not be used because of their mercury release which can not be denied, also after they have reached their final hard condition. Stocks's studies could, however, not be confirmed by most experiments afterwords. Especially the in vitro experiments can not be compared to oral conditions. It must be the task of internal medicine, neurologists, rhinologists and dermatologists to collect observations since the very first symptoms of chronic mercury poisonings can be expected in these areas. The pharmacologists have in general dismissed the possibilities of chronic mercury poisonings because of amalgam fillings.
Werkenthin,A. Kupferamalgam uber Bord, Zahnarztl.Rundschau 1929, p451. Copper amalgam overboard is the absolute requirement from Werkenthin. Rests from copper amalgam fillings must be completely removed before a new silver amalgam filling, which is completely harmless, is placed.
Also the neighbouring tooth and antagonists must not have copper amalgam fillings. Silver amalgam does not at all prevent the placement of 22-carat gold rings for crowns or caps. It is, however, necessary to wait 5 days after the placement of amalgam before the ring is placed. Silver amalgam beneath a gold cap can even be considered recommendable. If the amalgam-alarm from Stock could bring the authorities to prohibit copper amalgam, then we should be grateful.
Witzel, A. Zur Frage der Quecksilbervergiftung durch Zahnfullungen, Munch. Med. Wochenschr.
1926, 1021 (Author of the previously mentioned book) wrote: Based on own extensive studies the presence of large copper amalgam fillings when the saliva is very acid, might be harmful to health.
The gold- or platinum- containing silveramalgam fillings are without objections and constituted completely harmless filling materials. When properly prepared, amalgam fillings of silver-tinmercury alloy, contain no free mercury. Thus they can not give off free mercury in the mouth. The levels of mercury vapor should be minimal in the oral cavity. The possibilities for mercury poisonings from dental fillings seem today, with the improved amalgams, much less than previously and even then the recognized faulty copper amalgam fillings only rarely led to noticable damage.
Anyhow, one should for ever leave copper amalgam and specialize on noble amalgams.
Schoenbeck, F. (Prof. Biesenthal) Die Amalgamgefahr, Zahnarztl Rundschau 1926, 415; Gefahren der Amalgamfullungen, Zahnarztl. Rundschau 1926, 449; Amalgamfullungen und
Quecksilbervergiftung Deutsch. Monatschr. Zahnheilk. 1926, 435; Die Amalgamfrage, Munchn.
Med. Wochenschr. 1927, 1694; Untersuchungen uber Quecksilberausscheidungen bei Tragern und
Bearbeitern von Amalgamfullungen Dtsch. Monatschr. Zahnheilk. 1927, 208; Schadlichkeit der
Amalgamzahnfullungen Zahnarztl Mitteil 1928, 390; Zur Amalgamfrage Dtsch Zahnarztl Wschr
1928, 151. The question of poisons can not be simplified since all metals have a certain toxicity. In addition, the preparation and the conditions in the oral cavity will have influence. Experiments have shown that copper amalgam, before and after preparation, at 37 degrees continously releases mercury vapor. Microscopical examination of copper amalgam in fillings shows clearly free mercury, containing some copper, besides pieces of copper. This is understandable since the solubility of copper in mercury is small.
From these facts one must conclude that pure copper amalgam must disappear since these might be dangerous. However, these hazards can be reduced by addition of 2-3% tin. Then such combined copper-tin amalgams can be used without hesitation. Concerning the noble amalgams, conditions are quite different. The reaction products are Ag3Sn, Ag3Hg4 and mixed crystals of tin and mercury if the proportions during mixing are correctly chosen. One can thus state that such a correctly prepared noble amalgam, after complete hardening, should constitute no risk for the patient. However, this only applies to conditions when the alloy has been manufactured on a scientific basis and the proportions between alloy and mercury is correct; most amalgam fillings, prepared according to practice up to now, have an excess of mercury. Especially the electrical processes which can occur when amalgam fillings come into contact with gold fillings have been observed by Schoenbeck. The amalgam filling will be the less noble electrode with the potential of tin and dissolve and its corrosion potential will partly be carried over to the gold. Mainly tin will dissolve. Even if an immediate danger for mercury poisoning because of corrosion does not exist, one must consider that the amalgam surface is changed because of the dissolution of tin, e.g. it will be enriched in silver and mercury. The resistance agaist mechanical influences will then be reduced and there is the possibility that mercury-containing pieces are released and taken up by the body. In any case, contact between amalgam and gold alloys should be avoided if the saliva as electrolyte has access to both.
Feiler, R. Ein Beitrag zur Amalgamfrage, Zahnarztl. Rundschau 1927, 797-98. Feiler points out the dangers for the dental personell in addition to that for the patient and that amalgam can not at all be considered an ideal filling material. The use of copper amalgam can not further be trusted because of the reasons Stock has given and which he completely supports. But not only the copper amalgam fillings but also noble (silver) amalgam fillings undergo changes in volume and marginal adaption, despite careful preparation. This should mean a reduced use of amalgam fillings and duty to search for a substitute. Feiler finds that the cast silver filling and a new type of porcelain are good substitutes.
Seifert, K. Zur Streitfrage uber Quecksilberabgabe aus Amalgamfullungen. Zahnarztl. Rundschau
1926, 516. supports Stock's conclusions to some extent because of his own experience. He has concluded, based on observations, that persons with amalgam fillings have extremely little syphilis, that mercury in the fillings must act prophylactically against luetic infections. Thus, a continous uptake of mercury in the body must take place, an uptake which immmunises the body against lues without harming the body. The uptake is not of the extent that one has to fear a mercurial poisoning.
Joachimoglu, G, Die Gefahrlichkeit des Quecksilberdampfes. Med. Klin 1926, 1275. J. has the opinion that the statements on the hazards of amalgam fillings can not be correct. The removal of amalgam fillings, which Stock and Lewin recommends, is an exagerration. The mass experience has shown that poisonings do not occur with these compounds. Single cases, where the symptoms disappear after removal of the amalgam fillings, prove nothing since these are contradicted by millions of cases where amalgam fillings, even after 25 years have not led to any symptoms at all.
The syndrome, which Stock describes as light mercury poisoning, is difficult to differentiate from neurasthenic symptoms which are so common today. When the symptoms disappear after the removal of a small amalgam filling in such cases, then the causal connection is not at all proven. The post hoc ergo propter hoc is a dangerous line for medicine. Any experienced physician knows that suggestion plays an enormous role in such cases.
Ritter, P. Die Gefahrlichkeit des Quecksilberdampfes, Med. klin. 1926, 1279; Gefahren der
Amalgamfullung, Zahnarztl. Rundshau 1926, 415; Die Gefahrlichkeit der Amalgamplomben
Zahnarztl. Rundshau 1926, 449; Entgegnung auf Stock zur Amalgamfrage, Zahnarztl. Rundshau
1926, 553; Zur Amalgamfrage, Zahnarztl. Rundshau 1929, 1471; Die Giftigkeit des
Kupferamalgams, Med Welt 1930 no.51. writes, that it is known that copper amalgam fillings, when they are lege artis prepared and have sufficient marginal adaption, are completely durable and without any harmful effect for the carrier. It is different when improperly made copper amalgam is used. But after the reports in the literature and practical experience, these side effects, if they appear in rare cases, are without any serious importance. The premise for the durability and harmlessness of any filling is certainly a sufficient mouth care which any dentist must inform his patients about.
Stock's fight has ended and it ended with the amalgam filling again back in its old, good place which it has had for one hundred years. Stock has been defeated but not without a hard fight. He should now have the courage to withdraw his opinion in the newspapers; he should add: errare humanum est.
Maschke, A. Experimentalphysiologische Untersuchungen uber die Beeinflussung geistiger
Leistungen durch Amalgamzahnfullungen Zahnarztl. Rundschau 1930, 990. Maschke systematically observed patients after placing silver amalgam or gold and porcellain as controls. The fillings were placed by skilled dentists who were very good in technical methods. Improper methods were therefore excluded. Nevertheless, within a rather short time the patients had erethismus and tremor mercurialis but no lymphocytosis could be observed. The symptoms appeared especially during stressful situations. "These symptoms clearly show that also the use of noble amalgams as filling material and when the fillings are properly placed, poisonings are not excluded. In the cases studied by me, the removal and exchange of amalgam for gold was therapeutically positive with increase of the psychical functions which were studied. On myself I could also observe that a violent migraine which I had every tenth day was reduced to a few times each year. It should be evident that people harmed by amalgam really need help."
Borgzinner, U. Die Giftigkeit von Amalgamfullungen, Munch. Med. Wochenschr. 1927, 1346. The author points out the importance of a mercurial etiology in unclear cases of ulcerative colitis. He noticed this because of a case of ulceration of the colon, positive for mercury in the urine. The patient had some time earlier got four copper amalgam fillings. No other source of mercury was found, despite careful search. "Should not this case alert us to stop using amalgam. If it apparently can cause ulcerative colitis, it should be able to cause many other lighter diseases.
Muller, O. Vorstellung eines Kranken mit abgelaufener Quecksilberintoxikation durch
Amalgamplomben Munch. Med. Wochenschr. 1929, 651. reports a case with gastrointestinal symptoms, exhaustion, sweating, pronounced loss of weight and increasing paleness. He had also anemia with a pronounced number of punctured red blood cells which indicated a disease similar to lead poisoning. In his mouth were two large and two small copper amalgam fillings. Two of these were in contact with a gold hook. The fillings were 2.5 and one year old. In feces there was large amounts of mercury. Eight weeks after removal of the fillings most of the symptoms had disappeared. There can be no doubt that large amounts of mercury passed into the body in this case.
There was no other contact with mercury. The presence of the copper amalgam and the contact with gold makes it very likely that the source of the mercury was to find in the amalgam fillings.
Wannenmacher, E. (Prof. Zahnarztl. inst. Univ. Tubingen) Die Amalgamfrage, Munch. Med.
Wochenschr. 1927, 1694; Ein Beitrag zur Amalgamfrage Dtsch Zahnarztl. Wochenschr. 1928, 152;
Schadlichkeit der Amalgamzahnfullungen Zahnarztl. Mitteil. 1928, 390. W. arrives, after a 3 years study, at the conclusion: The verdict on copper amalgam, with or without tin, cadmium or similar additions is negative. All experimental studies show that mercury is released from these amalgams in quite remarcable amounts. There is also the well founded danger that copper dissolves. In addition the preparation (heating) is especially dangerous to the dentist.
With the silver-tin-amalgams there is also a possibility for mercury release if not special proportions between alloy and mercury are followed. With carefully chosen proportions it is almost impossible that mercury is released from silver-tin- amalgams after hardening. The dentist should have access to an alloy with constant composition and which binds a constant amount of mercury, otherwise it is not possible to avoid a mercury excess. Any amalgam, copper or so called noble amalgam, which shows free mercury after complete hardening, should be rejected since then it is very likely that mercury can be released and there is a possibility that the patient can come to harm. In addition, one must be careful that no amalgam filings are placed close to gold crowns. Then the gold will be tarnished or even destroyed and also in such cases there is a possibility that considerable amounts of mercury can be absorbed by the patient.
At the meeting of the Society for Natur- und Heilkunde, may 1927, H. Fuhner reported on:
Chronische Quecksilbervergiftung und Amalgamgefahr. He stated that so far no chronic poisoning has been reported with urine mercury of hundredths of milligrams daily but poisonings have been noted with levels of tenths of milligrams. From silver amalgam there are only rarely levels of that magnitude in the urine and this should more originate from dissolved mercury than from evaporated.
It is the task of the dentist to prevent the resorbtion of the amalgam fillings in his patients by persuading them to practice good mouth hygiene and to eat suitable food. Copper amalgam should not be used. Under certain conditions; no contact with gold and other metals and not too large amalgam surfaces, the use of silver amalgam fillings seems to be completely without danger.
Rebel, H. Bericht uber das Amalgamreferat des Zentralvereins deutscher Zahnarzte zu Dusseldorf,
Deutsch Zahnarztl Wochenschr. 1926, 485. Rebel states: According to the reports from dental institutes, inner medicine, pharmacology and chemistry, on the current experience and laboratory experiments, also animal experiments, the objections against amalgam as a dental filling material are without foundation. Only in rare cases of hypersensitivity to mercury, something which also occurs against other medicines and certain foods, copper amalgam fillings might be harmful to the organism.
Kruger, R. Gibt es eine chronische Quecksilbervergiftung durch Amalgamzahnfullungen? Munch.
Med. Wochenschr. 1927, 1346; Eine zweckmessige Amalgamfullung. Dtsch. Monatschr. Zahnheilk.
1927, 266. Kruger considers the copper containing amalgam to be an especially appropriate filling.
He emphasizes the good properties of copper amalgams, mainly the good marginal adaptation. The less good properties: easily abraded, the mercury release and the coloring of the tooth can be prevented by the addition of tin and silver. The final amalgam of choice thus consists of mercury and nearly equal parts silver and tin and more or less copper. The main advantage is that these amalgams have a stability which no other amalgams can reach and it has also a noble composition. Also teeth with such fillings have an extremely small incidence of secondary caries at the margins. Gold, in contrast to other metals in the mouth, is not at all a contraindication for the use of amalgam. Also the placement of new gold fillings close to amalgam is possible and completely harmless. A necessity is that no excess mercury is present in the fillings. There are thus no health objections. The fact that macroscopically, also after several years, not the slightest change, not the slightest loss can be seen, indicates that nothing from the fillings has passed into the body. No mercury could be found in any urine sample.
According to Lewinski, E. Ein Todesurteil uber das Kupferamalgam? Zahnarztl. Rundshau 1926,
517; Die Amalgamfrage Deutsche Monatschr. Zahnh. 1926, 208., copper amalgam has the following advantages: 1. It is more resistant than noble amalgams. 2. It is very slowly abraded when the biting force is strong. 3. It is strongly antiseptic. To prevent dissolution an addition of 2-3 % tin should be used. 4. It is three to four times cheaper. One must, according to Lewinski, try to escape the mercury
psychosis which started after Stock's alarming paper and not let oneself be forced into a corner by more or less amateurish statements.
Finally, jan. 1, 1932, "The Ministry of Health has, in connection with the statements by prof. Stock, taken the inititative for extensive studies on dental fillings. We herewith state: Gold-, silver- and copper-amalgams are completely harmless. The state governements have been informed about these results."
Amalgam Fillings as a Possible Source of Mercurial Poisoning. C.F. Bodecker, D.D.S., F.A.C.D.
Professor of Dental Histology and Embryology, Columbia University Dental School, New York,
N.Y.
Dental Items Interest 48, 1926, 637
The close relationship which the teeth bear to the general health has been proven in numerous cases and, in consequence, the medical profession is liable to blame infected teeth for many ailments.
Some patients have been cured by the removal of offending teeth but doubtless the matter has been carried to the extreme in numerous cases.
And now, news comes from Germany which will send a wave of despair through the dental profession and may also disquiet the public at large.
Professor Alfred Stock Director of the Kaiser Wilhelm Institute of Chemistry in Dahlem, Berlin, believes that amalgam fillings cause a stealthy, chronic form of mercurial poisoning, which manifests itself in ennervation, neurasthenia and a weakening of the memory (Stock, A. Zeitschr. angew. Chemie No.15, 1926).
Before going into the details of Stock's report, I wish to say that we must not be hasty in forming our conclusions.The stakes are too large to be lightly cast aside, nor should we blindly accept the verdict of one man in a matter of such vital importance. If amalgam as a filling material would have to be discarded, we can safely say that the mass of the people would not be able to have any permanent dental work done because gold inlays are still a luxury. On the other hand, if Stock's contention should prove to be true, then amalgam as a filling material must go, or the technique must be so modified as to make it safe.
Prof. Stock's Experiments: Professor Stock, a noted chemist has for many years, in the course of his experiments, been in constant contact with mercury. During this time, he suffered from various symptoms, which increased as time went on, until he despaired of continuing his work. His memory, which was previously excellent, seemed to become weak; lack of energy set in as well as an inability to solve mathematical problems. In 1923, the electrically driven ventilation plant was stopped on account of the expense of running the motor. From this time on, the symptoms appeared in aggravated form and finally mercurial poisoning was diagnosed, not only in Stock but in all who worked in this laboratory.
The air in these rooms was analyzed and found to contain only a thousandth to a hundredth of a milligram of mercury per cubic meter. Air having 12 milligrams of mercury vapor is considered saturated; we therefore see that the quantity found in the analysis of the air in Stock's laboratory was infinitessimal. As man consumes approximately one-half a cubic meter of air per hour, we note that the amount of mercury vapor inhaled by Stock and his assistants was minute. And yet this minute quantity did cause a slow poisoning, even though it was so difficult to diagnose.
And here the possibility appealed to Stock that dental amalgams may likewise be a source of mercurial poisoning. He, therefore, experimented with both copper and silver amalgam fillings and found that, if extracted teeth containing such fillings are heated to about 3O° C. (body temperature is
37° C.) considerable fumes of mercury are given off. It is to be noted that this ensued not only from new and freshly mixed amalgam, but also from old fillings.
These are the experiments which have alarmed the German public, and it is imperative that an able chemist should corroborate these findings.
After the exact amount of mercury vapor, given off at body temperature has been defined for a specified mass of amalgam, a toxocologist must decide whether such a quantity can affect the health of an individual. It is also of vital importance to discover whether the formation of mercury vapor continues for years after the placing of the filling, for if this is the case, we must take all the amalgams in the mouth of the patient into account.
One specific case is cited by Stock: A colleagne, suffering from continued headaches, had a large amalgam filling, around which the gingiva was considerably inflamed. Some time after this filling was removed, the local and general symptoms disappeared.
In answer to this case, I say decidedly and emphatically that we must nut jump to conclusions, particularly not with such scant proof! I will wager that every dental practitioner, who has a pair of eyes and uses them, has noted marked gingivitis around many a large amalgam filling. But the cause of this inflammation of the gingiva is not the amalgam nor the mercury; it is the result of a lump of metal overhanging the margin of the cavity, because when this is carefully trimmed away and smoothed, the irritation subsides.
The dental profession of Germany, headed by Professors Schoenbeck, Schroeder and Ritter do not accept Stock's contention. They have not, in consequence, modified their use of amalgam.
Even though this matter may pass off with a simple scare, it will serve to show the importance of care in the use of mercury by the chemists and physicists.It will also sound a note of warning to dental practitioners to thoroughly condense amalgam fillings, and to remove every trace of excess mercury. This can best be done by the use of annealed gold pellets for they then take up the mercury more readily.
Whatever the future may bring, we must await the results of the above described chemical tests.In the meantime let us keep both feet on the ground and not allow the pendulum of fadism to swing from one extreme to the other.
Pelham, N. Y., July 15, 1926.
THE EFFECTS OF MERCURY VAPOR ON THE UPPER AIRWAYS
(Die Wirkung von Quecksilberdampf auf die oberen Luftwege)
Alfred Stock Chemischen Institut der Technischen Hochschule, Karlsruhe Naturwissenschaften 23,
1935, 453-456
The chronic mercury poisoning which had almost been forgotten, is again considered after I, nearly ten years ago, told about the bad experiences I and my collaborators had and which I emphatically described (Comp. Die Gefahrlichkeit des Quecksilbers und der Amalgam-Zahnfullungen, Z. angew.
Chem. 41, 1928, 633; Med. Klin. no. 29/30, 1928; Zahnarztl. Mitt. 19, 1928, 370, 377, 390). In many places the hazards of the devious, volatile, metallic poison are still underestimated. The poison does not only threaten all persons who occupationally come into contact with it (physicists, chemists, physicians, dentists, workers in mercury-using factories, in hat factories etc), but also many other persons (amalgam dental fillings, broken thermometers, old mirrors etc). Because of my publications, hundreds of cases of chronic mercury poisoning have become known to me, most of them because of occupation; a considerable number, however, also because of amalgam dental fillings.
Together with a number of collaborators (F. Cucuel, F. Gerstner, R. Heller, H. Kohle, A. Kreyer, H.
Lux, E. Pohland, W. Zimmermann), I have tried to clarify a number of questions connected with mercury poisoning: improvement of the analytical determination of very small amounts of mercury, analysis of mercury in organic material, the distribution of traces of mercury in nature, the oxidation of mercury by air, mercury levels in human excretions normally and during poisoning, the distribution of absorbed mercury in the body etc.
Mercury which enters the body through the respiratory tract is extremely more unpleasant than a several times larger amount swallowed into the gastrointestinal tract. Primarily this is because mercury more easily and rapidly enters the blood and lymph circulation; to a large extent, however, because of the circumstances which will be described in this communication. In real life, chronic mercury poisonings are nearly always caused by inhaled mercury vapor.
As is generally known (comp. E.W. Baader & E. Holstein, Das Quecksilber usw. Berlin: R. Schoetz
1933) the symptoms of chronic mercury poisoning, apart from the nervous-psychic disturbances, appear at the places of excretion of the metal; in the gastrointestinal tract (necrosis of mucosa, diarrhea, bleedings) and in the kidneys (inflammations up to deadly damage). The central nervous system will also be more or less involved. An accumulation of mercury occurs mainly in the kidneys. Apparently, small, continous doses of mercury (The presence in the body of mercury in milligram amounts, absorbed as vapor for a long time, disturbs already noticably the human organism. Mercury in this form belongs to the most potent of poisons.) act in similar ways as today is known about the actions of lead (According to F. Blumenthal & K. Jaffe': Eczema and Idiosyncrasy, Berlin: S. Karger 1933): "The action oflead is a continous migration of lead through the body and the total amount excreted is equal to that taken in. The organism itself remains almost free of lead. The chronic lead poisoning is thus not the result of a chemical accumulation, but a dynamic accumulation. Continously repeated insults finally, after a symptom-free period, produce the picture of a chronic poisoning: stomach pains, arthralgia, paralysis and encephalopathies. These symptoms follow an irregular, remitting course, appearing also during long periods without contact with lead."
The effects of mercury on the sites of entrance into the body, the nose and related areas, have been too little discussed. Already Fleischmann (Dtsch. Med. Wschr. 1928, no 5) emphasized in his report from the "mercury study" of the Berlin Charite', started by Kraus, that the patients almost always complained about symptoms from the upper airways, about catarrhs of the olfactory mucosa etc. and
I have described this effect of mercury in my first publication of 1926. However, the work by Baader
& Holstein reports only little on this subject (p 122): "In addition to a tendency for bleeding noses
(enlargement of the nasal veins), wet or dry chronic catarrhs of the nose (Bruggemann), which exposed persons often complain about, no specific nasal disease has been noticed." The mentioned work by Bruggemann (Z. Laryngol. 15, 1926, 107) has the title: " A rare cause of chronic nasal irritation (insidious mercury poisoning)." She describes a case of occupational mercury poisoning and arrives at the conclusion: "for us rhinologists, it is especially important that, during an insidious mercury poisoning, besides general nervous symptoms, the nose and the upper airways will be affected by catarrhs and chronic irritation, long before the typical mouth affections appear... In all cases where there is a possibility for inhalation of mercury vapor, one should think of an insidious mercury poisoning when one finds nasal irritation with an unclear etiology."
This is quite correct. However, such cases are not at all rare. It is the intention with this short report to notify the readers of Naturwissenschaften, including many persons who come into contact with mercury and also many physicians, about this affection. A more extensive report will later be published elsewhere.
An effect on the nasal mucosa can be expected. It is certainly the first place the inhaled metal has opportunity to be oxidized and transformed into soluble form under the influence of water vapor, air and heat. This primarily happens where the inhaled air stream contacts the mucosa; the ethmoid cells and the nasopharynx. In these places bacterial infections often start and dust and smoke deposits form, very likely enhanced by the vortex formation. The mercury which is not trapped here, will then be almost completely absorbed in the lungs with their enormous surface area, something we have previously determined.
The binding of relatively large amounts of mercury in the upper airways could be demonstrated in animal experiments (we acknowledge the generous help from prof. E.v.Gierke. The analyses were made by A. Kreyer). Two rabbits were placed in weakly mercury-containing air (vessel with mercury in the cage). In the nose and upper nasal mucosa we found 6.5 ug and 6.1 ug mercury in the two rabbits, whereas the mercury levels in the mercury- accumulating kidneys were not more than 19.3 and 32.6 ug, a proof that the total amount of absorbed mercury was rather small.
That mercury affects the mucosa of the nose seems also quite understandable considering the sensitivity of other mucosal tissues (e.g. the mouth and the intestines) towards the metal.
In the first report on my own poisoning (Z. angew. Chem. 39, 1926, 461) I wrote: "Soon also the upper airways were affected; in the beginning light and occasional nasal catarrh, then permanently tight nose, later almost continous catarrhs of the olfactory mucosa with often bloody mucus production and crust formation, violent throat inflammations and pains in my ears connected with impaired hearing and smell." These observations have then been confirmed by many other cases of poisoning. In addition, not rareley chronic problems appeared in connection with the immediate mercury effects, especially sinusitis (and in the mouth the teeth and jaw bones were affected). These problems remain after the poisoning has disappeared and require special treatments.
The nasal problems are nearly always accompanied by "nervous- psychic" disturbances: Pressure and headache between the eyes, tiredness, depression, lack of interest in intellectual work, impaired memory etc. Connections between affections of the nose and such impairments of general well-being are generally known from e.g. when one has a stuffed nose. That the characteristic "nervouspsychic" disturbances which are called erethismus mercurialis, at least during the first stages of mercury vapor poisoning, are connected with this and not with a more general disturbance of the nervous system (which undoubtedly appear later during the poisoning), is demonstrated by several different observations. If the irritated nasal mucosa is anaesthesized with cocain, rinsed with physiological saline or even exposed to fresh, cool air, then the symptoms diminish or disappear.
The effect of cocain is not a general cocain effect since improvements only result if certain places in the upper nose are treated. Most clearly the role of the nose is shown by the facts described below.
The chronic mercury vapor poisoning leads often to an allergic hypersensitivity towards traces of mercury vapor. Baader and Holstein state correctly: "The hypersensitivity is often the only consequence of a mercury poisoning." Concerning myself, this is exactly what happened, which several years of observations have shown. Numerous reports, obtained from collegues, physicians, dentists etc, show that this also applies to many others. I will describe my own case more in detail since I know that best and since it apparently is typical of many other cases.
I presume that I was not especially mercury sensitive by Nature. First after a long -and I must today say - very thoughtless contact with mercury, the chronic poisoning developed. In the ten years which have elapsed since the poisoning was recognized and after which I have been very careful with the poisonous metal, all of it must have disappeared from the body. The excretions contain since several years not more mercury than normal levels (comp. A. Stock & F. Cucuel, Z. angew. Chem. 47,
1934, 641). The allergic mercury sensitivity has, however, remained to such a high degree that the staying in laboratories in which the air contains just a few micrograms per cubic meter (as unfortunately is the case with many laboratories at the Karlsruhe Chemische Inst.), already after half an hour causes symptoms which increase with prolonged exposure. The levels will not affect other persons in such short times. The symptoms will follow the course described here: light dizziness,
"irritation", impaired thinking, light pressure between my eyes, tiredness, headache in the forehead, a feeling of tight nose (mucosal swelling without mucus production), impaired hearing and light singing in my ears because of blocked eustachian tubes, a "furry" feeling of dryness in the upper nose and throat, the formation of thick, white secretion. With longer or repeated staying in such rooms there will be slightly bloody secretions, some blood clots and crusts (In the area of the ethmoid cells, not the nasal septum. Very chracteristic for mercury effects! Also when I have severe, ordinary catarrhs, these manifestations do not appear.), intense headache with vertigo, finally intense catarrhs which might give opportunity for subsequent infections which also will affect the throat. In the first stages, the symptoms disappear quickly when mercury exposure ceases, especially if I stay in fresh air. At later stages the complete disappearance will take several days up to a few weeks.
That the symptoms really are caused by mercury follows from the experiment with sublimate solution which will be described below. Other irritating vapors have not been present in the rooms at all. No words of explanation are needed to understand how disturbing such an idiosyncrasy is for anyone who can not avoid visiting such mercury-containing rooms. One can not enough call upon care in the handling of mercury. The danger of acquiring a lasting idiosyncrasy is a new reason for a warning. Once acquired it will not go away again. Also after a long holiday it remains unchanged.
In addition, in my case the sensibilisation of the nasal mucosa because of mercury is not restricted to only mercury but also extends to other chemicals (e.g. sulfur dioxide and chlorine) and tobacco smoke (Such extensions of allergic manifestations are not unusual. Comp. the mentioned work by
Blumenthal & Jaffe'.). In the latter mercury might also have a role. Cigarettes and cigars contain various amounts of mercury (A. Kreyer found up to 0.4 ug mercury in each cigarette), which during smoking is transferred to the air (not to the smokers mouth as we determined in special experiments).
It seems evident that this can not be a general poisoning and a profound disturbance of the nervous system when we have such rapid effects but must be a local reaction of the metal at the site of absorbtion. Then the previous conclusion is further supported: that the first "nervous-psychic" symptoms which accompany chronic mercury poisoning have their origin in the upper airways. The following "experimentum crucis" appears to give a definite proof: I tested the effects of an extremely dilute mercury II-chloride solution on my nasal mucosa (Also the normal nose is generally sensitive to sublimate. A.J Kunkel, Handbuch der Toxikologie (Jena 1901), p. 145: "The mucosa is extremely sensitive towards mercury solutions: still 1:50 000 is corrosive when the nasal mucosa is rinsed with it and 1:100 000 (i.e. 10 ug/ml) will still be unpleasant.")
One day, when I felt healthy, both objectively and subjectively and when I was in no other way in contact with mercury, I sprayed, with a fine vaporizer, 3 ml of a 0.6% saline solution containing
0.05 ug mercury as sublimate, into the upper nose. Most of this solution certainly again came out.
The amount of mercury which the mucosa really absorbed might be estimated to 1/100 ug (1/100
000 000 g). However, the effect was not to be mistaken about. After about two hours I had weak pressure between my eyes, after another two hours the tight, furry-dry nose and after another few hours light headache. Blowing the nose demonstrated a thick, opaque-white slime which apparently caused the furry feeling. The white, thick secretion lasted, accompanied by an uncomfortable nasopharyngeal catarrh and dizziness, about 24 hours and then disappeared rather quickly and completely with all other symptoms. The whole series of events was in all details similar to the symptoms which a short stay in weakly mercury- containing air precipitated.
Then there should be no doubts about the connections between the irritation of the nasal mucosa and the first "nervous-psychic" symptoms which mercury causes. The extent of such manifestations should, in the individual case, be determined by the anatomy of the nose and the properties of the nasal mucosa. In addition, the nasal affections are similar when the mercury poisoning is caused by amalgam dental fillings. This supports my previously stated presumption that, when amalgam fillings cause health disturbances, it is the mercury vapor which enters the airways which has a major role, apparently a more important one than the much larger amounts of mercury which passes from the amalgam into the gastrointestinal tract.
Various observations indicate that the primary nervous-psychic symptoms of a chronic mercury poisoning is caused by traces of mercury which passes from the nose into nearby parts of the brain.
We will report elsewhere on such studies.
THEMERCURYCONTENTOF HUMAN EXCRETIONSANDHUMANBLOOD
(Der Quecksilbergehalt der menschlichen Ausscheidungen und des menschlichen Blutes) A.Stock &
F.Cucuel Zeitschr. angew. Chem. 47, 1934, 641-647
Mercury levels of human excretions, in feces and urine, are of importance for the diagnosis of chronic mercury poisonings (In exhaled air there is hardly any mercury even after considerable exposure; whether mercury evaporates through the skin has not yet been studied; it is not likely).
Today we know that chronic mercury poisoning is more common than was presumed ten years ago
(A.Stock, this Journal 41, 1928, 633; Med Klin no 29/30 1928; Compare also A. Zangger: Arch
Gewerbepathol. Gewerbehyg 1, 1930 539)
Its first symptoms, almost only nervous-psychic, e.g. transient depressions, headaches, impaired memory, are so little specific that the clinical diagnosis often is difficult. It will be more clear when certain later symptoms appear: easily bleeding gingiva, oral inflammations, chronic catarrhs, sometimes diarrhea, kidney inflammation etc. The patients will often be treated by neurologists, laryngologists, internists etc, and mercury will not be considered the cause.
Opportunity to absorb mercury and for chronic mercury poisonings are frequent. Because of its specific properties (permanence, liquid form, high density, electrical conductivity, formation of plastic amalgams) the toxic metal finds increasing applications in industry, science and also as a
dental filling material (Compare E.W. Baader & E. Holstein: Mercury, its production, technical use and toxic properties with extensive documentation of occupational mercury poisoning, including therapy and prophylaxis. Berlin. R. Schoetz Publ 1933. This excellent work deals with several of the questions which are discussed here. Unfortunately it was not possible to include the new research which improved methods of mercury determination have made possible).
The liquid properties and most importantly the considerable volatility already at ordinary temperatures, enhances its dissipation and its unnoticed entry into the human body. Mercury uptake and thus the possibility for chronic mercury poisonings is present e.g. for all persons who work in mercury-using industries; thermometer-, mercury rectifier-, mercury lamp-, amalgam-, felt hatmanufacture etc. and in several other occupations: physicists, chemists, medical doctors (blood pressure measurement) etc, but also many persons who occupationally have nothing to do with mercury (for instance because of amalgam fillings, treatments with mercury-drugs, broken thermometers and similar causes). As not previously recognized sources of mercury, felt hats must be noted. During manufacture, a tanning solution of mercury and nitric acid is used. We could measure that felt hats, also after long-term use, released noticable amounts of mercury to the air. A hat which had been in use for a year was placed in a glass jar of 15 l for two hours at room temperature. In 20 l of air which was led through the jar (10 l/h) 0.5 ug was found. With four new hats from various manufacturers: 0.5 ug, 0.6 ug, 1.3 ug and 2.3 ug mercury. The latter hat delivered at 35 oC not less than 60 ug mercury when we repeated the experiment. Since the hats will reach similar and even higher temperatures in summer and since it is known that our body also absorbs mercury through the skin (mercury ointments!), many persons must absorb mercury in this way. It can not be excluded that also the mercury which is absorbed through the skin can have harmful effects. If this is correct, it should be a positive change, not only for the workers in the felt hat industry (information about the chronic mercury poisonings in this industry can be found in the book by Baader & Holstein) but also for the carriers of the hats if the mercury- tanning disappeared from the manufacture.
If mercury poisoning is suspected, the doctor will often ask: is there mercury in the excretions and do the levels suggest a mercury poisoning? Unfortunately it is not that simple that mercury poisoned persons excrete mercury whereas urine and feces of healthy persons are free of mercury. All humans take up some mercury with food and excrete it regularly again. As we have reported earlier
(Naturw.sch. 22, 1934, 390), there are traces of mercury at an average level of 10-8, i.e. 1/100 mg per kilogram, in every inorganic and organic natural substance, also in the ground, in water and in all food. According to our measurements, a human with ordinary eating habits will on the average ingest - with large variations - 5 ug mercury with food daily (thus the observations by P. Borinski a few years ago have been experimentally verified; Klin. Wochenschr. 10, 1931, 149; comments on this A. Stock Ibid 10, 1931, 454).
Reliable studies on such questions, which require the analytical measurements of very small amounts of mercury down to 1 ug and less, have only been possible after the development of new analytical methods (Determination of these small amounts of mercury in organic material: A. Stock,
F. Cucuel & H. Kohle, this journal 46, 1933, 187. All analyses in the present study have been performed according to the methods described there). The older analyses can only be considered reliable to a limited extent (this is the case for our own measurements as well as those of other researchers, e.g. Borinski's, who often found no mercury in the excretions although we now know it is always present).
The anlyses can frequently have contained too much mercury because of the previously overlooked mercury content of most reagents; more often the mercury levels must have been far too low since the treatments of organic material is more difficult than presumed.
We have therefore used the new analytical methods to examine the often disputed question of the mercury content of the human excretions again. Three groups of persons have therefore been examined:
A. "Mercury-free" no exposure to mercury except with food is apparent. Especially they have no amalgam fillings.
B. "Amalgam carriers" with amalgam dental fillings but without other apparent contact with mercury
C. "Mercury workers" who also come into contact with mercury in other ways.
Since mercury excretion often varies from day to day, we have analysed feces (F) and urine (U) from the test persons for several consecutive days if possible. The recorded amounts of mercury refer to the amount of daily excretion and the weight or volume is recorded. Within brackets we have also noted the amounts of mercury for 100 g feces or 1000 ml urine to obtain an evaluation of the concentrations.
A. MERCURY-FREE
It is difficult to find such persons. One can hardly believe how seldom the absence of amalgam fillings (also persons who previously have had amalgam fillings and who might retain mercury in the body are not suitable) coincides with an occupation which completely excludes any contact with mercury. For instance, most students at our university (Techn. Hochschule, Karlsruhe) were not suitable because of the mercury levels in the air of the laboratories and the workshops; especially the urine from amalgam-free students contained clearly a little (a few micrograms/1000 ml) more mercury than from really mercury-free persons. It is actually only possible to talk about really
"mercury-free" with reservations. It is e.g. always possible that the persons live or work in rooms where once a mercury thermometer has been broken. This can have the consequence that the air in the room contains mercury for years which can elevate the mercury levels of the excretions.
We report of three cases which, according to information we could obtain, could be considered really mercury-free.
I. D. Six year old boy.
Day Feces g ug Hg (ug Hg/100g) Urine ml ug Hg (ug Hg/l)
1 85 0.45 (0.5) 1000 0.3 (0.3)
2 133 0.4 (0.3) 500 0.6 (1.2)
3 115 1.75 (1.5) 1000 1.7 (1.7)
4 80 8 (10 ) 1000 0.7 (0.7)
II. O. 55 year old worker in a soap factory
1 245 2.3 (0.9) 1000 0.3 (0.3)
2 80 0.4 (0.3) 765 0.2 (0.3)
3 183 3.5 (1.9) 1050 1.1 (1.0)
4 260 6.5 (2.5) 1060 0.4 (0.4)
III. S. 22 year old woman, no occupation
1 300 4 (1.3) 860 0.6 (0.7)
2 102 1.4 (1.4) 700 0.7 (1 )
3 180 1 (0.6) 680 0.5 (0.7)
4 195 12.5 (6.4) 830 0.7 (0.8)
5 102 1.4 (1.4) 945 0.7 (0.8)
6 200 6 (3 ) 850 0.4 (0.5)
To obtain more material we collected urine from several persons at various places and measured the average mercury level. The donors had no amalgam fillings and, according to what we could find out by asking, not anything else to do with mercury. The urine mercury level from 19 patients, collected at a doctor's office was 1.1 ug/1000 ml, a little more than the mean of the measurements above. Also here there is a possibility that one or more of these patients had absorbed mercury from other sources and that the mean thereby was elevated. The drawbacks of these average measurements, lacking a careful evaluation of each case, we learned from the following experience.
A collection of 40, not amalgam, urine samples from a hospital yielded 390 ug/1000 ml!
Investigations showed that the collection vessels had been desinfected with sublimate solution and that 1/3 mg of mercury had come into the sample.
Since we, in this study, will examine lowest levels of mercury present in human excretions, the carefully controlled single cases are the most valuable.
The three analyses above are in many ways informative: The mercury content of the feces varies from day to day within a rather wide range, related to food. Our analyses of seven dinners at the
Karlsruhe student resturant showed mercury levels between 0.25 and 3.3 ug, mean 1.6 ug
(Naturw.sch. 22, 1934, 392). Especially some food, primarily fish, was quite mercury rich. Also the method of food preparation will affect the amount of mercury which will be in the final meal.
According to experiments described in section D, most of the mercury which has been introduced into the gastrointestinal tract leaves the body through the intestines without being absorbed into the blood circulation. The mean of 14 measurements of feces contained each day 3.5 ug (2.3 ug/100g).
The mercury content of the urine is on the average considerably smaller and less variable than that of the feces. The mean of 14 analyses was 0.65 ug/day or 0.7 ug/1000 ml. Also many other single measurements yielded values between 0.5 and 1 ug in the daily volume of urine from amalgam-free persons.
The mean daily excretion of mercury in mercury-free persons is thus 4 to 5 ug, i.e. the same amount as that taken in with food. An accumulation of mercury in the body does not take place; this is also apparent from the fact that there is no noteworthy difference between younger (I) and older (II) persons and is also shown by analyses of autopsy material. This will be reported elsewhere.
A direct relationship between mercury levels in feces and in urine was not demonstrated.
B. AMALGAM CARRIERS
In this group the amount of mercury which will be released in a single case will be closely dependent on the number , surface area, condition and age of the amalgam fillings. Perhaps also individual variation in the properties of the saliva will have influence. Average values have therefore little value in this context. We report here three characteristic cases:
IV. V. 22 year old student of construction technology, no occupational exposure to mercury. Several carefully prepared silver amalgam fillings of faultless, polished and silver-white appearance placed by his first dentist (the most recent filling one year earlier. No signs of mercury poisoning.
Day Feces g ug Hg (ug Hg/100g) Urine ml ug Hg (ug Hg/1000 ml)
1 162 8 (5 ) 750 1.8 (2.4)
2 190 35 (18) 835 0.5 (0.6)
3 82 8.2 (10) 825 2.7 (3.3)
4 165 16 (10) 550 2.4 (4.4)
5 177 25 (14) 700 4.2 (6 )
V. H. 33 year old upholsterer. Not exposed to mercury. Several older amalgam fillings. No symptoms.
1 229 21 (9 ) 720 2.8 (3.9)
2 160 9.5 (6 ) 940 0.4 (0.5)
3 115 14 (12) 1050 0.5 (0.5)
4 150 10 (7 ) 950 1.0 (1.1)
VI. S. 22 year old student of chemistry. Many amalgam fillings, several of less good appearance.
According to clinical examination a chronic mercury poisoning was likely. No normal kidney function; notably small amounts of urine.
1 205 29 (14) 410 1 (2.4)
2 52 16.5 (32) 260 1.5 (5.8)
3 105 36.5 (35) 450 2.5 (5.6)
4 115 50 (43) 250 1.5 (6 )
If this group is compared to the mercury-free group the following differences appear: The mercury levels in the feces are much higher, here on the average 21 ug daily or 17 ug/100g compared to 3.5 ug or 2.3 ug/100g. Also in urine some more mercury was excreted with large variations. In extreme cases also the mercury levels of the urine will be much higher:
VII. Older man who, in addition to many amalgam fillings, had a gold crown in his mouth
(something dentistry considers not allowed because of the possible galvanic processes but which the dentists often ignore in practice).
11.2 ug Hg in 780 ml urine (14.4 ug/1000ml). He had suffered from stomatitis for years and had also other symptoms which indicated a mercury poisoning.
VIII. Sm. Chemistry student. 42(!) carefully placed, mostly small amalgam fillings. We will describe this case more in detail since it was investigated carefully, both analytically by us and clinically - the father of the student is himself an MD. The student had for several years suffered from troubles which were, lacking a better explanation, explained by a latent tuberculosis and which finally increased so much that he had to abandon his studies. We found in his urine 1/ in 500 ml 19.5 ug
Hg; 2/ in 400 ml 13 ug Hg (mean 30 ug/1000ml). This finding suggested a chronic mercury poisoning. The symptoms were actually nearly all present. The student had all the amalgam fillings exchanged for gold fillings. Also a granuloma at the root of a filled tooth was treated. After a few weeks he had completely recovered, was full of energy and eager to go back to work. Three months after amalgam removal the mercury level in urine was still 20 ug/1000 ml. 1.5 months later we analyzed the urine on five consecutive days.
Day 1. urine 490 ml: 5 ug Hg (10.2 ug/l)
2. 895 10.8 (11.1 )
3. 690 9 (13 )
4. 615 6 (9.8 )
5. 785 8.7 (11.2 )
The mercury level had thus further diminished. We took the opportunity to study if the mercury excretion could be enhanced by diuretics (three times daily 1.5 g Diuretin). Such an effect could not be demonstrated.
Day 1. 610 ml: 7.9 ug Hg (13 ug/l)
2. 640 7.6 (11.9 )
3. 560 6.8 (12.2 )
4. 1005 5 (5 )
5. 715 5.7 (8 )
It is remarcable that the mercury level of his blood hardly changed (comp. sect E no XX). It was before removal of the fillings 5.4 ug/1000g and 3 months after removal 4.2 ug/1000g, corresponding to about the normal level. The sustained, only slowly reduced mercury excretion in urine, can apparently be explained by the release of mercury which has accumulated in the kidneys.
There is no doubt that the excess of mercury excreted, by the amalgam carriers, originated from the fillings. In some places it is still disputed that amalgam releases mercury (Here we primarily consider silver (noble) amalgam. Copper amalgam has hardly any defendant. In aged copper amalgam fillings one can often see mercury drops with the naked eye). Therefore no special proof is really needed. It is generally known that also the best fillings in time are abraded, i.e. that material is lost, also mercury (which constitutes 50 % or more of their contents). The corrosion of the silver-tinmercury alloys to which the so called noble-amalgams for dental fillings belong, have recently been the subject of a careful scientific study by N. Brecht-Bergen under conditions similar to those in the mouth (Z. Elektrochem. angew. physik. Chemie 39, 1933, 927. Dissertation Techn. Hochschule,
Karlsruhe 1933).
During this study it was found that first tin dissolves, with the result that the surface will be coroded.
Further it was shown that the mercury in these amalgams have a certain vapor pressure which is 10-
15 % of that over pure mercury.
Our above results are a new clear proof that also the best amalgam fillings release mercury.
According to our results, the main part of the mercury released from amalgam will be excreted through the intestines, certainly partly in the form of finely divided, unchanged amalgam fragments.
It is possible, that when amalgam fillings cause a poisoning, it is the mercury which is released as vapor and which enters the lungs, which causes the damage. That the mercury which enters the body through the respiratory organs is much more poisonous than that which comes into the stomach, is proved by animal experiments on which we will report later. When these presumed conditions are present, it could explain why amalgam fillings in some cases cause damage and in others not. The amount of mercury which comes into the lungs must be quite dependent on conditions in the specific case, above all the position of the fillings in relation to the flow of inhaled air. The differences can hardly be explained by different sensitivity to mercury since it is not mercury sensitivity but mercury insensitivity which is the exception, something many publications report and which is also shown by the observations one of us made on himself and his collaborators (comp. e.g. the work by Baader &
Holstein or the studies by the Badener prof. of occupational medicine E. Holzmann, this journal 42,
1929, 999 (transl. note: abstract of a paper by Holtzmann, Zentralbl. Gewerbehyg. Unfallverhut 16,
1929, heft 1))
OCCUPATIONALLY EXPOSED
In the excretions of persons who are exposed to mercury in an occupational setting, the mercury levels are often much higher than in the groups we have described so far. There are many studies in the literature and we again refer to the book by Baader & Holstein and to the analyses which S.D.
Rieselman made on workers at the mercury extraction plant at Nikitowka in the Donez area (Arch.
Gewerbepath. Gewerbehyg. 1, 1930, 508). He found between 60 and 2900 ug Hg/1000 ml in 22 urine measurements, an average of 786 ug/1000 ml and in 14 measurements of feces 30 to 4800 ug in each portion. Also he concluded: "Only some individuals show a biological resistance to mercury poisoning."
We have studied two glass blowers who often make mercury manometers. The air in the workshops contained mercury.
IX. L. 27 years old. Glass blower for 6 years. An analysis of the air in the room gave 37 ug/m3
Day Feces g ug Hg (ug Hg/100g) Urine ml ug Hg (ug Hg/1000 ml)
1 126 43 (34) 1350 21.5 (16)
2 185 18.5 (10) 1155 28 (24)
3 287 35 (12) 1100 27.5 (25)
4 120 34 (28) 1020 76 (75)
5 228 2.5 (1.1) 1120 25 (22)
6 70 9 (13) 910 28 (30)
X. J. 48 years old. Glass blower for 34 years. Several symptoms indicating mercury poisoning: headaches, restlesness, insomnia. In the workshop there was 50-120 ug Hg/m3. Not even these relatively high levels are even a hundredth of what mercury- saturated air can contain.
Day Feces g ug Hg (ug Hg/100g) Urine ml ug Hg (ug Hg/1000 ml)
1 163 154 (94) 645 34 (52)
2 23 13 (57) 850 42 (49)
3 115 118 (103) 1245 50 (40)
4 76 235 (310) 1085 50 (46)
5 81 44 (54) 465 40 (86)
We also measured the mercury level of his blood and found 65 ug/1000g, a level far above normal
(comp. sect E). Because of the continous exposure to the mercury containing air, his whole body was impregnated with mercury. Even so, the absolute amount of mercury in the body is even in this case extremely small: only about 6*10-8 of the body weight, i.e. about 5 mg in the whole body.
Then we have assumed that the mercury concentration in the whole body was the same as that of blood (which is hardly correct; e.g. in the kidneys it should be far higher.)
Mercury affected this manual worker less in his work than much smaller amounts of mercury affect people who have intellectual work. Maybe also Bacchus protects the glassblowers, with their understandable thirst, against the insidious Mercurius.
After the workshop was cleaned from mercury and rebuilt for mercury work (floor without joints, strong ventilation) the mercury level only reached a few ug/m3 (which could originate from the gas heating), the man's problems slowly diminished. After a few weeks we, however, still found 200 ug/1000 ml in urine but only 6.3 ug/1000 g in blood, about the normal level and a new proof that the kidneys accumulate mercury.
As we have described above, the intellectual performance is affected at far lower levels of mercury.
The first symptoms: pressure around the head, lack of interest in work, difficulties to think, impaired memory, will naturally affect the intellectual worker more than the manual one. We could study two new cases where chemists, because of work in mercury-contaminated rooms, had acquired light but evident mercury poisonings.
XI. Dr.B. In the laboratory air 40 ug/m3. In urine 13 ug/1000 ml.
XII. Dr.Br. In the laboratory air 35 ug/m3. In urine 11 ug/1000 ml.
An additional similar case:
XIII. Mrs P. slept in a room in which some years earlier mercury had been spilled. Clear signs of chronic mercury poisoning. In urine 17 ug/1000 ml.
Such mercury levels thus indicate poisonings.
D. Experiments with excretion of orally administered small amounts of mercury.
The observation that mercury excretion often occurs irregularly and intermittently led to these experiments. We gave each one of the mercury-free persons we used in section A 200 ug Hg in the form of a HgCl2 solution and measured how the excretion took place. The results of the single experiments differed somewhat; the human body is certainly no chemical retort. a/ XIV. S. (comp. III)
Day Feces g ug Hg (ug Hg/100g) Urine ml ug Hg (ug Hg/1000 ml)
1 244 4.6 (1.9) 1150 1.3 (1.1)
This value corresponded to what we found in III. In the morning of day 2 we gave 200 ug Hg as
HgCl2 solution (1 ml).
2 34 4.2 (12) 730 21 (28)
3 204 45 (22) 915 0.8 (0.9)
4 45 33 (73) 880 53 (60)
5 134 32 (24) 1440 2.2 (1.5)
6 no feces 820 4.6 (5.6)
7 56 9 (16) 1000 18 (18)
8 78 5 (6.4) 880 2 (2.2)
9 200 2.5 (1.2) 835 1.5 (1.8)
The mercury level in urine and feces had again reduced to normal levels. The 200 ug of mercury, administered as sublimate, had been excreted from the body almost completely. We recovered, after subtraction of the normal amount of mercury (5 ug daily), 190 to 195 ug. Of this a little more that half, 105-110 ug, was excreted with the feces in a steadily diminishing amount. The rest was excreted in urine in a remarcably irregular fashion: On the first day a rather large portion, on the second the level reduced to the normal level, on the third almost a quarter of the total amount of administered mercury appeared, on the fourth again almost normal, on the following days again increasing and then finally back to the original level.
Two other experiments followed a similar course only the mercury levels in urine were smaller.
They varied, however, again considerably from day to day, even fell below the original value which for unknown reasons were somewhat higher than in the experiments III and IV one year earlier. This variation can only be explained by an inhibition of kidney function which affected the mercury excretion. We describe the values from a fourth experiment where we, instead of measuring 24 h urine, collected 12 h samples: a/
Day Feces g ug Hg (ug Hg/100g) Urine ml ug Hg (ug Hg/1000 ml)
1 145 2.3 (1.6) 920 3.7 (4.0)
On the morning of day 2 we gave 200 ug Hg
2 197 5.9 (3 ) 185 0.6 (3.2)
330 0.52 (1.6)
3 25 16.5 (66) 470 1.55 (3.3)
350 1.35 (3.9)
4 160 90 (56) 700 1.25 (1.8)
415 1.35 (3.3)
5 73 14 (19) 315 2.05 (6.5)
515 1.45 (2.8)
6 no feces 440 1 (2.3)
275 1 (3.6)
7 228 15 (6.6) 395 0.4 (1 )
105 0.5 (0.5)
8 198 7.5 (3.8) 470 1.2 (2.6)
260 0.6 (2.3)
9 97 3.5 (3.6) 470 1 (2.1)
475 1.2 (2.5)
Also this time the excretion of mercury in the feces was regular (about 130 ug). However, in urine we could not, with one exception, find more than normal values. It is notable that the mercury levels of "morning" and "evening" urine were similar.
A corresponding test with another person (IV) gave the same result. More than half of the added mercury was excreted via the intestines; in urine the mercury level was nearly normal. Why transiently higher levels were also found in urine in experiment XIVa can not yet be answered and must await further experiments which also might give clues to the mechanisms of the reduced mercury excretion in the kidneys. Perhaps variations in the intake of food has a role.
E. MERCURY LEVELS IN BLOOD.
In connection with the described tests, we also determined in a number of cases, the mercury levels of human blood, to see if blood tests could be used for diagnosis of mercury poisoning. Mercury analysis of blood corresponds to that of other biological material, however, the following should be noted: Since blood during treatment with potassium chlorate and hydrochloric acid foams very much, the oxidation must take place in a large (at least 1.5 l) vessel and the hydrochloric acid must be added in small portions. Aggregations which are difficult to divide and which readily form, are broken up with a glass rod. After filtering off undissolved material, a solution is obtained, which after copper sulfate addition and hydrogen sulfide treatment, is viscid, slimy, organic-containing, partly charred and hard to filter. Before precipitating, it is useful to add filter mass (Schleicher &
Schull Co) and to heat the precipitate for lengthy time. Because of the presence of organic substances in the solution, often the CuS-HgS precipitation is not complete (with some experience one can recognize the light blue solution which is suitable for the electrolysis). The precipitate, after the sulfide treatment, must therefore be solubilized and once again treated with copper sulfate, hydrogen sulfide etc. For the less experienced in the analytical method this is always to recommend.
The blood, mostly 100 to 200 g, was obtained from the venous vessel of the arm. Our studies are so far rather limited but allow, however, already certain consistent conclusions.
XV. Middle aged woman without amalgam fillings or other apparent contact with mercury.
140 g blood: 0.87 ug Hg (6 ug/1000 g)
XVI. 86 year old woman, also without apparent exposure to mercury and dead because of atheriosclerosis.
94 g blood: 0.6 ug Hg (6 ug/1000 g)
In another mercury-free case where also the urine was measured and found to be relatively low in mercury, 100 g blood contained only 0.1 ug Hg (1 ug/1000 g), a value which was so low that it fell outside the range of the other ones.
XVII. Assessor. Some older amalgam fillings
210 g blood: 0.7 ug Hg (3 ug/1000 g)
XVIII. Man with seven amalgam fillings placed within the last year.
122 g blood: 0.5 ug Hg (4 ug/1000 g)
XIX. Chemist, several amalgam fillings
142 g blood: 0.5 ug Hg (4 ug/1000 g)
XX. Chemistry student (see no VII). 42 amalgam fillings; clear chronic mercury poisoning.
115 g blood: 0.62 ug Hg (5.5 ug/1000 g)
In urine: 36 ug Hg/1000 ml (!). A few months after removal of the fillings: In 90 g blood: 0.38 ug
Hg (4 ug/1000 g), in urine 20 ug/1000 ml.
XXI. Tailor (see no VII). Many amalgam fillings and a gold crown. Clinical results suggested mercury poisoning.
57 g blood: 1.55 ug Hg (27 ug/1000 g). In urine 14.5 ug/1000ml.
In this case substantial amounts of mercury appeared to have reached the blood from the amalgam fillings. However, also in this case an unknown source of mercury might have been present (broken thermometer etc.). Since the man lived outside the city we could not determine this.
The following cases are persons who presently or previously had been exposed to mercury in their occupation.
XXII. Man who suffered from mercury poisoning two years ago. Since then not more in contact with mercury.
148 g blood: 0.5 ug Hg (3.5 ug/1000 g)
XXIII. Chemist. According to clinical examination light mercury poisoning.
50 g blood: 0.25 ug Hg (5 ug/1000 g)
XXIV. Merchant who for some years had slept in a room with mercury spill. Symptoms of mercury poisoning had been present but had at the time of analysis nearly disappeared.
100 g blood: 0.31 ug Hg (3 ug/1000 g). In urine 3.2 ug/1000 ml
XXV. Wife of the former (see no XIII). The symptoms had not disappeared as much as for her husband.
109 g blood: 0.42 ug Hg (4 ug/1000 g). In urine 17 ug/1000 ml !
XXVI. Man who cleans mercury pumps. General neurasthenic symptoms.
206 g blood: 0.5 ug Hg (2.5 ug/1000 g)
XXVII. Similar occupation. Symptoms suggesting mercury poisoning
187g blood: 1 ug Hg (5.5 ug/1000 g)
XXVIII. Similar occupation.
143 g blood: 1.45 ug Hg (10 ug/1000 g)
XXIX. Chemist (see no XII). Works much in a room with 35 ug Hg/m3. Clear signs of a beginning mercury poisoning.
124 g blood: 0.9 ug Hg (7.5 ug/1000 g). In urine 11 ug/1000 ml.
XXX. Assistant in a chemistry lab. Apparent light mercury poisoning
146 g blood: 1.2 ug Hg (8 ug/1000 g)
XXXI. 55 year old man. Works since 6 years in a mercury rectifier factory. Comes much in contact with mercury. Signs of poisoning
172 g blood: 1.75 ug Hg (10 ug/1000 g)
XXXII. Glass blower (see no X). In the room up to 120 ug/m3. Various symptoms of mercury poisoning.
100 g blood: 6.5 ug Hg (65 ug/1000 g!).
When the mercury level in the air after cleaning up the workshop had been reduced to 2.5 ug/m3, it also dropped fast in his blood to the normal value. In 127 g blood: 0.8 ug Hg (6.5 ug/1000 g). In urine it remained high for a long time (see no X).
According to these results the human blood normally contains a few ug mercury in 1000 g; 6 to 7 ug is still not unusual. The levels do not rise to any noticable extent when a considerable mercury exposure occurs from mercury-containing air or amalgam fillings. Is this exposure stronger, the mercury level of the blood can be notably elevated (no XXI, XXXI, XXXII). After cessation of exposure, it will soon drop to the normal level, whereas the urine level can be elevated for a much longer time (compare especially no XX, XXV and XXXII). Urine analysis is therefore much better than blood analyses when abnormal mercury levels in the body are to be tested for. The results prove that the kidneys catch the mercury which has come into the circulation and slowly releases it into the urine.
In order to recognize mercury poisoning and maybe also for the treatment, we will give an evaluation of this study together with further experiments which will be reported elsewhere. Below is a summary of what is presently known and what must be considered when mercury analyses are used for the diagnosis of mercury poisoning.
1. Because of the mercury content of food, also persons with no other opportunity to take up mercury, regularly excrete mercury. This "normal" mercury level is up to a few ug daily in urine with small variations, in feces several (up to 10 ug/day) with wider fluctuations. On average, "mercuryfree" persons daily excrete a total of 5 ug mercury, i.e. corresponding to roughly the daily intake. An accumulation in the body with increasing age does not take place.
2. Among carriers of amalgam dental fillings, the mercury level in the urine is often only slightly elevated (a few ug/day), in feces, however, mostly considerably higher than among mercury- free persons. The conditions vary according to number, size, sort and condition of the fillings. Under
unfavorable conditions, also the mercury level of the urine is elevated to several times the normal.
Our experiments also prove that also the best amalgam fillings give off mercury.
3. Many persons are in such a position that they might absorb mercury vapor in their occupation
(physicists, chemists, doctors, dentists, workers in mercury-using factories etc) or in other ways
(broken thermometers, felt hats etc). Already after exposure to weakly mercury containing air (1/100 of saturated or less), the levels in urine are markedly elevated above normal. Among people who are occupationally exposed, the amounts can reach several mg/day also in the feces.
4. Small oral doses (as sublimate) of mercury are excreted within a few days, mainly in the feces, in some cases also in the urine (notably irregularly). Mercury absorbed in the lungs differs and has more harmful effects (which will be reported later). Possibly the varying poisoning effects by the amalgam fillings are related to how much mercury enters the body through the respiratory route and how much through the intestines.
5. The mercury level of the blood is normally a few ug, up to 7 ug/1000 g. It is higher as long as mercury is inhaled as vapor. After cessation of exposure or when it is only exposure to small amounts of mercury as from amalgam, it is hardly different from normal, whereas the urine can contain much more. Mercury which enters the circulation is taken up by the kidneys and slowly excreted.
6. For the diagnosis of mercury poisoning the mercury levels of feces and blood are generally of little value. More important is the analysis of urine (methods: A. Stock, F.Cucuel & H. Kohle, this journal 46, 1933, 187. Unfortunately the limit for a simple spectrographic determination of mercury in urine is about 15 ug/1000 ml according to R. Probst, Arch. Exp. Pathol. Pharmakol. 169, 1933,
119, and this is too high for most practical purposes). The equipment and methods for urine are also simpler.
If there are only a few ug in 1000 ml this contradicts a continuing or recent, notable mercury exposure and against immediate health disturbances because of still present mercury (about the not rare secondary, also after the disappearance of the mercury, consequences of a chronic mercury poisoning, we will report in a later publication). If the urine contains a little more mercury than normal (up to 10 ug/1000 ml), a mercury poisoning is not excluded; if it is about 10 ug/1000 ml it is likely. The decisive factor is the clinical finding (nervous- psychic symptoms, depression, pressure in the head, bleeding gingiva, stomatitis, chronic catarrhs, occasional diarrheas etc without other apparent causes). It must be noted that mercury disturbs the function of the kidneys and consequently can reduce its own excretion. Because of the irregular appearance of mercury in the urine, it is recommended that analyses should be performed on a few consecutive days, or a mean value obtained from several days. The blood analyses can be of value when one has to determine whether a stronger exposure still exists.
On Evaporation, Solubility and Oxidation of Metallic Mercury
(Ueber Verdampfung, Löslichkeit und Oxydation des metallischen Quecksilbers)
A. Stock Zeitschr. anorg. u. allgem. Chemie 217, 1934, 241-253 (According to studies by F.Cucuel,
F.Gerstner, H.Köhle and H.Lux) (Details in the dissertations by F.Cucuel, Freiburg 1931;
F.Gerstner, Karlsruhe 1931; H.Köhle, Karlsruhe 1933)
The observation that mercury evaporates through a layer of water initiated a number of experiments on the solubility of mercury, its evaporation and its oxidation by air (short, preliminary report
Naturw.sch. 20,1932, 954). Many of the questions which were touched upon deserve careful quantitative studies. We have not been able to follow up these questions since they were outside our goals.
To determine the small amounts of mercury down to 0.01 µg, we used the methods we have developed in recent years (Z. Angew. Chem. 44, 1931, 200; 46, 1933, 62 & 187; Chem Ber. 67,
1934, 122).
In the absence of oxygen or air, mercury dissolves very little in water, however, in amounts which are measurable (H.Reichardt & K.F.Bonhoeffer, Z. Elektrochem. 36, 1930, 753 showed that mercury at higher temperature, 140° C, dissolved in larger amounts which could be measured spectroscopically). Our most careful experiments used the described apparatus in high vacuum.
In A we placed 100 ml quarts-distilled, vacuum deareated water and in the thin-walled, evacuated vessel B, we placed a few ml of highly purified, vacuum-deareated mercury. After complete evacuation, we separated the connection to the pump by melting at the constriction (A cooled in liquid air), broke B by careful shaking and placed the apparatus for a few days in a thermostat at
30°C.The circulation of the thermostat caused a certain movement of the liquid. Stronger movement was avoided in order to prevent colloidal dispersion of mercury in the water. Then we tipped part of the water into D, still in vacuum, disconnected at E and determined the mercury content in D.
Consistent results from several determinations: 0.02 - 0.03 µg Hg/ml. If the separation of mercury and water was done in air instead of vacuum, the measured amounts of mercury rose markedly already after a short exposure to air to 0.06 µg/ml and higher.
Fig. 1. Determination of the solubility of mercury in water in the absence of air.
At elevated temperatures the solubility is higher. We found 0.3 µg Hg/cm3 of water at 85°C; 0.6 µg at 100°C.
In dilute potassium hydroxide and -chloride the solubilities at room temperature did not differ from those of pure water.
In the presence of air considerably more mercury is dissolved because of oxidation.
After the publication of our previous paper we also found that similar observations had been made earlier by the medical profession (comp. K.Korr, On the uptake of mercury and its compounds in the body Lieb Ann 104, 1857, 341; W. Braunwart, On the solubility of metallic mercury in various liquids of the body. Dissert. Wurzburg 1898). In Handbook of Toxicology by Kunkel (Jena 1901), it is stated (p.123) with reference to this dissertation: "Metallic mercury is, in the presence of air, dissolved in traces already in distilled water.. much faster and to a greater extent.. in sodium chloride containing water."
The following experiments were conducted at 30°C:
1. 200 ml water in a 250 ml retort with flat bottom was underlayered with purest possible mercury, left undisturbed. After various times 2 ml was removed by pipette and analyzed. The same study was repeated with quarts vessels.
Time 6 24 30 48 70 94 hours
Glass 0.23 1.4 1.9 2.6 3.7 4.3 µg Hg/ml
Quarts 0.26 1.1 1.7 2.8 3.8 4.5 µg Hg/ml
Thus there was no saturation after 4 days. No difference between glass and quarts; the alkali of the glass does not affect the solubility.
2. Experiment of longer duration to determine the saturated concentration. Experimental setup as in
1. a/ left undisturbed b/ bubbled with oxygen in the water layer (end of oxygen tube closely over the mercury)
Time 2 4 8 16 30 50 60 70 days a/undist. 2.65 4.7 6.0 7.9 13.7 19.3 -- --µg Hg/ml b/oxygen 3.3 7.1 12.0 17.0 27.0 38.0
39.6 39.3 "
In b/ saturation is reached after about 2 months; in a/ not yet. The dissolved mercury at saturation
(39.5 µg/ml, corresponding to 42.6 µg HgO/ml is exactly the solubility of HgO at 30°C. We determined this again since published values varied.
3. Purest possible red HgO was vigorously shaken with water at 30°C. The samples, which were used for determinations, were centrifuged to separate suspended oxide. Results:
Time 4 6 8 Days
42.6 42.1 42.4 µg HgO/ml, mean 42.4 µg HgO/ml i.e. the same amount as was found in experiment 2b. That mercury, in the presence of air, dissolves as HgO (or a hydrated compound of HgO) was determined by potential measurements. The series
Hg/saturated HgO solution/saturated solution from the experiment in 2b/Hg showed no potential difference. Both solutions exhibited identical behavior during reduction with phosphorous acid and gave colloidal mercury solutions which showed the Tyndall phenomenon.
Energetically the oxidation is understandable: Hg + O = HgO + 21.5 cal. The slowness with which it takes place, also in the presence of oxygen, is noteworthy.
In aqueous solutions of alkalihydroxide, more mercury dissolves in the presence of air, again as IIoxide. Saturation is somewhat more rapidly reached. Experiments with 5 and 10 % potassium hydroxide (30°C, undisturbed):
Time 1 4 8 12 20 Days
4/ 5% KOH 18.5 35.7 55.0 55.5 54.0 µg HgO/ml
5/10% KOH 35.0 103 135 135 135 "
The saturated solution contained in 4/ 58.2 µg HgO/ml, in 5/ 146 µg HgO/ml. When we determined the solubility of HgO in 5 and 10 % KOH we found 56.3 µg HgO/ml and 148 µg HgO/ml. In stronger KOH not much more HgO dissolved; in a saturated solution 160 µg HgO/ml. The increased solubility compared to water can probably be explained by the formation of salt (2 KOH + HgO =
K2HgO2 + H2O or similar).
Mercury dissolves with a similar rate in chloride solutions in the presence of air, then as HgCl and the solution shows an alkaline reaction (Probably in the form of complex salt with the alkalichloride.
The opinion in the older literature that HgCl2 is formed is false, something which already Gewecke showed). Experiments with 5 and 10 % KCl solution (30°C, undisturbed):
Time 2 4 10 16 20 Days
6/ 5% KCl 15.9 22.0 21.0 20.0 21.0 µg Hg/ml
7/10% KCl 33.0 37.5 42.5 47.5 48.0 "
The final values correspond to 26 µg Hg/ml and 57 µg Hg/ml. A determination of the solubility of
HgCl showed in 5 % KCl solution 26 µg Hg/ml and for 10 % KCl 56 µg Hg/ml. If mercury is left covered with chloride solution, crusts of calomel will form after a very long time.
With regard to the properties of mercury towards the living organism we made a similar study with the physiologically often used Ringer solution which contains the salts dissolved in blood (in 1000 ml: 8.0 g NaCl, 0.1 g CaCl2, 0.1 g NaHCO3, 0.07 g KCl). (30°C, undisturbed):
Time 0.5 1 2 3 6 8 Days
8/ Ringer 1.55 2.15 2.5 2.75 2.75 2.7 µg Hg/ml
The final value corresponds also here to the solubility of HgCl in Ringer solution (we found 2.8 µg
HgCl/ml, i.e. 2.4 µg Hg/ml). It is lower than in stronger KCl solutions but is reached faster (as the graphic presentation in the dissertation by Kohle p. 31 & 33 especially clearly shows).
That also water and aqueous solutions take up mercury from mercury vapor is shown by some other experiments, conducted at room temperature:
9. When 800 ml water had been in a 7000 ml vessel in the presence of Hg-containing air for 48 h the water contained 1.6 µg Hg, the air 26 µg Hg (3.9 µg Hg/1000 ml).
10. 200 ml water in a 7000 ml vessel with Hg-containing air. Shaken for 5 days. In the water 2.0 µg
Hg; in the air 22 µg Hg (3.2 µg/1000 ml).
Also at equilibrium (which was nearly reached in exp. 9) the water will only take up a small fraction of the mercury in the air. This appears to be connected to a dissociation of HgO which is likely to be enhanced by the low vapor pressure of mercury in these experiments (about 3*10-4 mm). That HgO already at ordinary temperatures gives off mercury vapor to the air is shown by the following experiment:
11. Purest HgO covered the bottom of a 4000 ml vessel. In the air above we found: after 2 4 6 Days
a/ at 20°C 2.8 3.0 3.0 µg Hg/1000 ml
b/ at 30°C 7.0 7.2 6.8 "
This corresponds to a mercury vapor pressure of 2.8*10-4 mm at 20°C, of 6.3*10-4mm at 30 °C. (It can hardly be a simple dissociation 2 HgO<--->2Hg +O2. For this is given that p2Hg.pO2 = K. If, in our experiment, pO2 equal to the partial pressure of O in the air (160 mm), the the dissociation constant will be (2.8*10-4)2*160 = 12*10-6. The total pressure which HgO must produce in vacuum follows from pHg=2pO2 and will be 45*10
-3 mm, the partial pressure of Hg 30*10-3 mm, i.e. more than the saturated pressure of Hg at 20°C which is only 1.8*10-3 mm. HgO should thus be unstable in vacuum and dissociate to a O-pressure of about 4 mm. However, we could certify that it does not at all give off such amounts of O in vacuum. Also the calculation of pO2 from other data gives far smaller values than the one above. According to Rothmund, Z. phys. Chem. 31, 1899, 74:
10-8 and according to Allmand, Z. Elektrochem 16, 1910, 261: 5*10-19 mm. The question needs further examination.)
It is thus considered that the air contained mercury as mercury vapor and not as HgO vapor. This was also the case; we could in such an experiment where the air should contain 14 µg Hg obtain not
less than 12 µg in a metal drop after condensation in liquid air. It is remarcable that the dissociation pressure at 20°C was equal to the mercury pressure in experiment 10.
Mercury vapor pressures of these magnitudes but with a greater range were found when we led air through a four-bulb tube with HgO and condensed the mercury which was taken up by the air with liquid air.
Also an aqueous HgO-solution gave off mercury to the air:
12. We led at 20°C air slowly (1 l/h) through a ten-bulb tube with saturated HgO solution (new solution for each experiment). The air took up 1.4-2.0 µg Hg/1000 ml, close to the values found in
10 and 11a. Also here could we with certainty demonstrate the metal by condensing in a capillary.
13. If we, instead of using an aqueous HgO solution, used the more HgO-containing, saturated solution in 5 % KOH, we found in the air at 20°C (1 l/h) in three tests 3.0, 3.1 and 3.4 µg Hg/1000 ml, again in agreement with the in experiments 10 and 11a found mercury concentrations.
The described experiments explain why mercury evaporates through water and aqueous solutions.
This can happen in two ways:
1. Mercury dissolves as metal and diffuses into the gas phase;
2. Mercury is oxidized to HgO, dissolves as such, and the HgO- solution gives off mercury to the gas phase. In the absence of air only the first is possible. The following two experiments (room temperature) compare evaporation of mercury through a water layer into air and into hydrogen gas
(carefully purified from oxygen); each time mercury was determined in water and in gas:
14: In a gas stream. Hg (40 cm2 surface area) with 2 cm water layer over; 2 l gas (1 l/h) was led over the water. a/ Hydrogen gas. Found in gas 2.0 µg Hg/1000 ml; in water 0.06 µg Hg/ml. b/ Air. In gas 1.5 µg Hg/1000 ml; in water 1.9 µg Hg/ml.
15. Undisturbed air. Hg in a 2000 ml vessel with 2 cm water overlayer; Gas at atmospheric pressure;
24 h at 11°C. The values are the means of three experiments: a/Hydrogen gas. In gas 5.3 µg Hg/1000 ml; in water 0.3 µg Hg/ml b/Air. In the gas 4.3 µg Hg/1000 ml; in water 1.4 µg Hg/ml.
(The vessel I was connected to another of similar size II. The latter was evacuated and we let half of the gas from I into the latter for analysis. The gas in II was then flushed out with 40 l mercury-free air into an U-tube in liquid air in which the mercury condensed.)
In 15a and 15b the gas was nearly saturated with mercury vapor. As expected the mercury levels, both for undisturbed hydrogen gas and for a hydrogen stream, was a little higher compared to air since in the latter some of the mercury in the water will be oxidized. Thus also the mercury level in the water is higher in the air-experiments than in the hydrogen gas experiments That the mercury level of the water, in the absence of air, in 14a and 15a is higher than in the previously described experiment in vacuum is explained by the fact that here mercury and water came into contact with air before the samples for analysis were removed.
In 15b the Hg level of the water is about 4 % and in 14b 5 % higher than the level in a saturated
HgO-solution. However, the mercury content of the air is nearly as large as in hydrogen gas and the conclusion must be that also in the presence of air, mercury immediately will pass into the gas phase as metal and not in a roundabout over HgO.
Mercury vapor behaves differently towards chloride-containing water. This takes up mercury completely:
16. 300 ml 10 % KCl solution in 7000 ml vessel shaken with mercury-saturated air at room temperature for 24 h. In the air we found 2.8 µg Hg, in the solution 49 µg Hg. Most of the mercury had disappeared from the air. In other similar experiments the Hg level in air was higher. Conditions will be more complicated in these experiments since HgCl, especially when exposed to light, can disproportionate into Hg and HgCl2.
17. Solutions of HgCl in 10 % KCl solution released considerable amounts of mercury into the air:
We led 6 l air at room temperature over 20 ml of such a HgCl-saturated solution (surface area 25 cm2) at a rate of 1 l/h. The air contained 7 µg Hg. Compare also exp.28b.
Blood completely absorbs mercury from air:
18. 300 ml bovine blood was shaken with Hg-containing air with a high concentration in a 8000 ml vessel for 24 h. No mercury could be found in the air (blind value of 0.1 µg). In the solution we found 38.0 µg Hg. Apparently the HgCl which will form will bind to proteins and other substances and not be released again. This latter experiment makes it understandable that our lungs almost completely absorbs inhaled mercury vapor.
In organic solutions mercury dissolves more than in water (in pentane at 65°C 6.5 µg/ml according to Reichardt & Bonhoeffer). We have studied the conditions in benzene according to the same methods as we used with water (to determine mercury in benzene we burned this after addition of four times alcohol or extracted the mercury with chlorine water. Comp Z. Angew. Chem. 46, 1933,
190). Benzene dissolved, in the presence or absence of air, at room temperature 1.5-2 µg Hg/ml.
When we led air or hydrogen gas for 2 h (5 l/h) through the saturated solution, the mercury level sank in both cases to about 1 µg Hg/ml. There is no oxidation by air. Corresponding to the higher solubility, also diffusion of mercury through benzene is faster than through water.
19. Methods as in 15; undisturbed gas; 11°, 24 h. Mean of three experiments: a/ Hydrogen gas. In gas 6.9 µg Hg/1000 ml b/ Air. In gas 4.8 µg Hg/1000 ml In a the hydrogen gas was nearly saturated with mercury.
20. Gas flow. Hg surface of 35 cm2, over that 1 cm layer of benzene. 20°. Air at 1 l/h. In the air we found 4.5-5.5 µg Hg/1000 ml. Also here the air was nearly saturated with mercury. It is surprising how fast mercury diffuses through benzene.
We report some less systematic experiments which originated from practical, physiological or occupational hygienic considerations.
21. Some solutions were left in contact with mercury-containing air (6 µg/1000 ml) for 10 hours under identical conditions: Petri dishes of 10 cm diameter, 1 cm liquid height, room temperature.
The solutions contained: a/ distilled water 2.2 µg Hg, b/ egg albumin solution 1.0 µg Hg, c/ bovine blood (undiluted) 21 µg Hg. The egg albumin solution showed no particular property to absorb
mercury. That it contained less mercury than water might depend on its higher viscosity. In contrast the blood took up ten times more mercury than water. Apparently, in additition to the chloride content, also the property of hemoglobin to transfer oxygen is important (comp. exp. 18).
22. Mercury uptake by some solid materials. Pieces of similar size (10*10 cm) were hung freely in a vessel through which mercury-containing air passed (again 6 µg Hg/1000 ml). The mercury uptake was on average: Filter paper 3-4 µg Hg, (We have already earlier showed that filter paper, after storage in a laboratory, contains mercury and must be washed with chlorine water before it can be used for determinations of small amounts of mercury.) Cotton absorbed 2.7 µg Hg, linen 4.9 µg Hg, silk 3.5 µg Hg, rayon 2.0 µg Hg, wool 0.3 µg Hg, turnips 200 µg Hg (We measured these since we used them as mercury-containing food for animals in studies on the distribution of mercury in the body. Dry material thus absorbed relatively little mercury. However, the studies showed that clothing absorbs mercury from mercury- containing air. The damp turnips absorbed much more mercury. The mercury penetrated into the inner of the slices:
23. The outer 1-2 mm of a turnip slice contained 20 µg Hg, the inner 5 mm 12 µg Hg.
The mercury-treated slices did not release mercury into the air:
24. 170 l air was led during two hours over a slice which had absorbed 225 µg Hg; The total amount in air was only 0.1 µg Hg.
25. Evaporation of mercury through various liquids. Hg surfaces of 30 cm2; over that the various liquids in 1 cm high layer; A slow air flow (6 l air, 1 l/h, Hg-free air) was passed over the liquids
(Apparatus: Dissert. Gerstner p. 26); temperature 20°. Mercury in air in µg/1000 ml.
Free mercury surface, uncovered: 12 (which corresponds to the saturated value at this temperature); water 0.2; benzene 6; paraffin oil 0.2; glycerol 0.5; carbon disulfide 3; sulfur chloride 6; phenyl mustard oil 9; through sulfur milk no mercury penetrated (prep. boiling sulfur with calcium carbonate and precip. with HCl). Remarcable is that benzene (exp 19 & 20) and organic liquids, especially the oil, easily lets mercury vapor pass through.
26. Similar experiments with solid substances (again 1 cm layer, apparatus as in 25); µg Hg/1000 ml air: Powdered sulfur 10; tetraphosphorous trisulfide 12; silica gel 1; activated charcoal almost nothing, after 3 months storage 1; iodine-treated activated charcoal nothing, after five months storage nothing. Sulfur and also the phosphorous sulfide hardly inhibits evaporation of mercury.
Iodine-charcoal is an excellent absorbent for mercury vapor (It is manufactured by Auergesellschaft,
Berlin. comp. A. Stock, Z. Angew. Chem 47, 1934, 64).
27. In some other experiments we mixed air which was passed over uncovered mercury with small amounts of other gases; other methods as in 25. Mercury in µg Hg/1000 ml gas: With hydrogen sulfide (damp, 5 vol%): 9, with chlorine (5 vol%) 0.3; with iodine (1 mg/1000 ml) almost nothing.
Here it it noteworthy that the presence of hydrogen sulfide hardly affected the evaporation of mercury. With iodine a layer of HgI and HgI2 formed within a short time.
28. In the following experiments (methods as in 25) we measured, in addition to the level in air, also the dissolved amount of mercury in the aqueous solutions:
Liquid In air. µg Hg/1000 ml In liquid. µg Hg/ml a/ water 0.2 1.3 b/ 5% KCl 0.2 5.2 c/ 5% H2SO4 0.9 6.0 d/ 50% " 0.2 3.0 e/ conc " 0.1 23.5 f/ 1% KOH 0.3 6.0 g/ 10% " 0.6 7.5 h/ 50% " 0.05 0.4
The large mercury absorbtion by the concentrated sulfuric acid is probably caused by an immediate reaction between this and the mercury. The especially low absorbtion by the concentrated KOH can be explained by its viscosity. In one of the experiments with dilute sulfuric acid we could demonstrate that mercury again evaporated from the acid and could be precipitated as a metal drop.
Finally some observations on the evaporation of small mercury droplets: The droplets which are obtained e.g. with the micrometric mercury determination, evaporate extremely slowly. With droplets of 8 µg and 80 µg weight (diameter 105 and 225 µm) we could find no reduction in size after several months in air when left undisturbed. When we had distributed 100 µg Hg by careful distillation in a 2 mm tube as a fine surface precipitation and led 250 l air in three hours over it, the air only contained 1.9 µg Hg. This result is surprising when one remembers how fast a large surface of mercury gives off metal to the air (comp. exp 25). An explanation might be that also mercury, as other nobler metals, e.g. silver, is oxidized on the surface and that the thin oxide layer in the small droplets is less easily broken than in larger ones which vibrate in an air flow (The surface oxidation has been suggested several times, recently by K.Schafer, Z. Physik 77, 1932, 212. Maybe also observations like those of K.Freudenberg & H.Eyer, Z. physiol Chem 213, 1932, 232, that mercury of common purity inhibits the activity of insulin whereas highly purified metal does not, can be explained by an oxide content of the less pure metal.)
29. We led an air flow over three mercury drops of various sizes at room temperature (1-2 l/h). The table shows the reduction of the diameter (um) and the weight (µg):
I. II. III.
Start of exp. 291 um,173 µg 143.5 um,21.2 µg 80.8 um,3.85 µg
After 5 days 286 163 143.0 21.0 not measurable
After 16 " 272 145 138.5 19.0 78.4 3.50
Weight loss 28 µg 2.2 µg 0.35 µg
Loss µg/um2 2.4*10-3 1.6*10-3 1.3*10-3
In a similar experiment in hydrogen gas instead of air we found:
Start of exp. 27.4 µg 14.10 µg 7.97 µg weight loss
µg/um2 6.7*10-3 8.7*10-3 9.3*10-3
In hydrogen gas the evaporation is higher than in air, something which is in agreement with a surface oxidation. However, this could also be explained by a more rapid diffusion rate in hydrogen gas. The results from the experiments do not differ much when related to surface area. Before any firm conclusions can be drawn, the experiments must be repeated under more exact experimental methods; careful regulation of temperature and air flow.
Our reports show how the improved methods for mercury analysis have made possible or easier the experimental study of many new questions. The observations on oxidation and evaporation of mercury explain several facts which have been so far hard to understand.
For instance it is now clear that the evaporation of mercury is not inhibited by a layer of water. The relation between mercury, water and air is also one of the causes why we and others had difficulties when we tried to produce an air flow with a certain low mercury concentration by cooling saturated air to a temperature with the appropriate mercury vapor pressure (Comp. A. Stock & W.
Zimmermann, Monatschr 53/54, 1929, 786 & 55, 1930, 1; K. Müller & P. Pringsheim Z. Physik 65,
1930, 739). One of the premises is, which has now been shown, the careful drying of the air
Another fact is often disputed. When mercury containing air is inhaled, the mercury is nearly completely retained. Now we know that in lungs are the best conditions for oxidation of mercury, blood with a large surface area, oxygen, elevated temperat ure. (The mercury is oxidized primarily to HgCl; According to K.Voit, HgCl reacts with proteins, blood etc under formation of soluble mercury compounds).
Also we have an explanation for the occurrence of mercury in all samples of rain water because of oxidation and solubilisation of mercury in the atmosphere. Mercury, in high dilution, appears to exhibit a circulation; evaporates from the ground and returns with rain water. The general occurrence of mercury in all substances (which we will report next) should be connected with this behavior. Since it is known how effective mercury can be as a catalyst and as a catalyst poison
(comp. G.Bredig & K.Ikeda Z. phys. Chem 37, 1901, 63), one can suspect that this distribution of mercury also is of biological importance.
The Mercury Content of the Human Body
(Der Quecksilbergehalt des menschlichen Organismus)
Biochemische Zeitschrift 304, 1940, 73-80
XXX Report on the effects and distribution of mercury
A. Stock, Berlin-Dahlem
In a recently published paper in this journal J. Bodnar, Ö. Szep and B. Weszpremy discuss the natural mercury level in the human body (Biochem. Zeitschr. 302, 1939, 384), i.e. the mercury content of the organs, originating from (mercury-containing) food but not from other sources. The authors determine mercury in various organs of three persons who have died of severe diseases.
They were considered "mercury free" and had not, as carefully as this could be determined, been in contact with mercury when they lived and had no amalgam fillings. Bodnar et al obtained the following values (nanograms/g; ng/g = µg/kg wet weight):
################################################################
All values in the original paper are in µg/100 g. They have been changed to ng/g (nanograms/g) which is the usual unit today.
################################################################
20 y woman 62 y woman 19 y woman
Pneumonia Heart failure TBC
Kidney 174 223 580 ng/g
Liver 170 103 446
Lung 53 94 506
Blood 78 342 346
Gall bl.
+contents -- -- 325
Spleen 362 700 422
Heart 255 -- 340
Stomach + -------» 310
intest. 26 -- 325
Brain 6.3 46 445
Muscle -- -- 6
The three series of measurements do not agree very well and also give higher values than earlier, singular measurements which have been published. Especially the blood values are too high. In our extensive study on live persons (Stock & Cucuel, Z. angew. Chem 47, 1934, 641) we found in
"mercury-free" persons only up to about 7 ng/g whereas these values are 50 times higher (not 500 times as the authors write), i.e. even more than the peak levels which are reached during a mercury ointment (250 ng/g) treatment. We have also, in connection with mercury poisoning, for a long time been interested in the question of normal levels in human organs. And in which organs does it accumulate? We have been able to collect a substantially larger and more conclusive material. We intended to publish it together with still not finished studies but because of the paper by Bodnar and collaborators I will report on the current observations.
In order to possibly avoid pathological complications we took our autopsy material from persons who had died by accident or suicide and not because of diseases (which also the Hungarian researchers plan to do). The University clinic for Forensic and Social Medicine (director: Prof. Dr.
Müller-Hess) supported us generously.
We differentiate between the two groups A: Mercury-free and B: Carriers of amalgam dental fillings.
Previous work had shown that the excretions from persons in the B group is generally much higher than from group A. A carrier of a few small, insignificant amalgam fillings (case I) has been included in group A where it also doubtless belongs according to the measurements. A good criterium for uptake or not uptake of "unnatural" mercury is found in the Hg-level of the kidneys; the limit is about 100 ng/g. We include an amalgam-free case (case VIII) in group B since in this case there could be no doubt about mercury uptake from some other source.
The analyses were made according to previously reported methods and experience. Again it was evident that there are many sources of errors (e.g. Hg in the reagents, glass vessels, water and laboratory air) which can affect the determination of the smallest amounts of mercury. Mercury determination in organs of 1 g weight or less requires extreme demands on training and self- critique of the analytical scientist.
The table contains our analytical results in ng/g wet weight. After the name of the organ is the usual weight of the organs we obtained for analysis. From this one can obtain the approximate amount of mercury found in any measurement; they were often as low as a few hundredths of a microgram. 0 means that no Hg was found, and -- no measurement (mostly because we did not obtain the organ).
Cases: A. Hg-free I-VI
I. 28 y male painter. CO-poisoning
II. 15 y male plater apprentice. Occupational accident
III. 18 y female shop assistant. Fall from window
IV. 26 y male manual worker. Occupational accident
V. 25 y male carpenter. Occupational accident
VI. 29 y male shop assistant. Veronal poisoning
B. Amalgam carrirs etc.
VII. 24 y female servant. Hydrochloric acid poisoning
VIII.37 y widow. Drowning
IX. 31 y male painter. Occupational accident
X. 60 y male factory superwiser. Sleeping pill poisoning
XI. 21 y female. Housewife. CO-poisoning
In some of the cases we made some single measurements (ng/g):
In VIII we found: Tongue (61 g) 8 ng/g
Pancreas (39 g) 3
Aorta (18 g) 2
Skin (13 g) 6
Cartilage (16 g) 6
Bone (10 g) 13
Bone marrow (16 g) 19 These measurements did not show anything special; they were in the same range as the other values from heart, spleen muscle.
________________________________________________________________
I II III IV V VI _ VII VIII IX X XI
A. Mercury-free _B.Amalgam carriers etc
________________________________________________________________
1.Cerebral _
cortex(40g) 8 2 1 3 7 9 _ 15 563 108 23 9
2.Brain _
ventral(40g) 9 4 2 -- -- 4 _ 13 -- 80 17 --
3.Cere- _
bellum(40g) 6 4 2 3 7 30 _ 14 1180 158 19 10
4.Basal _
ganglia(40g) 6 4 2 3 7 4 _ 11 348 60 23 6
5.Brain stem _
(10g) 11 4 0 -- -- 8 _ 20 515 263 5 --
6.Olfactory _
bulb (0.6g) -- 31 87 19 6 -- _ 480 224 191 -- 132
7.Pituitary _
gland(1g) 133 61 -- -- 40 81 _ 232 -- 130 158 40
8.Spinal cord _
(7g) 5 1 1 6 6 17 _ 14 137 43 9 22
9.Lymph nodes _
(2g) 18 4 21 1 0 0 _ 69 160 120 18 6
10.Thyroid (20g) 18 5 5 9 7 94 _ 30 65 58 354 29
11.Soft _
palate(10g) 7 4 12 -- -- 12 _ 53 9 12 36 --
12.Epiphysis _
(0.9g) -- -- -- 4 0 -- _ -- -- -- -- --
13.Salivary _
gland(10g) -- -- -- 4 0 -- _ -- -- -- -- 34
14.Tonsils (10g) -- -- -- 10 9 -- _ -- -- -- -- 44
15.Kidney (40g) 40 46 30 82 76 102 _5130 369 141 728 167
16.Adrenal (10g) -- -- 9 2 46 13 _ 161 2 9 53 43
17.Liver (40g) 12 47 6 25 42 118 _ 460 61 87 81 115
18.Spleen (40g) 4 5 3 -- -- 5 _ 54 12 9 21 --
19.Lungs(40g) 9 7 5 -- -- 9 _ 49 12 20 16 --
20.Heart (40g) 7 4 1 3 5 12 _ 55 16 9 22 47
21.Stomach (40g) 19 5 1 -- -- -- _ 46 -- 10 35 --
22.Large _
intest.(20g) -- -- -- -- -- -- _ -- -- -- -- 78
23.Appendix (5g) 4 11 -- -- -- 1 _ 234 22 6 13 --
24.Gall bl.+ _
bile(10g) -- -- -- 10 21 -- _ -- 13 -- -- 37
25.Testes or _
ovary (10g) -- -- -- 1 5 -- _ -- 0 -- -- 1
26.Muscle (40g) 5 3 3 1 5 6 _ -- 8 -- -- 15
27.Fat(10g) 18 -- -- -- -- 5 _ 478 4 14 -- --
28.Blood (25g) 4 4 2 -- -- 31 _ 31 6 7 10 --
29. Hair(5g) -- -- 49 -- -- -- _ -- 216 -- -- --
In XI we could analyse a gallstone (1.4 g): 11 ng/g
In IV we obtained the kidneys in pieces: cortex right (22 g) 92 ng/g cortex left (25 g) 96 marrow right (17 g) 61 marrow left (14 g) 53
The cortex thus contained substantially more Hg than the marrow. We did not otherwise find any great differences between the both kidneys.
We analysed an additional three samples of hair from women (washed and degreased): 1. (46 g)
2740 ng/g; 2. (5 g) 746 ng/g; 3. (25 g) 300 ng/g. These are considerably higher than the also high ones in the table. We do not know how much use of Hg- containing preparations, oils etc and maybe also the high Hg- level in the street dust (see below) or felt hats has to do with this or whether an accumulation of mercury from the body actually takes place in the hair.
For group A, mercury-free, one can draw definite conclusions from the table. Hg is present in most natural animal and vegetable matter and also in the human body to a level of 10-9 to 10-8, i.e. 1-10 ng/g. That single measurements differed can not change this conclusion. In some organs it will accumulate. Primarily this is the case with the kidneys as our animal experiments also show. The level will be about 10 times higher than in the mercury-poor organs. In addition, it will accumulate in the liver even if it is to a lesser extent than in the kidneys (the exception VI will be discussed below).
No accumulation takes place in the the heart, lungs, stomach, brain, the relatively mercury-poor muscles and also not in the spleen which Bodnar et al consider the most mercury-rich organ. The blood contains, also in contrast to the opinion of the Hungarian researchers, not more mercury than we previously found in living people (exception again VI). However, the blood values in dead people might not be too important since blood can and will change Hg-level after the cessation of the circulation.
In case VI we find values which differ from the others: more mercury in the cerebellum, spinal cord, thyroid, liver and also blood. This case where the cause of death was veronal poisoning, must be considered pathological. A special uptake of mercury must have taken place and the distribution of mercury in the body has not followed the usual pattern, maybe influenced by the (slow) effect of the poison and also previous disease. It should have been appropriate to exclude this unclear case. I have not done so in order to avoid any conditions but also to show that one has to avoid too general conclusions from a limited material. As really conclusive one can consider cases I to V, in which
young, healthy persons had a rapid death. In these cases the results agree to an extent which can be expected from such physiological studies.
An elevated level of Hg is also found in the olfactory bulb and especially in the pituitary gland. The latter is a surprising finding which will be discussed below. The appearance of higher levels in the nose and in the olfactory bulb have already been found in animal experiments and has also alsmost always been confirmed in the ongoing studies on human material. This can be explained by the fact that also for "mercury-free" persons there is another source of continous exposure to mercury in addition to food: Dust (for smokers also tobacco smoke which will not be further discussed here).
Dust contains, especially in the cities with their soot-containing air, much Hg. We found earlier
(Naturw.sch. 22, 1934, 390) in the soot from cooking stove 3500 ng/g, a factory 28000 ng/g, in
Karlsruhe street dust 870 ng/g. The dust in Berlin does not differ. A dust sample from an open place in a densely populated area contained in june, i.e. the season without heating, 940 ng/g, another from a street 310 ng/g Hg. The dust on the ground consists mainly of sand and silicate fragments.
From the inhaled, more soot-rich dust, Hg must deposit in the olfactory mucosa and then reach the organs with connections to the nose, primarily the olfactory bulb.
The results in group B, the carriers of larger amalgam fillings, do not allow such conclusive results.
One must expect less uniformity. The amalgam fillings give off Hg as vapor (as HgCl2- vapor, comp. Ber. Dtsch. Chem. Ges. 72, 1939, 1844) which is inhaled and also solubilized or particulate
Hg to the gastrointestinal tract. The amounts will be very variable and depend on the composition of the amalgam (Cu- or Ag-amalgam), size, position, age and mechanical load on the filling, pH of the saliva etc. At least in case VII, poisoning by hydrochloric acid, the unusually high amounts of Hg
(kidneys 5130 ng/g!) in almost all organs suggest another source of mercury. The often high level of
Hg in hydrochloric acid is not a sufficient explanation. Opportunity for "unnatural" uptake of mercury is common: treatment with Hg-containing compounds (ointments, drugs), staying in Hg- or
HgCl2-containing air (broken thermometers, old amalgam mirrors, open or evaporated HgCl2 solutions, occupational exposure to Hg or HgCl2 etc. (In older hospitals the air is constantly more or less Hg-containing). Whether one or more such exposures has happened in a specific case can rarely be determined for deceased people. If the samples originate from people with a violent death (which is certainly better than undoubtedly pathological cases which constituted the material in the work by
Bodnar et al and where unnatural uptake of mercury must have occurred), it is mostly very difficult to obtain information on such circumstances.
Despite these uncertainties one can draw some definite conclusions from group B. They agree with conclusions from group A.
The general Hg-level in amalgam-carriers is, as could be expected, clerly more than normal. The kidneys are again the principal accumulators of Hg and the level is several times higher than in the liver (because of the size of the liver the comparison of total amounts of Hg in these organs will be different). The spleen is not more Hg-rich than lungs, heart, stomach etc. Especially small amounts are found in the muscles. The Hg-level in blood is only elevated above normal in VII and despite the impregnation of the organism with Hg in this case, only moderately so. A new confirmation that the circulating Hg in blood is rapidly taken up by the kidneys (and apparently also by the liver). Notable is the high Hg-level in brain and brain stem in cases VIII and IX. The elevated levels in olfactory bulbs and hair have been discussed above.
Also in this group the most conspicious finding is the accumulation of mercury in the pituitary gland
(1580 ng/g in X!, unfortunately we could not obtain the olfactory bulbs in this case) and also -maybe connected with this - in thyroid and lymph nodes.
The observation that the pituitary gland, which despite its small size, is of such importance for the regulation of the hormonal status, accumulates mercury to levels similar to the kidneys, should be of extreme importance for the mechanism of chronic mercury poisoning. If an above normal Hg-level disturbs the functioning of the pituitary gland as it is known to do with the kidneys (inflammation, anuria, uremia etc), then almost all symptoms of the up to now quite mysterious chronic mercury(- vapor) poisoning can be explained. Before this is discussed more in detail, more material will be studied. Our current, because of the difficult analyses rather time-consuming, studies might answer the following questions: How does mercury enter the pituitary gland; from the general circulation or
(as it appears) from the nose? Where does it go from the pituitary gland? Into the brain and in which parts of the brain? Is there a connection between the Hg-level in the pituitary gland and in certain other glands? What is the level of mercury in the organs in various pathological cases? What diseases causes the elevated mercury levels?
The answer to these questions might, in addition to mercury poisoning, be of value also for the treatment of other types of poisonings.
We are, in addition, also studying the changes in blood mercury levels during the course of mercury ointments. No values have up to now been published.
My gratitude to the German Research Council and the Schering AG for supporting also this study, to
Helene Heintze, Ruth Lehmann and Elisabeth Grube for careful analytical work.
Summary
The "normal" Hg-level, i.e. the level not originating from nonnatural sources has been determined in a large number of human organs (with about 250 micro-Hg determinations). As study material we used bodies from persons who had died a violent, fast death in order to avoid pathological complications.
The general level og Hg in the human body is similar to that in the organic world, in animals and plants and in general in the range 1-10 ng/g wet weight. In carriers of amalgam filings it is -often considerably - higher.
In some organs Hg accumulates, especially in the kidneys, to some extent also in the liver and conspiciously so also in the pituitary gland. This unexpected finding is of utmost importance for understanding the mechanisms of chronic mercury poisonings especially and probably also for medical understanding of poisonings in general. If the functioning of the pituitary gland is disturbed by elevated levels og Hg in similar ways as that of the kidneys, something which must be presumed, then almost all symptoms which so far have been difficult to interprete, can be explained. Maybe also directions for therapy can be inferred. The studies will be continued in various directions.
According to our findings, the higher levels for the normal Hg- content, reported by others, can only be explained by other sorces of exposure for the pathological material which was used.
In addition to food, also inhaled dust is a source which continously exposes the organism to traces of mercury.
GALVANIC BURNS OF THE ORAL MUCOSA
L. Hollander, M.D., Pittsburgh
JAMA 99, 1932, 3834
In a recent contribution, Everett S. Lain called the attention of American dermatologists to an important and what might appear as a relatively frequent cause of lesions of the oral mucosa (1).
Three patients have come under my observation recently in whom annoying lesions of the oral mucous membrane disappeared on the removal of amalgam and gold dental fillings and other gold appliances in accordance with the principles outlined by Lain. Each instance can be considered clinically to have been a galvanic burn of the oral mucous membrane.
REPORT OF CASES
CASE 1. Mrs. A. P., aged 28, was examined, March 10, 1930, on account of multiple, recurrent and exquisitely painful ulcers of the oral mucosa, resembling the clinical picture of aphthous stomatitis.
The ulcers first appeared about two years before and usually numbered from fifteen to thirty at various times, being always decidedly worse just before her menstrual periods. A routine examination revealed little of importance.
Mouth smears were negative. Gastric analysis showed a low content of hydrochloric acid. The pharynx and the cornea were in a condition of anesthesia, as one at times finds in hysteria.
Testing of sensitivity to foods both by intradermal injections and by the trial method proved nothing.
When the patient was given dilute hydrochloric acid in doses of 30 minims (2 cc.) the lesions of the mucous membrane increased.
Slowly the patient was so much worse that she found it extremely difficult to masticate her food. She was then placed at absolute rest in bed, on a milk diet, for a period of six weeks. There was some improvement, but the ulcers continued to recur.
Shortly after Lains communication, all the amalgam fillings were removed from her teeth and replaced with temporary (cement) fillings. Within ten days there was a great change and since then there has been no recurrence of the ulcers, though two menstrual periods have passed.
CASE 2. L. W. O., a man, aged 31, was examined, June 16, 1931, on account of a sore tongue of four months duration. The sore complained of was a whitish-gray elongated patch about 2.5 cm. long and 1 cm. wide, affecting the under and lateral surface of the right side of the tongue opposite, a gold fitting of a so called hygienic fixed bridge, which occupied the space of an extracted lower right first molar. There were two other similar patches on each side of the buccal mucosa. The patient complained of a metallic taste. He smoked about twenty cigarets a day.
Smears of the mouth, and general and serologic examina tions, proved nothing.
On account of the appearance of the lesions and the history of a fair amount of smoking, I considered the lesions as smokers patches, but the discontinuance of the use of tobacco had no effect on the lesions.
Further questioning proved that these lesions began shortly after the hygienic fixed bridge was placed in the mouth.
Examination also showed a number of amalgam fillings in the teeth. On removal of the gold bridge, all the lesions disappeared. In January, 1932, the same gold bridge was replaced and within one week the same lesion of the tongue and on the right buccal mucous membrane and also the metallic taste reappeared. Within a week after the second removal of the gold bridge the lesions and the metallic taste disappeared, and the patients mouth since then has remained well.
CASE 3. N. K., a man, aged 41, consulted me, Dec. 15, 1931, on account of painful and recurring ulcers of the mouth, which clinically resembled those of aphthous stomatitis. This condition had been recurring for a period of eighteen months. There were eight lesions in the patients mouth, each one oblong and sharply defined, with an inflammatory halo around a necrotic center, which was covered by a yellowish pyogenic membrane. He did not complain of a metallic taste. He had many amalgam fillings in his teeth and also a gold crown over the lower left incisor tooth. After the removal of this crown, the ulcers disappeared and have not recurred since.
Comment: Each instance seems to fit to the fact that the principle of Lain is correct and that two dissimilar metals suspcended in normal saliva, which is a fair electrolyte (Hodgen, quoted by
Lain) complete a galvanic battery.
Summary: One case of so-called smokers' patches (leukoplakia) and two cases of aphthous stomatitis-like ulcers of long standing were cured when the metals producing the galvanic burns of the oral muccosa were removed, after all sorts of other therapy failed.
1. Lain, E. S.: Chemical and Electrolytic Lesions of the Mouth Caused by Artificial Dentures, Arch.
Dermat. & Syph. 25:2131 (Jan.) 1932.
Electrogalvanic phenomena of the oral cavity caused by dissimilar metallic restorations
By E.S. Lain, M.D., and G.S. Caughron, D.D.S., Oklahoma City, Okla. Journal of the American
Dental Association 23, 1936, 1641- 1652
Human saliva contains the necessary elements for a good electrolyte, whether its chcmical reaction is neutral, acid or alkaline; therefore, a galvanic battery has been constructed in every oral cavity where restorations have been made from two or more electropotentially dissimilar metals. This fact is as fundamental as the law of gravity.
In archives of medical and dental history, the possibility of electrogalvanism between dissimilar metallic restorations has been mentioned and a few clinical case reports published at intervals since the earliest days of metallurgic dentistry, though not until within the past six years, since a more thorough analytic and clinical study has been made, has this problem become one of, serious pathologic significance.
One of us (E.S.L.) made mention of phenomenon more than a decade ago, but, like other physicians or dentists, did not consider the matter of sufficient consequence to demand immediate clinical and laboratory investigation. It was late in 1930, after our observation of a succession of cases of oral cavity lesions in which all other etiologic factors could be eliminated, that the urge for a thorough investigation of the oral electrolysis began.
The first case report and comments (1) on this subject were made before the American Medical
Association in 1931. In two additional articlcs (2) further laboratory studies, case reports and clinical investigations are reported which are believed to fully justify certain deductions and conclusions.
Other physicians and dentists have, since 1931, made similar studies and published their findings and case reports in dental and medical journals, which have, in the main, agreed with our own. This paper, therefore, is largely a review and confirmation of our previous work, but is based upon an
examination and study of more than 1,000 additional oral cavities which contained dissimilar metallic restorations,
Studies of resistance of mouth structures and of spectroscopic examinations of tissue taken from ulcers and leukoplakia areas have further revealed the pathologic process of oral electrolysis.
SUBJECTIVE SYMPTOMS
The common symptoms of electrochemical change in the mouth we have classified as follows:
1) metallic or salty taste, immediate, in occurrence, though later tolerated or perhaps forgotten; (2) increased salivary secretion; (3) burning or tingling sensation, usually occurring first on the margins of the tongue; (4) occasional nerve shocks and pulp sensitivity from connecting restorations or from connections made by a spoon or table fork; (5) pathologic changes in the blood, kidneys or other organs, probably caused by absorption of ionized toxic metals, and (6) general discomfort in the mouth, irritability, indigestion, loss of weight and, in some cases, reflex radiating neuralgic pains through branches of the fifth trigeminal nerve.
During the course of our clinical studies, one of us (G.S.C.) has been particularly interested in the possibility of reflex sensory nerve disturbance arising from oral electrolysis.
Three positive cases of erosion and ulcer of the buccal and lingual mucosa had also presented a more or less constant neuralgia-like pain radiating from the area of the ulcers through the sympathetic branches of the trigeminal nerve. We have noted in some cases a slight itching, stinging, puckering sensation, especially at the trigeminal nerve endings on the mucosa. This may be explained on the basis of the law of referred pain.
After the establishment of a homogeniety of dental restorations in each case, not only did the mucous lesions promptly heal without other treatment, but also the neuralgic pains slowly subsided and did not recur.
As the trigeminal or fifth nerve has both motor and sensory functions with branches that supply the various soft and hard structures of the oral cavity, it is not wholly speculative to assume that certain cases of persistent radiating neuralgia may be laid at the door of oral cavity galvanism.
OBJECTIVE SYMPTOMS
Metals. 1. Disintegration and discoloration of metallic restorations: The electropositive metals give evidence of erosion characterized by a clean, bright appearance. In electronegative restorations, there is often a darkened, tarnished color, the result of the presence of sulfides and other ionized products, which have migrated from the potitive metals, such as aluminum, zinc, tin, nickel and copper, through the saliva, to be deposited on the electronegative gold, platinum or silver fillings etc.
2. Dental cement: Cement that contains a high percentage of zinc is also strongly elcctropositive in relation to the noble metals; hence, when it is exposed to the saliva, its rapid solution occurs. This permits a loosening or falling out of fillings, both silver and gold.
Mucosa. - In examination of the mucosa, there are found: (1) erythema with congestion and blanching of the mucosa, and evidence of intermittent or chronic irritation; (2) prominence and sensitivity of both anterior and posterior groups of the papillary bodies of the tongue; (3) erosion areas and ulcers on the margins, and denuded patches, geographic linguae, on the dorsal areas of the tongue, even the more severe symptoms being periodic and influenced by a change in diet, and (4) leukoplakia, a grayish, slightly elevated, precancerous lesion, usually resulting from a long period of chronic irritation, which may be nature's warning before more serious pathologic processes develop.
Electrogalvanic lesions upon the mucosa most frequently occur adjacent to or near the positive metal, though some times occurring elsewhere.
Both visible lesions and subjective symptoms produced by electric irritation in the mouth depend on many conditions, such as: (1) the degree or amount of electric potential which may be generated between metals, the current flow being intermittent or continuous, varying with resistance of tissue and positions of the mouth and tongue; (2) toxicity of certain metals used in restoration alloys; (3) duration or time since the completion of the necessary elements of the galvanic battery.
Contributing factors consist of: (1) any rough or ill-fitting dentures or fillings; (2) infections by various microorganisms, and diseases that may also affect the oral mucosa; (3) alcohol, tobacco or other habitual mouth irritants, and (4) congenital or acquired personal sensitivity to certain metals, such as aluminum, nickel, copper, tin, and zinc, which is well known to dermatologists and industrial physicians.
We have repeatedly observed that infections, excessive use of alcohol or tobacco, disease and drug eruptions appear to lower tissue resistance to electric current, and, hence, give an increased meter reading. A variation of the pH of saliva either to a strong acid or an alkaline, will give an increase of meter readings of from 30 to 50 per cent.
The paramount factor is the electro chemical difference in the heterogeneous metals used in dental restorations; in other words, their relative positions as found in the Standard Electromotive Series of
Metals.
TABLE 1. METALS IN ELECTROMOTIVE FORCE SERIES
Poaitive End; Lithium, Cesium, Rubidium, Potassium, Sodium, Barium, Strontium, Calcium,
Magnesium, Aluminum, Manganese, Zinc, Chromium, Cadmium, Iron, Thallium, Cobalt, Nickel,
Tin, Lead, Hydrogen Oxide, Arsenic, Copper, Bismuth, Antimony, Mercury, Silver, Palladium,
Platinum, Gold, Fluorine, Chlorine, Bromine, Iodine, Oxygen; Negative End
Positive cases of electrogalvanism will begin to improve at once and all lesions except leukoplakia, which is a hypertrophy of tissue, will heal promptly after the removal of prostheses of either the positive or the negative group. When lesions have healed, new restorations made with perfectly homogeneous metals are a guarantee against recurrence.
May we reemphasize a statement made in each of our former papers: Before a final diagnosis of electrogalvanic injury to the oral mucosa is made, one should try to eliminate the possibility of certain fungus and Vincent's infections and skin eruptions, such as syphilis, lichen planus, herpes, erythema multiforme, lupus erythematosus and gastrointestinal and blood dyscrasias, which may also cause similar lesions on the oral mucosa. To do this, it may be necessary to consult both an internist and a dermatologist
LABOBATORY EXPERIMENTS AND DIAGNOSIS
An attempt was made with a wheatstone bridge, a galvanometer and other instruments to evaluate the factors of heat, resistance and direction of current flow through the various tissue structures of the oral cavity. We learned that the calories of heat generated by the average amount of electric current in the mouth are probably insufficient to cause an immediate destsuction of tissue or a burn.
We found that normal tooth enamel offers a very high resistance to current flow. Maxillary bone ranks second, or next highest, registering 18,900 ohms.
The buccal mucosa is next in order, registering 2,300 ohms. We were surprised to learn that the tongue gives the least resistance, 960 ohms, of all oral structures when tested either transversely or longitudinally.
There are many other important factors in electrical determinations which might raise a question as to the accuracy of our estimations, though our findings do suggest the possible answer to the question as to why the tongue appears to suffer the most frequently and severely of all oral structures.
The electrochemical potentiality or behavior of dental metals toward each other may be satisfactorily tested en bloc before casting into forms for various kinds of restorations by immersion in a glass tray containing a buffered solution, preferably of pH 5.8 (acid), then make a contact of each with electrodes connected with the poles, negative and positive, of the microammeter.
For making electric estimations of potential damage to tissues, we prefer a Weston microammeter, model No. 440, which has a range of 75 microamperes. A model No. 220 has a scale of 200 microamperes, which is needed in only a few cases. The microvoltage, if desired, may be obtained by multiplying the microamperage by the ohms of resistance, which is recorded on a test of each instrument before leaving the factory.
REVIEW OF LITERATURE
From 1878 to 1918, Palmer, Chase, Mayer, Patrick, Morrison, Grant, Davis, Essig, Hepburn,
Manning and perhaps two or three others mentioned the possibility of electric phenomena occurring between different metallic prostheses in the oral cavity. Their discussions dealt almost entirely with the possibility of such phenomena and with reports of laboratory studies for confirmation.
They apparently reasoned that electrolysis between dissimilar restorations was of insufficient degree to cause any pathologic changes in the oral structures. Grant even suggested that the stimulation of such a current was perhaps a benefit instead of injurious. Palmer and Mayer actually ridiculed the whole subject.
Essig and Manning considered the matter more seriously, and each gave one case report. Essig's patient experienced frequent electric shock between filling . Manning reported tissue structure damage where a gold metallic clasp surrounded another tooth containing a silver filling.
TABLE 2.
Sex Age Restor Ca P Mg B Sn Cu Si Oth.
time
1-S Leukoplakia, M 45 14Y XXX XX XXX XX Norm gingival and buccal patches
2-A Early leukoplakia, gingival F 23 8Y XXX XX XXX XX Norm
3-E Leukoplakia, lip M 78 20Y XX XX XX XXX XX Norm
4-S Leukoplakia, XX XX XX XX tongue ulcers, M 50 18Y XXX XXX
XXX XXX XXX XXX Nor gingival
5-O Ulcers, buccal F 50 9Y XXX XXX XXX XXX Nor.
Excess Iron
6-M Ulcers and F 32 10Y XX XX XX XX Nor geographic tongue
A biospectrometric examination of biopsy specimens taken from the mouths of six patients who had ulcers, geographic tongue and leukoplakia revealed that there had been an excessive cataphoresis of calcium, phosphorous, magnesium, tin, copper, silicon and boron, which are electropositive elements commonly used in fillings, etc., cements and dentifrices. (Abnormal amounts only)
Chase, who had given more study to the problem, suggested that every plugged tooth doubtless became a galvanic battery ready for action only when the stimulant of an acid saliva surrounded it.
He, therefore, considered a guttapercha water-tight filling best for the arrest of decay, rather than dissimilar metals
Palmer suggested the possible occurrence of disintegration and of loss of fillings as the results of oral electrolysis (4).
Ewing (1929) suggested that "some metallic compounds used in plates devdop measurable quantities of electricity, which is probably a factor in irritation of oral tissues."
Bloodgood (1929) suggested that now and then a patch of leukoplakia can be produced by irritation of a tooth, especially one with a metallic filling."
Hollander, Hyams, Macdonald, Rattner and others have each published one or more positive cases of oral mucosa lesions caused by dissimilar dental restorations.
Hyams made a meticulous study of orthodontic materials in thirty-three cases and reports in detail histories of three cases that gave positive symptoms of electric irritation. He concludes that, in the light of positive findings of others and his own studies, it is wise to aim for homogeneity in the composition of orthodontic appliances, and to select filling materials which are not likely to set up electrogalvanic currents.
Macdonald has published five cases which he diagnosed galvanic burns from dissimilar metallic reconstructions. Each of his cases was immediately improved or entirely relieved by a replacement with like metal.
Rattner has published one very striking case of burning tongue and other symptoms thoroughly studied at intervals by several physicians over a period of seven years. His patient was given prompt
and permanent relief by a removal of two amalgam fillings and replacement with gold, which was homogeneous with other gold fillings in the mouth.
Soloman and Reinhard have several times sincc 1932 published discussions of possible electrogalvanism in the oral cavity and offer confirmatory experimental proof that the elements of a galvanic battery do exist in a mouth containing electrochemically different metallic restorations.They also agree with a suggestion made by Chase that since every amalgam filling is composed of several electropotentially dissimilar metals, probably each filling constitutes a miniature battery. They further emphasize that an electrical action from dental metals must be classified as a source of chronic irritation, and should be included among the etiological factors of precancerous and cancerous lesions of the buccal cavity.
They recently published an exaustive bibliography and brief review of dental and medical literature in which former physicians and dentists have mentioned or commented on the possibility of galvanism in the oral cavity between dental metals.
In a limited review of this bibliography, we have failed to find wherein prrevious authors have attempted to make an extensive clinical study of this problem. They seem not to have fully appreciated the pathologic significance of chronicity of oral electrolysis.
The subject of electrical potentiality between unlike metallic restorations has also been mentioned by five or six European physicians, though the subject was not given serious consideration until about 1930, when Lippmann, of Leipzig, reported three cases that presented both visible lesions and severe systemic symptoms of metallic poisoning. Two of his patients were wearing highly electropositive upper full dentures of zinc and a lower partial denture of Randolph metal.
Each eventually suffered extreme constitutional symptoms of metallic toxemia with kidney, blood and other disturbances.
As proof of his conclusions, he removed the offending dentures for a period. This gave his patients complete remission of all the former symptoms, after which he re placed the dentures, prompt recurrence of all the previous symptoms resulting.
UlIman (1932) reported nine cases at a joint gathering in Vienna of dentists and physicians. He likewise proved his contentions by experimental removal and replacement of the clashing electrochemical dental metals in several cases.
Freidlander (1932, Hamburg), delivering a postgraduate dental thesis, reported seventy-six cases of visible and other symptoms of electrogalvanism in the mouth from dissimilar metals. Several of her patients submitted to experimental proof of removal and replacement. Her statistical tables show that
56 per cent of her cases having dissimilar restorations were conscious of, or exItibited, oral mucosa injury.
COMMENT
Large statistical tables in clinic cases are cumbersome and tedious, and may reflect any idea about which the author may be overenthusiastic. Therefore, we shall present only a summary of symptoms and lesions found in a careful tabulated study of more than 1OOO adults whose mouths contained two or more dissimilar metals: those having minor subjective symptoms, such as metallic taste, tingling, intermittent sensations of tongue, 69 per cent; electric shocks, prominence of papillary bodies of the tongue, occasional erosions, 33.7 per cent; patches, geographic tongue, ulcers of th buccal or lingual mucosa, 28 per cent; leukoplakia and other precancerous lesions, 6.2 per cent.
One or more of the above-named symptoms may occur concurrently in the same patient, though rarely before several months, and, in most cases, from ten to twenty years after the elements for an electric battery have been completed in their mouth.
In a previous presentation of this subject, the possibility that leukoplakia might be caused by electrical discharges, and its precancerous significance were mentioned, but this type of lesion was not elaborated on. We have since observe many additional cases of leukoplakia, which usually occur nearby or in direct contact with the electropositive prostheses. One patient, first examined four years ago, and who refused to have the prostheses changed, was recently recalled for reexamination. A second patch of leukoplakia has since developed, on the opposite buccal surface, and the original patch now gives all clinical appearance of having become malignant.
Considering that every oral cavity containing dissimilar metallic restorations is a constant potential chronic irritant, the percentage or number of persons who seek the aid of a dentist or physician is surprisingly small.
It is a common and somewhat perplexing observation that in certain cases presenting a relatively high meter reading, there are no visible lesions of electric injury in the mouth; nor are the patients conscious of any appreciable discomfort except perhaps an occasional metallic taste or electric shock when a fork or spoon may complete the circuit between two opposite restorations.
On the other hand, we have observed numerous patients who suffer from metallic taste, burning of the tongue and perhaps erosions of the tongue or patches of leukoplakia on the gingival or buccal mucosa though registering a current of not more than 4 to 10 microamperes.
Admitting that the determination of electrical units generated between dental structures as made by our present instruments of measurement, the microammeter and galvanometer probably are only approximate estimations of the actual current potentiality, we may partially account for this seeming contradiction of ordinary processes of tissue injury.
REPORT OF CASES
CASE 1 (Fig. l.) Mr. H had been wearing an upper aluminum denture many years; with no trouble until three years previously, when a partial vulcanite lower denture with large gold bar was placed.
Immediately, a metallic taste, with puckering and stinging sensations of the tongue and buccal mucosa, was noted. He came in May 18, 1932, because of sore mouth and a patch of grayish proliferating precancerous leukoplakia on the anterior hard palate. The electric measurement was
110 microamperes. The entire aluminum denture revealed evidence of electrolytic disintegratian to marked degree, having several perforations in its base. The upper aluminum denture was discarded and the lower partial denture retained. The mucous patches healed and the leukoplakia began to fade after two weeks. At the end of four months, the leukopiakia had undergone almost complete resolution. A new upper denture of vulcanite was made, which the patient has since worn with comfort, The general health has improved and the mouth has remained healthy during the past four years.
CASE 2 (Fig. 2). Mrs. C came in July 1935 complaining of a congenitally furrowed tongue which was easily irritated. She had had a total of eight silver fillings (no gold) placed by dentists in various
large cities during the past eight years. During the past three or four years, she had had a metallic taste, nerve shock and intermittent erosion and ulcer of the tongue. She had become extremely nervous, with loss of appetite and weight and resorted to occasional doses of narcotics in order to secure rest. Wellknown internists in several of the larger cities had made gastric analyses and prescribed diets, medicines, rest, etc., which gave only partial relief. On examitiation, from 10 to 40 microamperes was registered between various and different colored silver amalgams. July 6, all fillings were removed, marked relief beginning within a few hours. Six days later, the tongue and other mucous lesions had entirely healed. As the general condition had improved, all cavities were refilled with high-grade gold. The patient was reexamined Feb. 28, l93& She has had no recurrence and has continued to improve, and is now enjoying perfect health.
CASE 3 (Fig. 3). Miss M (Case 6, Table 2) Came in Jan. 9, 1936. Restorations of two gold crowns and two or thre silver fillings had been made ten years previously. Soon afterwards, a metallic taste caused minor discomfort. Three years previously, three or four additional silver fillings were placed in molars. Increase in the sensations was noted on the margins of the tongue, with general oral discomfort. Six months previously, two gold bridges had been placed, one above another in the lower jaw. Also, other silver fillings were placed. Immediately, increasing discomfort, erosion, ulcer of the tongue and radiating neuralgic pains through the sympathetic branches of the trigeminal nerve were noted. Denuded-like patches (geographic tongue) began to spread from the margins over the dorsum of the tongue. The patient had now become extremely nervous, with loss of appetite and weight. She was taking 6 grains of amytal at night in order to secure rest. From 16 to 18 microamperes was registered between the prostheses. January 11, all gold was removed, noticeable relief beginning within a few hours. The amytal was discontinued the second night. The ulcers healed in seven days. The geographic patches on the tongue healed in three weeks. The neuralgia slowly subsided. The blood count has improved and there has been a gain in weight. Spectroscopic examination of biopsy specimen taken from the patch on the margin of the tongue, January 22, revealed an excess deposit of copper, tin, magnesium and phosphorus.
SUMMARY AND CONCLUSIONS
1. In every mouth in which there have been placed two or more restorative metals, electrochemically dissimilar, there has been established a galvanic battery, which serves as a chronic irritant.
2. The most important factor in estimating the volume of electric current between various dental alloys is their relationship to each other as determined by the standard electromotive force series of metals.
3. Common symptoms consist of discoloration, erosion and disintegration of metals used in restorations; metallic taste, ulcers and geographic tongue; with tingling and occasional electric shocks when dissimilar prostheses come in contact with each other.
4. Systemic symptoms or visible lesions depend on many conditions, such as duration of the current, the presence of certain diseases and infections and counterirritants such as ill fitting prostheses, as well as the use of alcohol and tobacco.
5. The more striking and serious lesions, such as chronic ulcers, leukoplakia and cancers, or the blood dyscrasias may not appear for many months, sometimes ten to twenty-five years after the elements constituting an electric battery have been placed in the mouth.
6. Positive cases of electrolytic injury are promptly relieved by removal of either the positive or the negative metals. There are no recurrences after replacement with restorations which are electrochemically balanced.
7. Quantitative spectroscopic analysis of tissue taken from lesions in the mouth gives positive evidence of ionization and cataphoresis of dental metals and dentifrices.
8. Oral electrolysis can be avoided by testing dental materials in buffered solution outside the mouth before casting into forms for restorations.
9. Electrogalvanism between heterogeneous dental restorations is a serious pathologic problem, demanding early solution and correction through the cooperation of the metallurgist, the dentist and the physician.
1. Lain, E S.: Chemical and Electrolytic Lesions of Mouth Caused by Artificial Dentures, Arch.
Derm. & Syph., 25:21-31 (Jan.) 1932.
2. Lain, E. S.: Electrogalvanic Lesions of Oral Cavity Produced by Metallic Dentures, JAMA.
100:717-720 (March 11) 1933; Electric Phenomena in Oral Cavity, D. Digest, 40:214 (June) 1934.
3. Footnote 2, second reference
4. Palmer, S. B.: Dental Decay and Filling Materials Considered in Their Electrical Relations, Am.
J. D. Sc., 12:105, 1878-1879; Electricity in Mouth, D. Items Int., 10:399-402 (Sept.) 1888; Electro-
Chemical Theory, Am. J. D. Sc 14:166,1880-1881.
5. Chase, H. S.: Filled Teeth as Galvanic Batteries, D. Cosmos, 21:106 (Feb.) 1879; Some
Observations and Experiments Connected with Oral Electricity, Am. J. D. Sc, 12:18-25, 1878-1879.
6. Mayer, Charles: No Battery in Tooth, D. Advertiser, 21:103- 107, 1880. 7. Patrick, J J. R.: Oral
Electricity and New Departure, D. Cosmos, 22:543-546 (Oct.) 1880.
8. Morrison, M. A.: Electric Currents of Oral Cavity, Dominion D. J., 14:86, 1902.
9. Grant, R. C.: Galvanism, Gold, Amalgam and Hahnemanian Theory, D. Digest. 8: 1110-1122
(Dec.) 1902.
10. Davis, C. P.: Electrolysis in Mouth, D. Items Int., 27:694- 695 (Sept.) 1905.
11. Essig, C. J.: American Textbook of Prosthetic Dentistry, Philadelphia: Lea & Febiger, 1896.
12. Hepburn, V. B.: Behavior of Metal Fillings in Mouth, Brit. D. J., 33:1131-1139, 1912.
13. Manning, P. R.: Electrobiologic Theory of Dental Caries, Pac. D. Gaz., 26:335-370, 1916.
14. Ewing, James: Bull. Chicago D. Soc., 9:7 (June 21) 1929.
15. Bloodgood, J. C.: Cancer of Mouth, J.A.D.A., 16:1354 (Aug.) 1929.
16. Hollander, Lester: Galvanic Burns of Oral Mucosa, J.A.M.A., 99:383 (July 30) 1932.
17. Hyams, B. L.: Electrogalvanic Compatibility of Orthodontic Materials, internat. J. Orthodontia,
19:833 (Sept.) 1933.
18. Macdonald, W. J.: Chemical and Electrogalvanic Burns of Tongue, New England J. Med.,
211:585 (Sept. 27) 1934.
19. Rattner, Herbert: Burning Tongue, Arch. Derm. & Syph., 31:701-702 (May) 1935.
20. Solomon, H. A and Reinhard, M. C.: Possibility of Oral Cancerous Lesions from Electrical
Causes, D. Digest, 39:142 (April) 1933; Electric Phenomena from Dental Metals, D. Survey, 9:23
(Dec.) 1933: Electrical Currents from Dental Metals as Etiological Factors in Oral Cancer, Am. J.
Cancer, 22:606-610 (Nov.) 1934.
21. Footnote 5, first reference.
22. Lippmann, A.: Disorders Caused by Electric Discharges in Mouth in Artificial Dentures,
Deutsche med. Wchnschr., 56:1394 (Aug. 15) 1930.
23. Ullmann, Karl: Leukoplakia Caused by Electrogalvanic Current Generated in Oral Cavity, Wien. klin. Wchnschr., 45:84O (July 1) 1932 (abstr.).
24. Freidlander, Ruth: Electrolytic Manifestations in Oral Cavity in Presence of Two or More
Metals, Monat. f. Zahnheilk., August I5, 1932 (ahstr.).
HISTORICAL VIGNETTE:
Calomel and the American Medical Sects During the Nineteenth Century
G. B. Risse
Mayo Clin Proc, Jan 1973, Vol 48
Behold Washington, who had passed through the battles of his country unharmed, and who in his last illness had, in the brief space of twelve hours, ninety ounces of blood drawn from his veins, and in the same space of time taken sixty grains of calomel! (1 grain = 65 mg) Who wonders that he should request his physician to allow him to die in peace?
In a discourse before the Massachusetts Medical Society, Oliver Wendell Holmes issued in 1860 the often quoted verdict: . . I firmly believe that if the whole materia medica, as now used, could be sunk to the bottom of the sea, it would be all the better for mankind, and all the worse for the fishes.
Holmes was reacting strongly to contemporary medical therapy, especially the prevailing overmedication with potentially toxic drugs. In his speech, he chastised American credulity and extravagance in swallowing all these harmful remedies. Zeroing in on the famous physician
Benjamin Rush and his treatments, Holmes sarcastically declared that perhaps since the Declaration of Independence the American people had become convinced that as heroes they could only be satisfied with a heroic medical practice.
The reference to Benjamin Rush as one of the principal proponents of such a "heroic" therapy in
America was appropriate. Rush had popularized such a therapeutic approach during the devastating epidemic of yellow fever which struck Philadelphia in August of 1793. Chaos and confusion reigned at the time regarding the origin and transmission of the disease, to the extent that muskets were discharged from windows and the militia fired salvos with their cannon to purify the supposedly contaminated air.
In the midst of the panic, the local physicians tried all the conventional remedies of the 18th century
- purging and bleeding in moderation, administering cool drinks, producing blisters, and wrapping the body in blankets dipped in vinegar. Yet, despite all these procedures, the death rate from the epidemic increased inexorably, and Rush was impelled to study previous accounts of yellow fever in the hope that they might yield some useful information applicable to the dramatic and frustrating circumstances. These writings stressed the fact that the gastrointestinal tract was filled with putrid and fermenting biliary substances. These poisonous, decomposing humors certainly needed to be eliminated from the body before a cure of yellow fever could be achieved.
Believing that his lack of success was due to insufficient purging of the noxious bile, Rush devised a vigorous purge which contained 15 grains of Jalap, a tuberous root long used as a purgative, and 10 grains of mercurous chloride or calomel. Rush administered this powder in three daily doses, one every 6 waking hours. The effects of the powder exceeded Rushs expectations, since it seemed to cure four out of the first five patients who received it. One of them received a total of 80 grains of calomel. The recovery of this patient, whose funeral had already been arranged, supplied Rush with the first proofs regarding the efficacy of the mercurial purges in the treatment of yellow fever.
The term calomel seems to have been coined in the 17th century (from calos, good, and melas, black), perhaps because its ingestion brought about the expulsion of dark stools containing mercurial sulphides. More characteristic, however, were the greenish stools, obtained after the ingestion of considerable amounts of calomel, a phenomenon erroneously attributed to an increased secretion of bile.
The use of calomel as a cathartic gained favor in the mid-18th century. Benjamin Rushs teacher at
Edinburgh, the famous William Cullen, had recommended its use in his famous materia medica, describing it as a stimulant which could affect every secretory system of the body, from the salivary glands, bowels, and liver to the kidneys. Rushs fellow student, the Scottish physician John Brown, although not mentioning calomel by name, recommended the use of purgative stimulants which were to be used as debilitating agents when the body was in a general state of excessive excitement, a condition which included virtually all febrile illnesses.
The entire rationale behind the use of this mercurial compound, although now included and expressed in the language of the newer stimulation theories imported from Scotland, was an age-old concept, already formulated in ancient Egypt. The primary therapeutic task was to eliminate the highly undesirable materia peccans from the gut. Since the stools were mostly greenish, hope was expressed that in the process of elimination enough bile would be excreted to eliminate the clinical jaundice.
Hence, Rush, with little trust in the so-called healing powers of nature, another trait acquired at
Edinburgh, embarked on his course of vigorous purging with the mercurous chloride. This approach was supplemented by profuse and repeated bleeding. In subsequent yellow fever epidemics in the late 1790s, some of Rushs patients ingested up to three or four doses of calomel daily, each of about
20 grains, for a grand total of 350 to 400 grains over a period of only a few days. Fortunately for many of these patients, the great initial gastrointestinal irritation produced by the yellow fever itself precluded the absorption of the otherwise fatal amounts of mercury.
Nevertheless, the ingestion of calomel produced, in many cases, all the symptoms of acute mercurial poisoning. These toxic effects, notably salivation, were in fact taken for signs that the calomel was having the desired therapeutic effect. The ash gray appearance of the mouth and pharynx, caused by protoplasmic precipitation in the musoca, was common and painful. Within a few days after ingestion, severe stomatitis with excessive salivation appeared. Patients had ulcerated lips, cheeks, and tongue, soreness and inflammation of the gums, plus loosening and frequent loss of teeth. Some unfortunate children died with perforations of their cheeks, buccal gangrene, and osteomyelitis of the maxillary bones.
Generally, there was gastric pain associated with vomiting and gastrointestinal cramps after the ingestion of calomel. In some cases, bloody diarrhea occurred, which was ascribed to the disease rather than as a side-effect of the calomel. The larger doses were considered to have a so-called sedative effect, no doubt because of the more severe systemic consequences of the mercurial poisoning. Nevertheless, Rush apparently had success with his treatment. Calomel was called the
"mercurial antidote" and even the inoculating powder because it was thought to prevent yellow fever just as smallpox inoculation prevented smallpox.
By the end of the 18th century calomel was used in almost every variety of febriIe illness. In 1813,
John Warren, president of the Massachusetts Medical Society, published a book about the mercurial practice in febrile diseases. His thesis was that violent means were sometimes necessary to remove violent diseases. The body's constitution could not, in Warrens view, be influenced simultaneously
by two actions, disease and drug treatment. Calomel was viewed as a potent stimulus entering in competition with other febrile stimuli. The body, unable to be subjected to both of these factors at the same time, was thought to drop the disease, getting rid of its putrid effects through the purgative and diuretic action of the calomel.
Therefore, all infectious diseases could be favorably treated with calomel. Smallpox, measles, diphtheria, hydrocephalus, pneumonia, pleurisy, dysentery, and rheumatism were all attacked by the use of calomel. Further, calomel was also used in intermittent fevers - malaria, cholera, typhoid fever, and the seasonal diarrheas of children. Clearly, the mercurial preparation had acquired the status of a therapeutic panacea in the early decades of the 19th century in America. Appropriately, it was called by some the Samson of the Materia Medica.
Firmly wedded to the prevailing system of medicine, and engulfed in an aura of true rational therapy directly derived from speculative pathology, calomel was thought to be extremely useful, generally used with blood-letting. Thus, in some areas of the South, 100 to 200 grains of calomel were given in one dose to patients with the idea that it is but trifling with the life of a man to give him less of a remedy than his disease calls for, as one southern physician put it.
But the public could not be duped indefinitely. The first rumblings of discontent appeared in the mid
1820s as the use of calomel as a panacea probably reached its zenith. In 1825, a poem appeared in a
Virginia publication depicting the dire consequences of mercury poisoning and urging physicians to quit using calomel:
How'er their patients do complain
Of head, or heart, or nerve, or vein,
Of fever, thirst, or temper fell,
The Medicine still, is Calomel.
Since Calomels become their boast
How many patients have they lost,
How many thousands they make ill,
Of poison, with their Calomel.
Certain physicians, like those trained in the new French clinical school, expressed reservations about the rationale for heroic purging with calomel and the bleeding. If these professionals questioned the contemporary therapeutics, the public in general could hardly be blamed for harboring similar doubts. Thus, it is not surprising to find the public, especially pioneers migrating westward, returning to a brand of domestic medicine which had flourished a century ago.
Faced by a medical profession torn with dissension over medical theories, and still practicing heroic medicine, a crucial gap in health care developed in America which was filled by various groups interested in providing alternative ways of curing people and keeping them healthy. One of these sects was Thomsonianism, founded by a self-appointed healer, Samuel Thomson (1769-1843), who had become disenchanted with orthodox medicine.
In 1822, Thomson declared that: The practice of giving poison as medicine, which is so common among the medical faculty at the present day, is of the utmost importance to the public; and is a subject that I wish to bring home to the serious consideration of the whole body of people of this country, and enforce in the strongest manner on their minds the pernicious consequences that have happened and are daily taking place by reason of giving mercury, arsenic and other deadly poisons to cure diseases.
By contrast, Thomsons method of treatment was based on the use of some herbs which, according to the author, would promote digestion and aid nature. The popularity of such an alternative to the heroic treatment with calomel and bloodletting is attested to by the rapid spread of the Thomsonian system of botanic medicine from its origin in New England. It is estimated that in Ohio alone at least half of the states population adhered to the new therapy based on herbs in 1835, or in other words, a total of four million people preferred the botanic treatments over calomel and other drugs.
The other medical sect to appear in the 1830s was Grahamism, a movement founded by the temperance lecturer from Pennsylvaina, Sylvester Graham (1794-1851). The movement stressed vegetarianism, including whole-wheat products such as the wheat bread and crackers which still carry Grahams name.
In its first volume of 1837, the Graham Journal published the following statement:
To think of the tons and thousands of tons of poisonous medicine in the solid form, and the oceans of liquid poison which are given, and are still being administered. . . . To remember, at the same time, that all this misery, instead of being designated as punishment by a sanguinary Deity, was self inflicted, or at least caused, first or last, by the errors of the race.
While Thomsonianism was stressing botanic therapy, Grahamism emphasized and promoted better hygiene and dietary measures in order to get well. Both became popular substitutes for regular medicine, together with a third sect, which had reached America from Germany and Austria about
1840: hydropathy. This movement also warned people against the toxic drug treatment and suggested the external and internal use of water instead. The movement became extremely popular, especially in the east, by promulgating a hygienic system in many ways similar to Grahamism.
In some medical circles, the use of calomel gradually came under criticism, as evidenced by the speech already quoted of Oliver W. Holmes and that of Samuel Jackson of the University of
Pennsylvania.
In 1844, another physician, T. D. Mitchell of Transylvania University, accused many of his fellow physicians of killing their patients with lethal doses of calomel. Most of those American physicians who had trained in Paris reacted strongly against the widespread belief in medical systems. By implication, they opposed the use of a drug which was supported and dependent on these theoretical speculations. One of them, Elisha Bartlett, professor of medicine at the University of Maryland, wrote of calomel in his famous Essays:
It is constantly administered on all occasions in all diseases and in all their stages. It has, literally, in some instances, been made an article of daily food sprinkled upon buttered bread and mixed with it before baking! I suppose it is no exaggeration to say, that there is more calomel consumed in the valley of the Mississippi and its tributaries than in all the world beside.
But physicians such as Holmes and Bartlett were, to a great extent, lonely voices. The majority of practitioners, especially west of the Appalachian Mountains and in the South, continued using their favorite drug, as evidenced in some of the textbooks.
The fact that calomel was still used rather extensively certainly contributed to the rise of another sect imported from Germany - homeopathy. In the two decades before the Civil War, this mode of healing made great inroads into the medical care of this country. In contrast with the already mentioned more popular medical sects which stressed a do-it-yourself healing and health
maintenance approach, homeopathy emerged in America as a coherent system and practice of medicine.
While orthodox medicine continued to be condemned for flagrantly violating and ignoring nature and its restorative powers, homeopathy boasted a simple, unifying theory of disease. It is true that a fancy theory of disease and a learned and professional attitude may impress patients, at least initially; but if the cures fail miserably, such a varnish of wisdom, as well as pretensions of erudition and certainty, will crumble under the weight of the therapeutic failures. However, homeopathy became a success in America, unequalled anywhere in the world. Among other reasons for this rise was the fact that this sect effectively treated two of the widespread scourges afflicting our land in that period: cholera and typhoid fever.
Rather than the purges with calomel, the large amounts of opium, the bleeding, and the blisters, the homeopathic physicians provided innocuous, high dilutions of some of their mineral and botanic principles. One of these homeopathic practitioners, John Ellis, wrote: The presence of the Asiatic cholera in 1849 in the city of Detroit, and the success which attended the homeopathic treatment of that disease, was instrumental in calling the attention of large numbers of the most intelligent and influential citizens to the new practice and establishing it upon a firm basis.
The abuse of calomel was still widespread during the Civil War, although the concepts and practice of heroic medicine were undergoing gradual change. Thus, by 1863, the Surgeon General of the
Union Army issued a circular forbidding the inclusion of calomel and tartar emetic in the medical supplies for the troops. Hammond's order included a statement on the abuses of calomel by the military surgeons, who had produced many cases of profuse salivation and the apparent occurrence of mercurial ulcerations and gangrene presumably of the buccal and intestinal mucosas.
The medical journals and societies of Ohio were the first ones to vigorously protest the ban of calomel. Not surprisingly, the established physicians felt that calomel was essential to the practice of medicine. It was clear that calomel had truly become the symbol of orthodox medicine, and its ban was viewed as a threat to the prestige and position of the entire profession. As the editor of a
Chicago medical journal stated in 1863, the regular practitioners still looked at calomel as the central sun around which the whole world of medicine revolves.
Physicians in various parts of the country were enraged at the thought that a regular medical doctor, now occupying the highest medical office in the federal service, had taken away one of the most highly prized weapons of their trade. What disturbed them even more was the implication that calomel was both inefficacious and toxic. The ban clearly seemed to vindicate the repeated claims made against calomel by such irregular practitioners as the homeopaths, botanic physicians, the new eclectics, and those magnetic healers roaming through the countryside curing people by laying on hands. The American Medical Association itself accused the Surgeon General of having grossly insulted the medical profession. Needless to say, the opposition of regular medicine to the calomel ban was one of the factors leading to the eventual dismissal of Dr. Hammond.
Physicians, particularly in the South and West, continued to administer calomel in the post-Civil
War decades, generally in high doses. The indications for the drug were cholera, typhoid fever, numerous cases of diarrhea in adults and children, meningitis, mumps, tonsillitis, scurvy, tuberculosis, gout, rheumatism, and many more. Since it was tasteless and did not cause immediate nausea, it was a favorite remedy for children. Toxic manifestations were usually blamed on the manufacturer, for not properly removing the corrosive sublimate or mercuric chloride.
Among the pioneers in the frontier was a man called Andrew Taylor Still (1828- 1917) who lived in northern Missouri where his father was a missionary and physician to the Shawnee Indians in the
1830s and 1840s. As stated in his autobiography, Still was particularly discouraged by the obvious inefficacy of the medical treatment being dispensed, especially for those patients afflicted with the periodic epidemics of cholera, typhoid fever, and smallpox and the endemic problem of malaria. His fear of the heroic but ineffective drug treatments was greatly reinforced during his service in the
Union Army during the Civil War. Still emerged from that conflict determined to establish a new science of healing not based upon the use of all those poisonous drugs.
This belief was greatly reinforced when, in the spring of 1864, Still lost three of his children to an epidemic of spinal meningitis, an event which blatantly exposed the total inefficacy of contemporary therapeutics. Still was later to recall:
When I was about 14 years old I was salivated. I took several doses of calomel. It loosened my teeth.
To day I am using part of a set of store teeth because I lived in a day and generation when people had no more intelligence than to make cinnabar of my jawbone.
Still was to associate the renewed emphasis on the healing powers within the body with the manipulative tradition of domestic medicine still present at the American frontier. Such an assoclation led to the establishment of osteopathy, a healing movenent which Still tried to explain time and again as a genuine form of medical practice which had substituted spinal manipulation and body massage for drugs.
From his writings, there is no doubt that Still believed in the iatrogenic origin of many diseases treated by orthodox medicine. After reviewing a series of heroic drugs, the founder of osteopathy concluded:
We know they will kill, we do not know that they ever cured a single case of sickness, but we know they have slain thousands. . . . Their place is to ruin for life, and osteopathy considers life too precious to place its chances in jeopardy by any means or methods.
When another movement based on the manipulative tradition of domestic medicine appeared in
Davenport, Iowa, in 1894, its founder also stressed his opposition to the orthodox methods of medical treatment, which were dying only slowly in the American hinterland. Daniel David Palmer
(1845-1913), defending his new sect of chiropractic, argued that the use of "heroic" drugs was rapidly becoming a thing of the past and that the value of the drugless methods of curing disease was being widely recognized. Declaring that the human body should be repaired rather than poisoned by drugs, Palmer contended that herbs and minerals - he did not touch on calomel specifically - produced Symptoms which were more severe than the diseases they were expected to cure. He summed up his feelings by stating that:
Doctors who make it a business to administer poison in liquid and solid form, should not continually be warning people against the dangers of drugless healers. . . . People are becoming too intelligent to dose their stomachs for all human ailments; they no longer cater to the whims of drug mongers.
Thus, the initial appeal of both osteopathy and chiropractic was their promise of healing the sick without the use of heroic medicines. They both stressed the decline of the drugging profession, as they called regular medicine, and strongly advertised the abandonment of drugs for treatment.
At about the same time, another selfstyled healer denounced the prevailing cures without mentioning calomel. In her main work, Science and Health, Mrs. Mary Baker Eddy questioned, in 1875, whether the contemporary materia medica was a science or a bundle of speculative human theories. She
realized that any beneficial action of these drugs was merely psychological and closely related to the patients individual faith in their healing power. Recognizing that Thomsonianism, hydropathy, and homeopathy had contributed to a decrease in "drugging", Mrs. Baker viewed Christian Science as the ultimate drugless approach which went beyond the highest homeopathic dilutions and clearly became pure spiritual healing.
To summarize, then, the use of a potentially toxic mercurial compound, calomel, has been presented.
Because of Rushs prestige and his dramatic cures during the yellow fever epidemics, the drug was employed in an everwidening range of diseases until it reached the status of a true panacea. Calomel was included in the medical systems both as a purgative for those believing in bad humors, and a stimulant for the physicians who speculated about a pathology based on the solid parts of the organism. Thus, the calomel ingestion became a rational therapy, a form of treatment based on the genuine knowledge of health and disease. It became the distinctive sign of rational physicians to use calomel as opposed to the ministrations of irregular empirics or quacks. However, the lack of pharmacologic knowledge and controlled studies easily led to abuses. The only way for practitioners to ascertain the effects of calomel was to increase the dosage until the symptoms of acute mercurial toxicity became apparent. Although there were many other medical, socioeconomic, and cultural factors responsible for the rise of sectarian movements, few received as much publicity and explicit criticism as did calomel. Through their attacks on this drug, the various American medical sects effectively bolstered their popularity with the public by emphasizing their therapeutic superiority over orthodox medicine.
Once the administration of calomel, the "Samson in the Materia Medica" had become the trademark of rational medicine, its removal from the therapeutic armamentarium became very difficult. Until late into the 19th century, and even at the beginning of our own time, physicians remained devoted to a drug which reflected their superior rational healing art. In spite of the uselessness and, in the case of calomel, the inherent toxicity of the drug, many practitioners continued to stubbornly use the medication until the growth of experimental therapeutics.
Yet, in the face of this so-called rational medical practice, the American public expressed in most unmistakable terms their disapproval. For almost a century, the popular loss of confidence in medicine created tremendous obstacles for the regular profession.
ACRODYNIA OR HOW TO FAIL TO RECOGNIZE MERCURY POISONING FOR MORE
THAN 100 YEARS
Mats Hanson
How many physicians have heard the story of how medical science eradicated the disease called acrodynia? Very few probably since the discovery and cessation of a major posoning is hardly anything to be proud of. However, medical science ought to learn an important lesson from a disease which cost numerous children's lives - completely unnecessarily. Unfortunately the sentence under mercury in Casarett & Doull's Toxicology seems to be true: Man is apparently a poor student of history.
__________________
Anyone who has experienced the toxic effects of amalgam fillings and has compared the symptoms with those reported in the mercury literature, is amazed that the poisoning has not been recognized at any of numerous visits to doctors during years or decades. The oral symptoms (salivation, ulcers, metallic taste, bleeding gingiva and general irritation of mouth and upper airways) directly indicate mercury poisoning and in addition there are usually numerous other typical symptoms: psychic, neurologic, gastrointestinal etc.
Damage from medicines is called iatrogenic and it is certainly not an easy task to bring dentists to admit that a practice they thought was beneficial for the patients in reality caused damage. It appears to be even harder to get the medical profession to recognize that numerous patients with symptoms indicating anyone of a number of disaeses are mercury poisoned.
The problem is certainly not new, especially not regarding mercury. The metal and its chemical compounds have been used widely; in numerous medicines, for disinfection, electrical apparatus, thermometers and barometers, photographic purposes, toys, cosmetic preparations, paints etc. There are several cases described where children have played with mercury and distributed the metal at home.
The ignorance is still baffling. In a recent electronic magazine I found a description of experiments with lasers to produce holographic pictures. The hologram was obtained by having the laser beam reflected from a drop of mercury towards the object to be photographed and a film. "The drop of mercury can be obtained from a broken thermometer... The high voltage is directly life- threatening to touch and looking into the laser beam can give irreversible eye damage." Not a word about mercury giving off toxic vapor, especially if heated by a beam of light.
CALOMEL
A mercury compound which was earlier much in use was calomel, monovalent mercury chloride
(mercurous chloride), Hg2Cl2. The substance which has a low solubility, was considered harmless despite a large number of reported cases of poisoning. It was commonly used as a medicine for gastrointestinal irritation. A large dose caused diarrhoea and the patient got rid of both the medicine and the possible problem-causing bacteria. However, an apparently common practice was to take much smaller doses which made the medicine pass the gastrointestinal tract slowly, allowing time for absorption. There have been cases of severe brain degeneration after several years of calomel use
(dementia, erethism, colitis and renal failure) (Davis et al, 1974)
Calomel was, however, used in many preparations, often without any indication on the label of the calomel content. A popular use was as worm-chocholate against intestinal parasites. Another use, mainly in english-speaking countries, was to treat irritation when the teeth of small children broke through with teething- powder, containing calomel. "wherever the British flag waved, teething powders were almost a nutritient of infants." According to several early publications calomel had sedative properties and that might have added to its popularity (Bayles, 1879, Hatchett, 1884). The powder was sold in groceries and drug-stores. One of the manufacturers in England reported in 1954 that 30 million packages were sold each year. Studies showed that about 50% of all british mothers used such powders to treat their children.
In Sweden and on the european continent teething powders were little used but instead calomel in worm-chocholate, a variety of mercury compounds, in medicines made up at pharmacies and in chemical-technical preparations, e.g. "germicidal soaps", 5 grams of mercuric chloride in the bathtub for eczema etc. Everyone has been exposed to mercury in vaccines and other preparations.
Absorption and side effects from calomel treatment of children should have been anticipated from earlier experience, early warning were not lacking, eg. Cruickshank, W., Remarks on the absorption of calomel from the internal surface of the mouth; accompanied with a preliminary sketch of the history and principal doctrines of absorption in human bodies. London 1779; And what happened to
the children's teeth after mercury exposure? Hutchinson J., On the malformation of the teeth, caused by giving mercury to infants (Edinburgh Med J 1897). Warkany (1966) cites Underwood (1865) who suspected the harmless calomel, prescribed in small amounts, as the villain that caused ptyalism, ulceration of the gums, sloughing of the palate, and falling out of the teeth. He knew of several such cases which resulted in the death of the patient.
ACRODYNIA
What were the consequences of this human mercury impregnantion? What are the consequences of mercury exposure from amalgam today? A clue to the magnitude of the problems caused by mercury might be obtained by studying the medical records of the disease called acrodynia. This is quite rewarding since there are careful descriptions from both before and after the mercury etiology was recognized. Even the psychosomatization was not missing. Spitz and Wolf (1946) described under the title "Anaclitic depression" a syndrome among children in a nursery (5-11 months of age).
Several of the children died and arrested development was noted in others. The authors considered the illness to be comparable to melancholia in the adult and caused by "withdrawal of the love object". The psychic diagnosis is discussed (and rejected) in a review paper by Leys (1950) where these cases were considered typical of acrodynia.
The first appearance, at least in a sufficient number of cases to be recognized as something special, was in a building-block at rue del'Orsay in Paris in sept. 1828. In the house a number of children but also adults fell ill. An infectious agent was suspected. The epidemic was described in medical journals and subsequently cases were reported from other places, often isolated cases among children but sometimes groups of children and also adults were affected. Epidemics from prisons and military camps were reported.
The disease spread during the 19th century and at the end of the century it had spread to large parts of the world; In England, Australia, the southern USA and other english-speaking countries mainly children below 2 years of age were affected. The peak was at 9 months of age. On the continent the peak was at 2 1/2 years and continued up to 9 years. In England 585 deaths because of acrodynia were officially registered between 1939 and 1948. In the year 1952-3, acrodynia cases constituted
3.6 % of all visits to the children hospital in a british city. In Australia the disease had epidemic forms. The responsible virus was discussed and its mode of transmission from person to person.
Epidemics could occur in isolated, rural areas. The cause was unknown.
SYMPTOMS
The disease had other names besides acrodynia. Because of the swollen, painful hands and feet with peeling skin and a reddish color, it was called pink disease. Skin problems in other parts of the body was also common. After physicians who described various features, it was also called Feer's disease,
Selter's disease and Swift's disease. More symptom-describing was erythema arthriticum epidemicum, vegetative neurosis of childhood, vegetativ encephalitis, erythroderma polyneuritis, throphodermatoneurosis, primary emotional disorder. A physician wrote: ".. it is difficult to imagine anything more pathetic than a baby suffering from pink disease with complete apathy and loss of interest in his his surroundings."
The children had pains in hands and feet and these were often swollen, damp, sensitive to touch and felt cold. Demyelination was noted in nerve biopsies. There were disturbances of blood circulation and temperature regulation; in severe cases fingers and toes could be lost by gangrene. Blood pressure and catecholamine levels were often high. The victims exhibited extreme weakness of muscles; they usually stopped standing and walking. Loss of weight, tremor and shaking, cramps and uncontrolled movements, abdominal tenderness and gastrointestinal troubles belonged to the clinical picture. Also conjuctivitis and fever was reported in earlier descriptions; fever was apparently very common in Germany and Switzerland where the most common misdiagnosis was scarlet fever. In a considerable number of cases there was salivation, swollen gingiva, loss of teeth and necrosis of the jaws.
WHAT CAUSED THE DISEASE?
Guesses were numerous. Vitamin deficiency, neurosis, endocrine disturbance, adrenal insufficiency, electrolyte imbalance, allergy, hysteria, trikinosis, rye fungus. The similarity to pellagra (vitamin B3deficiency) was pointed out several times. There were studies to assess possible contacts with animals; unknown viruses and a variety of microorganisms were suspected.
The similarity to arsenic poisoning was noted in 1889. Mercury poisoning and the similarity in symptomatology to effects of mercury treatments with grey ointment was first suggested in 1846 and again in 1922. A physician wrote that year " For a while I had the idea that it could be a metal poisoning. Several of my patients had been treated with large doses of calomel at the onset of the disease. There were, however, cases where no calomel treatment could be found and this drug could be eliminated."
Why did he think about mercury? The reason was the oral changes. "A symptom which is almost unknown in every disease except poisoning with mercury or phosphorous." In the USA the idea of poisoning also appeared. Bilderback described a number of cases 1920 and noted that the disease " was more like a low-grade poisoning or a deficiency disaese than an infection. The children were, however, well-fed. low-grade toxemia remained."
In 1945 an americal physician, Warkany, got the idea to send an urine sample to a laboratory for metal analysis because of the similarity with arsenic and thallium poisonings. The urine contained
360 micrograms Hg per liter and no other metals. Additional measurements demonstrated mercury in most urine samples, however not in all. Careful studies showed mercury exposure in every case, most often from teething powders. Warkany wrote that "its seems rather odd that one could not detect the injurious mercury at the entrance of the alimentary canal, whereas it could be demonstrated at the end of the urinary tract." The onset of disease could be delayed weeks to months after the mercury exposure. There were also cases of typical, acute, poisonings, immediately or after weeks followed by acrodynia (suggesting the involvement of immune reactions).
Often the exposure to mercury could be difficult to find. In a series of 40 patients 19 had been exposed to calomel in teething powders, 6 as other types of tablets or powders and 7 worm- medicine. Four cases had been exposed to ammoniated mercury for skin treatment and 3 cases had been exposed to mercuric chloride after washing diapers in sublimate solution. Another case had been exposed to mercuric iodide. Broken barometers, sublimate- impregnated wood, paint and recently broken fluorescent lamps have been other sources of exposure.
The mercury etiology was doubted since many children had high mercury levels in urine without showing the symptoms of acrodynia. An estimate indicated that about one child of 500 exposed developed acrodynia. There was never any study if there were any other signs of disease or if mercury-exposed children got other diagnoses if the symptoms were different from those usually connected with pink disease.
CALOMEL FORBIDDEN - ACRODYNIA DISAPPEARED
The sale of calomel powders was forbidden or restricted in several countries, first in Australia. The epidemics quickly disappeared. USA followed but in England the disease continued since the mercury etiology was slow to be accepted. In USA the FDA had attempted to remove calomelcontaining teething powders as early as 1931. In England a court case got the preparations off the market in 1953. Still sporadic cases are reported from various parts of the world, always in association with mercury exposures. Warkany pointed out that the disease disappeared without any acrodynia-foundation, no parent support group, no research money and in silence.
One of the most interesting aspects of acrodynia is the immunologic/allergic connection. This was noted very early, long before mercury was found to be the causative factor. In 1927, Helmick wrote:
"Referring to the nervous symptoms, we are immediately impressed with the similarity to that typifying an allergy." Other symptoms led the author to the same conclusion. Baumann (1949) distinguished several types of "hypersensitivity" reactions to mercury:
A. Acute Hg-allergy
1. Reaction after external Hg-application (Hg-ointments,
mercurochrome etc) a/ local dermatitis
b/ generalized exantheme and dermatites with or without
fewer
2. Reactions after internal Hg-uptake
a/ acute calomel disease
b/ acute calomel disease with subacute progression
(erythrodermia, chronic pigmentation) and sometimes
complications (meningoencephalitis, anaphylactic
purpura, lipoid nephrosis etc)
c/ Hg-disease by amalgam fillings
B. Subacute allergic disease (late reaction following external
and internal Hg-medication
1. Neuroallergic reactions
a/ Syndrome of acrodynia of childhood
b/ Polyradiculo-encephalitic syndrome
2. Agranulocytosis
3. Lipoid nephrosis after overdosed worm-treatments
It is interesting to note that Guillain-Barre' syndrome also occurred as a complication of acrodynia
(ref. in Warkany, 1953).
It was also noted that acrodynic reactions in exceptional cases could be precipitated by arsenic, gold and thallium. Some children developed acrodynia after vaccinations. The mercury content of vaccines was noted but the number of certain cases was too low to draw definite conclusions. In
Sweden we have noted severe reactions in both children and adults after vaccinations with mercury, especially if the mother has been exposed to mercury during pregnancy (having fillings placed or removed, female dentists and dental assistants)
Fanconi et.al. (1947) tested several acrodynic children with patch tests with various mercury compounds. The children were seldom positive. In some cases a positive reaction (local reaction) was present at the peak of the disease and absent a few weeks later. It was also observed in isolated patients that a skin area (on the back) where nothing was seen at the time of testing, suddenly flared up when the child accidentaly got another worm-treatment with swallowed calomel. Patch testing could also induce systemic reactions. Certainly these observations cast serious doubts about the value of skin tests for mercury and the ADA assumption that only a negligable fraction of the population is allergic to mercury, based on useless tests. A more true statement would be that only a small fraction of the population can not tolerate amalgam on the skin without local allergic reaction.
The sometimes severe neuroallergic reactions in acrodynia and his own observations on neurologic patients, led Baash (1966) to the conclusion that multiple sclerosis was an adult form of acrodynia, a neuroallergic reaction, in most cases caused by mercury from amalgam fillings. The hypothesis seems to be a perfectly logical one which can explain every puzzling feature of MS. Our experience in the patient organization certainly verifies Baasch observations. Apparently Baasch had contact with Fanconi, one of the first researchers to adopt and clarify the mercury etiology of acrodynia.
Pseudo-acrodynia with some features of the real disease was produced in animals by various treatments. Today relapsing allergic encephalomyelits is produced in animals by injection of brain tissue and is considered a model for MS. However, a much more rewarding approach would be to look at the role of mercury. It might then turn out that exactly the same happens as with acrodynia.
"A subtle, complicated, and no doubt molecular disease was eradicated by such a prosaic measure as removing calomel from oldfashioned teething powders and worm medicines." (Warkany, 1966).
"There were data on electrolyte changes explaining the symptoms of acrodynia and their alleviation by subtle saline treatments. But these data did not take into account the one electrolyte that mattered, namely mercury." (Warkany, 1966).
Literature:
Baasch, E. Theoretische Ueberlegungen zur Aetiologie der Sclerosis multiplex. Die Multiple
Sklerose eine quecksilberallergie? Schw. Arch. Neurol. Neurochir. Psychiat. 98, 1966, 1-18
Baumann, T. Calomel-Krankheiten, Schw. Med. Wochenschr. 79, 1949, 725-730
Bayles, G. Sedative action of calomel, Med. Rec. N.Y. XV, 1879, 453
Cruickshank, W., Remarks on the absorption of calomel from the internal surface of the mouth; accompanied with a preliminary sketch of the history and principal doctrines of absorption in human bodies. London 1779
Davis LE, Wands, JR, Weiss SA, Price DL & Girling EF Central nervous system intoxication from mercurous chloride laxatives Arch Neurol 30 1974 428-431.
Fanconi, G., Botsztejn, A. & Schenker, P.
Ueberempfindlichkeitsreaktionen auf Quecksilbermedikation im Kindesalter mit besonderer
Berucksichtigung der Calomelkrankheit Helv. Paediatr. Acta 2, suppl 4, 1947, 3-46
Hatchett, R.J.H. Calomel, an instantaneous nervous sedative, South. Clin. Richmond VII, 1884, 97
Helmick, A.G. Symptomatology of acrodynia as a basis for a new line of investigation as to its etiology, Arch. Pediatr. 44, 1927, 405-410
Hutchinson J., On the malformation of the teeth, caused by giving mercury to infants Edinburgh
Med J 1897 n.s. i 119-121.
Leys, D. A review of infantile acrodynia (Pink Disease). Arch. Dis. Childh. 25, 1950, 302-310
Spitz, R.A & Wolf, K.M. cited in Leys, D. 1950
Underwood, A.L. Mercurial gangrene, Cincinnati Lancet and Observer 8, 1865, 585
Warkany, J. Acrodynia and mercury, J. Pediatr. 42, 1953, 365
Warkany, J. Acrodynia - Postmortem of a disease Amer. J. Dis. Child. 112, 1966, 147-156
The papers by Warkany are highly interesting and recommended. They also contain many further references.