Background
advertisement

Characterisation of discriminant rheumatoid arthritis (RA) fibroblastlike synoviocytes antigenic target in RA patients.
E Solau-Gervais1, D Lefranc2, C Dupont1, V Dutoit2, J Dewailly1, C Fontaine3, S Dubucquoi2. RM
Flipo1, L Prin2,
A mettre dans l’ordre souhaité
Department of Rheumatology (1), Immunology (2) and Orthopaedics surgery (3)
Lille University Hospital, FRANCE
Correspondence and reprints:
E Solau-Gervais
Department of Rheumatology,
Hôpital La milétrie, CHU Poitiers
86000 Poitiers, FRANCE
Tel.: +(33) 549 444 370
1
Abstract
Objective: Synovitis which is a major characteristic of the rheumatoid arthritis (RA) disease, is a
consequence of synovial membrane (SM) hypertrophy, resulting from the hyperplasia of fibroblasts like
synoviocytes (FLS). Also, it seems of interest to study reactivity against the proteins of the RA SM or
RA FLS. This study was undertaken to compare the reactivity patterns displayed in RA and healthy sera
against FLS proteins.
Materials and methods: Serum IgG response patterns in patients with RA (n=46) and healthy subjects
(n=16) were compared after exposure to protein extracts of human FLS obtained from RA Synovial
membranes. To determine IgG antibody responses, post-exposure sera were analysed by Western
blotting technique and the data obtained were then further evaluated using Linear Discriminant Analysis
(LDA). Protein identification was successively performed by 1-D and two-dimensional (2-D)
immunoblottings, followed by mass spectrometry (MS) analysis and a database search.
Results: When sera IgG responses were evaluated on a RA FLS, Chi2 analysis allowed us to distinguish
IgG specific reactivities towards five antigenic targets specifically linked to RA disease. LDA allowed
us to identify a cluster of discriminant set of immune reactivities towards putative targets which
distinguished RA subjects from healthy subjects with a sensitivity of 89% and a specificity of 93 %.
Fourty spots were successfully matched with 2-D Coomassie blue stained gels leading to the
identification of 3 proteins (BiP, lamin A/C and annexin 11) of the 5 discriminant antigens.
Conclusion: In this study we highlight the existence of discriminant serum IgG profile against RA FLS
in RA patients compared to healthy subjects and suggest the interest of a combination of IgG response
against a cluster of antigen to improve the diagnosis sensitivity of RA.
2
Introduction
Rheumatoid arthritis (RA) is a chronic systemic disease characterised by inflammation of the joints and
the destruction of cartilage and bone. Although RA can affect all peripheral joints – with the exception
of distal interphalangeal joints, erosions tend to occur earlier in the wrists, hands and feet than in knees
or hips 1. Clinically, synovitis is a major characteristic of the RA disease. Synovitis is a consequence of
synovial membrane (SM) hypertrophy resulting from the hyperplasia of fibroblasts like synoviocytes
(FLS) and the infiltration of T cells and macrophages2 involved in inappropriate and chronic
inflammatory responses. The efficiency of anti-CD20 therapy3 4 and the presence of rheumatoid factor
(RF) and anti-citrullinated peptide antibodies such as filaggrin5, fibrin6 or vimentin7 in RA patients, also
underline the potential role of B lymphocytes in the physiopathology of RA8. Nevertheless, even though
the presence of RF and anti-citrullinated protein (anti-CCP) antibodies are required for the diagnosis of
RA, almost 50% of patients in the early stages of the disease have negative RF and anti-CCP
antibodies5. As such, several other antigens (collagen9, heat shock protein10) have been proposed as
putative targets. Serological proteomic approaches (SERPA) have been recently used to identify new
immunogenic targets recognized by serum IgG. Using fresh human placenta as a substrate,
enolase11 was found to be a discriminant target in very early RA. Using chondrosarcoma cells, a
human stress protein, BiP (immunoglobulin binding protein), was also identified as a putative antigen12
13
. In these two studies only 24.8% of RA sera recognized the 50 kDa
11
band and 30% of RA
patients possessed serum autoantibodies to Bip {Corrigall, 2001 #25}. Consequently, neither of these
antigens has definitively been implicated in the pathophysiology of RA and it seems that a spectrum of
reactivity rather than one reactivity is implicated for RA diagnosis and could be also involved in the
chronically immune destructive process of RA.
By testing distinct human tissue targets, consensual immune patterns of self recognition, named
immunological homunculus, have been demonstrated in healthy subjects14 15. In multiple sclerosis (MS),
we have found discriminant immune patterns compared to healthy subjects that distinguished the IgG
responses towards self antigens derived from healthy or MS brain homogenates from healthy subjects16.
3
Using a large panel of antigens from fibroblast-like synoviocytes (FLS) cultured from synovial
membranes, we compared here by immunoblotting, the serum IgG repertoires from patients with
rheumatoid arthritis and healthy subjects. Our analysis lead to the identification of discriminant self IgG
reactivity when RA sera were compared to healthy sera against RA FLS. In addition to protein
previously described as potent targets of antibodies present in RA sera, our results emphasizes a
targeting on a new protein, lamin A/C, which belongs to the intermediate filament family.
4
Materials and methods
Patients:
Sera were obtained from 62 patients and kept frozen at -80°C until used. Forty six patients were
diagnosed with clinically definite RA according to ACR criteria17. Sera from 16 healthy subjects were
tested as normal controls. All patients were followed up in the Department of Rheumatology. Table I
summarizes the epidemiological characteristics of patients with RA.
The synovial samples were obtained from other RA patients after synovectomy or arthroplasty. All of
these patients had been diagnosed with clinically definite RA according to ACR criteria17. Wrist and
finger synovial membranes (SM) were obtained after synovectomy. Elbow, knee and hip SM were
obtained after arthroplasty. All subjects had given their written informed consent.
Cell isolation and culture:
Synovial membranes were minced with scissors and digested with Dulbecco's modified Eagle's minimal
essential medium (DMEM) (Sigma, Poole, UK) with 600 U/ml of collagenase type XI (Sigma, Poole,
UK) for 90 mn at 37°C. Cells were washed in DMEM with 10 % foetal calf serum (FCS) (SeraLabHarlan, CrawleyDown, UK) and seeded into 25 cm2 tissue cultured flasks. Confluent cultures of
adherent fibroblasts like synoviocytes (FLS) were passaged at 1:2 ratio in 150 cm 2 flasks. Cells were
detached from the flasks with 0,25% trypsin (Life Technologies, Paisley, Scotland). The cells used
during the study were limited to between passage 3-8. FLS were cultured in DMEM supplemented with
10% FCS.
Rheumatoid factor and anti-cyclic citrullinated antibody
IgM rheumatoid factors (BMD, Marne la Vallée, Paris) and anti-cyclic citrullinated antibodies (Inova,
San Diego, USA) were measured by Elisa, using commercially available tests and following
manufacturers’ instructions.
5
SDS-PAGE
The FLS cells were homogenized in Laemmli buffer and heated at 95°C for 10 min. Eighty (80) l of
this lysate was loaded per well onto a 10 to 20% gradient polyacrylamide gel beside a molecular mass
marker (Amersham Pharmacia Biotech). Just before electrophoresis, the homogenates were reduced
with 10 mM DTT (Sigma-Aldrich). Electrophoresis was performed for 12 hours in Tris/glycine buffer at
100 V.
Blotting and analysis procedures
Proteins were transferred onto 0.45-m PVDF membranes (GE healthcare) at 0.8 mA/cm2 and later
saturated with 5% non-fat dried milk. Each well was cut into 30 strips, 3-4 mm wide. Western blotting
was conducted with total sera, diluted 1/100 in TBS (100 mM Tris (pH 8.0), 0.3 M NaCl) containing
0.5% Tween 20 (w/v) and 5% non-fat dried milk. After incubation for 1 night at 4°C, the IgG Abs were
revealed with an anti-human FcHRP-conjugated Ab (1/10,000; Sigma-Aldrich). Fluorograms were
prepared using an ECL kit (Amersham Pharmacia Biotech). Densitometric analyses were performed on
nonsaturated autoradiographs using the Quantity One software (Bio-Rad, Hercules, CA) apparatus to
localize and compare the IgG immune profile patterns. The Ab reactivities were superimposed and
aligned using Diversity database 2.2 software (Bio-Rad). Immune profiles were analysed when two
independent assays had produced identical patterns.
Statistical analysis
The data were expressed in binary mode (0 = absence of reactivity against antigenic band; 1 = presence
of reactivity against antigenic band) so that IgG Ab patterns could be analysed using either the Chi2 or
Fisher’s exact test. This approach allowed us to select the most relevant band showing qualitatively
different immune recognition patterns between healthy subjects and RA. In a second phase, linear
discriminant analysis (LDA) was used to balance the discriminating Ags between the populations of
individuals. All Ags with a p value < 0.05 in the previously mentioned statistical tests were selected for
6
LDA 18. Using a stepwise logistic regression model, and supported by the LDA method, we were able to
isolate a subgroup of SM Ags on the basis of their power to discriminate between the different
populations involved in the study. On the basis of the presence (x 1) or absence (x 0) of each selected
Ag, and the coefficient previously defined by LDA, a score was calculated for each subject as a
representative value of the individual immune profile, using the following formula: score = Ag1 coef1 x
(0(absent) or 1(present)) + Ag2coef2 x (0(absent) or 1(present)) + Ag3coef3. . . . Initially, the analysis
focused on discriminating between RA patients and healthy subjects. Threshold values were determined
using a receiver operating characteristic (ROC) curve. A test was used to evaluate concordance with
clinical data.
Bidimensionnal electrophoresis
The FLS were lysed in buffer (7M urea, 2M thiourea (sigma), 50 mM C7BzO (Calbiochem), 4% triton
100X (sigma), 1X anti-protease (Roche), and 1% DTT (Sigma)). Following incubation at room
temperature for 1 hour under shaking, the cell lysate was then centrifuged at 20000g for 20 min at 4°C,
and the supernatant was recovered. The protein concentration was measured by 2D-QUANT KIT (GE
Healthcare).
Immuno-electro-focalisation (IEF) was performed with an IPGphor III (GE) using precast 18 cm pH 310 linear IPG gel strips (GE). Equal amounts (1 mg) of total proteins were mixed with rehydration
solution to a total volume of 300 µL with 2% v/v pharmalytes pH 3-10 (GE). Sample load was realized
by in-gel rehydratation and IEF was performed at 150 V for 1 h; 300 V for 1 h; 1000 V for 1 h; and
7500 V for 10h. The current was limited to 50 µA per gel strip. After IEF separation, the IPG strips were
stored at -70°C until further use or immediately equilibrated in equilibrium buffer (50 mM tris-HCl, pH
8.8, 6M urea, 30% v/v glycerol, 5% w/v SDS), and 2.5% w/v DTT for 2x10 min then including 2.5%
w/v iodoacetamine for 1x10 min. Equilibrated IPGs were transferred to a polyacrylamide gradient gel (T
= 9–16%) containing bis-acrylamide (C = 2.6%). Electrophoresis was performed using a Protean II xi 2D cell (Bio-Rad). 90V applied until the front line of bromophenol blue reached the bottom of the gel.
7
For Western blotting, gels were electroblotted onto PVDF membranes (GE Healthcare) and treated as
described earlier.
For MALDI-TOF MS analysis of proteins, gels were fixed with 50% v/v ethanol, 3% v/v
orthophosphoric acid for 2h. After 3 washes in distilled water, the gels were stained with Coomassie
brillant blue G-250 (Sigma).
In-gel digestion and MALDI-TOF MS analysis
Excised plugs from CBB-stained gels, were destained with 200 mL 50% ACN in 10 mM NH4HCO3
and dried in a SpeedVac concentrator. Protein was digested overnight at 377C with sequencing-grade
trypsin (5 mg/mL; Promega Madison, WI, USA) in 50 mM NH4HCO3. The resulting peptides were
extracted twice with 25 mL 50% ACN/ 0.1% TFA. The collected extracts were lyophilized, and were
resuspended in 10 mL 0.1% TFA and desalted on ZipTip C18-microcolumns (Millipore, Bedford, MA,
USA). Elution was performed with CHCA (5 mg/mL) directly onto the MALDI target (2 mL of the
solution was applied to a plated sample holder and introduced into the mass spectrometer after drying).
MALDI-TOF MS was used to obtain PMF for proteins using a Voyager DE-STR instrument (Applied
Biosystems, Framingham, MA, USA). Ions were accelerated at 20 kV and reflected at 21.3 kV. Spectra
were acquired in the delayed extraction, reflectron R mode. Scans (100–300) were averaged to produce
final spectra. Spectra were externally calibrated using the monoisotopic MH1 ion from three peptide
standards (trypsin autodigestion products: 842.510, 1045.564 and 2211.1046 Da).
Database search based on PMF spectra
The obtained peptide mass fingerprints spectra were analyzed by searching the National Centre for
Biotechnology
Information,
nonredundant
protein
database
with
ProFound
(http://prowl.rockefeller.edu/cgi-bin/Pro Found), Version 3.2. The parameters for each search were
varied in order to achieve the best possible results. The standard parameters were as follow: Homo
sapiens, 0–250 kDa Mr (depending on the region where the spot occurred in the gel), tryptic digest with
8
a maximum number of one missed cleavage. Peptide masses were stated to be monoisotopic, and
methionine residues were assumed to be partially oxidised. The identity of proteins was annoted using
the Swiss-Prot and TrEMBL databases.
9
Results
Selection of antigenic targets:
In a first step, we analyzed the self IgG response against RA synovial membranes (RA SMs) by
testing sera from RA patients and healthy subjects. RA SMs from different joints were compared (knees,
hips, fingers and wrists) and different patterns were obtained (data not shown). Wrist and finger RA
SMs appeared as the best tissue targets showing high number of IgG reactivities, even though the
protein concentration and distribution were similar for all lanes (as detailed in material and methods).
Further, comparative studies of self IgG patterns against wrist RA SMs obtained either with healthy sera
or RA sera, revealed inter-individual differences with only some conserved sets of protein bands.
Nevertheless, a higher number of protein bands was always found with RA sera, as illustrated in figure
1. To standardize the technique and as RA synovial membrane was not a homogenous tissue,we have
chosen to use fibroblast-like synoviocytes (FLS) isolated from these RA SMs as antigenic target (RA
FLS).
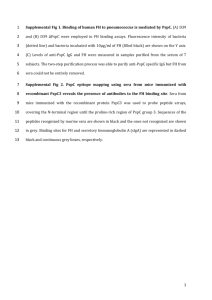
In a second step, self IgG patterns of RA sera were analyzed on RA FLS after 3 to 5 passages. As
shown in figure 2, the bands of reactivity were quite similar in the 3 tested conditions. Nevertheless, the
higher number of protein bands recognized by serum IgG was found with FLS from the 5th passage. All
the following experiments were performed with these targets. RA FLS P5 of different SMs were then
tested (one hip, one finger, two wrists, one ankle and one knee). As shown in figure 3, quite similar
patterns were obtained for each RA serum tested against these different targets (reproducibility>80%).
For calibrating each following experiments using different sources of RA FLS we always tested 3 sera
of reference having previously defined patterns. To acquire information regarding the protein expression
patterns of our RA FLS, total cell lysates were separated on nonlinear immobilized pH gradient strips
(pH 3–10) and fractionated in the second dimension on large-format SDS-PAGE gels. The separated
proteins were visualized by staining with colloidal Coomassie blue (figure 4). 40 spots were excised and
digested in gel with trypsin. The peptides were extracted and analyzed by MALDI mass spectrometry
10
(table 2).
Distinct serum IgG reactivities obtained with control and RA sera:
As previously found with RA SMs, comparative studies of self IgG patterns against RA FLS
obtained with sera collected either from 16 healthy subjects or from 46 RA patients, revealed interindividual differences with some conserved sets of proteins bands. As illustrated in figure 5, a higher
number of protein bands were recognized by IgG from RA sera (p=0,001). Four to 17 bands of
reactivity per strip were found with healthy control sera (median value of 7 bands per subject) when 7 to
24 bands of reactivity per strip were found with RA sera (median value of 15 bands of reactivity per
strip). After the alignment of all the patterns (n=62), 60 distinct protein bands were identified as shown
in table 3. Chi2 analysis and Fisher’s test allowed us to distinguish 13 protein bands specifically related
to RA patients. Among these protein bands, the linear discriminant analysis (LDA) allowed to point out
5 bands named (p19, p26, p30, p33, p37). Coefficient values associated with the presence or the absence
of each IgG reactivity assigned by LDA enabled the calculation of a score for each subject using the
following equation: 0.466 (0/1 p19) + 0.605 (0/1 p26) + 0.629 (0/1 p30) + 0.495 (0/1 p33) + 0.618 (0/1
p37). The results revealed an excellent degree of concordance with clinical data (k=0.93) (Figure 6). A
receiver operating characteristic curve (ROC curve) determined a cut-off at 0.55 and distinguish RA
from healthy subjects with a sensitivity of 89 % and a specificity of 93 % (figure 6). To further
characterize discriminant antigenic targets, a serological proteomic approach (SERPA) was performed.
First, RA sera able to recognize all protein bands previously defined as antigenic candidates in 1-DE,
were selected and used for 2-DE. The presence of multiple antigenic spots has been revealed by 2-DE
followed by immunoblotting assays. The superposition of antigenic spots (figure 7) and protein spots
revealed by a standard colloidal Coomassie blue-stained 2-DE (figure 4) enabled the selection of
proteins for further in-gel digestion and MALDI-TOF analysis. They were matched on a preparative gel
for subsequent characterization with MALDI-TOF as previously described, on the basis of peptide mass
matching. Such an approach allowed us to identify 3 proteins out of 5 discriminant bands (Table 4). The
presence or the absence of at least one of these 3 detected antigens (BiP, Lamin A/C, Annexin A11)
11
distinguishes RA from healthy subjects with a sensitivity of 76% and a specificity of 94% although the
sensitivity of each antigen was comprised between 38 to 48%.
12
Discussion
In this report, we identified in RA sera, peculiar IgG self reactivity directed against tissues or
cells involved in patho-physiology of RA. When RA synovial membranes (SMs) were first tested as
tissue targets, serum IgG reactivity patterns against protein extracts were different in large joints such as
hip and knee, and in small joints such as wrist and hands (data not shown), but higher reactivities were
always found with RA sera. Small joints RA SMs are obtained by synovectomy although hip or knee
joints RA SMs from arthroplasty. Thus, the inflammatory status of the SMs might be more important in
small joints, generating new cryptic or hidden self epitopes available for detection by western blots. For
technical reasons, most of the previous studies used SMs from the knee joints19
20 25 27
, even though
clinically detectable synovitis in RA is essentially present in small joints. The heterogeneous status of
RA SMs and the fact that standardarized techniques are required led us to develop the preparation of RA
FLS. Now FLS are considered as key cells of patho-physiology of RA (36). They proliferate in an
anchorage independent manner {Lafyatis, 1989 #62}, without contact inhibition and express
constitutively cytokines {Ritchlin, 2000 #63}. Although the significance of this phenotypic change
remains uncertain, some data suggest that this may involve resistance to apoptosis (Firentstein, nature,
2003). In addition, the proteomic map of RA FLS revealed a high content of detectable proteins. In
relation to previous data showing the revelance of some proteins targets (bip enolase) 40 spots were then
selected in our study for further characterisation. Twenty six of them were previously described {Dasuri,
2004 #20}. These FLS cellular protein could be classified into several function categories such as
cytoskeletal, metabolic, cell signalling of inflammation. Thus RA FLS appear a relevant source of
antigenic target with rich protein pattenr. RA FLS at different passages were tested to define the most
appropriate condition of culture. When FLS are used in culture, they are usually used between the third
and the eighth passage ({Kasperkovitz, 2005 #61}. The reactivity of a same RA serum has been
compared using RA FLS from the third and the eighth passage (data not shown). Most of the bands of
self IgG reactivities was similar in the different tested conditions but the best results were observed at
13
the fifth passage. In a previous study, freshly isolated FLS have been used {Zimmermann, 2001 #64}.
This approach is not convenient for our study because a large amount of proteins is required to perform
subsequent proteomic and immuno-proteomic analysis. When RA FLS from different joints (hip, knee,
wrist, ankle and finger) were used as potent antigenic targets, no significant difference was found in
term of self IgG reactivities. This can be explained by some evidence indicating that the transformed
phenotype of rheumatoid FLS constitutes stable long-term alterations that are maintained in the absence
of an environmental stimulus (muller-ladner, lehmann).
Peculiar IgG patterns against RA FLS proteins were found when RA sera were compared to
healthy controls sera. A comparative analysis of the 62 patterns obtained with all of the sera studied
showed that despite inter-individual patterns, qualitative and quantitative changes in detected protein
bands allow us to discriminate the two populations. A limited set of conserved bands of reactivity was
noted. It is not related to secondary antibody reactivity. In return, it might be related to the expression of
natural IgG self reactive responses (14) (Mouthon L JI 1995, 154, 5769). Linear discriminant analysis
allows to point out of five discriminant IgG reactivities, with a sensitivity of 89% and a specificity of
93%. While western blotting may not be routinely applicable, this result shows that the specific
diagnosis of RA requires not one but several markers. Serological proteome analysis (SERPA)
approaches have been successfully applied to detect new self antigens, in different diseases. In
neurological autoimmune diseases16, specific immune patterns associated with multiple sclerosis (MS)
but distinct from Sjogren’s disease and healthy subjects was described. In addition three different self
IgG profiles associated with three clinical forms of the disease were found in MS. SERPA was also used
to identified targets in lung cancers (Huang LJ, 2006), in hepatocarcinoma (Ward DG, 2006) and in
renal cell carcinoma (Unwin, RD, 2006). As far as rheumatic diseases are concerned, the respective
expression of mRNA and proteins on SMs has been studied. Two authors stress differential protein
expression profiles in RA and in osteoarthritis synovial tissues. They highlight the interest of studies at
the protein level19 20. Previous studies using Western Blot analysis have also found immune reactivities
14
towards Bip12 or alpha enolase11 21 in rheumatoid arthritis, and towards triosephosphate isomerase (TPI)
in osteoarthritis22. In RA, synovial membrane and its components play a pivotal role in the
pathophysiology of the disease (36). However, they have only been used on a few occasions to analyse
immunogenic reactivities. Blass and al., using total protein preparations from RA SM, detected the
68kDa antigen25, subsequently identified as Bip26. Previously, we used SM to show that antibodies in
synovial fluids react to several proteins in RA. This study highlights the fact that other tissues (dermal,
muscle and dermal tissue), unlike SM, are unable to identify antibodies27. Since looking for only one
IgG reactivity in RA failed to clearly distinguish RA from healthy controls, more than one IgG
reactivity seems to be involved in RA pathophysiology.
The combination of 1-D and 2-D immunoblotting allowed us to detected three discriminant
proteins. First, p26 which is a discriminant antigen for RA, present in 40% of RA sera has been detected
as the 78kd glucose regulated protein named BiP (binding immunoglobulin protein). BiP is a member of
the 70 kilodalton stress protein family that resides of the lumen of the endoplasmic reticulum (ER)
(Gaut, 1997). BiP plays a central role in the proper folding and assembly of proteins. BiP has been
already proposed to be a putative antigen in RA {Bodman-Smith, 2003 #21; Blass, 2001 #24} and BiPspecific autoantibodies were present in 63% of RA patients in Blass study {Bodman-Smith, 2004 #18}.
In our study we found the presence of BiP in 40% of RA patients but other isoforms of BiP may have
not been detected. Another protein to be detected is lamin A/C. Lamin A/C belongs to the family of
intermediate filaments. Mutations in the lamin A/C gene have been reported in a wide variety of
disorders,
including
lipodystrophies,
cardiomyopathy,
muscular
dystrophies,
neuropathy,
mandibuloacral dysplasia, restrictive dermopathy, and progeria. If a strong association of autoantibodies
to human nuclear lamin B1 with lupus anticoagulant antibodies in systemic lupus erythematosus has
been described {Senecal, 1999 #68}, no association between autoantibodies to lamin A/C has been
previously described in RA. The third targeted protein was annexin 11. The annexin gene family
comprises calcium-binding proteins. The structural characteristics of annexin have been extensively
15
analysed, unless for annexin 11 which is supposed to be a structural prototype (ref). Several functions
have been described for annexin including anti-inflammatory activities and involvement of signal
transduction {Lecona, 2003 #69} and recently it has been shown that annexin 11-depleted cells failed to
complete cytokinesis and died by apoptosis {Tomas, 2004 #70}. In our study, annexin 11 is not detected
by serum IgG from in healthy controls but detected in 36% of RA sera. Previous studies have already
detected annexin 11 in RA sera (Misaki Y, 1994 ; Jorgensen, 2000)
It is out of interest that the autoantibodies against RA found in this study are ubiquitous. Moreover the
sensitivity for the diagnosis of RA is increased when several antigens are present without influencing
the specificity, suggesting the interest of a development of a protein microarray to improve the diagnosis
of RA. Nevertheless to avoid any confusion with the diagnosis of RA, we have selected sera of patients
with erosions and anti-CCP positive. To confirm the interest of these three markers, our results had to be
validating with RA sera in absence of anti-CCP and with earlier disease. Moreover, rheumatoid factor
might have an influence on protein expression as interference with immunoanalyse has been described
{Hamilton, 1989 #67}. Study of serum IgG profile in RA patients before the apparition of rheumatoid
factor will be of interest.
In this study we highlight the existence of discriminant serum IgG profile against RA FLS in RA
patients compared to healthy subjects. Some of the discriminant proteins have been previously detected
such as BiP and annexin 11. But a new protein, lamin, involved as vimentin in cytoskeletal change, have
been also characterised. Here we highlight the interest of a combination of IgG response against a
cluster of antigen to improve the diagnosis sensitivity of RA. To corroborate our hypothesises, the
characterisation of a such cluster of targets identified on a broader population, would be useful.
REFERENCES
16
1. Scott DL, Coulton BL, Popert AJ. Long term progression of joint damage in rheumatoid arthritis. Ann
Rheum Dis 1986;45(5):373-8.
2. Tak PP, Smeets TJ, Daha MR, Kluin PM, Meijers KA, Brand R, et al. Analysis of the synovial cell
infiltrate in early rheumatoid synovial tissue in relation to local disease activity. Arthritis Rheum
1997;40(2):217-25.
3. Cambridge G, Leandro MJ, Edwards JC, Ehrenstein MR, Salden M, Bodman-Smith M, et al.
Serologic changes following B lymphocyte depletion therapy for rheumatoid arthritis. Arthritis
Rheum 2003;48(8):2146-54.
4. Edwards JC, Leandro MJ, Cambridge G. B lymphocyte depletion therapy with rituximab in
rheumatoid arthritis. Rheum Dis Clin North Am 2004;30(2):393-403.
5. Dubucquoi S, Solau-Gervais E, Lefranc D, Marguerie L, Sibilia J, Goetz J, et al. Evaluation of anticitrullinated filaggrin antibodies as hallmarks for the diagnosis of rheumatic diseases. Ann
Rheum Dis 2004;63(4):415-9.
6. Masson-Bessiere C, Sebbag M, Girbal-Neuhauser E, Nogueira L, Vincent C, Senshu T, et al. The
major synovial targets of the rheumatoid arthritis-specific antifilaggrin autoantibodies are
deiminated forms of the alpha- and beta-chains of fibrin. J Immunol 2001;166(6):4177-84.
7. Vossenaar ER, Despres N, Lapointe E, van der Heijden A, Lora M, Senshu T, et al. Rheumatoid
arthritis specific anti-Sa antibodies target citrullinated vimentin. Arthritis Res Ther
2004;6(2):R142-50.
8. Chaiamnuay S, Bridges SJ. The role of B cells and autoantibodies in rheumatoid arthritis.
Pathophysiology 2005;12:203-16.
9. Kim WU, Cho ML, Jung YO, Min SY, Park SW, Min DJ, et al. Type II collagen autoimmunity in
rheumatoid arthritis. Am J Med Sci 2004;327(4):202-11.
10. Hayem G, De Bandt M, Palazzo E, Roux S, Combe B, Eliaou JF, et al. Anti-heat shock protein 70
kDa and 90 kDa antibodies in serum of patients with rheumatoid arthritis. Ann Rheum Dis
1999;58(5):291-6.
11. Saulot V, Vittecoq O, Charlionet R, Fardellone P, Lange C, Marvin L, et al. Presence of
autoantibodies to the glycolytic enzyme alpha-enolase in sera from patients with early
rheumatoid arthritis. Arthritis Rheum 2002;46(5):1196-201.
12. Corrigall VM, Bodman-Smith MD, Fife MS, Canas B, Myers LK, Wooley P, et al. The human
endoplasmic reticulum molecular chaperone BiP is an autoantigen for rheumatoid arthritis and
prevents the induction of experimental arthritis. J Immunol 2001;166(3):1492-8.
13. Bodman-Smith MD, Corrigall VM, Berglin E, Cornell HR, Tzioufas AG, Mavragani CP, et al.
Antibody response to the human stress protein BiP in rheumatoid arthritis. Rheumatology
(Oxford) 2004;43(10):1283-7.
14. Mouthon L, Haury M, Lacroix-Desmazes S, Barreau C, Coutinho A, Kazatchkine MD. Analysis of
the normal human IgG antibody repertoire. Evidence that IgG autoantibodies of healthy adults
recognize a limited and conserved set of protein antigens in homologous tissues. J Immunol
1995;154(11):5769-78.
15. Stahl D, Lacroix-Desmazes S, Mouthon L, Kaveri SV, Kazatchkine MD. Analysis of human selfreactive antibody repertoires by quantitative immunoblotting. J Immunol Methods 2000;240(12):1-14.
16. Lefranc D, Almeras L, Dubucquoi S, de Seze J, Vermersch P, Prin L. Distortion of the self-reactive
IgG antibody repertoire in multiple sclerosis as a new diagnostic tool. J Immunol
2004;172(1):669-78.
17. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American
Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis.
Arthritis Rheum 1988;31(3):315-24.
18. Zimmermann CW, Grus FH, Dux R. Multivariate statistical comparison of autoantibody-repertoires
(western blots) by discriminant analysis. Electrophoresis 1995;16(6):941-7.
19. Lorenz P, Ruschpler P, Koczan D, Stiehl P, Thiesen HJ. From transcriptome to proteome:
differentially expressed proteins identified in synovial tissue of patients suffering from
17
rheumatoid arthritis and osteoarthritis by an initial screen with a panel of 791 antibodies.
Proteomics 2003;3(6):991-1002.
20. Tilleman K, Van Beneden K, Dhondt A, Hoffman I, De Keyser F, Veys E, et al. Chronically
inflamed synovium from spondyloarthropathy and rheumatoid arthritis investigated by protein
expression profiling followed by tandem mass spectrometry. Proteomics 2005;5(8):2247-57.
21. Kinloch A, Tatzer V, Wait R, Peston D, Lundberg K, Donatien P, et al. Identification of citrullinated
alpha-enolase as a candidate autoantigen in rheumatoid arthritis. Arthritis Res Ther
2005;7(6):R1421-9.
22. Xiang Y, Sekine T, Nakamura H, Imajoh-Ohmi S, Fukuda H, Nishioka K, et al. Proteomic
surveillance of autoimmunity in osteoarthritis: identification of triosephosphate isomerase as an
autoantigen in patients with osteoarthritis. Arthritis Rheum 2004;50(5):1511-21.
23. Firestein GS. Invasive fibroblast-like synoviocytes in rheumatoid arthritis. Passive responders or
transformed aggressors? Arthritis Rheum 1996;39(11):1781-90.
24. FitzGerald O, Bresnihan B. Synovial membrane cellularity and vascularity. Ann Rheum Dis
1995;54(6):511-5.
25. Blass S, Specker C, Lakomek HJ, Schneider EM, Schwochau M. Novel 68 kDa autoantigen detected
by rheumatoid arthritis specific antibodies. Ann Rheum Dis 1995;54(5):355-60.
26. Blass S, Union A, Raymackers J, Schumann F, Ungethum U, Muller-Steinbach S, et al. The stress
protein BiP is overexpressed and is a major B and T cell target in rheumatoid arthritis. Arthritis
Rheum 2001;44(4):761-71.
27. Lafyatis R, Flipo RM, Duquesnoy B, Capron A. Antibodies in rheumatoid synovial fluids bind to a
restricted series of protein antigens in rheumatoid synovial tissue. Arthritis Rheum
1992;35(9):1016-27.
28. Hueber W, Kidd BA, Tomooka BH, Lee BJ, Bruce B, Fries JF, et al. Antigen microarray profiling
of autoantibodies in rheumatoid arthritis. Arthritis Rheum 2005;52(9):2645-55.
29. Kraan MC, Reece RJ, Smeets TJ, Veale DJ, Emery P, Tak PP. Comparison of synovial tissues from
the knee joints and the small joints of rheumatoid arthritis patients: Implications for pathogenesis
and evaluation of treatment. Arthritis Rheum 2002;46(8):2034-8.
30. Lionel A, de Seze J, Didier L, Sandrine FN, Sylvain D, Patrick V, et al. Evolution of self-reactive
IgG antibody repertoires in patients with relapsing-remitting multiple sclerosis. Immunol Lett
2005;97(1):55-62.
31. Lacroix-Desmazes S, Mouthon L, Kaveri SV, Kazatchkine MD, Weksler ME. Stability of natural
self-reactive antibody repertoires during aging. J Clin Immunol 1999;19(1):26-34.
32. Riente L, Chimenti D, Pratesi F, Delle Sedie A, Tommasi S, Tommasi C, et al. Antibodies to tissue
transglutaminase and Saccharomyces cerevisiae in ankylosing spondylitis and psoriatic arthritis.
J Rheumatol 2004;31(5):920-4.
33. Zou J, Zhang Y, Thiel A, Rudwaleit M, Shi SL, Radbruch A, et al. Predominant cellular immune
response to the cartilage autoantigenic G1 aggrecan in ankylosing spondylitis and rheumatoid
arthritis. Rheumatology (Oxford) 2003;42(7):846-55.
34. Duftner C, Dejaco C, Klauser A, Falkenbach A, Lakomek HJ, Schirmer M. High positive predictive
value of specific antibodies cross-reacting with a 28-kDa Drosophila antigen for diagnosis of
ankylosing spondylitis. Rheumatology (Oxford) 2006;45(1):38-42.
35. Dasuri K, Antonovici M, Chen K, Wong K, Standing K, Ens W, et al. The synovial proteome:
analysis of fibroblast-like synoviocytes. Arthritis Res Ther 2004;6(2):R161-8.
36. Kasperkovitz PV, Timmer TC, Smeets TJ, Verbeet NL, Tak PP, van Baarsen LG, et al. Fibroblastlike synoviocytes derived from patients with rheumatoid arthritis show the imprint of synovial
tissue heterogeneity: evidence of a link between an increased myofibroblast-like phenotype and
high-inflammation synovitis. Arthritis Rheum 2005;52(2):430-41.
18
Legends:
Figure 1: Serum self IgG reactivities against wrist RA SMs:
Comparative immunoreactive patterns against wrist SMs extracted proteins obtained with sera collected
either from healthy subjects (healthy control sera) or from RA patients (RA sera). Representative data
respectively obtained with 5 healthy control sera and 5 RA sera. As revealed by Western blotting, the
different patterns obtained with RA sera showed a higher number of protein bands than those observed
with healthy sera.
Figure 2: Choice of the antigenic targets: representative data obtained with RA wrist FLS
Comparative immunoreactive patterns of RA sera obtained by using RA FLS protein extracts at 3
different passages (RA FLS P3, RA FLS P4, RA FLS P5). Quite similar patterns were found for each
RA serum tested in the 3 conditions. Nevertheless, the best immune reactivity was found by using RA
FLS P5.
Figure 3: Sources of RA FLS:
The immunoreactive patterns against RA FLS protein extracts from different joints (wrist, hip, finger,
ankle, knee) were analysed. Quite similar patterns were respectively found with 3 RA sera (1, 2, 3),
tested against the different RA FLS.
Figure 4: Representative protein map obtained with RA wrist FLS
Two-dimensional separation of proteins extracted from RA wrist FLS. Spot were numbered according
to swiss-prot nomenclature.(details given in table 2).
Figure 5: Comparative self IgG reactivities of healthy sera and RA sera:
Immunoreactive patterns against wrist RA FLS protein extracts, obtained with sera collected either from
RA patients or healthy subjects. A higher number of antigenic bands were always noted with RA sera
(median value of 15 bands per patient) compared to those obtained with healthy control sera (median
value of 7 bands per subject).
Figure 6: LDA distinguishes the IgG immune patterns of healthy subjects and RA patients
In A, the graph shows that the calculated scores of each subject according to the LDA. In B, Receiver
operating characteristic (ROC) curve allows to define a cut-off value at 0.55 and shows a sensitivity of
89% and a specificity of 93%.
Figure 7: Characterization of discriminant antigens detected with RA sera:
19
Two representative two-dimensional immunoblots probed with 2 selected RA sera. Spots related to
antigenic reactivities (p26, p30, p37) were then analysed by MALDI-TOF-mass spectrometry after ingel digestion with trypsin.;
20