Coronary Artery Disease - The Oliver King Foundation
advertisement

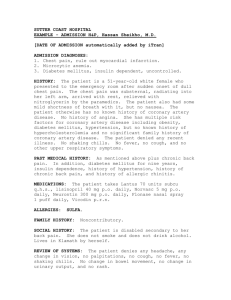
Sudden Arrhythmic Death Syndrome Dr. Simon Modi – Consultant Cardiologist/Electrophysiologist, Dr. Robert Cooper – Cardiology Specialist Registrar, Suzanne Kelly – Heart Rhythm Specialist Nurse Liverpool Heart and Chest Hospital Coronary artery disease: Coronary artery disease (CAD) is common in the Western world, but mainly occurs over the age of 35 years. Cholesterol and fat build up in the arteries that supply the heart muscle and cause narrowing and sometimes blockages to the blood supply of the heart. Complete blockages tend to cause significant heart attacks whereas narrowing tends to cause chest pains or tightness on exertion (angina). The heart’s rhythm can be disturbed during angina or due to long-term damage that a heart attack causes to the heart muscle. Coronary artery disease is very uncommon in young athletes. Occasionally coronary artery problems occur due to developmental problems (from birth) where the coronary arteries develop abnormally and become trapped between other organs in the chest causing narrowing of the arteries from outside pressure. Also, spasm or cramping (sudden, reversible narrowing of the arteries not caused by fat or cholesterol) of the arteries can occur leading to disruption of the heart’s rhythm. Most people with CAD will experience some symptoms of chest pain, tightness, shortness of breath, arm/jaw/shoulder or neck pain with exertion. There are many tests to investigate coronary artery disease. ECGs themselves are often normal unless taken during periods of chest pain or exercise. An angiogram (injecting dye directly into the arteries) is the clearest way of diagnosing coronary artery disease if doubt exists from other testing. Angiogram showing Coronary Artery Disease Left = blockage of right coronary artery (red arrow). Right = normal flow down artery after implantation of stent