Supplementary Information (doc 356K)
advertisement
")
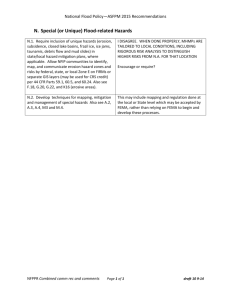
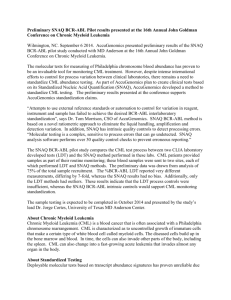
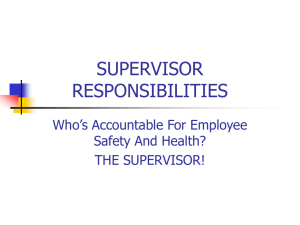
PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS SUPPLEMENTARY INFORMATION Table of contents Supplementary methods – Page 2 Supplementary results – Page 4 Supplementary references – Page 5 Supplementary tables – Page 6 Supplementary figures – Page 10 1 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Supplementary methods Multiple regression modelling As subdistribution hazards provided a direct link between the candidate variables and the cumulative incidence probabilities of dying of CML, the Fine-Gray model was preferred to standard Cox regression and cause-specific hazards.1,2 However, analysis of the cause-specific hazards of the event of interest and of all competing risks, supports the understanding of the event dynamics.3 Furthermore, for standard Cox regression, a particular SAS macro in order to model fractional polynomials for the continuous prognostic candidate variables was available.4 With the SAS macro, the statistically most suitable polynomial transformation for each variable was identified when modelling its influence on the cause-specific hazard of dying from CML. These transformations were then also used for investigating the influence on the subdistribution hazard with the Fine-Gray model. Interpretation of the results was based on both hazard models. The need to include interactions in a multiple model was examined. To assess the assumption of proportional hazards, for both regression models, Schoenfeld residuals were investigated.5,6 Cutoff identification For identification of cutoff(s) dividing the score into different risk groups, 1000 bootstrap samples were drawn with replacement from the original dataset. 7 Within each bootstrap sample, the minimal P value approach8 helped to determine the cutoff defining two groups with most different cumulative probabilities of dying from CML according to the Gray test statistic. A kernel density estimator was used as a smoothing function to visualize the selected cutoffs.9 Only cutoffs with P values <0.05 after Bonferroni adjustment for multiple testing were considered. After the decision on 2 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS the cutoff(s) based on the kernel density estimator, the calibration of the resulting risk groups of a new model was assessed with a calibration plot.10 Supplementary results Variables with prognostic influence on the cause-specific hazards of dying of CML In the situation of competing risks, it is recommended to also investigate causespecific hazards and the hazards of all competing events.3 Applying the Cox model with cause-specific hazards of dying of CML, in addition to age, spleen size, peripheral blasts, and platelet count, also sex and its interaction with hemoglobin were identified as significant prognostic factors. Supplementary Table 3 shows this best model in the 2190 patients with data to all candidate variables. Using only the four variables of the EUTOS long-term survival (ELTS) score, results in all 2205 evaluable patients are given in Supplementary Table 3. The cause-specific hazards ratios of the four variables in Supplementary Table 3 and the subdistribution hazards ratios reported for the ELTS score in Table 3 of the main manuscript are largely alike. This concordance suggests that the four variables have an actual effect on the cumulative incidence probabilities of dying of CML and their significance is not (just) due to an indirect effect on causes of death unrelated to CML. According to the Schoenfeld residuals, for the variables of the ELTS score, the assumption of proportional subdistribution hazards was appropriate. For prognostic analyses in the presence of competing risks, rather the use of the Fine-Gray model is recommended and the more parsimonious model of the ELTS score was preferred over the cause-specific hazards model which additionally identified sex and its interaction with hemoglobin as prognostic variables. 3 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Variables with prognostic influence on the hazards of death unrelated to CML Whether using the Fine-Gray model or the Cox model, age, sex, its interaction with hemoglobin, and white blood cell count were identified to be influential on the hazards of death unrelated to CML (Supplementary Table 4). Since the Akaike information criterion was applied for model selection, P=0.091 (sex, Table S4) was acceptable. As expected, the hazard for death unrelated to CML increased with age. Sex needs to be interpreted together with its interaction with hemoglobin; while the level of hemoglobin had hardly an influence on the hazards for male patients, it was influential with respect to females. Women with low hemoglobin levels had higher hazards of death unrelated to CML than males and women with higher levels of hemoglobin. Starting from hemoglobin levels higher than 10 g/dL, the hazards of women were lower than the hazards of men. Higher WBC counts corresponded to reduced hazards of CML-unrelated death. Again, by and large, the outcome of both hazard models is the same (Supplementary Table 4). In conclusion of all prognostic modelling, the events “death due to CML” and “death unrelated to CML” seem to be independent. 4 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Supplemental references 1. Andersen PK, Geskus RB, de Witte T, Putter H. Competing risks in epidemiology: possibilities and pitfalls. Int J Epidemiol. 2012;41(3):861-870. 2. Fine JP, Gray RJ. A Proportional Hazards Model for the Subdistribution of a Competing Risk. Journal of the American Statistical Association. 1999;94(446):496509. 3. Latouche A, Allignol A, Beyersmann J, Labopin M, Fine JP. A competing risks analysis should report results on all cause-specific hazards and cumulative incidence functions. Journal of Clinical Epidemiology. 2013;66(6):648-653. 4. Sauerbrei W, Meier-Hirmer C, Benner A, Royston P. Multivariable regression model building by using fractional polynomials: Description of SAS, STATA and R programs. Computational Statistics & Data Analysis. 2006;50(12):3464-3485. 5. Therneau TM, Grambsch, PM. Modeling Survival Data: Extending the Cox Model. New York: Springer; 2000. 6. Scrucca L, Santucci A, Aversa F. Regression modeling of competing risk using R: an in depth guide for clinicians. Bone marrow transplantation. 2010;45(9):13881395. 7. Davison AC, Hinkley, DV. Bootstrap Methods and Their application. Cambridge: Cambridge University Press; 1997. 8. Altman DG, Lausen B, Sauerbrei W, Schumacher M. Dangers of Using “Optimal” Cutpoints in the Evaluation of Prognostic Factors. Journal of the National Cancer Institute. 1994;86(11):829-835. 9. Silverman BW. Density estimation for statistics and data analysis. London: Chapman and Hall; 1986. 5 PFIRRMANN et al 10. PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Putter H, Fiocco M, Geskus RB. Tutorial in biostatistics: competing risks and multi-state models. Statistics in Medicine. 2007;26(11):2389-2430. Supplementary tables Table 1. Established baseline prognostic scores in chronic myeloid leukemia. Formula Sokal Scorea Sokal score Risk group = exp ( 0.0116 x (age [in years] – 43.4) Low risk: <0.80 + 0.0345 x (spleen size [cm below costal margin] – 7.51) + 0.1880 x ((platelet count [in 109/L] /700)² – 0.563) Intermediate risk: + 0.0887 x (blasts [% in peripheral blood]– 2.10) ) ≥0.80 and ≤1.20 High risk: >1.20 Euro Scoreb Euro score = ( 0.6666 x age [0 when age < 50 years; 1, otherwise] Low risk: ≤780 + 0.0420 x spleen size [cm below costal margin] + 0.0584 x blasts [% in peripheral blood] Intermediate risk: + 0.0413 x eosinophils [%in peripheral blood] >780 and ≤1480 + 0.2039 x basophils [0 when basophils [% in peripheral blood] < 3; 1, otherwise] High risk: >1480 + 1.0956 x platelet count [0 when platelets count [in 109/L] < 1500; 1, otherwise] ) x 1000 EUTOS scorec EUTOS score = 7 x basophils [% in peripheral blood] Low risk: ≤87 + 4 x spleen size [cm below costal margin] High risk: >87 EUTOS indicates European Treatment and Outcome Study. a Sokal JE, Cox EB, Baccarani M, Tura S, Gomez GA, Robertson JE, et al. Prognostic discrimination in "good-risk" chronic granulocytic leukemia. Blood 1984; 63(4): 789-799. b Hasford J, Pfirrmann M, Hehlmann R, Allan NC, Baccarani M, Kluin-Nelemans JC, et al. A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. Writing Committee for the Collaborative CML Prognostic Factors Project Group. J Natl Cancer Inst 1998; 90(11): 850-858. c Hasford J, Baccarani M, Hoffmann V, Guilhot J, Saussele S, Rosti G, et al. Predicting complete cytogenetic response and subsequent progression-free survival in 2060 patients with CML on imatinib treatment: the EUTOS score. Blood 2011; 118(3): 686-692. 6 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Table 2. Causes of death in the in-study registry. Number of cases Percent 92 44 Second cancer 50 24 Cardiovascular event 21 10 Infection 12 6 Other causes 21 10 Chronic myeloid leukemia (CML) Not related to CML (total: 104 cases, 50%)a Hemorrhagy 3 Old age 3 Acute leukemia unrelated to CMLb 2 Renal failure 2 Bone marrow aplasia 1 Car accident 1 Cerebrovascular adverse event 1 Chronic lung disease 1 CML (no progression reported)c 1 Ernia 1 Liver failure 1 Pemphigo 1 Poisoning 1 Suicide 1 Surgical complication 1 Unknownd Total aIn 6 n=208 100% none of the 104 cases, a “date of CML progression” was reported. bFurther information for the assessment “unrelated to CML” was not known. cFurther information for the assessment “CML” was not known. dIn 12 none of the 12 cases, progression of CML was reported. 7 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Table 3. Cox models with cause of death due to CML as event of interest and with censoring for death due to other causes. Significant prognostic factors in 2190 patients with complete data to all nine candidate variables. Variables Lower 95% Upper 95% Estimation of Cause-specific confidence limit confidence limit P coefficient hazard ratio for hazard ratio for hazard ratio (Age in years/10)3 0.0029 1.003 1.001 1.005 0.002 Spleen size, cm below costal margin 0.0539 1.055 1.017 1.096 0.005 Blasts, % in peripheral blood 0.0910 1.095 1.015 1.182 0.019 ((Platelet count x 109/L)/1000)-0.5 0.3998 1.492 1.073 2.074 0.017 Sex (coding: 0 = male, 1 = female) 2.8272 16.898 2.321 123.013 0.005 Interaction: hemoglobin, g/dl x sex -0.2581 0.773 0.642 0.930 0.006 Significance of the four prognostic factors part of the EUTOS survival score, now using all 2205 evaluable patients. Variables Lower 95% Upper 95% Estimation of Cause-specific confidence limit confidence limit P coefficient hazard ratio for hazard ratio for hazard ratio (Age in years/10)3 0.0027 1.003 1.001 1.005 0.004 Spleen size, cm below costal margin 0.0628 1.065 1.029 1.197 <0.001 Blasts, % in peripheral blood 0.1042 1.110 1.027 1.104 0.007 ((Platelet count x 109/L)/1000)-0.5 0.4034 1.497 1.078 2.079 0.016 8 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Table 4. Significant prognostic factors in all 2190 patients with complete data to all 9 candidate variables when causes of death unrelated to CML were of primary interest. Fine and Gray model keeping patients with the competing event death due to CML in the risk set. Variables Lower 95% Upper 95% Estimation of Subdistribution confidence limit confidence limit P coefficient hazard ratio for hazard ratio for hazard ratio (Age in years/10)3 0.0077 1.008 1.006 1.009 <0.001 Sex (coding: 0 = male, 1 = female) 2.2045 9.066 0.702 117.084 0.091 Interaction: hemoglobin, g/dl x sex -0.2291 0.795 0.640 0.989 0.039 (White blood cell count x109/L)/100 -0.3915 0.676 0.512 0.893 0.006 Lower 95% Upper 95% Cox model with censoring at time of death due to CML. Variables Estimation of Cause-specific confidence limit confidence limit P coefficient hazard ratio for hazard ratio for hazard ratio (Age in years/10)3 0.0078 1.008 1.006 1.009 <0.001 Sex (coding: 0 = male, 1 = female) 2.4272 11.327 1.127 113.830 0.039 Interaction: hemoglobin, g/dl x sex -0.2470 0.781 0.642 0.951 0.014 (White blood cell count x109/L)/100 -0.3890 0.678 0.514 0.893 0.006 9 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Supplementary figures Figure 1. Kernel density of 997 optimal cutoffs according to the minimal P value approach. One thousand bootstrap samples with n = 2205 were drawn from the original dataset. After P value adjustment for multiple testing, in 997 samples, a statistically significant best cutoff was identified. A smoothing function of these 997 cutoffs resulted in the three-headed kernel density. The cutoffs at the two highest peaks, 1.5680 and 2.2185 led to the definition of three risk groups for the new score. 10 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS Figure 2. Cumulative incidence probabilities of dying of chronic myeloid leukemia in 1120 patients of the out-study registry. a Stratification of the risk groups according to the Sokal score. Number of patients still at risk (n) at different years of observation Year 0 2 5 8 High risk, n 259 219 142 15 Intermediate risk, n 411 384 261 28 Low risk, n 450 420 298 37 At 2, 5, and 8 years, horizontal crossbars indicate the upper and lower limit of the 95% confidence interval (CI) for the estimated probability. 11 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS b Stratification of the risk groups according to the Euro score. Number of patients still at risk (n) at different years of observation Year 0 2 5 8 High risk, n 131 110 67 5 Intermediate risk, n 523 480 336 38 Low risk, n 466 433 298 37 At 2, 5, and 8 years, horizontal crossbars indicate the upper and lower limit of the 95% confidence interval (CI) for the estimated probability. 12 PFIRRMANN et al PROGNOSIS OF LONG-TERM SURVIVAL IN CML PATIENTS c Stratification of the risk groups according to the EUTOS score. Number of patients still at risk (n) at different years of observation Year 0 2 5 8 High risk, n 149 128 86 8 Low risk, n 971 895 615 72 At 2, 5, and 8 years, horizontal crossbars indicate the upper and lower limit of the 95% confidence interval (CI) for the estimated probability. 13