Surfactant Biology and Pulmonary Fibrosis: A ChILD Shall Lead Them
advertisement

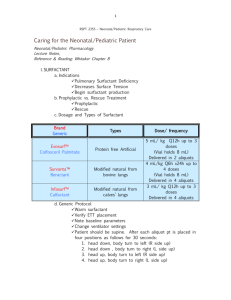
Surfactant Biology and Pulmonary Fibrosis: A ChILD Shall Lead Them Lawrence M. Nogee, M.D. Professor of Pediatrics Division of Neonatology Department of Pediatrics Johns Hopkins University School of Medicine Baltimore, MD USA 21287 Contact information: Mail: CMSC 6-104A 600 N. Wolfe Street Baltimore, MD 21287 USA Phone: 410 614-3355 Fax: 410 614-8388 E-mail:lnogee@jhmi.edu Word count: 1751 Pulmonary surfactant is the mixture of lipids and proteins needed to reduce surface tension in the alveolus and prevent end-expiratory atelectasis. Surfactant deficiency as a result of pulmonary immaturity is the principal cause of the respiratory distress syndrome (RDS) observed in prematurely born infants, and surfactant inactivation contributes to the pathophysiology of acute RDS observed in older children and adults. Genetic mechanisms disrupting the normal production and metabolism of surfactant components have been recognized as the cause for some forms of children’s interstitial lung disease (ChILD) previously considered to be idiopathic 1 . While these diseases are rare, they are associated with considerable morbidity and mortality. Understanding for the basis for these disorders also has implications for lung disease in older children and adults. Surfactant components are synthesized, stored and secreted by alveolar type II epithelial cells (AEC2s), and genetic mechanisms affecting the expression of surfactant components may not only lead to functional surfactant deficiency, but serve as a source of endogenous injury to AEC2s. These observations, along with studies on genetic causes of pulmonary fibrosis in adults, support the hypothesis that chronic injury to AEC2s is an important mechanism for pulmonary fibrosis across all age groups. Surfactant is comprised of approximately 90% lipid by weight and 10% protein. Two low molecular-weight, extremely hydrophobic proteins, Surfactant Proteins (SP-) B and C are critically important in order to enhance the surface-tension lowering properties of surfactant lipids. Both SP-B and SP-C are components of the mammalian-derived exogenous surfactant preparations used to treat premature neonates with RDS. SP-B and SP-C are encoded on separate genes, termed SFTPB and SFTPC respectively. Both are synthesized as larger precursor proteins (proSP-B, proSP-C) that need to be proteolytically processed to the mature SP-B and SP-C proteins found in surfactant. Surfactant also contains two larger, structurally related glycoproteins, SP-A and SP-D. These proteins are part of the collectin family, containing collagenous and lectin-like domains, and have important roles in innate immunity in the lung, as well as roles in immunomodulation and surfactant metabolism. There are two genes for SP-A (SFTPA1, SFTPA2) and a single gene for SP-D (SFTPD). Surfactant lipids and proteins are packaged within the AEC2 in lysosomally-derived organelles called lamellar bodies, and secreted by exocytosis of the lamellar bodies. A member of the ATP Binding Cassette (ABC) family of transporter proteins, ABCA3, is highly expressed in AEC2s and localized to the limiting membrane of lamellar bodies. ABC proteins hydrolyze ATP to transport substances across biological membranes, and ABCA3 has a role in the transport of lipids critical for surfactant function into the lamellar body. The expression of surfactant lipids and proteins is developmentally regulated, with their expression increasing with advancing gestation. The transcription factor, NKX2.1, also known as thyroid transcription factor 1 (TTF1), has an essential role in the expression of the surfactant proteins and ABCA3. Mutations in the genes encoding surfactant components have now been recognized as the etiology for lung disease of variable onset and severity, ranging from fatal RDS in full-term infants to pulmonary fibrosis in adults who may be asymptomatic until the 5th or 6th decade of life. SP-B deficiency was the first recognized of these disorders, which results from loss-offunction mutations on both SFTPB alleles. Infants affected by this autosomal recessive disorder generally present with hypoxemic respiratory failure in the immediate neonatal period and diffuse lung disease that radiographically resembles RDS in premature infants. The disease is generally progressive, with death usually occurring within three months despite maximal medical support, and lung transplantation is the only effective therapy. The disorder is exceeding rare, with an estimated incidence of < 1 in one million live births. Aside from the lack of SP-B, secondary abnormalities are observed in other surfactant components which also contribute to the pathophysiology of the disorder, including an inability to fully process proSP-C to SP-C, and an abnormal surfactant lipid profile. Normally formed lamellar bodies are not observed in SP-B deficient AEC2s by electron microscopy, which instead contain large, organelles with vacuoles and poorly formed lamellae. Genetically engineered mice in which SP-B production is able to be turned off as adults develop lung abnormalities when SPB levels fall to 20% to 30 % of control values, supporting the notion that there is a critical level of SP-B needed for normal lung function. These findings, combined with the observations that rare children with mutations resulting in partial deficiency can survive the newborn period and the overlap of lung pathology findings in SP-B deficient children with those observed in some forms of ChILD, specifically chronic pneumonitis of infancy and desquamative interstitial pneumonia, led to the investigation of other components of the surfactant system in these disorders. Loss-of-function mutations on both alleles of the gene encoding ABCA3 (ABCA3) cause diffuse lung disease that is variable in its onset and severity inherited as an autosomal recessive disorder. Affected infants may present with an RDS-like phenotype similar to that of SP-B deficient infants and have progressive, fatal disease. Others may have mild, transient neonatal lung disease, thought to be either mild RDS, transient tachypnea or pneumonia, or have no pulmonary symptoms in the neonatal period, but present later in life with pulmonary symptoms along with clubbing, pectus excavatum, and/or failure to thrive 2. Prolonged survival is possible with affected patients > 30 years of age identified. Such individuals have at least one mutation predicted to result in some ABCA3 protein, compared to more severely affected infants with clear-cut complete loss-of-function mutations, suggesting that genotype may be an important predictor of outcome, with relatively milder phenotypes due to mutations that allow for some retained ABCA3 function. A lack of normal lamellar bodies in AEC2s from ABCA3 deficient infants which instead contain small, dense bodies with eccentrically placed electron dense cores giving them a “fried-egg” appearance supports a role for ABCA3 in lamellar body biogenesis. These observations coupled with the findings of abnormal phospholipids profiles in bronchoalveolar lavage fluid obtained from ABCA3 deficient infants undergoing lung transplantation and in lung tissue of ABCA3 null mice support a role for ABCA3 in transporting surfactant lipids into lamellar bodies. The observations that some affected children had minimal or no neonatal lung disease suggests that these children produced sufficient amounts of surfactant perinatally, and that other factors are important in the pathophysiology of the chronic lung disease due to ABCA3 deficiency. The incidence and prevalence of ABCA3 deficiency are unknown, but the relative frequency with which ABCA3 deficient compared to SP-B deficient infants have been identified suggest that it may be the most common cause of genetic surfactant dysfunction. Mutations on one SFTPC allele are sufficient to cause disease, and the mechanism is thought to be due to a gain of toxic function, with mutations inducing misfolding of proSP-C. The misfolded protein elicits the unfolded protein response, with secondary downstream events resulting in direct toxicity to the AEC2, including apoptosis and secondary inflammation. Sporadic disease may result from de novo mutations, or lung disease may be inherited as an autosomal dominant trait with variable penetrance. The age of onset of disease is highly variable, even amongst family members with the same mutation, ranging from presentation in infancy (tachypnea, hypoxemia in room air, clubbing, failure to thrive) to the onset of dyspnea associated with pulmonary fibrosis in the 5th or 6th decade of life. Neonatal lung disease due to SFTPC mutations has been reported, but is unusual. Factors responsible for the variable severity of disease remain largely unknown, although there may be interactions with mutations in other surfactant-related genes, such as ABCA3, and viral infections. The incidence and prevalence of lung disease due to SFTPC mutations are unknown. SFTPC mutations appear to be a rare cause of idiopathic pulmonary fibrosis in adults, but suggest a role for toxicity to and loss of AEC2s as possible primary events in the pathogenesis of pulmonary fibrosis. Mutations resulting in loss-of-function or deletions of one copy (haploinsufficiency) of the gene for TTF1 can cause lung disease with the phenotypes ranging from neonatal RDS to ILD in older children and adults. As the protein is also expressed in the thyroid gland and the central nervous system, affected patients may also exhibit signs of hypothyroidism or neurological symptoms (Brain-Thyroid-Lung Syndrome) 3. Chorea is the most specific neurological finding, but young infants may have non-specific findings of hypotonia and developmental delay. Both isolated hypothyroidism and chorea have been reported due to TTF1 haploinsufficiency. Whether isolated pulmonary disease occurs and the full range of pulmonary phenotypes due to TTF1 mutations remains to be determined. As TTF1 is important in the expression of multiple surfactant-related genes in AEC2s, it is unknown if the lung disease results from reduced expression of primarily one protein or combined effects. Mutations in the genes encoding the components of telomerase have been recognized as causes of familial pulmonary fibrosis in adults, and mutations in SFTPA2 were recently reported in two kindreds with familial pulmonary fibrosis and lung adenocarcinoma 4, 5. Loss of telomere length leads to death of replicating cells and AEC2s serve as progenitor cells for the lung epithelium after injury as well as being responsible for surfactant production. Thus the linkage of both of these genes to adult-onset pulmonary fibrosis further supports the hypothesis that injury to the AEC2 cell may represent a primary event in the initiation of pulmonary fibrosis, as exemplified by genetic causes of ChILD. Therapies aimed at improving surfactant homeostasis and AEC2 function in ChILD patients may therefore have roles in adult lung disease as well. The identification of genetic causes of ChILD allows for potential non-invasive diagnosis by genetic testing and such testing is now available in clinical diagnostic laboratories. Limitations of genetic testing include cost, the time needed to obtain results particularly in a critically ill or rapidly deteriorating child, and unknown sensitivity of such testing. Current approaches may miss mutations in untranslated regions as well as large deletions, insertions or rearrangements, and the interpretation of results may not be straight-forward. In addition there are likely to be mutations in as yet undiscovered genes that result in similar phenotypes. Correct and timely genetic diagnosis will allow proper counseling of families regarding recurrence risk, and potentially eliminate the need for lung biopsy and its associated risks and morbidity. Currently there are no specific treatments available for ChILD due to genetic surfactant dysfunction, and only anecdotal reports different therapies which are difficult to evaluate given the variable natural history of some of the disorders. The evaluation of currently available and development of novel therapies are important areas for future research. References: 1. Wert SE, Whitsett JA, Nogee LM. Genetic disorders of surfactant dysfunction. Pediatr Dev Pathol 2009;12(4):253-74. 2. Doan ML, Guillerman RP, Dishop MK, et al. Clinical, radiological and pathological features of ABCA3 mutations in children. Thorax 2008;63(4):366-73. 3. Guillot L, Carre A, Szinnai G, et al. NKX2-1 mutations leading to surfactant protein promoter dysregulation cause interstitial lung disease in "Brain-Lung-Thyroid Syndrome". Hum Mutat;31(2):E1146-62. 4. Armanios MY, Chen JJ, Cogan JD, et al. Telomerase mutations in families with idiopathic pulmonary fibrosis. N Engl J Med 2007;356(13):1317-26. 5. Wang Y, Kuan PJ, Xing C, et al. Genetic defects in surfactant protein A2 are associated with pulmonary fibrosis and lung cancer. Am J Hum Genet 2009;84(1):52-9.