Diabetes Emergency Care Plan
advertisement

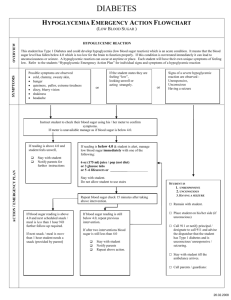
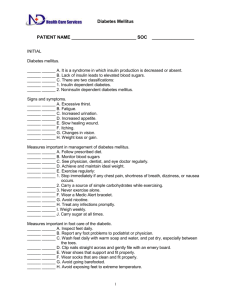
Diabetes Emergency Care Plan Individual Health Care Plan Student Name: _____________________________ Birthdate: _________ Grade: ____ Date: _______ Background information: Diabetes is a chronic illness that results from failure of the pancreas to make a hormone called insulin. Blood sugars are monitored to prevent low blood sugar (hypoglycemia) and high blood sugar (hyperglycemia). Medication: ________________________________________________ Signs and symptoms of Low Blood Sugar (hypoglycemia) can include: Tired, hunger, dizziness, shakiness, not feeling well, sweaty, drowsy, weak, headache, irritable, confusion, blurry vision, weakness, slurred speech, behavior change, poor coordination, labored breathing, loss of consciousness, seizures Other: ___________________________________________________________ Never send a child with a suspected low blood sugar anywhere alone! Emergency Action Plan for Low Blood Sugar: 1. Low blood sugar (hypoglycemia) is a medical emergency and requires immediate treatment. 2. If able, have student escorted to the Health Center or Office. 3. If possible, check blood sugar per plan. If you do not know how to test or there is no meter to test with……TREAT anyway. 4. Always, if in doubt, TREAT. 5. Give quick sugar source: 2 to 3 glucose tablets, 4 to 8 ounces of juice, 4 to 8 ounces of regular pop (not diet), 3 to 8 lifesavers, glucose gel product. 6. Stay with the child, repeat treatment if necessary in 15 minutes. 6. Call 911 for loss of consciousness or seizure. 7. Call parent/guardian. NOTE: High blood sugar (hyperglycemia) is a blood sugar reading typically greater than 240. Although high blood sugars are not good for the child, they do not generally pose the medical emergency that low blood sugars do. Symptoms can include frequent urination and extremely thirsty. Check blood sugar per plan. Parents must be notified of blood sugars greater than ________. Parent/Guardian Emergency Contact Information: #1 Call ___________________________ Home:___________ Work: __________ Cell: ____________ #2 Call ___________________________ Home: ___________ Work: __________ Cell: ____________ Parent/guardian is responsible for notifying after school activities program staff/adult/coach of all aspects of students diabetes needs. *** I understand that the above information may be shared with school district staff s needed to protect the health and safety of this student and to plan for a safe environment conducive to learning.*** Parent/Guardian Signature: _____________________________________________ Date: _______________ School Nurse Signature: _______________________________________________ Date: _______________ ___________________________________________________________________ Date: _______________ 5-17-13