Communication Skills for Children with Down`s Syndrome
advertisement

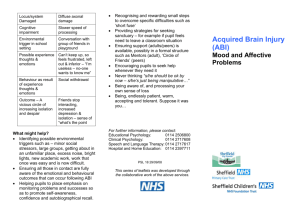
As the brain is developing and maturing throughout childhood, it is common for some problems to become evident months or even years after the original illness / injury. Such ‘late onset’ difficulties may emerge long after the pupil has been discharged from rehabilitation follow up. It is thus important that pupils with acquired brain injury are identified within the education system, and can be tracked throughout the education process. This will ensure that any emergent problems are associated with ABI and that appropriate guidance can thus be sought at any stage. Critical points educationally include when the pupil is changing school year, teachers and / or schools. Brain maturation continues throughout childhood and into adulthood. Critical points have however been linked with both entering and leaving adolescence. A pupil is coming into our school following ABI – what do we need to do? Key elements that will promote successful entry or re-integration to school include: Liaison with rehabilitation professionals, to gain a clear overview of the current situation and prognosis. Provision of information to rehabilitation professionals regarding: If known, the pupil’s prior learning style – both strengths and weaknesses. The structure of the school day. Resources available to support the successful entry / return of the pupil Setting up a review meeting with / seeking guidance from both rehabilitation and educational professionals, and parents regarding: Timing of reintegration e.g. a phased return to school which takes into account issues such as fatigue. Any necessary modifications to the school’s physical environment Any recommended changes to schedules / activities Coping strategies to support altered learning and / or psychosocial skills Monitoring the pupil across the weeks and months after entry / return to the school. Continued liaison with the rehabilitation professionals and relevant educational professions (e.g. educational psychology) Ensuring that information is passed on to receiving teachers and schools as the pupil moves through the education system, to ensure that the information regarding ABI is available throughout. For further information, please contact: Educational Psychology: 0114 2506800 Clinical Psychology: 0114 2717608 Speech and Language Therapy: 0114 2717617 Hospital and Home Education: 0114 2397711 This series of leaflets was developed through the collaborative work of the above services. PSL 13 29/09/08 Acquired Brain Injury (ABI) An Overview . While not every pupil will necessarily have every problem outlined below, the following summary illustrates areas of potential change. School staff should be aware of such potential changes when a pupil enters / returns to school following an ABI. What is Acquired Brain Injury? This leaflet aims to provide: An introduction to some of the consequences of Acquired Brain Injury (ABI). General advice regarding ways in which receiving schools can support pupils following ABI. What skills can be affected by ABI? The presentation of any of the problems identified below will be affected by the pupil’s age and level of development at the time of the injury / illness. Acquired Brain Injury (ABI) is the term applied when an illness or injury affects the development of a brain, which was previously developing along broadly normal lines. Cognitive and executive skills e.g.: Remembering (long and / or short term memory problems) Paying Attention Planning and Goal Setting Self – initiation, control, monitoring and evaluation Reasoning Thinking Flexibly and Problem Solving Information Processing Forming Judgments ABI does not describe disabilities that are present from birth (i.e. congenital or developmental difficulties). An ABI can result from: Trauma, including motor vehicle accidents, falls, and sporting injury Non-traumatic causes including infections, tumours, strokes, and anoxic damage i.e. lack of oxygen to the brain (e.g. through choking, strangulation or near drowning) Sensory, and motor skills e.g.: Vision Hearing Walking and other physical activities Incidence in the region of 200 per 100,000 population. Thus a large number of schoolaged children in city the size of Sheffield will sustain and live with the consequences of acquired brain injury. Perceptual skills e.g.: Judging depth or distance Psychosocial skills e.g.: Forming and maintaining friendships Understanding other peoples views or needs Behavioural skills e.g. distractibility, irritability, impulsivity – leading to acting in a way inconsistent with the setting. Mood changes e.g. anxiety, passivity, depression It is estimated that each year 3000 children in the UK will acquire new neurological or cognitive disability as a result of traumatic brain injury alone. While a proportion of pupils will have visible physical difficulties following ABI, the majority will have more subtle changes, related to altered cognitive abilities and / or psychosocial skills. . Language and speech skills e.g.: Understanding and using language Impaired ability to communicate in a manner appropriate to the social setting Retrieving known words Talking clearly Are there other signs of ABI which could affect education? Common problems include: Fatigue Headaches Frustration What does school need to know? When a pupil enters or returns to school following an ABI, their educational and / or emotional abilities and needs may be very different from before. Pupils with ABI differ from pupils with developmental learning or behavioural problems, as often they will retain a sense of their previous skills. They can be aware of, but unable to understand, the changes in these skills. The expectations of family and staff may need to change, in order to provide appropriate support, and introduce suitable and effective strategies to support the returning pupil. Schools need to be aware of the types of difficulty that can result from an ABI, and the ways in which learning can be affected. This will enable timely access to support and advice, both in the short and longer term.