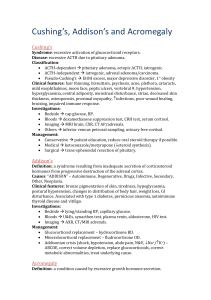
Acromegaly
advertisement

Acromegaly Stem Statement Please examine hands, face, look and proceed. Patient has headaches, increased sweatiness Approach 1. Hands a. Palm downwards – large, doughy, spade shaped, OA, double pinch test b. Palm upwards – sweatiness, CTS, wasting of thenar eminence, numbness 2. Elbows – ulnar nerve thickening 3. Proximal myopathy 4. Face – Transfrontal scar, prominent supraorbital ridges, greasy skin, broad nose, hirsute, thickened lips, macroglossia, teeth indentation marks on the side of the tongue, prognathism, splaying of teeth, malocclusion of teeth 5. Neck – Goitre 6. Lower limb – bowed legs, OA, pitting edema from CCF/CCB, heelpad thickened 7. Request for patient to remove shirt to inspect the trunk and axillae a. Skin tags b. Coarse body hair c. Acanthosis nigricans d. Gynaecomastia, galactorrhoea e. Kyphosis 8. Request a. Visual fields – bitemporal hemianopia, fundoscopy for angiod streaks b. CVS – cardiomegaly c. Abdomen – organomegaly, testicular atrophy, PR bleed for Ca colon d. BP - Hypertension e. Urine dipstick – glycosuria Presentation Sir, this patient has acromegaly as evidenced by presence of coarse facial features with prominent supraorbital ridges, broad nose and thick lips; a/w macroglossia with teeth indentation marks on the side of the tongue. There is also presence of splaying of the teeth with malocclusion and prognathism. I did not notice any scars on the forehead to suggest previous Transfrontal surgery. There is also no goitre There is presence of a large, spade like doughy hands with no sweating detected. There is no wasting of the thenar eminence and Tinel’s sign was negative. There are also no thickened ulna nerves at the elbows and no proximal myopathy. No features of OA of the hands and no bowing of the tibia. No pedal edema but presence of thickened heelpads. I would like to complete the examination by 1. Asking the patient to remove his shirt to look for Acanthosis nigricans, coarse body hair, skin tags, kyphosis and gynaecomastia/galactorrhea 2. Visual fields for bitemporal hemianopia 3. CVS – cardiomegaly 4. Abdomen exam for organomegaly 5. BP 6. Screen for DM 7. Ask for symptoms of headache, increase sweatiness and recent increase in shoe or glove size. Questions 1. What is acromegaly? a. Due to excess GH activity as a result of a pituitary macroadenoma occurring post puberty 2. What are the indicators of activity? a. Skin tags b. Increased sweatiness, headache c. Increased size of goitre/visual field loss/size of hands/Shoe size d. Hypertension e. Glycosuria 3. What are angiod streaks? a. Degeneration and fibrosis of Bruch’s membrane 4. List causes of macroglossia. a. Acromegaly b. Hypothyroidism c. Amyloidosis d. Down syndrome e. Haematological malignancy 5. What is the pathology of acromegaly? a. Pituitary macrodenoma 6. What are the complications? a. Metabolic and endocrine i. Diabetes mellitus in 20% of patients ii. Hypertriglyceridemia in 40% of patients b. Cardiovascular i. Hypertension ii. Cardiomyopathy and CCF c. Respiratory i. Acute dyspnea and stridor (upper airway narrowing) ii. Obstructive sleep apnea d. Abdomen i. Colonic polyps and malignancies (ie, colon cancer) ii. Organomegaly, testicular atrophy e. Neuromuscular i. Proximal myopathy ii. Nerve root compression – CTS, radiculopathy iii. Spinal stenosis f. Calcium and bone metabolism i. Hypercalciuria ii. Hyperphosphatemia iii. Urolithiasis 7. How do you investigate? a. Confirm the diagnosis by OGTT to look for non supressibility of GH (2ng/ml), can also screen for DM b. Other useful blood Ix i. IGF-1 – as a baseline and monitoring disease activity and treatment ii. Prolactin levels as 20% are associated with hyperprolactinaemia 1. low in hypopit 2. High because 1. Co-secretion 2. compression of pit stalk with interference of dopaminergic suppression of prolactin production iii. Pituitary function (SST, TFT, FSH/LH/Testos/Oestradiol) iv. Calcium levels – MEN type 1 syndrome c. Imaging (after diagnosis is confirmed) i. MRI of the pituitary fossa – macroadenoma ii. X-rays 1. Skull – Enlarged sella turcica, enlarged frontal, ethmoid and mastoid sinuses, thickened calvarium, enlarged mandible 2. CXR – cardiomegaly 3. Hand and feet X-rays – terminal phalangeal tufting and thickened heel pad (>23mm thick on a lateral X-ray) d. Others i. Formal perimetry ii. Obtain old photos iii. ECG - LVH 8. How would you manage? a. The definitive therapy is surgical which can be via transphenoidal or the transfrontal approach b. Radiation therapy if pt is not a suitable candidate c. Medical therapy i. Bromocriptine – dopamine agonist (PO) ii. Octreotide or long acting type (SC, daily vs monthly) iii. GH receptor antagonist – pegvisomant which is a recombinant DNA analogue (SC daily) 9. What are the conditions with excess GH besides acromegaly? a. MEN type 1 (PPP) b. McCune Albright syndrome – Polyostotic fibrous dysplasia, sexual precocity and café-au-lait spots c. Carney Complex – multicentric tumors in multiple organs, pigmented skin lesions and pigmented nodular hyperplasia (aut dominant)