Medical History Questionnaire
advertisement

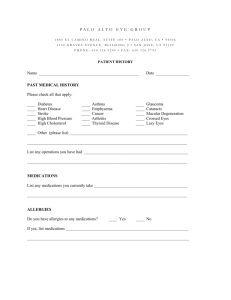
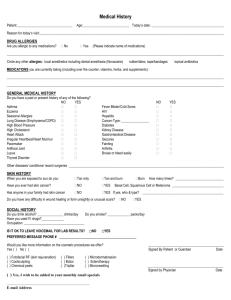
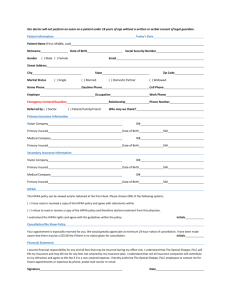
Medical History Questionnaire Medical History Do you have any allergies to medications? No Yes If yes, explain: _______________________________________ ______________________________________________________________________________________________________ List any medications you take (including oral contraceptives, aspirin, over the counter medications and home remedies): _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ List all major injuries, surgeries and/or hospitalizations you have had: _____________________________________________ ______________________________________________________________________________________________________ List any of the following that you have had: crossed eyes, lazy eye, drooping eyelid, prominent eyes, glaucoma, retinal disease, cataracts, eye infections or eye injury: ________________________________________________________________________ Do you wear glasses? Do you use tobacco products? Do you drink alcohol? Do you use illegal drugs? No Yes Do you wear contact lenses? No Yes No Yes If yes, type/amount/how long: ___________________________________________ No Yes If yes, type/amount/how long: ___________________________________________ No Yes If yes, type/amount/how long: ___________________________________________ Review of Systems Do you currently, or have you ever had any problems in the following areas (Please check column Yes or No): SYSTEM Constitutional-Fever, Weight Loss/Gain Integumentary-Skin Neurological- Headaches, Migraines, seizures Psychiatric Genitourinary- Genitals, Kidney, bladder Lymphatic/Hematologic- Anemia, Bleeding Problems Allergic Immunologic Eyes- Dryness, Mucous Discharge, Redness, Sandy or Gritty Feeling, Itching, Burning Eyes-Eye Pain or soreness, chronic infection of eye or lid NO YES SYSTEM Ears, Nose, Mouth, Throat- Allergies/Hay Fever Respiratory- Asthma, Chronic Bronchitis, Emphysema Vascular/Cardiovascular- Diabetes, Heart Pain, High Blood Pressure, High Cholesterol, Vascular disease Endocrine- Thyroid/Other Glands Gastrointestinal- Diarrhea/Constipation NO YES Bones, Joints, Muscles- Rheumatoid Arthritis, Muscle pain, Joint Pain Eyes-Loss of vision, Blurred vision, Distorted Vision/Halos, Loss of side Vision, Double vision Eyes- Foreign body sensation, Excessive tearing/watering, Glare/light sensitivity Eyes-Sties or Chalazion, Flashes/Floaters in Vision, Tired eyes Family History –Please note any family history (parents, grandparents, siblings, children; living or deceased) for the following conditions: No Yes Relationship to you Disease/Condition Blindness Crossed eyes Glaucoma Macular Degeneration Retinal Detachment Disease Diabetes ________________________________________________________ __________________________ Doctor’s Signature Date