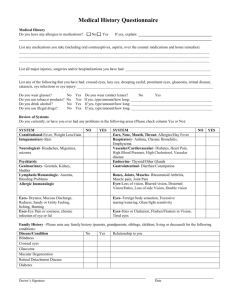
new patient medical history questionnaire
advertisement

Hudson Valley Eye Surgeons, P.C. Vassar Brothers Medical Mall 200 Westage Business Center Drive Fishkill, New York 12524 Phone: 845-896-9280 Fax: 845-896-0246 NEW PATIENT MEDICAL HISTORY QUESTIONNAIRE Name: Pharmacy: Date of Birth: / / Pharmacy Location: Sex: M 1. Have you ever had a previous eye injury, surgery, or laser surgery? Yes F No If yes, please describe: 2. Have you ever had a turned (crossed) eye or lazy eye? Yes No 3. Have you every been told that you have any of the following: Heart disease Yes No Cancer A Heart Attack Yes No A Birth Defect A Stroke or TIA Yes No Glaucoma High Blood Pressure Yes No Cataract Diabetes Yes No Retinal Disease Arthritis Yes No Yes Yes Yes Yes Yes No No No No No 4. Please list any other serious illnesses and major operations: 5. Please list all medications and eye drops you are currently taking, including dosages and frequency: 6. Please list all allergies to medications, including the reaction (what happened): 7. Do you have any close family members who have had glaucoma, cataract, or retinal disease? If so, please list. 8. Do you smoke or drink alcohol? Yes No Experts in Eye Care for Over 30 years – www.hves.com 08_2014