Dr. Ness Patient Health History Form
advertisement

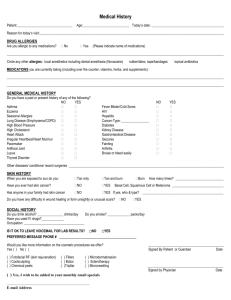
Rachel Ness, MD, PLLC Patient Health History Form Patient Name: __________________________________________________Today’s Date: _______________________________________ Birth Date: __________________________________________ Date of Last Full Body Examination: _______________________________ What are you being seen for today? (We ask that you focus on 3 concerns per visit to enable Dr. Ness to provide the most thorough care) 1. ______________________________________________________________________________________________________ 2. ______________________________________________________________________________________________________ 3. ______________________________________________________________________________________________________ 1. Have you ever had skin cancer? Yes No If yes, when, where on your body, and what type? _____________________________________________________ 2. Have any immediate relatives had skin cancer? Yes No If yes, who and what type? _____________________________________________________ 3. Do you have artificial joints, heart valves, pacemaker? Yes No If yes, where? ___________________________ 4. Do you require pre-op antibiotics prior to any dental procedures? Yes No 5. Have you ever had a reaction to local anesthesia or lidocaine/novocaine? Yes No If no, have you ever had local anesthesia? ___________________ 6. (Women) Are you or could you be pregnant? Yes No 7. Do you drink alcohol? Yes No How much? ____________________________ 8. Do you smoke? Yes No How much? ____________________________ 9. Do you use sunscreen? Yes No 10. Have you ever had a blistering sunburn? Yes No 11. Do you have any changing lesions or moles? Yes No 12. Have you ever had an abnormal mole removed? Yes No If yes, when and where on your body? _____________________________________________________ 13. Do any 1st degree family members have seasonal allergies, asthma, or atopic dermatitis? Yes No If yes, who? ____________________________ 14. List any surgical procedures and approximate dates below: _____________________________________________________ _____________________________________________________ 15. What is your occupation? _____________________________________________________ Circle any conditions you currently have or have had in the past: AIDS/HIV Eczema or Atopic Dermatitis Anemia Environmental Allergies Arthritis/Joint Deformity Epilepsy Asthma Fainting Bleeding Disorder/Blood Thinners Glaucoma Bowel Problems Heart Attack Cancer, what type? _________________ Heart Disease Chest Pain Heart Murmur Chicken Pox High Blood Pressure Chronic Cough Hepatitis Depression Herpes/Cold Sores Diabetes High Cholesterol Irregular Heart Beat Kidney Disease Liver Disease Lupus Multiple Sclerosis Pacemaker Phlebitis Psoriasis Psychiatric Care Seizures Stroke Thyroid Problems List any other diseases or health conditions we should know about that are not included in the list above: _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ Medications currently taking (please include over the counter medications, supplements, vitamins, etc.) _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ Allergies to medications or latex: _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ Pharmacy Name and City: ________________________________________________ Pharmacy Phone: ___________________________________________