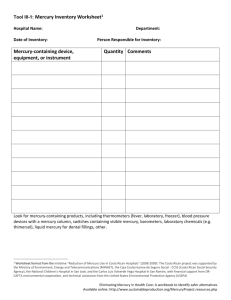
Chronic Mercury Poisoning and Mercury

From the Townsend Letter
June 2007
Chronic Mercury Poisoning and Mercury
Detoxification by Tom McGuire, DDS
Order this issue!
www.townsendletter.com
Introduction
Mercury is a neurotoxin and the most poisonous, non-radioactive, naturally occurring substance to which we can be exposed. Chronic mercury poisoning has reached pandemic proportions in the
United States and throughout the world. It will directly or indirectly cause, contribute or exacerbate every health issue known. The main cause: mercury amalgam (silver) fillings! It has been conclusively proven that mercury vapor is released from amalgams and stored in the body, and nearly 200 million people in the USA alone have these fillings. While the placement and safe removal of these toxic fillings is a dental issue, the effect caused by mercury vapor is a medical one.
My Position
I believe that chronic mercury poisoning is unquestionably underdiagnosed, and the enormity of this problem makes it imperative that every health professional understands how to diagnose and treat it. There is no doubt that unless the medical profession addresses the issue of chronic mercury poisoning and provides its patients with a sound and safe mercury detoxification program, any attempts to treat their patients' current health problems will not achieve the results desired by the practitioner and expected by the patients.
I've spent nearly ten years extensively researching chronic mercury poisoning, from its source and how it affects health to the safest, most effective, and most natural way to remove mercury from the body. The result is my newest book,
Mercury Detoxification: The Natural Way to Remove Mercury from Your Body . The book clearly explains how mercury affects the body, while guiding the reader through every step of the mercury detoxification process, including the following:
• testing for mercury;
• pharmaceutical chelators;
• intestinal and brain support;
• and the relationship of amalgam fillings to autism.
The book contains over 240 references and an extensive index and glossary. You can use it both for your own background knowledge and as an educational tool for your patients, taking advantage of my efforts without reinventing the wheel. Both the book and referenced abstracts are available on my website .
Because I believe it is so important to understand the need and value of a mercury detoxification program, I've chosen to provide you with some insights into the following:
• the reason we've become so mercury toxic;
• the primary source of mercury exposure;
• the ways in which mercury affects the body;
• and the need to educate yourself about mercury detoxification.
I hope this article will stimulate your concern, interest, and curiosity enough to learn more about what I consider one of the most significant and pervasive health problems of the twenty-first century: chronic mercury poisoning.
Brief History of Amalgam
Because amalgam fillings are the most common source of mercury exposure, I felt it would be worth knowing why they are still being used today and why you cannot count on the American Dental
Association (ADA) to educate the layperson, or the health professional, about the health hazards of these fillings. Amalgam was introduced in the early 1830s. It consisted of 50% silver filings and
50% elemental mercury. At that time, physicians also practiced dentistry, and because they knew mercury was a poison, the medical association banned its members from using it. But in those days, too, anyone could pull and fill teeth, and a number of the trades, referred to as "barber" dentists, began using amalgam. Because it was so inexpensive and easy to use, amalgam became very profitable for these "dentists." Seeing a significant revenue flow being lost to barber dentists, a group of doctor-dentists led a coup against the medical profession's ban on mercury. This took place in 1859 when they officially split from the medical profession and started their own association, the
American Dental Association.
What is the significance of the 1859 revolt? First, it legalized amalgam fillings. Second, it legitimized the right of dentists to poison their patients with mercury. From the beginning, the ADA denied mercury vapor was released from amalgams, but since such release has been conclusively proven, the ADA has finally acknowledged that fact. Yet instead of leading the effort to ban these toxic fillings, the ADA has taken a new, but indefensible position, by saying the amount of mercury released is so small that it doesn't constitute a health hazard. Once again, the ADA asks the public to trust it with their health.
What the ADA won't tell you is that mercury is far more poisonous than arsenic and lead; even one atom of mercury in the body is toxic. Simple logic dictates that because mercury vapor (80% of
which enters the body) is indeed released from amalgam fillings, such fillings should be deemed a health hazard and be banned immediately. (The irony is that 150 years ago, the medical profession considered it malpractice to place amalgams. Today, the ADA considers it malpractice to recommend their removal.)
The fact is that every patient you see who has amalgam fillings is mercury toxic to some degree. In the following sections, you'll learn how mercury is released from amalgam fillings and why so many people are being poisoned by it.
Amalgam Fillings and Chronic Mercury Poisoning
The amount of mercury vapor released from an amalgam filling is directly proportional to the temperature. In fact, heating the filling by such common actions as chewing, brushing your teeth, and drinking hot liquids can cause a significant release of mercury vapor. Other procedures can also dramatically increase the release of mercury vapor:
• when amalgams are placed into a cavity;
• when amalgams are removed;
• when amalgams are polished;
• when a gold crown is next to an amalgam filling;
• when you grind your teeth; and
• when teeth are cleaned.
Depending on the number of fillings present and the type and duration of filling stimulation, measurements of mercury vapor in the mouth can range from
36 mcg/m3 of air, when the filling is at rest, to over 4000 mcg/m3 ( see Table 1 ). The Agency for
Toxic Substances and Disease Registry (ATSDR) has set the minimal risk level (MRL) for continuous exposure to mercury vapor at 2.0 mcg/m3 of air per hour over a 24-hour period.
Table 1: Amount of Mercury Vapor Released from Amalgam Fillings
Chewing Food: 68 mcg/m3
Tooth Brushing: 272 mcg/m3
Placing an Amalgam: 2000 mcg/m3 or more
Removing an Amalgam: 4000 mcg/m3 or more
Polishing an Amalgam: 4000 mcg/m3
As you can imagine, it's possible for filling stimulation to take place throughout the day and during the night if one is a tooth-grinder (approximately 50% to 90% of the population). Mercury vapor will also continue to be released after stimulation for up to 90 minutes. Thus, everyone with amalgam fillings is being exposed to varying amounts of mercury daily, for as long as those fillings remain in the teeth.
Numerous other factors play a role in the amount of mercury vapor to which a person could be exposed and accumulate, and that amount will vary from person to person. For example, the amount
of mercury vapor released and absorbed by the above types of stimulation will be also be affected by the following:
• the number of fillings;
• the length of time they've been in the mouth;
• the size of the fillings;
• the frequency and duration of stimulation;
• the degree of the stimulation;
• and the health of the immune system.
For the majority of those with amalgam fillings, the total amount of mercury received from their fillings in a 24-hour period could easily surpass exposure limits set by every regulatory agency. The irony here is that regulatory agencies require that amalgam components be kept in a hazardous waste container in the dental office and also require that amalgam particles removed from teeth be kept in a hazardous waste container; then what would you consider a tooth with an amalgam filling in it?
Another important question the ADA has been asked, but has not answered, is, why must every business using mercury be monitored by regulatory agencies…except dentists?
Table 2 shows the
World Health Organization's (WHO) list of the main sources of mercury.
Table 2: The World Health Organization’s List of the Main Sources of Mercury
Source: Daily Intake of Mercury (mcg)
Amalgam Filling: 3.8 - 21
Fish: 3.0
Other Foods: 3.6
Water: 0.05
Air: 0.04
Yet in spite of the ever-increasing scientific evidence, the ADA continues to state that mercury amalgam fillings aren't a health hazard and insists that mercury isn't stored in the body. To them, it's a little mercury in and a little mercury out – with none left behind. Of course that is a ludicrous statement, and numerous tests for mercury have been used to prove that mercury does accumulate in the body.
The WHO has stated that there is no safe level of mercury and just one mcg of mercury contains approximately 43,00,000,000 atoms of it. (One gram of mercury, the amount found in just one large amalgam contains 1,000,000 micrograms – and that is a lot of mercury!) Dentists are also mercurytoxic, and their exposure to it could be even greater than those with amalgam fillings. Of note is that the dental profession in the USA places 100 million amalgam fillings a year and uses 34 tons of mercury in the process.
Depending on the amount of mercury that daily accumulates in the body, it can take a relatively long period of time before a related symptom appears. There are two primary reasons for this. The first is that the body is quite capable of removing mercury and other heavy metals, but that ability will
dramatically decrease over time if the exposure to mercury isn't eliminated. The second reason is because mercury is so ubiquitous. It spreads throughout the body and settles in every cell and tissue.
That means it can take years for enough to accumulate in any particular area of the body to generate an observable symptom. Of course, how quickly a symptom or symptoms will appear depends on the health of the immune system and the interaction and extent of the factors previously discussed.
It shouldn't be too difficult to see that even those with minimal exposure to mercury from their fillings are still receiving a substantial daily dose of mercury. In spite of the evidence, the ADA's position is that you aren't being poisoned until you express observable symptoms. As a health professional, you know that argument is utterly without merit. Every symptom related to chronic mercury poisoning has a threshold that must be reached before that symptom appears, but that doesn't mean you aren't being poisoned prior to reaching that point.
Other Important Factors to Consider
Space limits a detailed explanation of a number of other important issues relating to chronic mercury poisoning but, briefly, consider the following:
• The Direct and Indirect Effect of Mercury. Mercury poisoning is a double-edged sword. The direct damage is caused when mercury attaches to proteins and enzymes (anything with a sulfhydryl group is fair game), altering their function and ultimately killing cells. Indirectly it can severely weaken the immune system and significantly deplete the body's most essential antioxidant, glutathione
(GSH), weakening the body's ability to deal with other toxins and free radicals.
• Mercury Can't Be Detoxified by the Body. Everyone uses the term detoxification, including myself, but the fact is that mercury can't be "broken" down, and the body must physically remove it.
In the process, two molecules of glutathione are permanently lost for every atom of mercury that is removed and millions of atoms could be removed daily. This accounts for the depletion of glutathione.
• Mercury Doesn't Have a Half-Life. The fact is that mercury is not a radioactive substance and doesn't decay. It must be physically removed by a natural or pharmaceutical chelator.
The Long Reach of Mercury from Amalgam Fillings
Mercury released from amalgam fillings doesn't just affect those with the fillings. The fact is that the first time a person can be exposed to mercury from amalgam fillings is at the moment of conception.
Mercury readily passes through the placenta and enters the fetus, and if the mother has amalgam fillings, the fetus is being exposed to the mercury released from them.
The fetus doesn't have an immune system to protect it, and even small amounts of mercury will affect its development. The extent of the fetus's exposure to mercury will depend on how much mercury is released from the mother's fillings. Thus, it isn't difficult to imagine situations where the fetus is being exposed to enough mercury to cause, or certainly contribute to or make worse, every developmental and learning disorder, including autism. This is indeed something to seriously consider when anyone tells you that mercury amalgam (silver) fillings are not hazardous to health!
There's no doubt that mercury-containing vaccinations have played a significant role here, but vaccinations don't occur until after birth.
Summary
Here is what we know:
1. Mercury is an extraordinarily poisonous substance in very small amounts.
2. Even one atom will do some damage to the body.
3. Mercury is released from amalgam fillings, with the amount released and stored dependent on a number of factors.
4. Everyone who has, or had, these fillings is being poisoned daily by mercury.
5. The body has the ability to remove mercury, but unless the source is removed, it will become increasingly less effective at doing so.
6. Mercury accumulates in the body.
7. Mercury, because of its direct and indirect effects, can cause, contribute to, or make worse any health problem.
In closing, I chose to focus on chronic mercury poisoning instead of mercury detoxification because, unless you understand the extent and seriousness of this problem, I doubt you'd have much interest in a mercury detoxification program. However, once you do make the connection, all the information you need to know about detoxification can be found in my book.
I believe you owe it to yourself, and your patients, to at least consider the possibility that he or she could be suffering from chronic mercury poisoning. But you don't have to take my word for it. The fecal metals test is a very simple, at-home, inexpensive, and non-invasive test to diagnose chronic mercury poisoning in patients with amalgam fillings. (This test, available at Doctor's Data, and other tests for mercury are explained in my book.)
You now have an objective method of determining if your patient is mercury-toxic. If he or she is, the most obvious approach is to determine and eliminate the source of the mercury and implement a mercury detoxification program to support the body's efforts at removing it. My website, www.dentalwellness4u.com
, offers additional information on this subject and other oral health issues that can negatively affect overall health. My website also has the largest database of mercuryfree dentists, providing a referral source for your patients. I believe that diagnosing and treating mercury detoxification will benefit your practice and your patients. At the very least, I hope I've provided you some food for thought.
Correspondence
Tom McGuire, DDS www.dentalwellness4u.com
800-335-7755 dentwell@pacbell.net
Marie Flowe rs’ note: Just because a dentist’s name is on a list---whether it be the list from DAMS, the
IAOMT, or Dr. McGuire’s web site, does not make him safe. It is up to you to study the protocols for the safe removal of mercury fillings, interview the dentist and see if he is following the protocols.
For dentists that are listed at www.iaomt.org, Dr. David Kennedy recommends that you call Kym at the
IAOMT to see if the dentist is certified.
Some dentists listed on the IAOMT web site have only recently joined and may not yet have attended all the classes. www.MercuryPoisoned.com
References
Health, General
Crinnion WJ. Environmental medicine, part three: long-term effects of chronic low-dose mercury exposure. Altern Med Rev. 2000 Jun; 5(3):209-23.
Hanson M, et al. The dental amalgam issue. A review. Experientia . 1991 Jan 15; 47(1): 9-22.
Lindh U, et al. Removal of dental amalgam and other metal alloys supported by antioxidant therapy alleviates symptoms and improves quality of life in patients with amalgam-associated ill health.
Neuroendocrinol Lett.
2002 Oct-Dec; 23(5-6):459-82.
Immune System, Autoimmune, and Allergy
Bagenstose LM, et al. Murine mercury-induced autoimmunity: a model of chemically related autoimmunity in humans.
Immunol Res . 1999; 20(1):67-78.
Bartova J, Prochazkova J, Kratka Z, Benetkova K, Venclikova Z, Sterzl I. Dental amalgam as one of the risk factors in autoimmune diseases. Neuroendocrinol Lett.
2003 Feb-Apr; 24(1-2):65-7.
Hultman P, et al. Adverse immunological effects and autoimmunity induced by dental amalgam and alloy in mice. FASEB J . 1994 Nov; 8(14):1183-90.
Infertility and Birth Defects
Cordier S, Deplan F, Mandereau L, Hemon D. Paternal exposure to mercury and spontaneous abortions. Br J Ind Med. 1991 Jun; 48(6):375-81.
Gerhard I, et al. Heavy metals and fertility. J Toxicol Environ Health A . 1998 Aug 21; 54(8):593-
611.
Gerhard I, et al. Impact of heavy metals on hormonal and immunological factors in women with repeated miscarriages. Hum Reprod Update . 1998 May-Jun; 4(3):301-9.
Ziff S, et al. Infertility and Birth Defects: Is Mercury from Dental Fillings a Hidden Cause?
Bio-
Probe, Inc.; 1987. [ISBN: 0-941011-03-8.]
Intestinal
Barkay T, et al. Bacterial mercury resistance from atoms to ecosystems.
FEMS Microbiol Rev . 2003
Jun; 27(2-3):355-84.
Heintze U, et al. Methylation of mercury from dental amalgam and mercuric chloride by oral streptococci in vitro. Scand J Dent Res.
1983 Apr; 91(2):150-2.
Rowland I, Davies M, Grasso P. Biosynthesis of methylmercury compounds by the intestinal flora of the rat. Arch Environ Health.
1977 Jan-Feb; 32(1):24-8.
Rowland IR, et al. The methylation of mercuric chloride by human intestinal bacteria. Experientia.
1975 Sept 15; 31(9):1064-5.
Yannai S, et al. Transformations of inorganic mercury by Candida albicans and Saccharomyces cerevisiae. Appl Environ Microbiol.
1991 Jan; 57(1):245-7.
Relationship to Amalgam Fillings
Malmström C, et al. Conference on Trace Elements in Health and Disease. Stockholm May 25,
1992.
Nylander M, et al. Mercury concentrations in the human brain and kidneys in relation to exposure from dental amalgam fillings. Swed Dent J.
1987; 11(5):179-87.
Sandborgh-Englund G, et al. Mercury in biological fluids after amalgam removal.
J Dent Res.
1998
Apr; 77(4):615-24.
Weiner JA, et al. Does mercury from amalgam restorations constitute a health hazard? Sci Total
Environ . 1990 Dec 1; 99(1-2):1-22.
Release of Mercury
Aposhian HV, et al. Urinary mercury after administration of 2, 3-dimercaptopropane-1-sulfonic acid: correlation with dental amalgam score. FASEB J.
1992 Apr; 6(7):2472-6.
Begerow J, et al. Long-term mercury excretion in urine after removal of amalgam fillings. Int Arch
Occup Environ Health.
1994; 66(3):209-12.
Bjorkman L, et al. Mercury in saliva and feces after removal of amalgam fillings. Toxicol Appl
Pharmacol . 1997 May; 144(1):156-62.
Langworth S, et al. A case of high mercury exposure from dental amalgam. Eur J Oral Sci. 1996
Jun; 104(3):320-1.
Lorscheider, et al. Mercury exposure from silver tooth fillings. Emerging evidence questions a paradigm. FASEB J.
9:504-508, 1995.
Mahler DB, et al. Influence of liquid films on mercury vapor loss from dental amalgam. Dent Mater.
2002 Jul; 18(5):407-12.
Malmström C, et al. Silver amalgam: An unstable material. Danish Dental Journal.
Tidsskr. f. Tandlaeger. October 1989. [In Swedish] Hansson M, trans. Bio-Probe Newsletter.
Jan.1993;(1): 5-6.
Olsson S, et al. Model of mercury vapor transport from amalgam restorations in the oral cavity. J
Dent Res.
1989 Mar; 68(3): 504-8.
Pizzichini M, et al. Influence of amalgam fillings on Hg levels and total antioxidant activity in plasma of healthy donors. Sci Total Environ.
2003 Jan 1; 301(1-3):43-50.
Reinhardt JW. Side-effects: mercury contribution to body burden from dental amalgam. Adv Dent
Res.
1992 Sep; 6:110-3.
Skare I, et al. Human exposure to Hg and Ag released from dental amalgam restorations. Archives of
Environmental Health . 49(5): 384-394, 1994.
Toomvali C. Studies of mercury vapor in the oral cavity in relation to the number of amalgam fillings.
IFM-Kemi-EX 150. 1988.
Vimy MJ, et al. Intra-oral air mercury released from dental amalgam. J Dent Res . 1985 Aug;
64(8):1069-71.
Vimy MJ, et al. Serial measurements of intra-oral air mercury: estimation of daily dose from dental amalgam. J Dent Res . 1985 Aug; 64(8):1072-5.
Willershausen-Zonnchen B, et al. Mercury concentration in the mouth mucosa of patients with amalgam fillings. Dtsch Med Wochenschr.
1992 Nov 13; 117(46):1743-7.
Wolff M, et al. Mercury toxicity and dental amalgam. Neurotoxicology . 1983 Fall; 4(3):201-4.
Removal Protocol
Berglund A, et al. Mercury levels in plasma and urine after removal of all amalgam restorations: the effect of using rubber dams.
Dent Mater.
1997 Sep; 13(5):297-304.
Halbach S, et al. Steady-state transfer and depletion kinetics of mercury from amalgam fillings. Sci
Total Environ . 2000 Oct 2; 259(1-3):13-21.
Nimmo A, et al. Particulate inhalation during the removal of amalgam restorations.
J Prosthet Dent.
1990 Feb; 63(2):228-33.
Poiata A, et al. Mercury resistance among clinical isolates of Escherichia coli. Roum Arch Microbiol
Immunol.
2000 Jan-Jun; 59(1-2):71-9.
Summers AO, et al. Mercury released from dental "silver" fillings provokes an increase in mercury- and antibiotic-resistant bacteria in oral and intestinal floras of primates. Antimicrob Agents
Chemother.
1993 Apr; 37(4):825-34.
Resistance to Antibiotics
Edlund C, et al. Resistance of the normal human microflora to mercury and antimicrobials after exposure to mercury from dental amalgam fillings. Clin Infect Dis . 1996 Jun; 22(6):944-50.
Omura Y, et al. Role of mercury (Hg) in resistant infections & effective treatment of Chlamydia trachomatis and Herpes family viral infections (and potential treatment for cancer) by removing localized Hg deposits with Chinese parsley and delivering effective antibiotics using various drug uptake enhancement methods. Acupunct Electrother Res.
1995 Aug-Dec; 20(3-4):195-229.
Poiata A, et al. Mercury resistance among clinical isolates of Escherichia coli. Roum Arch Microbiol
Immunol.
2000 Jan-Jun; 59(1-2):71-9.
Summers AO, et al. Mercury released from dental "silver" fillings provokes an increase in mercury- and antibiotic-resistant bacteria in oral and intestinal floras of primates. Antimicrob Agents
Chemother . 1993 Apr; 37(4):825-34.
Supplements/Nutrition/Exercise
Andersen HR, et al. Effects of dietary alpha-tocopherol and beta-carotene on lipid peroxidation induced by methyl mercuric chloride in mice. Pharmacol Toxicol . 1993 Oct; 73(4):192-201.
Badmaev V, et al. Selenium: a quest for better understanding. Altern Ther Health Med . 1996 Jul;
2(4):59-62, 65-7.
Bapu C, et al. Fluctuation of trace elements during methylmercury toxication and chelation therapy.
Hum Exp Toxicol.
1994 Dec; 13(12):815-23.
Bapu C, et al. Restoration of methylmercury inhibited adenosine triphosphatases during vitamin and monothiol therapy. J Environ Pathol Toxicol Oncol . 1998; 17(1):75-80.
Biesalski HK, et al. Antioxidants in nutrition and their importance in the anti-/oxidative balance in the immune system. Immun Infekt. 1995 Oct; 23(5):166-73.
Bounous G, et al. Biological activity of undenatured dietary whey proteins: role of glutathione. Clin
Invest Med . 1991 Aug; 14(4):296-309.
Goyer RA. Nutrition and metal toxicity. Am J Clin Nutr . 1995 Mar; 61(3 Suppl):646S-650S.
Lovejoy HB, et al. Mercury exposure evaluations and their correlation with urine mercury excretion:
4. Elimination of mercury by sweating.
J Occup Med.
1973;15:590-591.
Rao MV, et al. Role of ascorbic acid on mercuric chloride-induced genotoxicity in human blood cultures. Toxicol In Vitro . 2001 Dec; 15(6):649-54.
Symptoms
Bailer J, et al. Adverse health effects related to mercury exposure from dental amalgam fillings: toxicological or psychological causes? Psychol Med . 2001 Feb; 31(2):255-63.
Clarkson TW. Mercury: major issues in environmental health. Environ Health Perspect . 1993 Apr;
100:31-8.
Hanson M. ABC on Mercury-Poisoning from Dental Amalgam Fillings. Handbook for victims of mercury-poisoning from dental amalgam.
Swedish Association of Dental Mercury Patients. Nov
1993.
Langauer-Lewowicka H, et al. Changes in the nervous system due to occupational metallic mercury poisoning. Neurol Neurochir Pol.
1997 Sep-Oct;31(5):905-13.
Lichtenberg H. Mercury vapour in the oral cavity in relation to the number of amalgam surfaces and the classic symptoms.
Journal of Orthomolecular Medicine . 1996;11(2): 87-94.
Malt UF, et al. Physical and mental problems attributed to dental amalgam fillings: a descriptive study of 99 self-referred patients compared with 272 controls. Psychosom Med.
1997 Jan-
Feb;59(1):32-41.
Siblerud RL. Relationship between mercury from dental amalgam and health. Toxic Substances
Journal.
1990;10:425-444.
Symptoms Improvement after Amalgam Removal
Eijkman MA, et al. Amalgam. XII. Amalgam removed and patient cured. Ned Tijdschr Tandheelkd .
1994 Feb; 101(2):50-3.
Jones L. Dental Amalgam and Health Experience: Exploring Health Outcomes and Issues for People
Medically Diagnosed with Mercury Poisoning. The Bulletin of the New Zealand Psychological
Society . 1999; 97: 29-33.
Kidd RF. Results of dental amalgam removal and mercury detoxification using DMPS and neural therapy. Altern Ther Health Med.
2000 Jul; 6(4):49-55.
Lichtenberg HJ. Elimination of symptoms by removal of dental amalgam from mercury poisoned patients, as compared with a control group of average patients.
J of Orthomolecular Med .
1993;8:145-148.
Lichtenberg HJ. Symptoms before and after proper amalagam removal in relation to serum-globulin reaction to metals. Orthomolec Med . 1996:11:195-204.
Siblerud RL.Relationship between mercury from dental amalgam and mental health. Am J
Psychother.
1989 Oct; 43(4):575-87.
Lindh U, et al. Removal of dental amalgam and other metal alloys supported by antioxidant therapy alleviates symptoms and improves quality of life in patients with amalgam-associated ill health.
Neuroendocrinol Lett.
2002 Oct-Dec; 23(5-6):459-82.
Ziff S. Consolidated symptoms of 1, 569 patients. Bio-Probe Newsletter.
March 1993; 9:2.
Testing
Apostoli P, et al. Significance of biological indicators of mercury exposure. Med Lav . 2003 Mar-
Apr; 94(2):231-41.
Bass DA, et al. Trace element analysis in hair: factors determining accuracy, precision, and reliability. Altern Med Rev . 2001 Oct; 6(5):472-81.
Crinnion WJ. Environmental medicine, part three: long-term effects of chronic low-dose mercury exposure. Altern Med Rev.
2000 Jun;5(3):209-23.
Hanson M, et al. The dental amalgam issue. A review. Experientia . 1991 Jan 15; 47(1):9-22.
Kazantzis G. Mercury exposure and early effects: an overview. Med Lav . 2002 May-Jun; 93(3):139-
47.
Lorscheider FL, et al. Mercury exposure from "silver" tooth fillings: emerging evidence questions a traditional dental paradigm. FASEB J . 1995 Apr; 9(7): 504•8.
WHO: No Safe Level of Hg
World Health Organization (WHO), Environmental Health Criteria 118: Inorganic Mercury.
1991;
28-33, 84-113.
Page 1 , 2 , 3