Bariatric surgery

BODY CONTOURING SURGERY AFTER MASSIVE WEIGHT LOSS
Fat Physiology
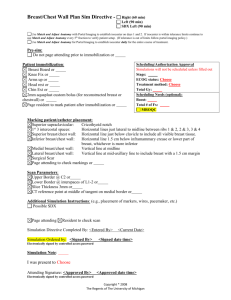
Classification of Obesity
Non Obese
Obese
Morbid obesity
BMI (wt
<18
18-24.9
25-29.9
30-34.9
35-39.9
40-49.9
>50
ht 2 ) Classification
Underweight
Normal
Overweight
Class 1 obesity
Class 2 Obesity
Class 3 Obesity
Super Obese
Epidemiology
Complex interplay of psychological, environmental, social, economic, geographic, cultural and genetic influences
65% of adults in US overweight, 30% obese, 4.7% severely obese.
Medical Issues
Weight gain of 5-8 kg is associated with a 2x increase risk of Type 2 DM
Incidence of heart disease is increased if BMI>25
Hypertension is 2x more common in obese
For every 1kg increase in weight, risk of arthritis increases by 10%
Reflux oesophagitis, Gallstones, Cholecystitis and cholelithiasis
Gout, osteoarthritis
Obstructive sleep apnea and respiratory problems
Malignancies - endometrial, breast, prostate, and colon cancer
Complications of pregnancy
Poor female reproductive health (such as menstrual irregularities, infertility, and irregular ovulation)
Stress incontinence, Uric acid nephrolithiasis
Psychological disorders (such as depression, eating disorders, distorted body image, and low self-esteem)
Bariatric Surgery
Indications (American college of physicians; Ann Internal Med 2005)
1.
BMI>40 who have failed diet and exercise, with or without the use of adjunctive drug therapy.
2.
BMI>35 with obesity related complications
Benefits of bariatric surgery (Buchwald JAMA 2004)
1.
Lipid disorders improved in 70% of patients
2.
Diabetes improved in 77%
3.
Hypertension improved in 78%
4.
Obstructive sleep apnoea improved in 86%
Weight Loss
Obesity difficulty to treat by conservative measures o First line remains diet and exercise o Limited benefit of pharmaceutical agents
Bariatric surgery is the only method capable of achieving significant weight loss with improvement of comorbidities
Liposuction has been shown not to have an effect on obesity-associated metabolic abnormalities (N Engl J Med. 2004 Jun)
Surgery
Types:
1.
malabsorptive a.
interrupt the digestive process b.
jejunal-ileal bypass – historical now c.
biliopancreatic diversion – most complex and induces the greatest degree of malabsorption. High side effects – nutritional deficiencies, foul smelling stools d.
Roux-en-Y gastric bypass – most common procedure
2.
restrictive a.
restrict food intake by altering size of stomach. b.
Weight loss slower than malabsorptive methods c.
vertical banded gastroplasty – avoids malabsorption but may cause reflux d.
adjustable gastric banding – reversible and long term adjustability
3.
combination a.
biliopancreatic diversion often combined with stomach reduction b.
gastric bypass
Despite massive weight loss, these patients differ physiologically from normal weight patients
They are at lifelong risk of anemia and other nutritional deficiencies
Physiology
Skin
Excess stretched skin with poor tone
Nutrition
With gastric bypass, anemia in 50%, vitamin/mineral deficiencies in 30-40%
Need daily supplement of multivitamins – especially folate and B12. o Folate absorbed in duodenum and proximal jejunum o B12 needs intrinsic factor from stomach, absorbed in ileum
B1(Thiamine) deficiency can cause Wernicke’s encephalopathy
Hypokalemia from diarrhea or vomiting
Hypocalcemia common
Low serum albumin may indicate severe malnutrition – may need TPN
Investigations
1.
FBC – monitor for anemia
2.
UEG
3.
Albumin
4.
Iron
5.
B12/folate
6.
APTT, INR
7.
fat soluble vitamins (A D E K)
8.
uric acid
Treat deficiencies with multivitamins
iron, folate
Adequate protein intake important for wound healing
Psychological
All patients should have a preoperative psych assessment o Impacts on outcome o Reduces postoperative anxiety o Some will benefit from psychotherapy and medications
Psychological screening tests include Eating Disorder Inventory, Beck Depression
Inventory, Minessota Multiphasic Personality Inventory
Although most will enjoy improvement in psychological indices, there is still a potential for difficulty in adjustment which may require ongoing psych care.
Defer surgery if patient has active psychiatric issues – wait until complete remission
Surgical Planning
Timing for Body Contouring Surgery
1.
Psychologically ready
Useful to refer patients to a nutritional counselor 2-3 months before surgery to give an added boost to weight loss and self image
2.
Stable weight
Stable weight for 3-6 months
Usually takes 12-18 months post bariatric surgery
Staging Surgery
In most cases, surgery should be multistaged, spaced at least 3 months apart
As a general rule, single-stage procedures of multiple body parts should be avoided. They expose the patient to prolonged operative times, increasing the likelihood of morbidities:
1.
hypothermia
2.
anemia
3.
thromboembolism
4.
wound-healing complications.
Sequence
Preoperative Evaluation
Fat distribution
Central/Peripheral/Diffuse/lipodystrophy
Android or Gynecoid
Tissue Deflation
Grades
1.
Deflated
2.
Mildly deflated
3.
Not deflated (minimal weight loss)
greater the drop in the body mass index, the greater the degree of tissue and skin laxity.
Most massive weight loss patients presenting for body contouring express interest in the lower trunk first. This is important because a lower body procedure (referred to as a lower body lift, belt lipectomy, or circumferential abdominoplasty) not only improves the lower trunk but also may have an effect on the thighs and back and, to a lesser degree, the chest.
In some male patients, a lower body procedure may have enough of an effect on the thighs and chest to negate the need for additional procedures.
Evaluation of anatomy
1.
Lower trunk a.
Old scars b.
degree of abdominal wall laxity c.
hernias d.
degree of rib flaring e.
extent of the buttock deformity [degree of ptosis and fat (lack of)]
2.
Upper trunk a.
Breast ptosis b.
Breast parenchyma amount c.
location of the inframammary fold d.
lateral inframammary fold usually displaced inferiorly e.
autoaugmentation or breast implants may be used to enhance shape and restore volume. Regardless of the technique, skin envelope reduction is a key component in shaping the female breast. Correction of the female breast deformity in massive weight loss patients is difficult, and residual deformities or recurrent ptosis is common. Some degree of asymmetry almost always occurs, and more than one procedure is frequently required to achieve an acceptable result
3.
Thighs a.
Often, a lower body procedure can have a positive effect on the thighs, most commonly the proximal anterior and lateral thigh b.
Determine the amount and location of excess skin. Most patients require a vertical excision with some horizontal component.
4.
Face a.
In general, the face of the massive weight loss patient ages prematurely b.
patients tend to lose more volume in the midface, and their skin is more lax and less elastic than the skin of non-massive weight loss patients. c.
In addition, patients may present with a marked excess of laxity in the neck region, with bowing and laxity of the submental angle that is significantly more pronounced compared with the non-massive weight loss patient d.
typically require more aggressive skin resection and volume augmentation.
The loss of volume can be addressed with techniques that incorporate shifting of the superficial musculoaponeurotic system or other techniques, such as autologous fat grafting. Conversely, some of the newer, longer-acting fillers may be an option for some patients.
Operative considerations
Staging liposuction safer - During liposuction at same time as lower body lift may complicate the procedure as significant oedema will compromise results and scars, with potential to complicate vascularity.
Techniques
Lower Body Contouring
Lower body lifts treats the lower trunk and thighs as a unit
Belt lipectomy will create a more defined waist with less impact on the thighs
Surgical goals
1. Flatten the abdomen
2. Recreate the umbilicus
3. Elevate the mons
4. Create a waist in females
5. Excision or liposuction of lower back rolls
6. Defining the buttocks (project, reshape or reduce)
7. Lifting the outer/anterior thighs
8. Improving the inner thighs
Markings
Mark patient slightly flexed at the waist standing up
Failure to mark the patient in this position may create undue tension, which can result in dehiscence.
The posterior aspect is usually marked first.
An estimation of where the scar will lie is based on the patient's anatomy as well as the degree of laxity on the lower thorax.
The upper marks tend to be convex, following the buttocks subunit, and are placed around the level of the posterior iliac crest. The degree of tissue laxity above the incision needs to be taken into account when determining the uppermost portion of the resection. Using a pinch test, the buttock and lateral thigh are serially mobilized up to the superior level mark to determine the inferior incision.
The majority of mobilization is going to come from below, with the upper incision being relatively fixed.
Ptosis of the mons is addressed first.
The mons is lifted vertically and the proposed incision is marked at the level of the pubic bone, generally 7 cm above the introitus.
The anterior lateral thigh skin is then mobilized up and onto the anterior superior iliac spine. The incision line in the pubic area extends laterally toward the anterior superior iliac spine.
With an upward and inward pull, this line is communicated laterally with the
(previously marked) posterior markings.
Patient positioning
Prone-supine or supine to lateral decubitus
Reduce risk of seroma by leaving a gliding layer of fat on the fascia and minimize diathermy use
important to abduct the legs to maximize the lateral take-out.
Gluteal Augmentation
deflated buttocks that look unnaturally flat and lack shape and definition.
A circumferential body lift can cause further flattening as the buttock skin is raised.
These patients can benefit from augmentation, which produces a more natural and aesthetically pleasing shape.
options for gluteal augmentation include
1. autologous augmentation
gluteal skin flaps, which is marked before surgery, is de-epithelialized and the tissue to be used for autoaugmentation is dissected and mobilized
2. fat transfer
3. implants
Silicone implants have been associated with less than optimal outcomes because of palpability and a greater risk of infection and dehiscence.
Mons reduction
when excess skin is present, a certain amount of the mons should be removed, in a vertical direction.
Ideally, the incision should lie at or just above the level of the pubic bone, with the mons pubis elevated to its proper position and then extended laterally.
important that the incision not be too low, as this could interfere with the lymph drainage system and/or innervation .
care should be taken so that the mons is not pulled too high, which may result in an alteration of the position of the clitoris and/or urethral meatus.
Umbilicoplasty
An abdomen that is too tight can interfere with healing at the umbilicus, because the excess tension can contribute to the development of skin dehiscence in this area or below it.
smaller is better when it comes to the umbilicus.
avoidance of a concentric circle diminishes the chance of the scar forming a concentric ring that contracts.
In patients with a stalk that is too long or too short or associated with a hernia, a neo-umbilical reconstruction may be considered, delayed or primarily
Closure
3 point closure – superficial fascia sutured to deep fascia
May cause nerve entrapment
Upper Body Lifts
consider breasts, lateral chest, and upper back. For procedures in the upper body, perform lower body surgery first, as these procedures affect the degree of work required for good aesthetic outcomes in the upper body.
In selected patients, liposuction can be an important first step for upper- and midback rolls
Excessive skin in the arms can affect the type of procedure that will be performed on both the anterior and posterior upper chest. The upper arm, lateral chest, and
breasts are intimately related, and in general, all require contouring for adequate rejuvenation of this area.
The surgeon may elect to address the upper torso (arms, back, and breasts) all in one stage or in several stages, treating either the breasts or arms first and completing the remaining area in a subsequent surgery.
Goals
2. To reshape/augment breast parenchyma to restore projection and fullness
3. To achieve appropriate nipple-areola complex position and size
4. To recreate/reposition the inframammary fold
5. To reduce the skin envelope
6. To eliminate prominent axillary skin rolls
7. To elimination mid- and upper-back rolls
Breast Reshaping
Breast deformity in these patients is much greater and more technically challenging than in non-massive weight loss patients.
Beyond the typical breast changes of glandular tissue loss and ptosis, there tends to be more asymmetrical volume loss in the massive weight loss breast, and there is more of a deflated and flat appearance of the breast.
Skin laxity is very apparent, and the degree of excess skin can be significant.
Most of these patients have grade III ptosis.
often present with prominent axillary skin or a fatty roll that usually continues well into the back.
suspending the breast tissue to the chest wall with sutures is helpful in shaping the breast. Good pillar closure helps support the breast and its new shape.
Relying on skin support to maintain shape in this or any patient group results in a loss of shape over time.
Aim for o Elimination of the horizontal and vertical excess o Recreation of the inframammary fold in its correct position o Adequate symmetry and nipple position o Good projection with superior fullness o Good lateral curvature of the breast
Options o mastopexy/augmentation in one stage
requires experience and a degree of expertise
Implant position can be difficult to control, and descent is common
in combination with significant transposition of the nipple-areola complex decreases vascularity and increases the risk for healing problems. o staged mastopexy and augmentation
Male breast
Nearly all morbidly obese men have some degree of breast hypertrophy, which is a result of both glandular and fatty tissue. Fatty tissue normally accumulates along the chest, flanks, and upper back in men.
After weight loss, there is a loss of definition of the inframammary fold, lateral chest wall bulkiness, excessive skin, breast ptosis, and, in some cases, excessive breast projection
As a general rule, the male nipple-areola complex is closer to the inframammary fold and just lateral to the breast meridian
critical that the patient have a realistic understanding of the scars that may be required to achieve the desired outcome.
Inverted-T mastopexy with extension toward the flank. This approach offers control of the nipple-areola complex, but the anterior chest scars are more obvious.
In cases where the inverted T will lead to an excessively long pedicle, which can create the potential for inadequate circulation or bulkiness of the central chest, a free nipple graft may be done with a horizontal skin excision
Lateral chest wall/Axilla
lateral chest wall excision usually done after the breast procedure.
It should be noted that this could affect the vascularity of the abdominal wall flap
(via Zone III – intercostals); therefore, lateral chest wall excision should not be performed with a lower body lift
Transverse Back excision
In women, mark in line with the bra strap
With the patient's arms up, the intended line of closure is marked (between the upper and lower outline of the brassiere), extending to the lateral chest wall
Arms
Rarely is liposuction effective alone
Patients must understand that these scars are longer and visible and may stay thick and heavy for a prolonged period of time
Photographs are imperative when discussing brachioplasty outcomes. Patients must be willing to accept the scar trade-off to have a more aesthetically pleasing shape and contour
Deformity can cross the axilla to the lateral chest wall and is often accompanied by lateral breast rolls.
Short scars cannot address distal skin laxity and have limited utility in the massive weight loss patient.
Most often, the incision has to extend onto the lateral chest wall proximally and to the level of the elbow distally
Most place scars at the bicipital groove others place it more posteriorly
Concurrent liposuction with resection is more problematic here than in the lower limb with respect to oedema
Positioning
Most commonly, the arms are abducted at 90 degrees and maintained on arm boards.
some have found that suspending the arms above the head allows unimpeded movement of arm skin and a more significant improvement in skin resection. In addition, the arms are elevated, which helps facilitate lymph drainage. When the arms are suspended, care should be taken to ensure that there is no stress on the brachial plexus, by securing the forearms
Method
Traditional T incision o difficult to remove the skin redundancy in the axilla, due to the excessive amount of skin between the anterior and posterior folds, without scars that are too visible. o At the transition between the middle and distal thirds of the arm , more fat should be maintained on the deep fascia and care should be taken to identify the medial antebrachial cutaneous nerve as it exits the deep fascia, often with the basilic vein o If the excision crosses the axilla, a Z-plasty should be performed to prevent scar retraction and axillary banding.
Thighs
thighs are one of the more difficult areas to contour.
characterized by poor skin tone and laxity. It collapses inferiorly in the anterior thigh and inferior medially in the medial thigh.
Lower body lift procedures often have a beneficial effect on the thighs, especially the lateral thigh and the proximal anterior thigh.
Because of this potential positive benefit, best to leave final thigh shaping until the result of the circumferential body lift is stable
Liposuction is an important adjunct here
Horizontal vs Vertical Resection
traditional Lockwood horizontal excision does not address the excess circumferential tissue found in most massive weight loss patients.
A vertical excision will address the circumferential laxity better with the disadvantage of a visible scar.
A vertical excision alone will not lead to vulval distortion
Markings
Mark with thighs flexed and knees abducted
Vertical component – posterior line 2-3 fingerbreadths behind the adductor longus tendon to the knee.
Method
depth of dissection anterior to the adductor magnus muscle should extend to the superficial or subcutaneous fat to avoid injury to the lymphatic system.
Posterior to this muscle, the dissection along the perineal crease should be at the level of the underlying muscle fascia. At that point, Colles fascia should be visible in the crease, and distal undermining of 4 to 5 cm along the thigh perineal crease is completed.
One of the most important elements in good closure during thigh procedures is to create low tension at the thigh perineal junction ;
excess tension can result in dehiscence and/or vulvar distortion. Abducting the thighs during the procedure helps ensure that this is accomplished.
Face
face is usually the last region to be addressed.
Volume loss is a normal part of facial aging, and this process becomes even more profound as these patients shed weight, producing a gaunt appearance.
Areas of concern include excessive facial fat atrophy, neck lipodystrophy, redundant skin/superficial musculoaponeurotic system, and loss of facial shape/elasticity
Other Considerations
Preoperative
Thorough evaluation by endocrinologist and anesthetists
Intraoperative
Intubation o may have increased risk of reflux
Hypothermia o Large area exposed o Warm theatre, warm fluids, cover areas not being operated on, warming blankets
IV Lines o Coordinate with anesthetist to see which limb can be used
Patient positioning o Shoulders: support to prevent shoulder subluxation, brachial plexus traction o Hip: Support iliac crest o Arms: pad elbows to protect ulnar nerve o Fave: protect eyes and cervical spine
DVT prophylaxis o Mechanical compression before induction o Heparin may be given 30-60minutes before induction in high risk patients ( no risk data on this subset of patients)
Postoperative Protocol
Most use short term steroids to reduce swelling, postop pain and postop nausea and vomiting
Some use diretics in cases of severe swelling
Compression garments o Most do not use for the arm as bleeding rare o Use of binders may compromise flap vascularity or increase abdominal pressure
Complications
1.
Bleeding
2.
Infection
3.
Seroma i.
Up to 50% incidence ii.
Reduce by a.
Leave a layer of fat on fascia b.
Eliminate dead space – 3 point suturing c.
Use multiple drains d.
Progressive tension sutures e.
1-2 ampules of doxycycline as an irritant infused through the drains f.
Fibrin sealants
4.
Wound breakdown/dehiscence
5.
Skin discoloration
6.
Swelling
7.
Fat necrosis
8.
Lymphocoele, lymphedema i.
Avoid with superficial dissection near the groin/axilla
9.
Damage to deeper structures
10.
Change in skin sensation
11.
Neuroma
12.
Vulval distortion
13.
Pubic distortion
14.
Nipple i.
Necrosis ii.
Malposition iii.
Scarring
15.
Umbilical i.
Necrosis ii.
Malposition iii.
Scarring
16.
Scarring
17.
Contour irregularites
18.
Over/Undercorrection
19.
Asymmetry
20.
DVT/PE