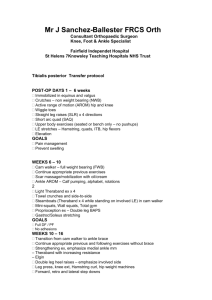
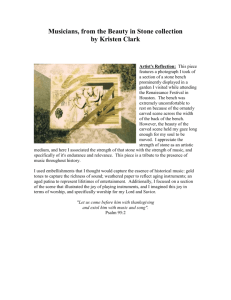
Heart Rate Recovery and Strength 1 Journal of Exercise Physiologyonline (JEPonline) Volume 13 Number 2 April 2010 Managing Editor Tommy Boone, PhD, MPH Editor-in-Chief Jon K. Linderman, PhD Review Board Todd Astorino, PhD Julien Baker, PhD Tommy Boone, PhD Eric Goulet, PhD Robert Gotshall, PhD Alexander Hutchison, PhD M. Knight-Maloney, PhD Len Kravitz, PhD James Laskin, PhD Derek Marks, PhD Cristine Mermier, PhD Chantal Vella, PhD Ben Zhou, PhD Official Research Journal of the American Society of Exercise Physiologists (ASEP) ISSN 1097-975 Fitness and Training Heart Rate Recovery Following Strength Exercise GEORGE VIEIRA1, ADRIANO EDUARDO LIMA-SILVA2, FERNANDO ROBERTO DE-OLIVEIRA3 1Physical Effort Laboratory/CDS/ Federal University of Santa Catarina, Florianópolis, Santa Catarina, Brazil, 2Sports Science Research Group, Federal University of Alagoas, Maceió, Brazil, 3Nemoh/ Federal University of Lavras, Lavras, Minas Gerais, Brazil ABSTRACT Vieira G, Lima-Silva AE, De-Oliveira FR. Heart Rate Recovery Following Strength Exercise. JEPonline 2010;13(2):1-9. The aim of this study was to analyze the effects of intensity, type of exercise, and gender on kinetics of heart rate (HR) recovery. Six men and six women (22.7 ± 2.1 years, 171.9 ± 10.9 cm, 66.3 ± 11.8 kg) performed two tests of 1RM in the leg press and bench press. After at least a 24-h period, the subjects performed a set until exhaustion at 80% of 1RM in bench press or leg press (in random order), followed by a 5-min recovery and then another set of the same exercise at 60% of 1RM. After five minutes, the subjects performed the same sequence in the opposite exercise. The values of HR (bpm) were mathematically adjusted, and the following variables were obtained: speed (τ) and amplitude (Amp) of decay, and HR at stabilization (HRbase). The HRbase was higher in leg press than in bench press (92 ± 18 vs 81 ± 18 bpm), with a tendency of the changes in HRbase being dependent on gender (bench press female= 85 ± 22 and male= 76 ± 12 bpm vs leg press female= 87 ± 21 and male= 97 ± 13 bpm, p=0.09). The Amp was similar for all intensities, exercises, and gender. The τ changed significantly with the type of exercise and gender (bench press female= 31.7 ± 14.6 and male= 62.3 ± 31.3 vs leg press female= 61.1 ± 17.6 and male= 53.9 ± 16.0 s, p<0.05). The intensity showed no significant effect on any of the studied variables. These results suggest that HR recovery is influenced by the type of exercise and the magnitude of these changes is dependent on the gender. Key Words: Upper Body Exercise, Lower Body Exercise, Cardiovascular Heart Rate Recovery and Strength 2 NTRODUCTION Resistance training has been the most effective method for development of muscular strength and it is currently prescribed by important health organizations to improve individual’s fitness and health (18). When incorporated into a comprehensive fitness program, resistance training has demonstrated to be able to reduce risk factors associated with coronary heart disease, non–insulin-dependent diabetes and to prevent lean body mass reduction caused by traditional exercise programs (4,18). Also, resistance training has become a common tool to prevent osteoporosis, functional incapacity and dynamic instability (18). The heart rate (HR) response to exercise allows noninvasive assessment of the behavior of the cardiovascular system during effort, as well as to determine the subjects’ fitness level. HR is easily monitored and can be used to control intensity of aerobic exercises (1). On the other hand, in strength exercises, the prescription and control of intensity are designed, mainly, for relative loads to onerepetition maximum (1RM) (11). However, this parameter does not provide the magnitude of stress caused to the cardiovascular system. The relationship between strength training and cardiovascular system responses has been recently explored (20) and can provide important information about the training intensity (12). The HR recovery is also a common used parameter to measure the cardiovascular fitness in aerobic exercises (5,9). Savin et al. (22) described the behavior of the HR after aerobic exercises and suggested that HR recovery decreases exponentially in two phases during short-term recovery. The first phase elicits a fast decay in HR (fast component) followed by a second phase of slower decay (slow component). The fast decay in HR observed after exercise could occur, mainly, due to the parasympathetic reactivation; and afterwards the reduction in HR would be attributed to the lowered sympathetic activity (2,9,14,24). Despite such evidence obtained in aerobic exercise, the behavior of HR after strength exercise is still little known. Different factors may provoke discrepancies in HR recovery including physiological and morphological differences between men and women (3), recruited muscle mass during exercise, differences between upper and lower limbs (20), and exercise intensity (10,21,23,25). The isolated or combined effects of these factors on HR recovery have not been extensively investigated. Therefore, the present study was designed to verify if there are differences in parameters derived from the HR recovery curve among different intensities, types of exercise, and gender. METHODS Subjects Twelve healthy subjects, six women (22.8 ± 2.8 years; 163.6 ± 6.3 cm; 57.5 ± 6.1 kg; 18.7 ± 4.3 % body fat) and six men (22.7 ± 1.6 years; 180.2 ± 7.6 cm; 75.2 ± 9.0 kg; 10.4 ± 1.8 % body fat), with experience in resistance training, were selected to participate in the study. All subjects signed an informed consent before initiating the tests. The adopted procedures were approved by the ethics committee of the Federal University of Santa Catarina. Procedures Initially, the subjects were submitted to anthropometric measurements to estimate the percentage of body fat. For women the skinfolds of triceps, suprailiac and thigh were measured and the body fat estimated by the Jackson, Pollock and Ward’s equation (16). For men the skinfolds of chest, abdomen and thigh were measured and body fat estimated by Jackson and Pollock’s equation (15). After the anthropometric measurements, the subjects performed two tests to determine 1RM (bench press and leg press, in random order). Before the tests a 10-min warm up was carried out and Heart Rate Recovery and Strength 3 consisted of a moderate running on a running track, followed by a specific warm up where it was allowed the execution of 1 set of 15 repetitions. After a 24-h period, the subjects returned to the laboratory and performed tests to obtain the highest number of repetitions until exhaustion (figure 1). The sequence was conducted at 80% and 60% of 1RM. This sequence was based on previous data obtained by Wilborn et al. (25) where it was demonstrated that cardiovascular stress was higher at 65% than 85% of 1RM. The execution of leg press vs bench press exercises were performed in random order. STAGE 1 STAGE 2 STAGE 3 Anthropometric measurements Tests of 1RM 24 hr Bench press Leg press Random Maximal number of repetitions assessment Bench press 80% 5-min recovery Bench press 60% 5-min recovery Random Leg press 80% 5-min recovery Leg press 60% 5-min recovery Figure 1. The Experimental Design. 1RM Tests The tests of 1RM were realized with the initial load established in accordance with the experience of the subject evaluated. The subjects were asked to execute a complete movement. In the cases where the subjects were able to execute two movements, a 5-min recovery period was permitted and the test was resumed with a greater load. A maximum number of three consecutive attempts were established to get the maximum load in each test. In case it was not possible to obtain the subjects’ maximum load, a change of exercise was permitted to alternate muscle groups and the maximum load of the other exercise was obtained. This last procedure was necessary for only one subject. Maximal Number of Repetitions Assessment The individuals were oriented to perform the movements in a moderate speed. All the sets were executed until exhaustion with 5-min interval between them. After each set of repetitions, the subjects remained laid on a bench in supine position during the five minutes. In all recovery intervals, the HR was measured at 5-sec intervals (Polar Electro Oy, S610i). The last value of heart rate obtained during the tests was referred as HRpeak. The number of repetitions (NR) was identified as being the total amount of exercise performed in each exercise. The total volume (TV) was calculated multiplying the weight by NR. Leg Press and Bench Press Exercises The execution of the exercises in our study followed the American College of Sports Medicine procedures and recommendations (17), regarding the use of the bench press to evaluate strength of arms, and leg press to evaluate strength of legs. Leg press tests were executed on a leg press machine (Vitally® mark, model ML209), and the bench press on a bench press machine (Vitally® mark, model ML206). Heart Rate Recovery and Strength 4 Data Analysis The values of HR (bpm) during the recovery phase were plotted against time (s) and adjusted with a mono-exponential function: HR = HRbase + Amp • exp - (t/τ) Where: HRbase is the HR at stabilization during the recovery; Amp is the amplitude decay of the HR; t is time for a given estimated HR value; τ is a time constant that represents the time necessary to reach 63% of the amplitude decay of the HR. The curves were adjusted to absolute (bpm) and relative values (%) of the HRpeak. Statistical Analysis Normal distribution of the data was checked by Shapiro-Wilk's test. A 3-way analysis of variance (factor 1 = intensity; factor 2 = type of exercise; and factor 3 = gender) followed by Scheffe’s post-hoc test were used for comparison among the variables derived from the monoexponencial adjustment (HRpeak, NR, and TV). Student’s t-Test for independent samples was used to compare 1RM between men and women, and Pearson’s linear correlation analysis for verification of associations between the variables. The values are presented as mean SD. Level of significance was established at p< 0.05 for all analyses. RESULTS The NR in the bench press exercise at 60% of 1RM did not show normal distribution and the comparisons that involved this variable were performed using a logarithmic scale conversion. The other variables were Table 1. Maximal load (1RM), maximal number of repetitions (NR), and total compared with original volume (TV) at 60% and 80% of 1RM in bench press and leg press exercises. values. Intensity Men Women Pooled Data 1RM –bench press (kg) 79.7 ± 12.5* 38.3 ± 7.5 59.0 ± 24.0 The maximum load, the NR, and TV of men 310.0 ± 71.5* 203.3 ± 43.2 257.0 ± 79.0 1RM –leg press (kg) and women in the two exercises are shown in 7±2 9±4 NR –bench press 80% 8 ± 4† Table 1. 1RM was 17 ± 3 23 ± 8 20 ± 7**,† NR –bench press 60% significantly different between the genders in 15 ± 10 16 ± 7 16 ± 9 NR –leg press 80% both exercises. The NR 28 ± 7 33 ± 11 30 ± 9** NR –leg press 60% for all intensities and types of exercise was 422.7 ± 160.2* 284.0 ± 151.1 TV –bench press 80% 353 ± 165† not significantly different between the 808.4 ± 207.1* 520.2 ± 164.0 664 ± 233**,† TV –bench press 60% genders, but women tended to perform 3562.7 ± 1908.7* 2606.7 ± 1196.8 3085 ± 1599 TV –leg press 80% higher NR than men 4998.0 ± 514.4* 3998.0 ± 1620.7 4498 ± 1260** TV –leg press 60% (p=0.09). The men performed a greater TV *Significant differences between men and women (p < 0.05). ** Significantly higher than the women for all than corresponding values at 80% of 1RM in the same exercise (p < 0.01). † intensities and types of Significantly lower than corresponding values in the leg press (p < 0.01). exercise (p= 0.047). The NR and TV were significantly higher in leg press than in bench press (p<0.05). The NR and TV were also higher in exercise performed at 60% than 80% of 1RM (p<0.05). Heart Rate Recovery and Strength 5 The HRbase was significantly higher in leg press (92 ± 18 bpm) than in bench press (81 ± 18 bpm) (p<0.05). There was a tendency for HRbase variations to be dependent on gender, with the interaction between gender and type of exercise near significance level (p=0.09). The women demonstrated greater values of HRbase in the bench press (85 ± 22 bpm) than the men (76 ± 12 bpm). On the other hand, in leg press, the highest values were showed by the men (97 ± 13 bpm) compared with the women (87 ± 21 bpm) (figure 2A). No significant effect of the intensity was found (p = 0.62). When expressed relative to the HRpeak, no significant effect of the type of exercise, gender, and intensity were found. The decrease in amplitude was similar for all the intensities, types of exercises, and gender whether expressed in absolute or relative values. The time constant (τ) modified significantly in accordance with the type of exercise, interacting with gender (interaction between the factors gender - type of exercise, p<0.05). In the bench press, the values were higher in men (62.3 ± 31.0 s) than in women (31.7 ± 14.6 s, p<0.05). However, the women showed greater values (61.1 ± 17.6 s) than the men (53.9 ± 16.0 s, p<0.05) in the leg press (figure 2B). The same behavior was found when using relative values. No significant effect of intensity was found (p = 0.37). The HRpeak was significantly higher in leg press (148 ± 17 bpm) than in bench press (126 ± 27 bpm) (p=0.002). The HRpeak was lower (in average 7%) during exercise at 80% compared to 60% of 1 RM for both exercises, but not reaching statistical significance (p=0.15) (figure 2C). No significant effect of gender was found (p = 0.30). 150 100 50 0 Bench press A Men Leg press Women 100 p<0.001 50 0 Bench press Leg press HRpeak (bpm) p=0.09 200 Time Constant (s) HRbase (bpm) Figure 2: HRbase (A), time constant (B) and HRpeak (C) in men and women after bench press and leg press at 60% and 80% of 1RM. 200 p<0.001 150 100 50 0 Bench press B Men Women C 60% of 1RM Leg press 80% of 1RM 1RM was positively associated with the time constant for all intensities and exercises (r values between 0.65 and 0.78; p<0.01). The TV was also positively correlated with the time constant in the bench press at 80% and 60% of 1RM (r= 0.78 and 0.86, respectively). The other derived variables of the HR recovery curve did not demonstrate significant associations with TV. The NR showed association with the HRbase only at 60% of 1RM in leg press and bench press (r= 0.68 and 0.64, respectively), and with the HRpeak in the bench press exercise at 80% of 1RM (r= 0.65; p<0.01). DISCUSSION The results of the present study indicate that HR recovery is influenced by both, type of exercise and gender. The HR stabilization was significantly higher after lower than upper body exercise but it may be gender dependent. The HR stabilization after upper body exercise was higher for women than men, but the opposite was observed when HR stabilization was measured after lower body exercise. Similarly, the time to attain stabilization after upper body exercise was significantly higher for men than women, but it was also the opposite of lower body exercise. In this study the HRpeak did not modify because of the intensity put on lower and upper body exercise. The total time of effort was not measured, however the NR and TV were greater at 60% of 1RM than Heart Rate Recovery and Strength 6 at 80% of 1RM in both exercises. Furthermore the results of this and other studies (10, 23, 25) indicate an existing peak zone for HR response during strength training between 50 and 80% of 1RM. Wilborn et al. (25) suggest that the higher increase in HR observed at lower intensities can be attributed mainly to the longer duration of effort. We established that HRpeak corresponded to the last value recorded during the exercise, even though this value did not always correspond to the greater value of HR. Despite of the latter, we did not find a significant difference between the greater value of HR during the test and the values of HR at the end of exercise (data not shown). These findings corroborate the results showed in others studies (10, 21, 19) demonstrating that the highest values of HR tend to occur at the final stage of strength exercises and, normally, occur in the complete repetition before the point of voluntary fatigue. It was expected since in strength exercises cardiovascular responses tend to raise when the muscles become fatigued, due to a combination of factors such as a greater voluntary effort of the fatigued muscles to continue generating the same strength and greater recruitment of accessory muscles (20, 21). Studies that have analyzed the HR recovery have adopted different recovery periods (24). In the present study, a 5-min recovery period was adopted. In a previous pilot study, we observed evidence that a 5-min recovery was enough to describe the behavior of the HR until its stabilization (HR base) in all the intensities, types of exercise, and gender used here. Moreover, in short-term recoveries such as the adopted in our study, the HR kinetics demonstrates to be well described by monoexponential adjustment (14,22). From a practical standpoint, it may be more interesting for coaches to measure HR recovery with short intervals. It was found in the present study that HRbase was higher in leg press than in bench press, suggesting that lower body exercise increase the HR of stabilization. Ichinose et al. (13) suggest that cardiovascular responses during dynamic and static exercises are mediated by some factors such as central command, feedback mechanisms via afferent nerves (group III and IV fibers), and arterial and cardiopulmonary baroreflexes. During heavy exercise, the arterial baroreflexes and muscle metaboreflexes are both activated regulating cardiovascular responses and sympathetic nerve activity. After strength exercises, the fast reduction in blood pressure can reflect on a rise in perfusion of vasodilated active muscle in combination with baroreflex response initialized during exercise (20, 21). Therefore, it is possible that the muscle mass recruited during exercise exerts an important function in the hypotension after exercise, and HR could rise as a compensatory mechanism to prevent acute reduction in blood pressure. This may explain the greater values of HRbase in the leg press than bench press. It was found in the present study greater values for HRpeak in the leg press, probably, due to the greater activated muscle mass and time of effort. Similarly, Imai et al. (14) indicated that the behavior of these cardiovascular variables could be explained by central mechanisms such as the release of inhibitory commands from the motor cortex to the parasympathetic center. On the other hand, at the end of exercise, there is an inhibition of the motor cortex followed by vagal reactivation preventing an excessive cardiovascular work after exercise. These data suggest that cardiovascular recovery is partially dependent on cardiovascular response during exercise. Moreover, afferent stimulation from peripheral chemoreceptor may justify a delayed sympathetic withdrawal and also contributing for maintenance of a higher HR after exercise. The differences in strength between men and women could be influenced by the type of exercise and the amount of recruited muscle mass. The women’s value for 1RM was at 48% of the men’s absolute value in bench press and at 66% for leg press. Ettinger et al. (8) verified that the muscle mass and the tension generated in a static exercise were lower in women than in men. Several Heart Rate Recovery and Strength 7 mechanisms mediate post-exercise recovery of the cardiovascular system, and these mechanisms can differently modulate men’s and women’s responses. There is evidence that women have lower tolerance to various orthostatic positions compared with men (6,7). The greater need for cardiovascular adjustment to oscillation in the body position observed in women may also help to explain, in part, the lower decreasing velocity of heart rate in the leg press. This may have occurred due to the change in body position after exercise (seated for supine position). The amplitude decay was similar between the types of exercise and intensities, supporting that HRpeak and HRbase exhibit a synchronous response to physical effort, which could also prevent acute post-exercise blood hypotension. However, the HRpeak demonstrated a significant association with the HRbase only at 80% in the bench press (r = 0.64, p<0.03) and in leg press (r = 0.84, p<0.01). Mcdougall et al. (21) suggest that the level of effort in strength exercises seems to be the most important factor for the rise in blood pressure during exercise. Therefore, higher intensities may unleash greater hypotensive effect after exercise and the heart rate may remain elevated during recovery to compensate for the sharp fall in arterial blood pressure. Thus, it is suggested that further investigations may determine the magnitude and influence the arterial pressure may exert on heart rate recovery and associated variables. CONCLUSIONS In conclusion, our observations demonstrate that the type of exercise is an important factor influencing HR responses during and after strength exercise. In addition, the HR recovery differences between leg press and bench press were strongly gender-dependent. Our results also suggest that HR during exercise is dependent on the intensity, but the same does not occur with HR recovery. In practical terms, we concluded that leg press have a higher HR response and these findings show the influence of muscle mass on the cardiovascular system; therefore if the objective of the strength exercise is to cause a lesser rise in HR then a lesser amount of muscle mass must be required. Address for correspondence: George Vieira, MSc. Servidão Marciano João da Silveira, 101. Florianópolis, Santa Catarina, Brasil, 88047-230. Phone (55) 0xx48-96022102; E-mail. george_vieira@hotmail.com. REFERENCES 1. Achten J and Jeukendrup AE. Heart rate monitoring: applications and limitations. Sports Med 2003;33(7):517-538. 2. Arai Y, Saul JP, Albrecht P, Howard HH, Lilly LS, Cohen RJ and Colucci WS. Modulation of cardiac autonomic activity during and immediately after exercise. Heart Cir Physiol 1989;25: 132-141. 3. Åstrand P and Rodahl K. Textbook of Work Physiology. New York: McGraw Hill, 1986. 4. Bjarnason-Wehrens B, Mayer-Berger W, Meister ER, Baum K, Hambrecht R and Gielen S. Recommendations for resistance exercise in cardiac rehabilitation. Recommendations of the german federation for cardiovascular prevention and rehabilitaton. Eur J Cardiovasc Prev Rehabil 2004;11(4):352-361. Heart Rate Recovery and Strength 8 5. Carnethon MR, Jacobs DR, Sidney S, Stenfeld B. Gidding SS, Shoushtari C and Liu K. A longitudinal study of physical activity and heart rate recovery: CARDIA, 1987 – 1993. Med Sci Sports Exerc 2005;37(4):606-612. 6. Carter III R, Watenpaugh DE and Smith ML. Selected contribution: Gender differences in cardiovascular regulation during recovery from exercise. J Appl Physiol 2001;91:1902-1907. 7. Convertino VA. Gender differences in autonomic functions associated with blood pressure regulation. J Appl Physiol 1998;44:R1909-R1920. 8. Ettinger SM, Silber DH, Collins BG, Gray KS, Sutliff G, Whisler SK, McClain JM, Smith MB, Yang QX and Sinoway LI. Influence of gender on sympathetic nerve responses to static exercise. J Appl Physiol 1996;80(1):245-251. 9. Fernandez TC, Adami F, Pereira Costa V, Lima Silva AE and De-Oliveira FR. Heart rate recovery as an index to aerobic aptitude. Revista da Educação Física/UEM. 2005;16(2):29137. 10. Fleck SJ and Dean LS. Resistance-training experience and the pressor response during resistance exercise. J Appl Physiol 1987;63(1):116-20. 11. Fleck SJ and Kraemer WJ. Designing resistance training programs. 2nd ed. Champaign (IL): Human Kinetics Books, 1997. 12. Hass CJ, Feigenbaum MS and Franklin BA. Prescription of resistance training for healthy populations. Sports Med 2001;31(14):953-964l. 13. Ichinose M, Saito M, Wada H, Kitano A, Kondo N, Nishiyasu T. Modulation of arterial baroreflex control of muscle sympathetic nerve activity by muscle metaboreflex in humans. Heart Circ Physiol 2004;286:701-707. 14. Imai K, Sato H, Hori M, Kusuoka H, Ozaki H, Yokoyama H, Takeda H, Inoue M and Kamada T. Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol 1994;24:1529-35. 15. Jackson AS and Pollock ML. Generalized equations for predicting body density of men. Br J Nutr 1978;40(3):497-504. 16. Jackson AS, Pollock ML and Ward A. Generalized equations for predicting body density of women. Med Sci Sports Exerc 1980;12(3):175-81. 17. Kenney WL, Mahler DA, Humphrey RH and Bryant CX. ACSM guidelines for exercise testing and prescription.Baltimore: Williams & Wilkins, 1995. 18. Kraemer WJ, Adams K, Cafarelli E,Dudley GA, Dooly C, Feigenbaum MS, Fleck SJ, Franklin B, Fry AC, Hoffman JR, Potteiger J, Stone MH, Ratamess NA, Triplett-McBride T. American College of Sports Medicine. Position stand on progression models in resistance training for healthy adults. Med Sci Sports Exerc 2002;34(2):364-380. Heart Rate Recovery and Strength 9 19. Mccartney N, Mcvelvie RS, Martin J, Sale DG and Mcdougall JD. Weight-training-induced attenuation of the circulatory response of older males to weight lifting. J Appl Physiol 1993, 74(3):1056-1060. 20. Mccartney N. Acute responses to resistance training and safety. Med Sci Sports Exerc 1999; 31(1):31-37. 21. Mcdougall JD, Tuxen D, Sale DG and Moroz JR. Arterial blood pressure response to heavy resistance exercise. J Appl Physiol 1985;58(3):785-790. 22. Savin WM, Davison, DM and Haskell WL. Autonomic contribution to heart rate recovery from exercise in humans. J Appl Physiol 1982;53(6):1572-1575. 23. Stone MH, Rozenek R, Rosenau L and Rosenau P. The effect of intensity on heart rate and blood lactate response to resistance exercise. J Strength Cond Res 1993;7(1):51-54. 24. Terziotti P, Shena F and Gulli G. Post-exercise recovery of autonomic cardiovascular control: a study by spectrum and cross-spectrum analysis in humans. Eur J Appl Physiol 2001;84:187194. 25. Wilborn C, Greenwood M, Wyatt F, Bowden R and Grose D. The effects of exercise intensity and body position on cardiovascular variables during resistance exercise. JEPonline 2004; 7(4):29-36. Disclaimer The opinions expressed in JEPonline are those of the authors and are not attributable to JEPonline, the editorial staff or ASEP.
 0
0
advertisement


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users