HYDRODYNAMIC THEORY OF DENTINAL PAIN PERCEPTION

HYDRODYNAMIC THEORY OF DENTINAL PAIN PERCEPTION
The pain sense in human teeth has some important differences from pain perception in other organs such as the skin: It is considered to be the only sensation which can be elicited by any stimulus applied to the teeth (excluding the periodontal receptors). Thus, there is no sense of warmth or cold, but only pain if the temperature exceeds certain limits - lower than 27 o C or higher than 45 o C (Matthews, 1977). While some authors have regarded the teeth as pressure-sensitive over a very high range of pressures, the most common sensation we usually experience is pain, whether with exposed dentin from enamel attrition or from a pulpal inflammation acting directly on nerve endings.
Distribution of Pain Sensitivity in Teeth
Most dental pain researchers agree on at least two things:
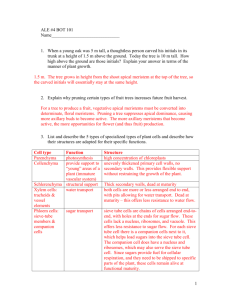
(1) the enamel of the teeth is completely insensitive, and (2) the dentin and pulp are sensitive to a variety of stimuli, including mechanical, thermal and chemical. The insensitivity of the enamel is not surprising, as that substance consists primarily of dry hydroxyapatite crystals with no demonstrable innervation. The pulp and dentin, on the other hand, are living structures which contain body fluids and identifiable nerve endings. One seemingly paradoxical finding is the sensitivity of the dentin-enamel junction; although no nerve endings can be seen in this region of the tooth, when the junction is inadvertently touched by a dental drill, the pain reaction can be sudden and severe.
Nerve Endings in Dentin
The sensory fibers in the pulp are branches of a plexus underlying the odontoblastic layer, the Plexus of Raschkow (Figure 1). The pulp nerves approach the horns of the pulp, then branch diffusely to form the plexus. Fibers arising from this network occasionally appear to cross the odontoblastic layer into the dentin.
There has been some controversy over the years about whether or not nerve endings are present in the dentinal tubules. From light microscopic observations, R.W. Fearnhead (1963) stated that,
"The question whether calcified dentin is innervated I now regard as settled. It is no longer a controversial topic. In suitable specimens nerve fibres can be demonstrated within the dentinal tubules". This is shown in the next two figures.
The histologist T. Arwill (1963), however, claimed that the fibers were located in the intertubular ground substance, and not in the tubules themselves. Two views of nerve fibers apparently crossing the dentinal tubules in the intertubular substance are shown in the next two figures.
With the advent of autoradiographic studies, researchers were able to study the distribution of trigeminal sensory branches.
Byers and Dong (1983) injected radioactive proline into the trigeminal ganglion and waited 20 hours until the isotope had been carried to the teeth by axoplasmic transport in sensory fibers.
Their radiographs clearly showed label reaching as much as 120 micrometers into the dentinal tubules, indicating the presence of sensory axons. Less than half the tubules showed the presence of label, but this was "hard" evidence of sensory endings in dentin.
Responses of Dental Pain Endings
D.S. Scott, in the 1960s, attempted to demonstrate the activity of nerves in the dentin directly, as shown in Figure 7, Part A.
Plastic tubes filled with conductive solutions were placed in freshly prepared cavities in the dentin of a cat's canine tooth.
Then heat was applied to the opposite side of the tooth, and the electrical responses recorded between the two electrodes, as shown in Part B.
the frequency of firing of nerve impulses increased. A small drop
When the temperature of the tooth was increased sufficiently, of acetylcholine applied to one of the cavities would produce a burst of impulses. And treatment of a cavity with acetylsalicylate would block the response to heating. (This was considered one of the early demonstrations of a peripheral analgesic action of aspirin.) Scott and others interpreted these findings as demonstrating unequivocally the presence of active nerve fibers in dentin.
At about the same time, a group in Sweden carried out a series of experiments which they believed to prove the active pain endings in teeth were not in the dentin, but in the pulp below the
predentin layer (Brännström, 1963; Brännström and Åström, 1964).
Using a premolar tooth about to be extracted for orthodontic reasons, they cut a groove around the cusp and broke it off, exposing fresh dentin. One observation was that the intertubular substance was a fluid, which beaded up on the dentin surface a few minutes after it was exposed.
This finding supports the theory that sensory endings are in the pulp: It is assumed that stimuli to the dentin which cause pain do so by movement of the tubular contents and the resulting displacement of nerve endings in the pulp. This is known as the hydrodynamic theory of dentinal pain perception. Some of the experiments which Brännström and co-workers did were: (1) Stimulating with a puff of air applied to the freshly exposed dentin resulted in a pain sensation.
(2) Drying the dentin for a few minutes with an airstream reduced the sensitivity to air puffs. (3) Application of dry filter paper to exposed dentin caused a pain sensation. (4) Application of filter paper soaked in isotonic potassium chloride, which is a potent nerve stimulator, did not cause pain.
These results were all interpreted to mean that no nerve fibers were present in the dentin. The results of Scott were explained by assuming that the nerve impulses he had recorded were electrically conducted from the pulp nerves to the electrodes by the conductive fluid in the tubules. Thermal stimuli were thought to produce movement of tubular contents because the coefficient of expansion of the fluid was much greater than that of the tubular
walls. As a kind of confirming experiment, Brännström (1963) applied suction to the exposed dentin and then extracted the tooth soon after and made a histological preparation as shown in Figure
9.
The tubular fluid was evidently so free to move that the negative pressure had caused odontoblastic nuclei to be sucked up into the tubules. The obvious conclusion was that with much less suction or positive pressure, the pulpal elements near the odontoblasts could be moved around significantly, disturbing the local nerve fibers.
The next piece in the puzzle came from Matthews (1970), who repeated Scott's experiments and then pushed the recording
electrodes further and further into the dentin cavities. The result was that, the closer the electrodes were to the pulp, the larger were the recorded action potentials in response to heating.
This indicated that the major source of nervous signals in the teeth was indeed in the pulp.
Confirming evidence of the hydrodynamic theory came from the work of Tal and Oron: A scanning electromicroscopic picture of freshly cut dentin, as shown in the next figure, reveals open dentinal tubules with Tomes' fibers protruding into the open space.
Topical fluoride, which is used as a treatment for abrasion hyperalgesia, resulted in the deposition of crystals within the dentinal tubules. It was assumed that part of the reduction of
pain with fluoride treatment was a result of this occlusion of the dentinal tubules. tubules is shown in Figure 12. Fibers from the plexus of Raschkow
A current summary of the innervation of the pulp and dentinal arise and innervate the spaces between odontoblasts, and some fibers do reach into the tubules, but only for 100 micrometers or so. Stimuli reaching the dentin may stimulate intratubular fibers, but also displace nerves in the pulp through hydrodynamic movement of the tubular fluid.
Interestingly, the hydrodynamic theory is able to account convincingly for the sensitivity of the dentin-enamel junction: If that junction is breached by a dental bur or other injury, the tubular fluid will be exposed to the outside pressure and undergo a sudden movement, causing excitation of sensory endings far from the enamel.
Innervation of the Teeth: Pain Sensory Pathways
From electronmicroscopic studies, it has been shown that pulp nerves in both feline and human teeth contain A and C fibers
(Beasley and Holland, 1978; Byers, 1984; Reader and Foreman,
1981). The C fibers include both afferents and sympathetic
postganglionic axons. The identification of A and C fibers by electrical stimulation of dentin near the tooth crown is shown in
Figure 13. Recordings were made from fine filaments dissected from the inferior alveolar nerve. The conduction velocities were calculated as the distance from the stimulating site to the recording electrodes, divided by the latency to onset of the action potential. For A fibers this was 13.9 6.4 m/s (mean
SD), and for C fibers it was 1.3 0.5 m/s.
The role of A and C fibers in dental pain perception was studied by recording from previously identified fibers while sudden cold stimuli were applied to the teeth (Jyväsjärvi and Knif-
fki, 1987). Stimuli were used which were known to cause pain sen-
sations in human teeth. When the mean rating of the subjective pain vs. time was plotted, it was correlated very closely with the time-course of firing of the A fibers.
The C fiber discharge was much slower and uncorrelated with the pain from cooling. This suggested a strong role for A fibers in transmission of pain induced by cold stimulation.
In a study of pulpal C fibers (Jyväsjärvi et al., 1988), it was found that they typically responded to thermal, mechanical, and chemical stimulation. Thus, they appeared to be polymodal nociceptive fibers. As these authors were aware of the role of polymodal nociceptors in sensitization and hyperalgesia (Chapter
4), they tried to sensitize pulpal C fibers by heating the tooth.
No persistent discharge was produced with thermal stimuli, but many C fibers developed an ongoing discharge after mechanical stimulation of the pulp. This was evidence for release of stimulating compounds in the periphery by irritation of pulpal elements.
The central pathways for dental pain perception are indicated in Figure 15. Afferents from the mandibular and maxillary divisions of the trigeminal nerve relay in the spinal sensory nucleus of V. From this region fibers cross the pons and many relay in the pontine reticular formation; ultimately they project to the intralaminar and ventroposterior thalamic nuclei, and thence diffusely to the cortex.
The projections of sensory axons innervating a tooth may be traced with the use of horseradish peroxidase (HRP, Furstman et al., 1975). HRP is injected into a pulp cavity, from where it is transported in sensory axons to their terminations. Following a 1-
2 day period for transport to occur, label was found in the trigeminal ganglion. Later studies (e.g Arvidsson and Gobel, 1981) used this technique to show that a single pulp nerve projected to the dorsomedial parts of the main sensory nucleus of V as well as the subnuclei oralis and interpolaris.
Chemical Theory of Dental Pain
As mentioned in connection with nociceptors in the skin
(Chapter 4), a variety of chemicals including substance P, histamine, 5-hydroxytryptamine, bradykinin and prostaglandins may contribute to sensitization and hyperalgesia around an injury.
This situation is also likely to exist in the dental pulp, where nerve endings are known to be sensitive to applied chemicals and where certain neurotransmitters and peptides have been shown to occur.
Olgart (1985) reported on some studies where the the activity of nerve endings in the pulp was recorded using a similar method to that of of Scott and Tempel (1963). The effects of applying various factors to the exposed dentin and pulp were observed, such as: (1) ammonia excited nerve responses as long as it was present in the dentinal cavity, (2) several amino acids could excite the nerves, (3) lactic acid and other organic acids failed to excite the nerves, (4) sucrose applied to dentinal cavities produced an immediate burst of nerve activity.
Immunohistological studies in which distinct compounds can be identified in tissues have also been applied to the dental pulp.
Olgart et al. (1977) found substance P-like immunoreactivity in small nerve fibers in the pulp, and the calcitonin gene-related peptide has also been identified in thin sensory axons of the pulp
(Silverman and Kruger, 1987).
CGRP is calcitonin gene-related peptide. Remember that calcitonin is a hypocalcemic hormone, that causes calcium deposition and removal from the circulation. Calcitonin is secreted by parafollicular cells from the thyroid, and from neural tissue. It is a single-chain peptide of 32 amino acid residues.
CGRP is made in nervous tissue and consists of 37 amino acids. CGRP mimics the action of calcitonin in some species, causing deposition of calcium, but not in others. CGRP and its binding sites are widely distibuted in the CNS, where it is
believed to serve as a neurotransmitter. CGRP is found in many bipolar neurons in sensory ganglia and produces marked vasodilatation.
Cohen et al. (1985) showed that pulps from diagnosed painful teeth had as much as 20 times as much prostaglandin E
2
and F
2
as pulps from asymptomatic teeth.
The phosphonucleotide adenosine triphosphate has recently been shown to act as a neurotransmitter in the nervous system
(Ralevic and Burnstock, 1998). This compound activates ATP receptors or purinoceptors. There are ligand-gated ion-channel purinoceptors called P2X and G-protein coupled receptors called
P2Y. In 2001 Alavi, Dubyak and Burnstock published evidence of P2X receptors in human dental pulp (Alavi et al., 2001). The slides of the pulp were stained with antibodies against the receptor P2X
3 and against neurofilament proteins, which serve as a marker of nerve fibers. The results showed the presence of P2X
3
receptor protein in the same location as nerve fibers.
Thus, although the story is not as complete as for cutaneous nociceptors, we should be mindful that chemical intermediates undoubtedly play a role in dental pain perception. Research in this area will perhaps help in forming strategies to alleviate dental pain and inflammation.
Referred Dental Pain
In Chapter 4, referred pain was defined as "pain felt at a normal site as a result of an injury or disease process in another region." The problem of referred dental pains is one which plagues dentists and has led to an entire system of differential diagnosis of dental pains (Bell, 1989).
Some types of oral pain appear to be referred but are not
(Mumford, 1982): An acute periapical abscess on an upper tooth may
drain into the submandibular gland, causing it to become painful if pressure is applied. This is not referred pain, but spread of infection. Also, pain in a molar tooth may cause muscle tension to develop so that the masticatory muscles become painful. This is not referred pain, but spread of pain so that the muscle actually becomes painful to the touch.
Referred pain is considered to arise from the convergence of sensory pathways, and the establishment of an irritable focus in the central nervous system by unusual activity in one sensory pathway. Thus, impulses coming from a normal, pain-free area set off centrally-directed signals which are interpreted as pain in the unaffected area.
Mumford and Newton (1974a, b) reported on some clever experiments with the human incisors which illustrate this effect: As shown in Figure 16, the teeth are stimulated via small metal electrodes with respect to a remote electrode placed on the skin.
When either the right or left central incisor is stimulated, pain is normally felt if the stimulus current exceeds 10 A. However, when both incisors are stimulated at the same time, pain is felt when the total current exceeds 12 A, rather than the 20 A which might be expected.
When the total current is 12 A, presumably each tooth is receiving about half, or 6 A. Hence, the pain threshold for each tooth has been reduced from 10 to 6 A by applying a normally subthreshold stimulus to a neighboring tooth. This implication of this result for referred pain is that, for instance, a tooth with an inflamed pulp may send out a subthreshold signal to the nervous system and reduce the threshold of the adjacent teeth. Then normally painless stimuli on the adjacent teeth may be felt as painful in the presence of activity from the inflamed tooth. This is a classic example of referred pain, where the sensory pathways
from two peripheral endings converge and affect the signals going on the the CNS.
A case history of referred pain (Mumford, 1982):
"A young woman complained of pain in the upper premolars which, on examination, appeared healthy. One of the lower premolars had obvious deep caries and needed treatment even if it did not prove to be the source of pain, but she was very reluctant to have the lower tooth treated because she naturally regarded relief of pain in the upper tooth as more important. The principle of referred pain was explained and the lower tooth was anaesthetised, wherupon pain in the upper tooth ceased, and the patient was quite impressed thought still somewhat mystified."
Pain may be referred from the teeth to other normal areas, or to the teeth from injuries or diseases in other areas. Some examples are given in Table I.
Table I. Pains referred from or to the teeth.
________________________________________________________________
From teeth To teeth
________________________________________________________________
Ear - earache Sinuses - sinusitis
Eye - infraorbital
tenderness
Ear - otitis media
Neck - neckache Mastoids - mastoiditis
Head - headache Neck - whiplash injury
________________________________________________________________
Pain may refer from one jaw to another, but is generally considered not to refer across the midline.
Acupuncture and Dental Pain
The analgesia resulting from mechanical or electrical stimulation of acupuncture needles has been known for a very long time. In the
1970s, some investigators studied the mechanism of this phenomenon
in the CNS (Linzer and van Atta, 1974). As the role of the descending pain-inhibitory system became clearer (Chapter 5), acupuncture analgesia was considered to be a form of stimulusproduced analgesia (SPA). It developed over several minutes and was blocked by IV application of the opiate antagonist, naloxone.
In 1973 Anderson et al. studied the effect of electroacupuncture on the pain threshold of human teeth. They measured the threshold with a vitalometer or pulp tester, which indicated the current in microamps at which pain was first felt.
Electric currents were then passed through needles or surface electrodes placed between the metacarpal bones of the hands and in the infraorbital region of the cheeks. Some of their results are shown in Figure 17.
Part A compares the average thresholds of three teeth in each jaw as a function of time. After the electrical stimulation is started. The threshold for pain in the teeth increases slowly during the period of stimulation, and remains elevated for almost half an hour after stimulation is stopped. Part B shows essentially the same result with needles or surface electrodes in the hands and cheeks. This type of study gives confirming evidence of the role of endogenous opoid mechanisms in pain inhibition.
We shall now turn our attention to a very different type of sensory system which is equally important to the survival of organisms - that of the sense of taste.