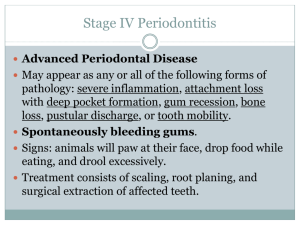
Possible Complications of Dental Procedures ( ) LOCAL
advertisement
 LOCAL")
Possible Complications of Dental Procedures ( ) LOCAL ANESTHESIA: They explained that local anesthesia is administered via injection, substances that cause reversible blockade of pain sensation, to make the treatment without pain. The local anesthesia may cause, among other things, ulceration of the mucosa at the injection site, pain, limitation of the mouth opening movement, decreased in blood pressure, syncope, urticaria, asthma, angioneurotic edema, and in rare cases ventricular fibrillation, or death, which may require urgent treatment. ( ) CONSERVATIVE DENTISTRY: The main purpose of these treatments is to remove the affected hard tissues, pulp protection, and restoration, to preserve the tooth and its function, restoring at the same time, whenever possible, the appropriate aesthetics. They explained that it is possible the appearance of a greater sensitivity, which usually disappear spontaneously, and that, especially in deep caries, can produce effects on the dental pulp that will require endodontic treatment, so the tooth will be fragile and may be necessary to carry out other reconstruction or placement of a prosthetic crown. I also understand that I may not be satisfied, aesthetically, with the shape and color of the tooth after the treatment, because the qualities of direct restorations will never be identical to their healthy appearance. ( ) ENDODONTICS The main purpose of the intervention is the elimination of pulp tissue when it becomes inflamed or infected, or with a granulomatous or cystic process, filling the pulp chamber and root ducts, preserving the tooth. I have been advised that, even the technique is practiced correctly, it is possible that the infection or cystic or granulation process, cannot be completely eliminated, so you may need retreatment or periapical surgery after a few weeks, months or even years. They also told me that it is possible the occurrence of postoperative sensitivity, change the color of the crown, the weakening and fracture of the tooth and the breaking of any instrument that might require other treatments. () PROSTHESIS The main purpose is the total or partial replacement of missing teeth, or the anatomical reconstruction of teeth that have lost structure. The operation consists in the preparation of the mouth by carving the adjacent teeth, or the proper management of soft tissue, and in making the impression to prepare the models. They have been told that the removable prosthesis can cause nausea, ulcers, aches, mobility in case of low bone support, which requires a process of adaptation that may require alterations and can be a long time, so must go periodically to visit the dentist. () SIMPLE EXTRACTION The procedure involves the extraction of a tooth from its alveolus, under local anesthesia, that after performed the diagnostic tests have been estimated accurately, has ruled out the implementation of restorative dentistry procedures, so that it becomes impossible to preserve . Despite having taken all the measures that have been considered necessary, may cause an infection, a profuse bleeding, rupture of the crown of the tooth, lacerations in the mucosa, displacement of the root to the maxillary sinus or other structures, fracture of the intraradicular partition wall, or maxillary tuberosity, temporomandibular joint dislocation, and even fracture of the jaw, which does not depend on the successful implementation of the intervention, they are unpredictable, in which case the physician will take accurate measurements, and continue the extraction. ( ) ORAL SURGERY Are the surgical interventions that are performed in the oral cavity to remove impacted teeth, infections, cysts or tumors affecting the jaws and / or soft tissues of the oral cavity or tongue, or to remodel these tissues to seat correctly dental prosthesis. They have been told that these operations, to clarify the incision of the oral mucosa or tongue, edematous processes can occur, inflammations, infections, hematomas, pain, mucosa lacerations, which does not depend on the form or mode of intervention performed, and its proper performance. They also explain that by their proximity, regardless of the technique used and its proper implementation, may be injured some other structure such as the inferior alveolar nerve or its terminal branches, or the lingual nerve, which involves anesthesia or numbness of the lip or chin area, which may be temporary or permanent, or the maxillary sinus could be the cause of sinusitis. () Periodontics Periodontal treatment aims the elimination of the etiological factors that cause disease of the tissues that support the teeth, through scaling techniques and root planing or periodontal surgery to prevent periodontal disease progression and ensure the maintenance of the teeth over time, function and aesthetics. I understand that even when carried out a successful implementation of the technical processes can occur edematous, swelling, pain or sores in the mucous membranes. They also explained that it is possible to increase sensitivity and tooth mobility, which should normally disappear spontaneously or by conducting subsequent treatments. Also will produce a lengthening of the teeth as a result of the elimination of the diseased tissue. I also understand that cause of the characteristics of periodontal disease, the required objective cannot be obtained, in whole or in part, irrespective of the technique and its proper implementation. () OTHER: Intolerance or allergies to anesthetics or medications required for treatment, ulceration of the mucosa in the injection point of anesthesia, pain, nausea, hematomas or discoloration of the skin or mucous membranes, limited movement of mouth opening, decreased blood pressure, and ventricular fibrillation may require emergency treatment. Inflammation, abscesses, bleeding, infections, bone sequestration, oral antral communications, oral nasal or fistula formation, increased sensitivity postoperative, weakening and fracture of teeth or portions of bone, or infectious processes. Sensitive or motor disorders such as anesthesia, paresthesia, hyperesthesia or movements alterations or muscle function. Need for other surgical procedures or treatments, accessories and tests, which should be performed at this clinic by their staff or even in other clinics and other professionals in dentistry. In case of implants, transplantation, of teeth or other tissues or materials, their loss or need to be replace due to intolerance, infection or abnormal masticatory forces. OTHER: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ APPROXIMATE DURATION OF TREATMENT: It is expected that the dental treatment indicated in this document take approximately ___________ months, however, also I understand that it can take more time, during which I must visit the dentist regularly according to the scheduled appointments, and especially during and after treatment, I must look carefully my dental hygiene through the techniques indicated above. INFORMED CONSENT AND DECLARATION OF ACCEPTANCE OF RISKS FOR ODONTOLOGY The Undersigned _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ in my personal capacity as a representative of a minor _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ I DECLARE: That Dr _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ explained me that I must receive dental treatment of _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ and explained and clarified in a vocabulary that is understandable to me, the size, scope and possible consequences, effects or inconvenience of the treatment above. Some of the possible complications, sequelae, disorders, risks or pre-, trans-or postoperative discomforts , are the following: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ I declare that if these complications occur, I accept the discomforts and risks mentioned and those listed as derivatives of the treatment. Any notes or Additional clarification is written on the back of this sheet and shall be fitted with the signature of the patient or the responsible person. DENTIST'S INSTRUCTIONS: I understand that failure the follow instructions that the Dr _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ indicated to me, the treatment may not have the expected success or complications may arise and need other interventions or treatments, without any implication that the previous have been executed incorrectly or without proper scientific and technical capacity required. Therefore, I manifest that I am satisfied with the information received and understand the scope and risks of the treatment. In these conditions: CONSENT I am agree that you can make me the dental treatments specified at the beginning of this document. In _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Date_ _ _ _ _ _ _ _ _ _ _ _ _ _ __ The patient or legal representative: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ DR. _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Witness _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _