Behavioral Intervention Plan (BIP)
advertisement
")
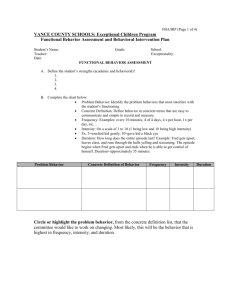
Rev. 11/06 Meeting Date: Stafford County Public Schools 31 Stafford Avenue Stafford, VA 22554 (540) 658-6500 (540) 658-6042 BEHAVIOR INTERVENTION PLAN [BIP] Student: LAST FIRST D.O.B M.I. Current Placement - School: Special Education: Grade: If Yes, List disability: Will BIP be part of the student’s IEP? Age (If yes, IEP goals should be considered in the BIP.) Steps 1 – 5 of the Functional Behavioral Assessment have been completed. 6. Summarize the targeted behavior(s): List the behaviors of concern that impede the learning of the student. Provide baseline data. 7. Replacement Behaviors/ Improvement: What are the replacement behaviors that the student needs to learn? What will be the student’s responsibility? 8. Positive Behavioral/ Environmental Supports/Interventions: What support(s) or plan will be placed within the classroom(s) and other environments to promote greater student success? What will be implemented to teach and monitor replacement behavior(s)? What will adult responses be when student engages in target behavior? What will adult responses be when student engages in replacement behavior Student Reinforcers: What reinforcers will be in place to motivate the student to learn and generalize new replacement behaviors? Will a checklist/chart be needed to document student performance? Will the student be on a schedule of reinforcement where rewards are provided? Who will be responsible for providing reinforcement? Implementation:Place Start Date: Person(s) Responsible: Date(s) of Proposed Review: Person(s) Attending (Attach any necessary documentation as the BIP is evaluated.) Position Person(s) Attending Position After reviewing the information, indicate your response by checking the appropriate space and sign below. I give permission to implement the Behavior Intervention Plan. I do not give permission to implement the Behavior Intervention Plan. ________________________________________________ (Parent Signature & Date) Rev. 11/06 Meeting Date: Stafford County Public Schools 31 Stafford Avenue Stafford, VA 22554 (540) 658-6500 (540) 658-6042 BEHAVIOR INTERVENTION PLAN [BIP] REVIEW – Form 2 Student: LAST FIRST D.O.B M.I. Current Placement - School: Age Grade: Special Education: If Yes, List disability: Will BIP be part of the student’s IEP? (If yes, IEP goals should be considered in the BIP.) Summarize target and replacement behaviors. Has there been an increase, decrease, or no change in the target behavior(s). (Attach data/documentation) Are supports/interventions appropriate? Do any modifications - additions or deletions need to be made to the current plan? Please document necessary action(s) and person(s) responsible for those changes. Action Item(s) Person(s) Responsible BIP Minutes – Additional Items Discussed Person(s) Attending Position Person(s) Attending Position After reviewing the information, indicate your response by checking the appropriate space and sign below. I give permission to implement the Behavior Intervention Plan. I do not give permission to implement the Behavior Intervention Plan. _______________________________________________________ (Parent Signature) _____/_____/_____ (Date)