a mixed methods study - King`s College London

GAY AND LESBIAN PEOPLE WITH IBD 1
Title: Experiences of gay and lesbian people with inflammatory bowel disease: a mixed methods study
Authors
Lesley DIBLEY MPhil, RSCN,RGN; Research Associate, Florence Nightingale School of Nursing &
Midwifery, King’s College, London, UK
Christine NORTON PhD, RN; Florence Nightingale Professor of Clinical Nursing Research, Florence
Nightingale School of Nursing & Midwifery, King’s College, and Imperial College, London, UK
Jason SCHAUB MSW; Senior Lecturer in Social Work, Buckinghamshire New University, High
Wycombe, UK
Paul BASSETT MSc; Independent statistician, Stats Consultancy, Amersham, UK.
Address for correspondence
Work
Lesley Dibley
Florence Nightingale School of Nursing and Midwifery
James Clerk Maxwell Building
57 Waterloo Road
London, SE1 8WA
Tel: 020 7848 3526
Email: lesley.b.dibley@kcl.ac.uk
GAY AND LESBIAN PEOPLE WITH IBD
Abstract
2
Chronic illness research involving lesbian and gay people typically focuses on HIV/AIDS, cancer, and mental health. The authors extend the evidence with a two-phase mixed methods exploration of gay and lesbian people ’s experiences with inflammatory bowel disease (IBD). Demographic, disease history, and outness data was collected from 50 community-based respondents, and 22 semi-structured interviews were conducted. Respondents used equivalent coming out techniques to reveal illness and sexual identity, though some find managing two challenging identities demanding. Of the 12 key themes identified, 8 resonate with concerns reported in the heterosexual IBD population, while four —sexual activity, receiving health care, IBD and lesbian and gay life, and identity and coming out —are unique to this study population.
The physical and practical aspects of IBD match those of the heterosexual community and can be managed similarly. Gay and bisexual men require precise information about sexual activity/restrictions from healthcare staff, who should also address the psychological needs of patients by enabling coming out and partner involvement.
Keywords : gay, lesbian, inflammatory bowel disease, identity, coming out, sexual orientation, healthcare, mixed methods
GAY AND LESBIAN PEOPLE WITH IBD
Introduction
3
Inflammatory bowel disease (IBD) is a chronic lifetime disease, often requiring intense periods of contact with gastroenterologists, specialist IBD and stoma nurses. Gay and lesbian (GL) patients have historically been poorly supported in health interactions (Albarran and Salmon 2000). Recent evidence suggests little improvement, despite worldwide progress addressing the rights of those with alternative identities (Sinding et al 2004; Fish 2010).
In the UK population of 62.3 million, 250,000 (0.4%) have IBD, and 3.6 million (5.9%) may be gay or lesbian: over 14,000 gay and lesbian people (GLP) in the UK may therefore have IBD. Disease characteristics, symptoms and complications are likely to be common to all, but it is not known whether social, psychological and illness-related concerns are similar, or if there are unique issues associated with having a different sexual identity and IBD, requiring additional support.
Inflammatory bowel disease
IBD, predominantly comprised of Crohn’s disease (CD) and Ulcerative Colitis (UC), follows an unpredictable relapsing and remitting course. Key symptoms include diarrhoea, weight loss, abdominal pain, vomiting and illness-related anorexia, anaemia and fatigue (Whayman et al 2011). Medical management includes use of powerful anti-inflammatory and biologic therapies, with potentially significant side effects. Surgical management includes bowel resection, temporary or permanent ileostomy, and ileoanal pouch construction (Mowat et al 2011). Prior to the introduction of biological therapies it was estimated that 30% –40% of UC, and 80% of CD patients would require surgery at least once (Rampton and Shanahan 2006); rates of surgery in the era of biologics have yet to be established
(Vester-Andersen et al. 2013). Extra-intestinal complications including iritis (inflammation of the iris of the eye) and arthropathy (disease of the joints with or without inflammation) can occur (Ardizzone et al
2008). Bowel control difficulties feature in both diseases (Norton et al 2013).
Coming out
GLP usually develop methods for revealing their sexuality. It is not known whether coming out methods
GAY AND LESBIAN PEOPLE WITH IBD 4 help or hinder when managing identity related to a chronic illness, including IBD (Axtell 1999; Corrigan et al 2009), or whether such methods might help non-GLP with IBD manage their illness identity effectively, although tentative comparisons have been made (Myers 2004). ‘Coming out’ refers to the process of revealing self-identity (Taylor 1999), and is achieved through a range of methods including making positive public statements, as discussed below (coming out techniques) and identified in Table
2). Despite recent positive changes in social attitudes towards homosexuals and conventionality of many GLP lifestyles, which often mirror heterosexual lives, homophobia still exists. Society and healthcare systems are heteronormative (assuming heterosexuality is the default assumption) (Johnson
2002) and heterosexist (attitudes favour heterosexuality)
(Röndahl 2006; Irwin 2007), affecting ability to seek healthcare. Lesbians have a higher incidence of alcoholism, smoking, and mental ill-health
(Spinks et al 2000), and higher risk of breast cancer (Cochrane et al 2001) compared with the general female population. Amongst gay men, key risks are HIV/AIDS (Martin 2005), smoking, drug and alcohol abuse (Ferri 2004), depression, diet-related body image issues (Siconolfi et al 2009), and anal papilloma (Reed et al 2010). These high-risk groups access health support less often than non-GLP with similar problems, with concerns about homophobic reactions from staff (Neville and Hendrickson
2006; Pennant et al 2009). Without revealing orientation, the holistic needs of patients cannot be met, and partner involvement may be overlooked (Wilton 2000).
The authors aimed to explore the parallels between coming out about sexual identity and IBD, to compare GLP IBD-related concerns with those of the non-gay IBD community, and to identify the social and psychological aspects of IBD in gay people.
Design
A mixed methods approach was used, based on Creswell and Plano Clark’s model (2007) an initial quantitative (survey) phase was followed by a qualitative (interview) phase. Findings from both stages are presented, and merged together in the discussion.
GAY AND LESBIAN PEOPLE WITH IBD
Sample
5
A purposive sample of GLP with IBD was recruited from across the UK using chain-referral sampling
(identified participants referring the study on to their known contacts) and strategic advertising (placing recruitment materials in locations which target the population of interest) (Lee and Renzetti 1990), including IBD and GL charities, online support forums, social networking sites, GL-friendly businesses and professional networks, continuing until no further participants could be located.
Phase one survey participants
From 13 recruitment sources, 66 people expressed an interest. The inclusion criteria were: either gender, identifying as GL, a diagnosis of IBD, aged over 18, living in the UK, understanding spoken or written English. 57 people completed the survey (55 online, 2 paper). Seven were incomplete, leaving
50 complete sets of data available for analysis.
Phase two interview participants
Survey participants could opt to also be interviewed. Selecting the same individuals for follow-up phases increases the likelihood of participants being knowledgeable about relevant issues, cements connections between phases of the study, and enhances study validity (Creswell and Plano Clark
2007). Thirty-four of the 50 survey respondents (68%) were willing to be interviewed. Twenty-two interviewees were selected to represent a range of ages, with equal numbers having CD and UC.
Completion of the online survey or return of the paper equivalent was taken as consent for phase one.
Written informed consent was collected from phase two participants before interviews commenced.
Data collection
Quantitative phase (survey)
The survey (Table 1 ) was developed utilising the study teams’ existing knowledge of IBD and GL issues, with reference to supporting literature (Shakespeare 1999; Hunter 2007; Corrigan et al 2009).
Key concerns of IBD patients have been confirmed in several studies (Casati et al 2000; Stjerman et al
GAY AND LESBIAN PEOPLE WITH IBD 6
2010; Jelsness-Jorgensen et al 2011). Techniques that GLP use to come out have been confirmed through research (Dooley 2009; Griffith and Hebl 2002). The Outness Inventory (Mohr and Fassinger
2000) is a validated scale measuring how ‘out’ (open about sexual orientation) respondents are to social, employment and religious contacts. To compare degree of outness about sexual orientation with outness about IBD, minor text adaptations were made. The phase one survey was available online, accessed via a URL link and secure password, or in hard copy. Data were collected between April and
October 2011.
Qualitative phase (interviews)
Twenty-two semi-structured digitally recorded interviews (22 - 67 minutes long), were conducted in participant’s homes or a venue of their choosing, between September and December 2011, continuing until data saturation. Field notes were maintained. All interviews began with the open question, ‘ Can you describe what life is like for you as a gay man / lesbian with IBD ?’ Prompts addressing issues identified in phase one data analysis were used to progress the interview. For example, ‘ You indicated in the survey that your top concern is body image. Could you tell me a little more about that ?’
Data analysis – achieving rigour
Quantitative analysis
Data were downloaded into Excel, paper surveys (n=2) were input by hand, and results imported into
SPSS and Stata for analysis. The same scales were used to assess both difficulty of coming out and degree of outness for IBD and for sexual orientation. As there was a pair of measurements from each patient and responses were normally distributed, a paired t-test was used to compare ease of coming out and degree of outness relating to respondents’ sexual orientation, and to IBD. Respondents’ concerns were summarised descriptively.
Qualitative analysis
Qualitative data were analysed using a pragmatic thematic approach (Fereday and Muir-Cochrane
2006). Free text responses from phase one were independently coded by two of the authors before
GAY AND LESBIAN PEOPLE WITH IBD 7 collaborating to develop initial themes. There was a high level of coding agreement. Having separate coding by two researchers helped refine the coding frames and enhanced the rigour of the analysis
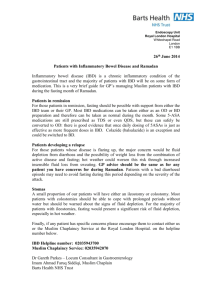
(Barbour, 2001). Phase two interviews were transcribed professionally. Initial themes from phase one data guided analysis of interview transcripts, new codes and themes also emerging. The authors analysed the interview transcripts independently, before collaborating to discuss and connect codes, identify themes, and agree and legitimise final themes (Figure 1). Trustworthiness is established in the connections between phases of the study, and in the relationship between phase one questions and responses (Table 2) which generated codes and themes to guide phase two data analysis.
Results: Phase one survey
Two-thirds of respondents were male (n=33; 66.0%); mean age 38 yrs, range 21-56 years; CD = 26
(52%); UC = 16 (32%); other form of IBD = 8 (16%). Mean symptom duration was 14 years, range 1-
49 years; mean diagnosis duration 12 years, range 0.3-45 years. Respondents were most likely to be white (98%), aged 31 - 40 years (42%) and in a civil partnership or same sex relationship (60%).
Phase 1 quantitative results
Coming out about sexual identity and about IBD
There was no significant difference between being out about sexual orientation (mean 5.1; SD 1.7) and about IBD (mean 4.9; SD 1.4) (p = 0.48), or between the difficulty of coming out about either IBD or sexual orientation (both 3.9 / 10) (Table 3). Respondents are therefore more out than not, in both identities, although most out to siblings, heterosexual friends, and mothers regarding gay identity, and to siblings, mothers and extended family regarding IBD identity.
Coming out techniques
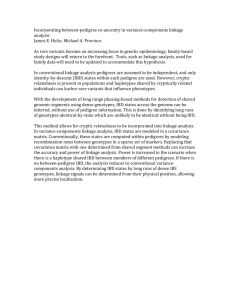
The seven techniques provided in the survey included methods of revealing information, and possible people to reveal to. ‘Waiting for an opportunity to be presented and then following it up to tell people about my sexual orientation / IBD’ was the most used strategy. ‘I never tell anyone about my sexual
GAY AND LESBIAN PEOPLE WITH IBD 8 orientati on / IBD’ was the least used, and never used in managing IBD identity. Most respondents ensured that their work manager knew about their illness, and that friends and work colleagues knew about their GL status (Figure 2).
Disease-related concerns of GLP with IBD
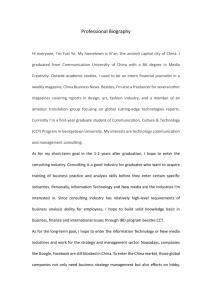
Respondents ranked eight IBD-related concerns in order of importance to them, from 1 (most important) to 8 (least important). Results were compared to the order of concerns in the general IBD population
(Casati et al 2000) (Table 4).
Phase 1 qualitative results
Six questions or prompts invited free-text responses. Twenty themes emerged, of which eight – employment, facilities for the disabled, toilets, poor public information, emotional impact, unpredictability, symptoms, and relationships - are familiar to anyone with IBD regardless of sexuality, and have been reported previously (Graff et al 2006; Dibley and Norton 2013). Twelve themes specific to GLP with IBD (Table 2), were subsequently used to guide phase two interviews.
Results: Phase two interviews
Fourteen gay males (63.6%) and 8 lesbians (36.4%) were interviewed; mean age 41 yrs, range 27 – 54 yrs; CD = 10 (45.5%); UC = 10 (45.5%), other form of IBD = 2 (9%). Mean symptom duration 14.8 yrs, range 2 - 49 yrs; mean diagnosis duration 15.9 yrs, range 0.5 - 42 yrs. Four central themes related to being a GLP with IBD were established. Themes are supported with verbatim quotes from phase one qualitative survey data (Lesbian Woman Survey - LWS; Gay Man Survey - GMS), and from interviews
(Lesbian Woman Interview - LWI; Gay Man Interview - GMI).
GL Sexual Activity
GAY AND LESBIAN PEOPLE WITH IBD 9
Gay men expressed concerns that others assume a relationship between their sexual behaviour and
IBD: “The only concern I ever have really is that people may judge and think it’s related to being gay and the whole anal sex thing ” [GMS-16], and that following surgery, especially after ileo-anal pouch formation, guidance on restrictions to non-heterosexual sexual activity is lacking:
But they don’t cover gay sex. So in the information leaflets ... [there is] always a section saying
‘sex and relationships’. And it says, oh it doesn’t affect your sexual life. You can still continue to have sex with your partner. And you’re like, ‘Well I can’t, because, you know ... [I’ve got this pouch]
’[GMI-6].
A sense of loss may arise when formation of a pouch, or perianal
Crohn’s disease, forces a change in preferred activity, precluding anal intercourse: “But I do feel robbed ... I feel robbed of the choice. I feel robbed of that flexibility within our sex life ” [GMI-21]. Lesbian women did not discuss sexual activity, or whether IBD limited activity. The only reference to sexual practice came from one woman who, several years following the formation of a permanent stoma, had chosen celibacy but did not elaborate on her reasons for doing so.
Receiving healthcare
Although uncertain whether healthcare professionals’ responses indicate homophobia, GL patients feel they are treated differently. Negative experiences could influence access to care: “I have felt so uncomfortable that it has got to the point now that I’ve said, ‘I don’t want to go into hospital any more. I’d rather die at home without treatment than go through all that stress ” [LWI-1]. Respondents described difficulties in having their partner or relationship acknowledged during healthcare encounters:
I was constantly getting, ‘ But ... you’re the person with this disease, you’re our priority .’ And I’m going, ‘No, he is my partner and therefore we come as a package....he needs to be part of this, you need to talk to him as well.’ [GMI-21]
GAY AND LESBIAN PEOPLE WITH IBD 10
Respondents made concerted efforts to ensure healthcare staff understood personal relationships, to make available the emotional support needed during hospital encounters:
Every form that I fill in, she is my partner… but it’s not often that they will read it before they talk to you. But even then when you say, ‘This is my partner,’ there’s still looks and ... they’re a little bit unsure. [LWI-17] and they tried to avoid causing distress to other patients by not displaying affection with their partner:
It’s a traumatic thing you’re going through, but you don’t feel, as a gay couple or as a gay individual, that you have that same freedom to express yourself in that way … once your visitors are gone, you’re left to the other patients in that space, you can’t escape it. So the last thing you want to do is create an atmosphere or feel intimidated, or make anyone else feel uncomfortable.
[GMI-3]
This desire to avoid causing offence, and the lack of private spaces in which to receive emotional and physical support from their partner, prevented adequate preparation for high-risk surgery:
[We] were not able to say goodbye to each other, we were not able to have a kiss and a cuddle because we were on a wa rd. It was very public, and it’s fine for heterosexual people ... but [we] learnt a long time ago that people, although very accepting, they can become quite different if you start showing physical affection ... [GMI-21]
IBD and GL life
Some respondents felt that IBD did not affect their GL life whilst others reported subtle issues making management of IBD symptoms more difficult. Those with more severe IBD reported a closer connection
GAY AND LESBIAN PEOPLE WITH IBD 11 between IBD and GL status, as more contact with health professionals prompted greater exposure of
GL identity.
Frequently, people with IBD leave the toilet only to return almost immediately. In public toilets, this may be misconstrued as ‘cottaging.’ This British gay slang term refers to anonymous sex in a public lavatory, or cruising for sexual partners (Church et al 1993) and is illegal (Ashford 2007). Concerns about the public’s perceptions have an influence on GL use of public toilets:
[Cottaging] is something that I don’t struggle with because what I tend to do is, I will go to the loo and I won’t leave the loo until I’m 100% sure that I’m right. And I’m not going to need to come straight back in again. [GMI-3]
The already stressful process of locating, accessing and using public toilets for people with IBD is compounded by gay-specific issues for GLP.
Body image is an issue for some gay men, so that disfiguring surgery resulting in either scars or a stoma can cause difficulties that prevent participation in the community: “I’m originally from [city] , big gay community there - all lads ... dancing in the clubs with their tops off, something I have never felt comfortable with because of the scar ” [GMI-3], or lead to a complete change in usual behaviour:
From the day I was told [the stoma] is basically going to be able to be reversed, I decided that I wasn’t even going to have any interest in relationships for the duration of the period that I had the stoma. [GMI-6]
Identity and Coming Out
Some respondents were not, or placed little value on being out, others found it easy to be out, and others emphasised the importance of coming out about their GL identity: “If you’re not at the very least open to yourself, if you’re not out to yourself about that, then you constantly feel alien ... by coming out,
GAY AND LESBIAN PEOPLE WITH IBD 12 you straighten out – strangely - your thinking” [GMI-5]. Since heterosexuality is the majority status, others may assume someone is heterosexual unless there is any obvious indication (outward appearance) or verbal confirmation (coming out statement or clue) to the contrary:
When I was working I made a point of letting people know I was [lesbian]. I did it in a lighthearted way – if someone asked about my boyfriend I would say “oh no, I don’t think my girlfriend would be very happy if I had one of those!” [LWS-9]
GLP who share information about their sexuality do so because it helps to avoid misdirection and because it reduces stress, benefitting health:
“I found it easier to be out in work than to have to watch what you say all the time. That causes more stress which leads to a flare up [of IBD] ” [LWS-16]. Not all respondents agreed, but many describe using sexuality coming-out tools to inform coming out about
IBD. The stress may be related to the stigma people can feel about both identities:
Some people are not happy talking about gay things, although that is improving through awareness. And some people certainly cower away and will not discuss bowel issues because it’s dirty, it’s not nice, it’s not table manners to talk about bowels and things. So I think there is a stigma attached to both of them. [GMI-15]
As with non-GLP with IBD, participants agreed that it was better for close family, friends, selected work colleagues and managers to know of their illness, since this improved understanding, support and the ability to manage the difficulties presented by IBD.
One aspect of identity for gay and bisexual men sometimes influenced by IBD relates to sexual practices. Broadly, gay men take an active (top, or insertive) or passive (bottom, or receptive) role in sexual activity. This role identity is definite for some, and flexible for others. Losing their preferred role because of IBD was shrugged off by some whilst others anticipated a period of adjustment:
GAY AND LESBIAN PEOPLE WITH IBD 13
I wasn’t 100 % [top or bottom] before and therefore it’s not a complete change for me. But I think the main change is mentally - how you think about sex and how you approach it. I used to quite regularly have sex with men who were more dominant in their character and physicality. Whereas now obviously I can’t do that. [GMI-6]
While participants emphasised that sexual activity does not dominate identity for a gay man, it may contribute to it. Identity can be affected by an enforced alteration to sexual practices.
Discussion
GLP develop coming out skills during identity formation, and daily negotiate encounters by choosing whether to pass, cover, or reveal their identity (Orne 2011). Our findings indicate that GLP with IBD often use the same skills to manage disease information. They secure social support for GL identity through close, personal relationships, and gain practical help and support in the management of their
IBD. By selecting different people for different identities, GLP may experience more positive interactions (Legate et al 2012), affirming their sense of identity, positive self-image and self-esteem
(Chaudoir and Quinn 2010). GL coming out skills may be helpful to anyone struggling to develop a more positive disease-identity (Corrigan et al 2009), regardless of sexual orientation, especially in
“hidden” conditions where the individual risks being unintentionally exposed by a bodily malfunction such as incontinence or an epileptic fit (Quinn 2006). Accepting chronic illness identity is part of the normalisation process in which illness is integrated and managed positively (Kralik and van Loon 2010).
Sexual activity in relationships concerns GLP as it does the heterosexual community (Jowett and Peel
2009). While sexual health in chronic illness is being addressed (Steinke 2005; Basson et al 2010) research into gay male needs focuses on HIV/AIDS, safe sex and wellness screening (Goldhammer and Mayer 2011; Bourne et al 2012; Hottes et al 2012). Lesbian sexual behaviours and related risks have only recently been addressed (Marrazzo and Gorgos 2012; Schick et al 2012). Anal intercourse is not exclusive to gay men, and anyone with IBD who engages in anal sex regardless of orientation,
GAY AND LESBIAN PEOPLE WITH IBD 14 needs specific advice on the sexual activity limitations caused by IBD. Such advice is difficult to locate, and there are no published data on the risks of anal intercourse where the recipient has IBD, or an ileoanal pouch. It is unclear if receptive anal sex increases the risk of faecal incontinence (Miles et al
1993; Chun et al 1997), and there is no evidence to suggest a greater risk of developing IBD in gay men and women. IBD typically begins with proctitis (inflammation in the distal end of the bowel), and mucosal inflammation due to disease decreases tissue integrity and increases risk of infection. Surgery at or close to the rectum - for example, end to end anastomosis following partial colectomy, or formation of an ileoanal pouch - will need protecting to avoid damage to suture lines or provocation of pouchitis.
Further research is needed to generate empirical evidence to support any advice relating to the risks of anoreceptive intercourse in IBD.
GLP have historically had a challenging relationship with healthcare (Fish 2010), reinforcing expectations that revealing sexuality may cause, and has caused, personal harm (Hitchcock and Wilson
1992; Sinding et al 2004; Platzer 2006; Dibble et al 2007). Heterosexual patients and spouses holding hands, offering physical comfort to give emotional support, and being involved together in care packages may be considered normal. GL patients may not feel able to be themselves because they do not wish to upset anyone. Without recognising these needs, healthcare staff may fail to provide support
(Walpin 1997; Röndahl 2006) and GLP may consequently avoid hospital care all together, or endure hospitalisation and other healthcare encounters without the benefits of full partner support (Katz 2009).
For GLP with IBD, facing acute or lifethreatening illness episodes without the opportunity to be ‘say goodbye’ could be potentially devestating for the remaining partner should the patient not survive. Study participants perceived that heterosexual patients and their partners do receive adequate support, although this may not be the case. HCPs should recognise and respect the unique needs of any patient and partner, regardless of sexual orientation or illness (Bonvicini and Perlin 2003; Fish 2010), by enabling private spaces for emotional support and involving all partners in care strategies.
The relationship between illness and GL status may influence the impact IBD has on lifestyle and identity. Those with milder, controllable disease seem able to draw lines of separation between these
GAY AND LESBIAN PEOPLE WITH IBD 15 two identities: symptoms perhaps have less impact, are less disruptive and therefore less apparent in social, public and employment spaces. Refractory disease (resistant to medical therapies) interrupts these spaces and invades privacy, requiring greater contact with medical and nursing staff and more hospital admissions. The person’s sexuality and relationship is thrown into the spotlight, symptoms disrupt most areas of life, and managing GL lifestyle and identity alongside chronic illness identity can be difficult. Body image, for example, emerged as a major concern for young gay men with disfiguring scars following surgery. Sexuality and body image issues following stoma surgery for any cause (Cohen
1991; Junkin and Beitz 2005), and in IBD in general (Muller et al. 2010; McDermott et al. 2014), have previously been addressed, reporting concerns similar to those reported in this study.
HCPs caring for GLP with chronic illness can use a range of written and verbal approaches to establish and maintain a therapeutic caring relationship (Dibble et al 2007), taking advantage of the commonest coming out technique - that of following up on an opportunity as it is presented. In providing written and verbal openings, the HCP creates the chance for GLP to reveal their status, paving the way for open dialogue, accurate assessment, and appropriate support.
There are study limitations which need consideration. The small sample size may reduce generalisability of quantitative findings as outliers (those who score very high or low) may be underrepresented. Recruiting for research into hidden groups is challenging, restricting opportunities to pilot research or determine whether the sample is representative.
Conclusion
Although managing two sensitive identities can be challenging, GLP use the same techniques and are out to the same degree about their sexual and illness identities. Intervention studies can test whether teaching transferable coming out skills to non-GLP with IBD, or any other chronic illness, enables more effective sharing of sensitive disease information. Most physical and practical aspects of IBD match
GAY AND LESBIAN PEOPLE WITH IBD 16 those of the non-GL community and can be managed similarly, although the impact on GL lifestyle and identity needs recognition. Staff can promote disclosure of sexual orientation or identity by providing opportunities for sensitive information to be revealed. Precise guidance, perhaps using GL-specific information leaflets, is needed from IBD specialist and stoma nurses to advise gay and bisexual men about sexual activity / restrictions. GL patients with IBD need help in achieving privacy and partner support in healthcare arenas. Further research, with a larger sample size, would add credibility to these early findings.
Ethical approvals
Ethical permission for the study was granted by the Faculty of Society & Health Ethics Panel at
Buckinghamshire New University (where the first two authors were employed at the time, and throughout the data collection period). The paper has not been submitted elsewhere, and no additional publications arising from this study exist.
Acknowledgements
The authors acknowledge the assistance of Mrs Dawn Evans (professional transcriber) with the qualitative interviews in Phase 2 of this study.
Source of funding
The study was funded in full by a grant (reference number SP2010-2) from Crohn’s & Colitis UK. The funding body assisted in recruitment by placing study details in the charity’s publication, and at their online social networking page, but had no other involvement in the design, conduct, or reporting of the study.
Conflicts of interest
There are no conflicts of interest to declare.
GAY AND LESBIAN PEOPLE WITH IBD
References
17
Albarran J,Salmon D (2000) Lesbian, gay and bisexual experiences within critical care nursing 1988 -
1999: a survey of the literature. Int J Nurs Stud 37 (5): 445-455.
DOI: 10.1016/S0020-7489(00)00024-9.
Ardizzone S, Sarzi Puttini P, Cassinotti A, Bianchi Porro G (2008) Extraintestinal manifestations of inflammatory bowel disease. Dig Liver Dis 40S : S253-S259.
DOI: 10.1016/S1590-8658(08)60534-4
Ashford C( 2007) Sexuality, public space and the criminal law: the cottaging phenomenon. J Crim Law
71 (6):506-519.
Axtell S (1999) Disability and Chronic Illness Identity: Interviews with Lesbian and Bisexual Women and their partners Journal of Gay, Lesbian and Bisexual Identity 4 (1):53-72. DOI:
10.1023/A:1023254408084.
Barbour, R. (2001) Checklists for improving rigour in qualitative research: a case of the tail wagging the dog? British Medical Journal . 322 (7294), pp. 1115 –1117.
Basson R, Rees P, Wang R, Montejo AL, Incrocci L (2010) Sexual function in chronic illness. J Sex
Med 7 (1 Pt 2):374-388, DOI:10.1111/j.1743-6109.2009.01621.x
Bonvicini K,Perlin M (2003) The same but different: clinician-patient communication with gay and lesbian patients. Patient Educ Couns 51 :115-122. DOI:10.1016/S0738-3991(02)00189-1
Bourne C, Zablotska I, Williamson A, Calmette Y, Guy R (2012) Promotion and uptake of a new online partner notification and retesting reminder service for gay men. Sex Health 9 (4) 2012-2367.
DOI:10.1071/SH11132.
Casati J, Toner B, De Rooy E, Drossman D, Maunder R (2000). Concerns of patients with inflammatory bowel disease: a review of emerging themes. Dig Dis Sci 45 (1):26-31.
GAY AND LESBIAN PEOPLE WITH IBD 18
Chaudoir S, Quinn D (2010) Revealing concealable stigmatized identities: the impact of disclosure motivations and positive first-disclosure experiences on fear of disclosure and well-being. J Social
Issues 66 (3):570-584. DOI:10.1111/j.1540-4560.2010.01663.x
Chun A, Rose S, Mitrani C, Silvestre A, Wald A (1997). Anal sphincter structure and function in homosexual males engaging in anoreceptive intercourse. Am J Gastroenterol 92 :465-468.
Church J, Green J, Vearnals S, Keogh P (1993) Investigation of motivational and behavioural factors influencing men who have sex with other men in public toilets (cottaging). AIDS Care 5 (3):337-346.
Cochrane S, Mays V, Bowen D, Gage S, Bybee D, Roberts S, Goldstein R et al (2001) Cancer-related risk indicators and preventive screening behaviors in lesbians and bisexual women. Am J Public Health
91 (4):591-597.
Cohen A (1997) Body image in the person with a stoma Journal of Enterostomal Therapy 18 (2):68-71.
Corrigan P, Larson J, Hautamaki J, Matthews A, Kuwabara S, Rafacz J et al (2009) What lesson do coming out as gay men or lesbians have for people stigmatised by mental illness? Community Ment
Health J 45 :366-374. DOI:10.1007/s10597-009-9187-6.
Creswell J,Plano Clark V (2007) Designing and conducting mixed methods research Thousand Oaks,
Sage Publications.
Dibble S, Eliason M, Christiansen M (2007) Chronic illness care for lesbian, gay and bisexual individuals. Nurs Clin North Am 42 (4): 655-674.
Dibley L, Norton C (2013). Experiences of fecal incontinence in people with inflammatory bowel disease: self-reported experiences among a community sample. Inflamm Bowel Dis 19 :1450-1462.
DOI:10.1097/MIB.0b013e318281327f.
Dooley J (2009) Negotiating stigma: lessons from the life stories of gay men. J Gay Lesbian Soc Serv
21 (1):13-29. DOI:10.1080/10538720802494784.
GAY AND LESBIAN PEOPLE WITH IBD 19
Fereday J, Muir-Cochrane E (2006) Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods 5 ( 1):5 pages. Available at: http://www.ualberta.ca/~iiqm/backissues/5_1/PDF/FEREDAY.PDF
Ferri R (2004) Issues in gay men's health. Nurs Clin North Am 39 (2):403-410.
Fish J (2010) Promoting equality and valuing diversity for lesbian, gay, bisexual and trans patients.
InnovAIT 3 (6):333-338. DOI:10.1093/innovait/inq110.
Goldhammer H, Mayer KH (2011) Focusing on sexual health promotion to enhance preventive behaviors among gay men and other men who have sex with men: report from a state-of-the-art conference. AIDS Behav 15 (Suppl.1):S1-8. DOI:10.1007/s10461-011-9907-0.
Graff L, Walker J, Lix L, Clara I, Rawsthorne P, Rogala L et al (2006) The relationship of inflammatory bowel disease type and activity to psychosocial functioning and quality of life. Clin Gastroenterol
Hepatol 4 (12):1491-1501.
Griffith K, Hebl M (2002) The disclosure dilemma for gay men and lesbians: coming out at work. J Appl
Psychol 87 (6):1191-1199.
Hitchcock J, Wilson H (1992) Personal risking: lesbian self-disclosure of sexual orientation to professional healthcare providers. Nurs Res 41 (3):178-183.
Hottes TS, Farrell J, Bondyra M, Haag D, Shoveller J, Gilbert M (2012) Internet-based HIV and sexually transmitted infection testing in British Columbia, Canada: opinions and expectations of prospective clients. J Med Internet Res 14 (2):e41. DOI:10.2196/jmir.1948.
Hunter S (2007) Coming out and disclosures: LGBT persons across the life span . New York, Howarth
Press.
Irwin L (2007) Homophobia and heterosexism: implications for nursing and nursing practice. Aus J Adv
Nurs 25 (1):70-76.
GAY AND LESBIAN PEOPLE WITH IBD 20
Jelsness-Jorgensen L, Moum B, Bernklev T (2011) Worries and concerns among inflammatory bowel disease patients followed prospectively over one year. Gastroenterol Res Pract DOI:
10.1155/2011/492034. Epub 2011 Sep 6.
Johnson C (2002). Heteronormative citizenship and the politics of passing. Sexualities 5 : 317-336 .
DOI:10.1177/1363460702005003004.
Jowett A, Peel E (2009) Chronic illness in non-heterosexual contexts: An online survey of experiences.
Feminism & Psychology 4 (4):454-474.
DOI: 10.1177/0959353509342770.
Junkin J, Beitz JM (2005) Sexuality and the person with a stoma. Journal of Wound, Ostomy and
Continence Nursing 32 (2):121-128.
Katz A (2009) Gay and lesbian patients with cancer. Oncol Nurs Forum 36 (2):203-207. DOI:
10.1188/09.ONF.203-207.
Kralik D, van Loon A (2010) Transitional processes and chronic illness. In: Kralik D, Paterson B, Coates
V, eds. Translating chronic illness research into practice . Wiley-Blackwell, Oxford:17-36.
Lee R, Renzetti C (1990) The problems of researching sensitive topics: An overview and introduction.
Am Behav Sci 33 :510-528.
DOI: 10.1177/0002764290033005002.
Legate N, Ryan RM, Weinstein N (2012). Is coming out always a "good thing"? exploring the relations of autonomy support, outness, and wellness for lesbian, gay, and bisexual individuals. Soc Psychol
Pers Sci 3 (2):145-152 DOI:10.1177/1948550611411929.
Marrazzo JM, Gorgos LM (2012) Emerging sexual health issues among women who have sex with women. Curr Infect Dis Rep 14 (2):204-211. DOI:10.1007/s11908-012-0244-x.
Martin G (2005) Reducing the risk of HIV in gay and bisexual men. Nurs Times 101 (34):38-41.
McDermott E, Moloney J, Rafter N, Keegan D, Byrne K, Doherty GA, Cullen G, Malone K,
GAY AND LESBIAN PEOPLE WITH IBD 21
Mulcahy HE (2014) Body image scale: a simple tool for assessing body image dissatisfaction in IBD.
Inflammatory Bowel Diseases 20 (2):286-290.
Miles A, Allen-Mersh T, Wastell C (1993) Effect of anoreceptive intercourse on anorectal function. J R
Soc Med 86 (3):144-147.
Mohr J, Fassinger R (2000) Measuring dimensions of lesbian and gay male experience. Measurement and Evaluation in Counselling & Development 33 :66-90.
Mowat C, Cole A, Windsor A, Ahmad T, Arnott I, Driscoll R et al (2011). Guidelines for the management of inflammatory bowel disease in adults. Gut 60 (5):571-607. DOI: 10.1136/gut.2010.224154.
Myers KR (2004) Coming Out: Considering the Closet of Illness. J Med Humanit 25 (4):255-270.
Neville S, Hendrickson M (2006) Perceptions of lesbian, gay and bisexual people of primary healthcare services. J Adv Nurs 55 (4):407-415. DOI: 10.1111/j.1365-2648.2006.03944.x.
Norton C, Dibley L, Bassett P (2013) Faecal incontinence in inflammatory bowel disease: associations and effect on quality of life. J Crohns Colitis 7 (8):e302-e311. DOI: 10.1016/j.crohns.2012.11.004
Orne J (2011) 'You will always have to "out" yourself': Reconsidering coming out through strategic outness. Sexualities (6) 681-703. DOI:10.1177/1363460711420462.
Pennant M, Bayliss S, Meads C (2009) Improving lesbian, gay and bisexual healthcare: a systematic review of qualitative literature from the UK. Diversity in Health & Care 6 (3):193-203.
Platzer H (2006) Positioning Identities: Lesbians' and Gays' Experiences with Mental Health Care .
Edmonton, Alberta, Canada, Qualitative Institute Press.
Quinn D (2006) Concealable versus conspicuous stigmatized identities. In: Levin S, van Laar C, eds.
Stigma and group inequality Lawrence Erlbaum Associates,Mahwah, NJ:83-103.
Rampton D, Shanahan F (2006) Fast Facts: Inflammatory Bowel Disease . Oxford, Health Press Ltd.
GAY AND LESBIAN PEOPLE WITH IBD 22
Reed A, Reiter P, Smith J, Palefsky J, Brewer N (2010) Gay and bisexual men's willingness to receive anal papanicolaou testing. Am J Public Health 100 (6):1123-1129. DOI: 10.2105/AJPH.2009.176446.
Röndahl G (2006) Heterosexual assumptions in verbal and non-verbal communication in nursing. J Adv
Nurs 56 (4):373-381.
Schick V, Rosenberger JG, Herbenick D, Reece M (2012) Sexual behaviour and risk reduction strategies among a multinational sample of women who have sex with women. Sex Transm Infect 88
(6): 407-412.
Shakespeare T (1999) Coming Out and Coming Home. J Gay Lesb Bisex Ident 4 (1):39-51.
Siconolfi D, Halkitis P, Allomong T, Burton C (2009) Body dissatisfaction and eating disorders in a sample of gay and bisexual men. Int J Men's Health , 8, (3) 254-264. DOI: 10.3149/jmh.0803.254.
Sinding C, Barnoff L, Grassau P (2004) Homophobia and heterosexism in cancer care: the experiences of lesbians. Can J Nurs Res 36 (4):170-188.
Spinks V, Andrews J, Boyle J (2000) Providing health care for lesbian clients. J Transcult Nurs
11 (2):137-143.
Steinke E (2005) Intimacy needs and chronic illness: Strategies for sexual counseling and selfmanagement. J Gerontol Nurs 31 (5):40-50.
Stjernman H, Tysk C, Almer S, Strom M, Hjortswang H (2010). Worries and concerns in a large unselected cohort of patients with Crohn's disease. Scand J Gastroenterol 45 (6): 696-706. DOI:
10.3109/00365521003734141.
Taylor B (1999) ‘Coming out’ as a life transition: homosexual identity formation and its implications for health care practice J Adv Nurs 30 (2): 520 – 525.
Vester-Andersen MK, Prosberg MV, Munkholm P, Bendtsen F (2013) Surgery rates in Danish incident cases of ulcerative colitis and Crohn ’s disease. J Crohn’s Colitis . 7 (Suppl.1) S257.
GAY AND LESBIAN PEOPLE WITH IBD 23
Walpin L (1997) Combating heterosexism: implications for nursing. Clin Nurs Spec 11 (3): 126-132.
Whayman K, Duncan J, O'Connor M (2011) Inflammatory Bowel Disease Nursing . Quay Books Division
MA Healthcare Ltd, London.
Wilton T (2000) Sexualities in health and social care . Open University Press, Buckingham.
GAY AND LESBIAN PEOPLE WITH IBD
Tables and figures
24
Phase 1 survey Type of data collected
Section 1 Demographic data: age, gender, sexual orientation, partnership status, location (county) in the UK, IBD diagnosis (CD, UC or other
[indeterminate, Crohn’s Colitis, or proctitis]), level of education, years of
Section 2
Section 3 symptoms and of diagnosis
Participant’s rank of eight IBD-related issues known to concern the non-
GL IBD population (Casati et al. 2000)
Completion of the original Mohr & Fassinger (2000) Outness Inventory,
Section 4 and an adapted for IBD version
Participant’s rating (0 - not at all difficult; 10 - extremely difficult, impossible) of degree of difficulty in telling others about their sexual orientation, and IBD;
Section 5
Identification of which, of seven strategies (Dooley, 2009;Griffith & Hebl,
2002), they use to share information about their sexual orientation, and
IBD
Free text responses providing detailed explanation of earlier quantitative responses
Table 1: Data collected across the five sections of the phase one survey
GAY AND LESBIAN PEOPLE WITH IBD
Pragmatic thematic analysis
Phase 1 qualitative data Phase 2 qualitative data
THEME: LGBT sexual activity
THEME: Receiving healthcare
THEME: Stigma / taboo
THEME: Social Rules
THEME: Identity
THEME: Other people’s reactions INTERVIEWS
THEME: It’s my business
THEME: Protecting others
THEME: Help & support
THEME: It’s who I am
THEME: Revealing one identity is harder than revealing the other
25
THEME:
LGBT sexual activity
THEME:
Receiving healthcare
THEME:
IBD and LGBT Life
THEME:
Identity and Coming
Out
Figure 1: Qualitative analysis and theme development showing the relationship between themes arising from each phase of the study
THEME: Using the same techniques to come out
GAY AND LESBIAN PEOPLE WITH IBD 26
Question
1. Please tell us anything else which concerns you about your IBD
2. Can you explain why it is difficult to share information about your BD?
3. Can you explain why it is difficult to share information about your sexual orientation?
4. If you DO NOT find it difficult to share information about your IBD, please try and explain why it is not difficult for you
5. If you DO NOT find it difficult to
Theme
LGBT sexual activity
Sample of responses in Phase 1
‘People associating my disease with my sexuality and supposed sexual habits, whether true or not;’
‘... one of the primary concerns has to be the impact on sexual relationships;’
‘privacy in hospital for patients in a same sex relationship’ Receiving healthcare
Stigma / taboo ‘Because any reference to bodily functions to do with 'poo' is a taboo area anyway. When you have to tell
Social Rules
Identity someone about your IBD you are basically talking about 'poo' and many people are uncomfortable with this which makes it harder;’
‘It is not a usual topic of conversation - people do not want to know the movements of your bowels and if you are incontinent’
‘At work the problem is that I don't want them to see me as the employee with Crohn's, so in a new job I wait until I've established myself before I tell them’
Other people’s reactions
It’s my business
Protecting others
‘I worry about the reaction from others (I know of people who have been attacked due their sexual orientation);’ ‘My family wouldn’t accept me being gay even though they know I live with a woman, they think we are friends!.’
‘questions about another person's sexual orientation are not the first thing I wish to know about them - so I tend to assume that it is the same for them about me ...it’s obvious to me that I am gay, and so do not feel the need to spell it out to everyone’
‘I would find it difficult to discuss with anyone who I feel may turn it against me or if it would have a negative effect upon them.’
Help & support ‘I think people should recognise we all have special needs and personal issues but... we can’t expect people to know if we do not tell them. It is part of me and easier to be open than to have people talking
It’s who I am behind back about my exhaustion or need to know where toilets are or not want to share facilities in accommodation if travelling with friends etc - I guess I just expect people to understand it, but I help them out with clear facts of what I need in the way of reasonable adjustments’
‘Being gay is part and parcel of my identity and life. I have taken the conscious choice to be as open as
GAY AND LESBIAN PEOPLE WITH IBD 27 share information about your sexual orientation, please try and explain why it is not difficult for you
6. Please use this space to tell us anything else you think we should know about coming out about your sexual identity, or telling others about your IBD / illness identity, or both
Revealing one identity is harder than revealing the other
Using the same techniques to come out possible, with all peers and contacts’
‘I do not like pretending to be someone I am not so will say I am gay in context with the conversation’
‘It is part of who I am and my life. I have a partner who I love greatly - I refuse to pretend he doesn’t exist’
“Coming out is such a bigger issue that causes much more problems for the gay / lesbian person’
‘I think sexual identity has always been more difficult topic to talk about mainly because all the cultural and religious reasons. Illness is usually more accepted - I feel’
‘Coming out for me was probably easier than discussing my IBD - you can see campness, but not always when someone is poorly’
‘I feel there is a connection with how I tell people I am gay and how I tell people I have IBD’
‘I think that having experience of having to explain about what can be sensitive issues can help when telling others about IBD as with b eing gay it’s part of everyday life as you are constantly coming out.’
Table 2: Questions and prompts to promote free-text expansion on reported quantitative data in Phase One of the study, with a sample of responses
GAY AND LESBIAN PEOPLE WITH IBD
Variable
28
Difficulty of coming out
Degree of outness
IBD
Mean (SD)
3.9 (2.7)
4.9 (1.4)
Sexual Orientation
Mean (SD)
3.9 (3.0)
5.1 (1.7)
P-value
0.95
0.48
Table 3: Difficulty of coming out (0-10 scale: 0 = not at all difficult, 10 = extremely difficult, impossible) and degree of outness about IBD (0-7 scale: 0 = not out at all, 7 = out to everybody) compared with the same variables for sexual orientation; statistical analysis using the paired t-test, comparing a paired response from each individual on the two scales
35
30
25
20
15
10
5
0
Share when necessary
Wait for opportunity
Steer the conversation
Ensure close friends know
Ensure work colleagues know
Ensure manager knows
Never tell anyone
Coming out about sexual orientation Coming out about IBD
Figure 2: Techniques and intentions for coming out about sexual orientation, and about IBD
GAY AND LESBIAN PEOPLE WITH IBD
Concern
29
GL ranking Mean Score for GL respondents
Range 0-8 (SD)
2.9 (2.1)
3.2 (2.3)
4.4 (2.0)
4.7 (2.1)
5.0 (1.9)
5.2 (2.4)
5.2 (1.8)
5.5 (2.4)
General IBD population ranking
(Casati et al 2000)
Energy / Fatigue
Control
Not reaching full potential
Body Image
Feeling a Burden
Feeling Dirty
Isolation and Fear
Lack of Information
1 (most important)
2
3
4
5
6=
6=
8 (least important)
Table 4: The order of disease-related concerns of GL and non-GL people with IBD using the concerns identified by Casati et al (2000).
5
7
6
3
4
8
1
2