Liver Function Tests
advertisement

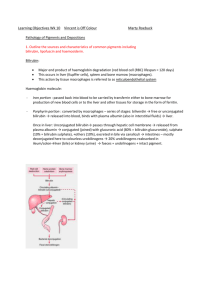
Liver Function Tests Contents: • Structural Unit • Physiology • Liver Function Tests • Bilirubin Metabolism • Reticulo-endothelial System • Hepatic uptake • Conjugation • Secretion of bilirubin into bile • Jaundice • Congenital Hyperbilirubinemias • Serum Enzymes in liver disease Introduction: The liver is the largest organ in the body It consists of two main lobes that together weigh from 1400 to 1600 g in the normal adult It is reddish brown in color and has a rich blood supply 1500 ml/min from two major vessels, the hepatic artery and the portal vein The hepatic artery, a branch of the aorta, contributes 20 % of the blood supply and provides most of the oxygen requirement The portal vein , which drains the gastrointestinal tract, transports the most recently absorbed materials from the intestines to the liver Structural Unit: The lobule which measures 1-2 mm in diameter, forms the structural unit of the liver. It is composed of cords of liver cells (hepatocytes) radiating from a central vein. The boundary of each lobule is formed by a portal tract made up of connective tissue containing a branch of the hepatic artery ,portal vein and bile duct . Human Liver Cell ortal tract containing Hepatic a., Portal vein and bile duct Between the cords of the liver cells are vascular spaces, called sinusoids, that are lined by endothelial cells and Kupffer’s cells The Kupffer’s cells are phagocytic macrophages capable of ingesting bacteria or other foreign material from the blood that flows through the sinusoids Primary bile canaliculi are located between the hepatocytes Hepatocytes form 60% , Kupffer’s cells 30%, endothelial cells, connective tissue and bile ducts 10% of the liver Physiology: The liver has a central role in the metabolism of carbohydrates, lipids, proteins, vitamins and hormones, as well as a role as a storage and excretory organ. It has an important role in detoxification and drug metabolism. Major Synthetic Activity of the liver: • Synthesis of proteins, carbohydrates, and lipids. • The liver plays an important role in synthesizing albumin and the majority of the - and - globulins. • All the blood-clotting factors (except VIII) are also synthesized in the liver. • Deamination of glutamate in the liver is the primary source of ammonia, which is then converted to urea. • The synthesis and metabolism of carbohydrates is also centered in the liver (Glucose is converted to glycogen, a portion of which is stored in the liver and later reconverted to glucose as necessary). • An additional important liver function is gluconeogenesis from amino acids. • Fat is formed from carbohydrates in the liver when nutrition is adequate and the demand for glucose is being met from dietary sources. • The liver also plays a key role in the metabolism of fat. • It is the major site for the removal of chylomicron remnants and for the conversion of acetyl CoA to fatty acids, triglycerides, and cholesterol. • Metabolism of cholesterol into bile acids also occurs in the liver. • Very low-density lipoproteins (VLDL), which are responsible for transporting triglycerides into the tissues, are synthesized primarily in the liver. • High-density lipoproteins (HDL) are also made in the liver. • Formation of ketone bodies occurs almost exclusively in the liver (When the demand for gluconeogenesis depletes oxaloacetate and acetyl CoA cannot be converted rapidly enough to citrate, acetyl CoA accumulates, and a decyclase in the liver liberates ketone bodies into the blood). • The liver is the storage site for all the fat-soluble vitamins (A, D, E, and K) and several water-soluble vitamins, such as B12. • Another vitamin-related function is the conversion of carotene into vitamin A. • The liver is the source of somatomedin (an insulin-like factor that mediates the activity of growth hormone) and angiotensinogen, and is a major site of metabolic clearance of many other hormones. Liver function Function Tests: The routine liver tests include the measurement of : - Total , direct and indirect bilirubin - Total proteins and albumin - Liver enzymes include : ALT ( Alanine transaminase ) AST ( Aspartate transaminase ) AlP ( Alkaline phosphatase ) GGT ( - Glutamyl transferase ) Not all of these tests are related to the functions of the liver. Except for the screening of healthy people (for insurance examinations or occupational medicine), liver function tests are usually employed in patients to: Confirm a clinical suspicion of the presence of liver disease. Give an idea about the severity and prognosis of the liver disease. Follow up the disease and evaluate therapy. Arrive at a differential diagnosis (e.g. cholestatic vs hepatocellular liver disease). Bilirubin Metabolism 1. Reticulo-endothelial System: It is mainly in liver, spleen and bone marrow. 80% of bilirubin formed from heme each day arise from red blood cells. The remaining 20% comes from red cell precursors destroyed in the bone marrow (ineffective erythropoiesis), and from other heme proteins such as myoglobin, cytochromes, catalase and peroxidase. Iron is removed from the heme molecule and the porphyrin ring is opened to form bilirubin. Bilirubin is soluble in lipid solvents but almost insoluble in water. These characteristics enable it to cross cell membrane readily, but special mechanisms are needed to make it water-soluble for carriage in plasma by protein-binding mainly to albumin forming indirect or unconjugated bilirubin. In this form, it does not readily enter most tissues, nor it is filtered at the glomerulus. The maximum capacity of albumin for bilirubin is 340 mol/L. Above this, it will lead to kernicterus in the newborn babies. 2. Liver: a) Hepatic uptake: The bilirubin-albumin complex appears to be associated by receptors on the plasma membrane of the hepatocytes, bilirubin taken up by a specific carrier (facilitated diffusion), leaving albumin in the plasma. b) Conjugation: Conjugation of bilirubin within the hepatocytes makes it water-soluble. The enzyme is BilirubinUDP-glucuronyl transferase forms bilirubin –diglucuronide (direct or conjugated bilirubin). c) Secretion of bilirubin into bile: Occurs against a high concentration gradient, a carrier mediated energy dependant process (active secretion). 3. Intestine: Bilirubin diglucuronide is degraded by bacterial action, mainly in the colon, being deconjugated and then converted into a mixture of compounds collectively termed urobilinogen (stercobilinogen). Urobilinogen is water-soluble, mostly excreted in the feces but a small percentage (20%) is reabsorbed and then mostly re-excreted by the liver After excretion, urobilinogen (colorless) is oxidized to urobilin (stercobilin) which is brown gives stools its color. Some of the reabsorbed urobilinogen passes through the liver into the systemic circulation and is then excreted in the urine (urobilin) gives the urine its yellow color. Jaundice: Jaundice is the yellowish discoloration of the skin and sclera due to hyperbilirubinemia. Bilirubin is a yellow pigment, its normal plasma level is 2-17 mol/L. Normally, more than 95% of bilirubin in the plasma is indirect (unconjugated). Jaundice becomes clinically apparent when the plasma bilirubin exceeds 50 mol/L. Jaundice may be classified into: 1) Pre-hepatic Jaundice: The production rate of bilirubin is increased, exceeding the excretory capacity of the liver. Overproduction of bilirubin occurs in all forms of hemolytic anemia, less commonly, in conditions where there is much ineffective erythropoiesis (e.g. pernicious anemia). Hematomas can also cause pre- hepatic jaundice. There is increase in plasma indirect (unconjugated) bilirubin. Bilirubin is not excreted in urine. Urinary urobilinogen concentration is increased. 2) Hepatocellular Jaundice: Hepatocellular damage due to viral hepatitis or toxins may interfere with the uptake of bilirubin, or with its conjugation or with secretion of conjugated bilirubin into bile. Both indirect and direct hyperbilirubinemia may occur in hepatocellular jaundice. Bilirubin and excess urobilinogen are found in urine . 3) Obstructive (Cholestatic) Jaundice: It is due to impaction of gallstones in the common bile duct or carcinoma of the head of pancreas or of the biliary tree. Jaundice is due to conjugated (direct) bilirubin. Bilirubin is detected in urine. Congenital Hyperbilirubinemias: They are all due to inherited defects in the mechanism of bilirubin transport. 1) Gilbert’s Disease (Syndrome): It is a common congenital disorder (autosomal dominant) of bilirubin transport affecting approximately 2% of the population, males more affected than females. The pathogenesis of the disease is complex. The activity of UDP-glucuronyl transferase is reduced and defects in the uptake of bilirubin by hepatocytes also occur. Gilbert’s disease characteristically causes mild fluctuating jaundice. Most patients have a plasma bilirubin less than 50 mol/L. Hemolysis is absent , other liver function tests are normal and there are no histological changes in the liver. § Gilbert’s disease is a benign condition and life expectancy is normal. It often presents in young adults and must be differentiated from other causes of unconjugated hyperbilirubinemia, such as hemolysis or hepatitis. In Gilbert’s disease, bilirubin concentrations increase with a 400 Kcal/day for 72 hours diet, and fall following phenobarbitone administration. Crigler-Najjar Syndrome )2 : This rare condition is due to low activity of bilirubin UDP-glucuronyl transferase ,gives rise to severe hyperbilirubinemia in neonates, leading to kernicterus and often early death . 3) Dubin –Johnson Syndrome and Rotor’s Syndrome: These rare disorders are characterized by a benign conjugated hyperbilirubinemia, accompanied by bilirubinuria. § In both syndromes, there is a defect in the transfer of conjugated bilirubin into the biliary canaliculi. § Urinary coproporphyrins are normal in patients with Dubin-Johnson syndrome, but increased in Rotor’s syndrome. A blackish-brown pigment is found in the liver in Dubin-Johnson but not in Rotor’s syndrome. Albumin: § Albumin has a long half-life of 20 days and levels fall slowly if no synthesis occur. Thus, serum albumin is usually normal in acute hepatitis. However, in chronic liver diseases such as cirrhosis, impaired synthesis may lead to low serum levels. § Serum albumin levels may be low due to loss into urine, gut or into a third compartment (ascitis). Serum globulins are usually increased in cirrhosis. Serum Enzymes in liver disease: a) Aminotransferases (ALT & AST): § Aminotransferases are involved in amino acid metabolism. § AST occurs in both the cytosol and mitochondria of cells while ALT is a cytosolic enzyme. § Increased amounts of both transaminases leak from inflamed or damaged hepatocytes due to acute or chronic hepatitis. § ALT is more specific for liver disease than AST b) Alkaline Phosphatase (ALP): • Originates from the liver, bone (reflecting osteoblastic activity) and the placenta. • Levels of ALP increase in cholestasis, mainly because of increased synthesis. 3. - Glutamyl transferase (GGT): • Increased serum levels of GGT are found in both hepatocellular and cholestatic disease. § Higher levels are found in cholestasis. Increased synthesis of GGT is induced by excessive ethanol intake. N.B. Hepatic Enzymes: § ALT and AST levels are raised mainly in hepatocellular disease. § AlP level is raised mainly in obstructive disease. § The increased in serum GGT levels are modest in hepatocellular disease and marked in obstructive disease.