Priority setting for voluntary services
advertisement

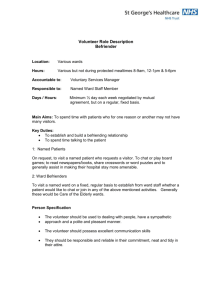
Priority Setting for Voluntary Services “Volunteering has a huge potential role in the context of more flexible, responsive and patient focussed health and social care services.” (Ivan Lewis, former Health Minister) S.U.H.T. Voluntary Services remains responsible for: Interpreters Service Work Experience Voluntary Services The intention is that we shall not either extend nor reduce the service from this defined scope. The purpose of this document is to identify the key strategic steps in enabling the Voluntary Services to effectively underpin the work of the Patient Improvement Framework. Whilst the delivery of the Framework is a corporate activity drawing on all aspects of the service, there are particular areas where Voluntary Services can add particular value in the delivery of the framework. This document highlights potential areas volunteers could further complement the work of the staff to release them to carry out their role to the benefit of the patient in alignment with performance and Trust objectives. Interpreters Service The increase in requests for interpreters remains a pressure on the in-house service. The retention rate of existing, (mainly Southampton General Hospital staff,) volunteer interpreters needs addressing. Interpreters need to be recognised in some way, i.e. KSF (Knowledge Skills Framework), appraisal or honorarium. There is a continual need to recruit and train volunteers to cover a diverse range of languages. The priority for this area is also to evaluate the service from a patient’s perspective this could be to establish a patient satisfaction survey. Work Experience A key challenge for SUHT is to maintain staffing levels in the face of increased numbers of staff reaching retirement age, a finite pool of school and college leavers and increased choice and competition for young people from other sectors. The Government has made a commitment to keep young people in education or training until the age of 19, and linked this policy to changes in the school curriculum designed to increase ‘employability’ skills. The development of a new health and social care diploma to realise one of the major priorities of the 14-19 education agenda and ensure more systematic opportunities for widening access and progression into health service careers will be one of the biggest challenges for our work experience programmes. We are actively working with schools and colleges to identify the needs of the curriculum and students. We must invest in our future workforce and ensure we are the hospital of first choice for tomorrows’ future staff. This work also enhances our reputation in the community. Voluntary Services The hospital is part of the local community. Tapping into that community provides us with a vibrant workforce and advocates. Volunteers play a variety of roles, at all levels, providing mutual benefit to staff, patients and visitors within the Trust. Their contribution can improve outcomes for a whole range of groups and across a range of care and planning pathways. Baseline Assessment In SUHT there are 866 volunteers registered as helping at Southampton General and Princess Anne Hospitals, in addition to this there are a further 170 at Countess Mountbatten House. (Appendix A.) This figure includes the voluntary organisations registered with us. There are currently 498 hospital volunteers these are currently deployed across a number of departments, (Appendix B.) The Voluntary Services Manager, in response to a direct request from staff, currently manages requests for volunteer support. Volunteers are interviewed, skills and strengths identified, then matched to Trust needs and volunteers are assigned to a vacancy. The current deployment of volunteers across Divisions and wards are shown in Appendix C and D. Appendix C shows the potential should all volunteers come in every week, Appendix D shows actual signing in during April 2008. Volunteers are encouraged to sign in every time in the Trust, however, many do not. they forget, reception is closed etc. Patient Improvement Framework Particular ‘Hot Spot’ areas identified by staff Appendix E shows the areas volunteers are currently complementing the work of the staff to support both them and patients for the Trust. The shaded areas on this table refer to areas where volunteers are awaiting training subsequent to becoming active. Many of these areas currently support staff in the ‘Releasing Time to Care’ (RTTC) initiative, however, we continue to engage with staff to ensure volunteers are being as fully utilised as possible. In the case of RTTC, we are piloting a volunteer trainer working along side a Senior Sister on Elderly Care to identify further areas that volunteers are able to assist or further assist to support this work. Appropriate tasks identified so far include, decanting stores (ie putting stock on shelves), making up the basic ward supply racks, making up admission and discharge packs. Emergency Department – Patient information and customer service Voluntary Services Manager (VSM) worked in conjunction with the service improvement redesign team to help address the issues within this department. Appropriate tasks for a volunteer to undertake to support staff were identified and implemented. Volunteers piloted this and have been placed. (See task description) * Possible increase in volunteer inputincrease in volunteer input to sit with patients, meet and greet, run errands, information and general support staff and patients, also escort patients to other departments, i.e. radiology. Wards with limited administration and clerical support Ward volunteers have this task as part of their ward role. Voluntary Services Manager to remind volunteers to prioritise this. Staff to be reminded that the Caldicott report and Data Protection clearly states that volunteers should not have access to patient identifiable data. Possible increase in volunteer inputVolunteers to be stationed on the Nurses Station to answer the phone, direct visitors, photocopy routine non-identifiable paperwork, i.e. make up admission and discharge packs, top up stationery etc therefore releasing staff to get on with their proper role with less interruptions (RTTC). This role will not be popular with volunteers; it may be achieved by linking in with Business study course providers and agencies like Wheatsheaf Trust etc to identify potential volunteers who are near work ready but needing experience in the workplace. Escorts – in particular Radiology At the RSH Radiology department there are good teams of SUHT volunteers who cover the busiest clinic times:meeting and greeting patients, escorting them to appointments or other departments, instructing them on the use of gowns and ensuring they maintain their dignity, encouraging patients not to leave valuables in the changing rooms, talking to them, re-assuring them and helping keep a smooth flow of patients through the clinic. Directing patients to the cafes and rest rooms. * Possible increase in volunteer inputThere are some volunteers in the SUHT Radiology department, however they are not used as Escort volunteers. They is potential for this. Hospital guides operate 9 – 4 Monday – Friday these volunteers are not utilised for this role either, although they could be, staff need to request a volunteer to undertake this task. Volunteers have been offered to staff there and have not been contacted. Liase with Radiology staff to ensure they contact volunteers to help. Falls * Possible increase in volunteer inputWard volunteers need to be alerted or check with staff which patients need assistance and call staff when the patient moves. Encourage patients to wear slippers or sensible footwear. Vigilant regarding wet floors. Infection Prevention Volunteers re-stock Infection Prevention leaflets around the Trust and support team as required. Volunteers train in Infection Prevention as part of their Induction and are encouraged to challenge staff; visitors and patients to ensure best practice. *Possible increase in volunteer inputRegular/termly ‘blitz’ of the Trust with infection control leaflets, gel etc. Guides to be Infection prevention ambassadors, offering hand gel to all on arrival. Medicines/ Discharge Volunteers placed in the Discharge lounge are fully utilised. They regularly pick up T.T.O’s as part of their role. At least one volunteer is in attendance from 10 – 5, Monday - Friday and are very much an active part of the Discharge team, additional volunteers have been placed on what is perceived as the busiest times to ensure staff are supported as much as possible. They collect patients from wards and take them to the Discharge room, collect forgotten items, serve refreshments, run errands, survey patients using the PDAs, sit and talk to patients, collect meals and generally help wherever needed. *Possible increase in volunteer inputA pharmacy runner volunteer? Assigned to pharmacy for peak times to ‘run’ T.T.Os to specific patients. Nutrition Volunteers are trained to help with feeding, declutter overbed tables, replenish water, talk about food to stimulate saliva glands, work with staff to identify patients who require assistance with cutting up food. Ensuring meals are delivered as soon as possible after arriving. Help make meal times a more social event and encourage patients to eat. This releases staff to attend patients with more acute needs. * Possible increase in volunteer inputFrom 30th October 2008, selected volunteers are to pilot a new feeding training programme working with Nutrition and Dietetics and speech and language staff. This pilot will take place on Tuesday and Thursday lunch times on G9 and will be closely monitored by staff. If this is successful it will be necessary to re-launch the role and recruit to it specifically. Training, supervision and support is paramount to make this a safe and successful role. Thromboprophylaxis There are no clear opportunities for volunteers to support and complement the work of staff in this area. Communication issues in general and in particular around ensuring information in languages other than English This is clearly an area for increased volunteer input and to these ends, a second interpreter’s course is currently being run with 20 volunteers and staff training to be interpreters. Consent forms from the Department of Health are issued to all interpreters in the interpreter’s own language to take to interpreter sessions with patients. Retention of interpreters, as previously stated, is a real issue and needs addressing to ensure an effective and efficient service. The service also needs evaluation from the patients’ perspective. Volunteers, as requested, by staff undertook a telephone audit. This was not overly successful with the questions and process being changed and restarted, no room supplied to carry out the task, no desk or phone were made available to volunteers and little encouragement, feedback or support. Volunteers ‘voted with their feet’ and did not continue to complete the audit, which, they said, had not been thought through properly. We were asked for many volunteers daily and full time, which is totally impractical, especially as the requester would not supply space a chair, or a phone to complete this task! PDA, Patient Survey All hospital volunteers are currently trained in the use of PDAs as part of their initial training. This is not a popular role for volunteers, they cite many different reasons ranging from staff not being very receptive, to patients not wanting to feedback to the role not being what potential medic volunteers want from their time in the Trust. Each of these issues are being addressed, Potential volunteers are told that this is the Trust priority and this role is a firm foundation for future courses as it aids good communication skills and how to approach patients. Volunteers are encouraged to observe the changes made to improve the service because of this survey. All schools and colleges who visit weekly are now trained in this form of volunteering, Hardley College, Testwood School and King Edward’s College being the main ones. *Possible increase in volunteer inputWith the onset of the Diploma, colleges and schools will have to liase with a health care provider to facilitate the 40 hours of contact needed to complete the course. There is potential here to involve further education providers to engage with this Trust to satisfy the course criteria and increase the number of Patient surveys completed, albeit term time only. Out Patient Departments Our out patient departments are the windows or showroom of this Trust and as such are a most appropriate area to support staff. There are some superb areas of good practice, for example the Laryngectamy Out patient department, where past patients support staff and patients by: - meeting and greeting patients, keeping an attendance register, encouraging patients to access information and other service providers approved by staff, making teas and coffees, befriending and talking to patients, and basically showing them there is life after a laryngectomy. This type of OPD volunteer role is rolled out as requested in the Trust for example, Audiology, orthopaedics, Child Health, but not uniformly, the good practice is found in ‘pockets’; a great deal depends on the member of staff. *Possible increase in volunteer inputFeature the role and encourage out patient departments to ‘adopt’ a volunteer. Make up discharge packs ready for staff use. A possible further effective use of volunteers within SUHT would be to endeavour to address the number of patients failing to attend out patient appointment. A pilot could be undertaken in a department renowned for a high percentage of non-attendees to appointments, ie Physiotherapy. Volunteers could be asked to phone or text elective patients and remind them of their appointments, (in-patient and out-patient). However, this would not be a popular role to recruit to, volunteers are giving the most precious thing they have, their time, they mostly want or require, for their courses, patient contact and to be part of a team. Should the Trust require this role to be developed the VSM would work with other agencies to identify people who are looking to gain a reference or admin skills. The role of the Voluntary Services Manager remains that of matching the needs of the Trust with the needs of the volunteer. Conclusion Many of the areas identified as being ‘hot spots’ do have volunteers active in them. However there is a great deal of work to be completed to ensure Voluntary Services is as effective as possible and will continue to work towards the tactical deployment of volunteers against SUHT strategic priorities in line with documents including: The Trust 20:20 Vision, SUHT Annual Plan, in particular pages 16, 18 Standards for Better Health, Essence of Care, The Patient Improvement Framework, Patient Experience Strategy, South Central NHS, our NHS, our Future – ‘Towards a Healthier Future’ Skills For Health – Sector Skills Agreement for Executive Summary (England) Volunteering England – Manifesto for Change. and other national and local initiatives. A great deal of ongoing work must be around communication of volunteer roles to staff. Of prioritising the volunteer workforce we have, to where the Trust need is. Of keeping aware and abreast of the changes in Trust priorities to ensure volunteers are ready and trained appropriately to meet the challenges of the day and the future. Volunteering is not the answer to all, however, carefully managed, volunteers are able to support the staff of this Trust to release them to care for our patients and make us a world renowned Trust, volunteers are proud to be part of. Comments in a card from a relative – To all the volunteers I just wanted you to know that you are very much appreciated. I could not have managed while my husband was here without your help in the different wards. I admire you all J Where Volunteers Help Hospital Broadcasting 14% Hospital Volunteers 63% 866 Volunteers League of Friends (x2) 20% Radio Lollipop 3% Appendix A Appendix B Appendix C OVERALL VOLUNTEERS PLACEMENTS AND HOURS ATTENDED EXTRACTED FROM PERSONNEL FILES AT SUHT – AUGUST 2008 DIVISION 1 – SURGICAL DIVISION 2 – UNSCHEDULED CARE Wards Trauma & Orthopaedics F1 2 vols F2 6 vols F3 4 vols F4 2 vols 6 hours 14 hours 13 hours 11 hours Surgical F5 F9 E5 E7 E8 5 vols 2 vols 3 vols 4 vols 7 vols 13 hours 6 hours 10 hours 16 hours 20 hours Eye Ward 1 vol 2 hours Surgical Admin Orthopaedics OPD Fracture OPD Surgical OPD Amputees Clinic Eye Hospital Admin Endoscopy Clinic Division 1 Totals 8 vols 4 vols 1 vol 1 vol 4 vol 1 vol 1 vol 22 hours 16 hours 3 hours 7 hours 7 hours 3 hours 2 hours 56 Vols 171 Hours Elderly Care G5 G6 G7 G8 G9 F8 Stroke Baddesley Ward 3 vols 20 vols 85 hours 6 vols 15 hours 2 vols 6 hours 10 vols 43 hours 1 vol 3 hours 3 vols 7 hours 7 hours Oncology C3 C4 General Oncology Macmillan Centre 1 vol 5 vols 6 vols 23 vols 4hours 18 hours 12 hours 80 hours Time 4 You Oncology Pharmacy Acute Medical Unit A&E 7 vols 1 vol 18 vols 12 vols 16 hours 6 hours 46 hours 28 hours Medical D5 D6 D7 D8 3 vols 3 vols 2 vols 3 vols 7 hours 6 hours 8 hours 8 hours DVT Clinic 3 vols 21 hours Division 2 Totals 132 Vols 426 hours DIVISION 3 – WOMEN & CHILDREN Princess Anne Hospital Burley Ward Broadlands Ward Bramshaw Ward Bassett Ward Delivery Suite Neo-Natal Admin OPD Ultrasound Breastfeeding Support Breast Screening 6 vols 5 vols 2 vols 2 vols 19 vols 3 vols 3 vols 2 vol 1 vol 20 vols 4 vols 18 hours 15 hours 6 hours 6 hours 53 hours 9 hours 8 hours 13 hours 4 hours 37 hours 11 hours G1 G2 G3 G4 Piam Brown Ward Children’s OPD Child Protection Child X-ray Bursledon House 2 vols 2 vols 1 vol 5 hours 12 hours 5 hours 6 vols 14 vols 1 vols 1 vol 5 vols 17 hours 53 hours 3 hours 2 hours 19 hours Division 3 Totals 52 Vols 166 Hours Child Health DIVISION 4 – SPECIAL SERVICES DIVISION 5 – DIAGNOSTICS & THERAPIES DIVISION 6 – TRUST HQ Cardiothoracic D2 D4 E1 E2 E3 E4 2 vols 5 vols 7 vols 5 vols 6 vols 4 vols Neurological Gen Neuro D & E wards Rehabilitation 3 vols 9 hours 14 vols 49 hours 5 vols 14 hours Radiology X-ray Infection Control Patient Appliances Haematology Speech Therapy Physiotherapy Pharmacy Occupational Health Dietetics Pathology RSH Audiology Discharge Lounge 2 vols 6 vols 1 vol 1 vol 7 vols 2 vols 3 vols 1 vol 2 vols 2 vols 1 vol 4 vol 9 vols Chaplaincy Admin/Clerical PALS PDA Cashier Talking Echo Complaints Library Hospital Charities Guides 61 vols 26 vols 1 vol 22 vols 2 vols 1 vol 1 vol 1 vol 1 vol 18 vols Maxillofacial 1 vol Division 4 Totals 52 Vols 166 hours Division 5 Totals 41 Vols 156 Hours Division 6 Totals 124 Vols 409 Hours 6 hours 24 hours 19 hours 16 hours 15 hours 12 hours 12 hours 19 hours 3 hours 2 hours 26 hours 9 hours 8 hours 3 hours 4 hours 12 hours 8 hours 15 hours 35 hours 134 hours 116 hours 3 hours 48 hours 4 hours 1 hour 4 hours 4 hours 4 hours 91 hours 2 hours Grand Total 457 Volunteers 1494 hours divided by 37.5 = 39.84 wte 1494 Hours Radio Lollipop 16 Vols 35 Hours League of Friends 119 Vols 493 Hours Hospital Broadcasting 110 Vols League of Friends – Eye Unit 24 Vols 72 Hours Appendix D SUHT GENERAL VOLUNTEERS – HOURS WORKED AND PLACEMENT- BY DIVISIONS APRIL 2008 WEEKS 1 2 3 4 TOTAL SURGICAL (Division 1) SHIFTS HOURS 10 33 10 30 7 21 7 22 34 106 UNSCHEDULED CARE (Division 2) SHIFTS HOURS 33 110 34 97 36 104 35 108 138 419 Total c/f WEEKS 1 2 3 4 TOTAL SPECIAL SERVICES (Division 4) SHIFTS HOURS 22 79 24 100 24 127 22 85 92 391 WOMEN&CHILDREN (Division 3) SHIFTS HOURS 14 52 8 31 10 35 13 45 45 163 217 shifts DIAGNOSTICS&THERAPIES (Division 5) SHIFTS HOURS 12 43 15 53 11 39 18 61 56 196 Total c/f Per Week Monthly total Total c/f Totals b/f MACMILLAN SHI HOURS FTS 23 80 92 Shifts Shifts 320 204 655 GUIDES SHIFTS HOURS hours - 688 Trust HQ (Division 6) SHIFTS HOURS 15 50 27 85 27 77 17 64 86 276 Shifts 234 RSH SHIFTS HOURS 10 91 10 37 40 364 40 148 hours - 863 PAH SHIFTS HOURS hours - 936 hours – 2487 Average week for staff p.p is - 37 ½ hour week x 4 Weeks = 150 Hours per 4 weeks. 8 32 26 104 Appendix E April Volunteer Hours Total = 2487 divided by 150 (f/t hours for 4 weeks ) equates to 16.58 full time members of staff nterpreters Discharge Lounge Guides/ Escorts Feeding Orthopaedics Laranjectomy Macmillan Red Cross PAT Dog Time 4You O.P.D. ie X-ray Ward Volunteer PDA Volunteer Patient Clinical Outcomes Stroke Heart Trauma Heart Attack Centre Diabetes Patient Experience Privacy & Dignity Communication Information Single Sex Accommodation Admission Process Patient Feedback Patient Safety Thromboprophylaxix Nutrition Acute Patients Infection Prevention Falls Reducing Medication Errors