Pharmacology 21a – Anti-Microbial Drugs
advertisement

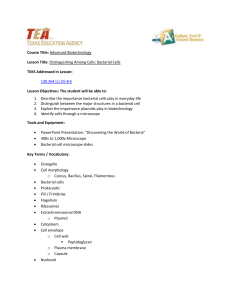
Pharmacology 21a - Anti-Microbial Drugs Anil Chopra 1. Understand the meaning of selective toxicity. How do human cells differ from 2. 3. 4. 5. 6. 7. microbes that offer us drug targets? What are the main classes of antibiotic drugs and how can they be distinguished according to their mechanisms of action. By what mechanisms are bacteria and other microbes becoming resistant to drugs? Understand why tuberculosis is a killer disease again and what are the modern ideas/drugs for the treatment of tuberculosis. Understand the types of fungal infections that can affect us and how can we utilise drugs to specifically target the fungus with affecting the host? Be aware of the different types of virus, how they use the host cell to replicate and some of the common diseases they can cause. What are the mechanisms of action of antiviral drugs and what are their side effects. Antimicrobial drugs need to kill or disable parasites without doing damage to the host cells. This is achieved by exploitation of different proteins and biochemicals that microbes possess. Generally, the more evolutionarily distant, the easier they are to kill. Differences between Prokaryotic and Eukaryotic Cells • • • • Cell Wall – Contains peptidoglycan, supports the underlying membrane which is subject to osmotic pressure. Genetic information – No nucleus, genetic material forms a single chromosome which lies loose in the cytoplasm. Plasma membrane – Bacterial membranes contain no sterols which may result in differential penetration to chemicals. Protein synthesis – Bacterial ribosome’s consist of 50s and 30s subunits, whilst mammalian ribosome’s consist of 60s and 40s subunits. Selective Toxicity Selective toxicity depends on the existence of exploitable biochemical differences between the microbe and host cell The degree of exploitable differences depends on how far apart the host and parasite are evolutionary Prokaryotes are evolutionary very different to eukaryotes and so are easier to target Eukaryotes are more similar biochemically to host cells and so are more difficult to target Drugs Which Affect Folate Name Sulphanilamide, sulphamethazole. Usage - Anti-Microbial – it is bacteriostatic. Mode of Action Folate is required for DNA synthesis in all organisms. Folate is taken into eukaryotic cells whereas bacterial cells have to synthesise folate. P-aminobenzoic acid is essential for the synthesis of folic acid in bacteria. Sulphanilamide competes with P-aminobenzoic acid for its enzyme dihydropteroate which results in bacteriostasis. The bacteria are not killed but they can no longer divide which makes it easier for the host to kill the bacteria. Side Effects and Pharmacokinetics - Readily absorbed in the GI tract and maximum plasma conc. is reached within 4-6 hours Side effects - nausea, vomiting, headache - mental depression - rarely cause hepatitis, hypersensitivity reaction and bone marrow suppression. Name trimethoprim Usage – Anti-Microbial – it is bacteriostatic. Generally used for urinary tract and respiratory infections. Mode of Action – in order to synthesise thymidilate, (an important co-factor in DNA synthesis) folate is needed in the form of tetrahydrofolate. This pathway can be inhibited by a folate antagonist (which inhibits the enzyme dihydrofolate reductase) but trimethoprim only inhibits this pathway in bacteria (not humans). Side Effects and Pharmacokinetics - Administered orally Side effects - Nausea, vomiting - Skin rashes Drug Combination Name - co-trimoxazole. Made up from - sulphamethazole and trimethoprim. Usage – anti-microbial. Used for infections with pneumocystis carinii, which causes pneumonia in patients with AIDS, co-trimoxazole is used in high doses. Mode of Action Since sulphonamides affect the earlier stage in the same metabolic pathway i.e. folate synthesis, they potentate the actions of trimethoprim. When given in combination the drugs are effective at one-tenth or less of what would be needed if each drug was given on its own. Drugs That Interfere with The Synthesis of Peptidoglycan Peptidoglycan cell walls are found only in bacteria. They consists of layers of multiple backbones of amino sugars – alternating N-acetyl-glucosamine and Nacetylmuramic acid residues forming a lattice structure sometimes many layers thick. It allows bacteria to resist osmotic pressure. Schematic diagram of the biosynthesis of peptidoglycan in a bacterial cell (e.g. S. aureus ). M UDP Glycine (gly) residues Amino acids of the peptide side - chain on muramic acid M UDP UMP G Pi UDP (gly) 5 UDP Inside C 55 lipid M P P C 55 lipid P P C 55 lipid G M P C 55 lipid P G M P P C 55 lipid Cell membrane P P G G P C 55 lipid M Outside M ß- lactam antibiotics Penicillins Cephalosporins Monobactams Carbapenems (The acceptor) Name – penicillin Usage – anti-microbials. Different penicillins used for different microbes. Mode of Action Penicillin is a β-lactam antibiotic. It is formed from 6-aminopenillanic acid, which consists of a thiazolidine ring linked to a β-lactam ring. They interfere with the synthesis of the peptidoglycan in the bacterial cell wall by inhibiting the transpeptidation enzyme causing the cell to collapse. Penicillin’s may be destroyed by enzymes - amidases and b-lactamases. Side Effects and Pharmacokinetics - - Metabolised by liver and excreted in urine When given orally different types of penicillins (over 50) have differing degrees of absorption depending on stability in acid and food interactions Widely distributed in body fluids – passing into joints, pleural and pericardial cavities, bile, saliva, milk and across the placenta As lipid insoluble do not enter mammalian cells and so do not readily cross the BBB – except when meninges are inflamed when can cross in therapeutic doses Elimination is mainly renal – 90% by tubular secretion Can produce drug resistance: - β-lactamases can be produced by certain bacteria, and now these drug-resistant bactera have sepread significantly. The most resistant are streptococci. The solution is to co-administer a β-lactamase inhibitor. - The outer membrane of bacteria are becoming less permeable. - The binding sites for penicillin are changing by mutation. Side effects can include hypersensitivity reactions and GI disturbances due to their effect on gut flora. Name Cephalosporins Cephalexin (oral), Cefuroxime & Cefotaxime (parenteral). Usage – used as an antimicrobial especially in bacterial meningitis. Mode of Action These too, inhibit the synthesis of the peptidoglycan cell wall. Side Effects and Pharmacokinetics Also have produced bacterial resistance due to production of β lactamases hence it is normally combined with other antibiotics. - Can be given orally, parenerally, intravenously or intramuscularly. - Widely distributed in the body and some can pass the blood-brain barrier. - Metabolised by the liver and excreted in the urine and in bile. - Some can cross the blood brain barrier e.g. cefotaxime can be used in bacterial meningitis. Side Effects: • Hypersensitivity reactions. • Nephrotoxicity has been reported (especially with cephradine). • Diarrhoea can occur with oral cephalosprins. Drugs that Affect Protein Synthesis Name Tetracylcines: tetracyclin, doxycycline, minocycline Usage – they have an incredibly broad spectrum and are able to target gram positive and gram negative bacteria and some protozoa. Mode of Action – these are actively transported into the bacteria where they compete with tRNA for the amino-acid binding site and thus stop the synthesis of proteins. They are bacteriostatic. Side Effects and Pharmacokinetics Have also produced resistance due to mechanisms developed by the bacteria to excrete the tetracyclines out of the bacteria. - Administered orally and parenterally. - Since tetracycline’s chelate metal ions (e.g. iron), forming a non-absorbable complex, absorption is decreased by the presence of milk, certain antacids and iron preparations. - They enter most fluid compartments in the body. - Metabolised in the liver and excreted by the bile and in urine. - T ½ = 2 hrs Side Effects - they can cause GI disturbances by direct irritation and by modification of gut flora. - Because they chelate ions, they can cause deformities and staining in bones and teeth. - Can produce vestibular disturbances and photosensitivity. Name – chloramphenicol Usage – wide-spectrum bacteriostatics. Mode of Action - Chloramphenicol binds to the 50S subunit of the ribosome and inhibits transpeptidation and thus protein synthesis. It is also bacteriostatic. Side Effects and Pharmacokinetics Resistance has developed due to the production of chloramphenicol acetyltransferase. Because it is plasmid mediated, it can be transferred between bacterial species. - Administered orally or parenterally. - Metabolised in the liver and excreted in urine and bile. Side effects include: - depression of bone marrow causing pancytopenia - decrease in all blood cell elements. - Chloramphenicol should be used with great care in new-borns because inadequate inactivation and excretion of the drug can result in 'grey baby syndrome' - vomiting, diarrhoea, flaccidity, low temperature and an ash-grey colour - which carries a 40% mortality rate. - Hypersensitivity reactions can occur, as can gastrointestinal disturbances and other alteration of the intestinal microbial flora. Name Aminoglycosides Gentamicin Usage Effective against many aerobic Gram -ve and some Gram +ve bacteria. Mode of Action Aminoglycosides inhibit bacterial protein synthesis by binding to the 30S subunit of the ribosome, causing an alteration in codon: anticodon recognition. This causes the production of faulty proteins which then do not function. They are bactericidal. Their uptake into the bacterial cells depends on an oxygen dependent active transport system which can be blocked by chloramphenicol. Side Effects and Pharmacokinetics Resistance has developed due to a number of factors: It can be inactivated by bacterial enzymes (the genes for which are coded for on the plasmids). Difficulty in penetration into the bacteria. The solution to this is to co-administer with penicillin. Mutations to the binding site on the 30S subunit of the ribosome. - Administered intravenously or intramuscularly. Cannot be given orally as is polar and will not be absorbed in the GI tract. - Do not enter cells or cross the blood brain barrier. - Metabolised hepatically and excreted in the urine. - Polycations and so highly polar – therefore not absorbed in the GI tract - Binding to plasma proteins is minimal - Do not enter cells or cross the BBB - T1/2 = 2-3hrs - Elimination virtually all by glomerular filtration - Tissue concentrations increase during treatment and can become toxic after 1 week without altered dosing – dose modification needed in long term use Side Effects Toxic in high doses – should be monitored. Ototoxicity involves progressive damage to and destruction of the sensory cells in the cochlea and vestibular organ of the ear. Nephrotoxicity - damage to the kidney tubules. Anti-mycobacterial Agents The two main diseases caused by mycobacteria in humans are tuberculosis and leprosy. The problem is that when phagocytosed, they can survive in phagocytes. Tuberculosis is making a comeback because of drug-resistant strains spreading in third world countries and in prisons and homeless shelters. Drugs Used to Treat Tuberculosis Names Combined isoniazid, rifampicin, pyrazinamide (plus ethambutol if the organism is suspected to be resistant). RIPE. Usage The full combination of drugs is used for the first 2 months and then for the next 4 months only isoniazid and rifampicin are used. Mode of Action Isoniazid: works by inhibiting the synthesis of mycolicacids, important constituents of the cell wall and peculiar to mycobacteria. It is bacteriostatic on resting microbes and can kill dividing organisms. Rifampicin: works by inhibiting RNA polymerase in prokaryotes (not eukaryotes). It is also active against most other Gram +ve bacteria as well as many Gram -ve species. It enters phagocytic cells and can kill intracellular micro-organisms. Pyrazinamide: it causes tuberculostasis in an acidic pH (but does nothing at a neutral pH). It is effective against the intracellular organism in macrophages, since after phagocytosis the organism will be contained in phagolysosomes in which the pH is low. Side Effects and Pharmacokinetics Isoniazid - Administered orally or parenterally. - It can penetrate into most body tissues including necrotic tuberculous lesions. - Metabolised in the liver and excreted in the urine. Genetic differences determine whether this is slow or fast. Slow acetylation have a better therapeutic response. Rifampicin - Administered orally. - Metabolised in the liver and excreted in the urine and bile. - Side effects include GI disturbance and skin ruptures. Pyrazinamide - Administered orally - Distributed around the bodily tissues penetrating well into the meninges. - Metabolised in the liver and excreted in the urine. - Side effects include arthralgia (associated with high concentrations of plasma urates). GI tract upsets, malaise and fever. Anti-Fungal Drugs There are 2 main types of fungal infection (mycoses): Superficial infections - Affecting skin, nails, scalp, mucosal membrane. They can be classified into:o Dermatomycoses - infections of the skin, nails and hair are caused by dermatophytes. The commonest are due to Tinea organisms e.g. Tinea pedis - causing 'athlete’s foot'. o Candidiasis - yeast like organisms which infect the mucous membranes of the mouth (thrush), or vagina, or skin. Systemic infections - Affect deeper tissues and organs. o Primary systemic fungal infections are rare and generally occur in defined endemic areas of the world. In the UK the commonest systemic fungal infection is candidiasis - an infection with a yeast like organism. Name – Nystatin Usage – because it is not absorbed at all by mucous membranes, it is generally used in skin and GI tract fungal infections. Mode of Action – it binds to the bacterial cell membranes where it interferes with permeability and membrane transport functions by forming a hydrophilic ion channel. Nystatin has a selective action, binding avidly to the membranes of fungi and some protozoa, less avidly to mammalian cells and not at all to bacteria. This is because the membranes of fungi contain ergosterol as opposed to cholesterol. Side Effects and Pharmacokinetics - administered topically - Side effects are rare, include nausea and vomiting. Name – miconazole Usage – broad spectrum anti-fungal. Mode of Action – they block the synthesis of ergosterol (in fungal membranes) by blocking the enzyme that converts lanosterol to ergosterol. This changes the fluidity of membranes and interferes with the action of membrane associated enzymes – causing inhibition of replication. Side effects and Pharmacokinetics - Administered by intravenous infusion for systemic infections and orally for infections of the GI tract. - Has a short plasma half life and therefore needs to be given every 8 hours. Side effects include GI disturbances, blood dyscrasias. Anti-Viral Drugs Viruses consist of DNA or RNA wrapped in a protein coat or capsid: DNA viruses: poxvirus (smallpox), herpes viruses (chicken pox, shingles, herpes and glandular fever), adenoviruses (sore throat, conjunctivitis), and papillomaviruses (warts). RNA Viruses: orthomyxoviruses (influenza), paramyxovirus (measles, mumps), picornaviruses (colds, meningitis, poliomyelitis), retroviruses (AIDS), arenavirus (meningitis, Lassa fever). In order to replicate they have to attach to a cell membrane, enter a cell and use its metabolic processes. The nucleic acid of the virus then uses the cell's machinery for synthesising nucleic acid and protein and the manufacture of new virus particles. - As viruses use cellular metabolic machinery it is hard to find effective drug targets There are some virus specific enzymes that can be targeted Most current drugs work while the virus is replicating By the time infection is clinically detectable the process of viral replication is so advanced that intervention is very difficult Name – Acyclovir Usage – has high specificity for the herpes simplex virus and also some effect on cytomegalovirus causing glandular fever. Mode of Action – it is converted to monophosphate by thymidine kinase in viruses (it also occurs in humans but it is converted to triphosphate); it is therefore only adequately activated in infected cells. Acyclovir triphosphate inhibits viral DNApolymerase, terminating the chain. It is 30 times more potent against the herpes virus enzyme than the host enzyme. Side Effects and Pharmacokinetics Resistance is beginning to develop due to changes in the viral genes coding for thymidine kinase or DNA polymerase. - Metabolised in host cells by phosphatases and excreted in the urine. - Administered orally, intravenously and topically - It is widely distributed around the body including the CSF. Side effects • Local inflammation if i.v. • Renal dysfunction • Nausea and headache HIV and its Treatment Name Zidovudine (Azidothymidine) Usage In patients with AIDS, it reduces the incidence of opportunistic infection (e.g. Pneumocystis carnii pneumonia), stabilises weight, reverses HIVassociated thrombocytopenia, stabilises HIV associated dementia and reduces viral load. If it is given to people who are HIV+ but have not developed AIDS, it can dramatically prolong life expectancy. In HIV+ mothers it reduces the risk of transmission of the virus to the foetus by 66%. Mode of Action It is an analogue of thymidine. It works in retroviruses by inhibiting reverse transcriptase. It is converted to its triphosphate form in cells where it then competes with the cellular triphosphates in the formation of the viral DNA by reverse transcriptase. It does not affect α-DNA polymerase in mammalian cells but can affect γ-DNA polymerase in mitochondrion- lead to side effects. Side Effects and Pharmacokinetics Resistance has developed recently due to mutations resulting in amino acid substitutions in the viral reverse transcriptase. The resistant strains can move between targets if the virus is transmitted. - Administered orally but can be given intravenously. - It can pass through mammalian cells and enters the CSF and brain freely. - It is metabolised hepatically and excreted in the urine. Side effects: - anaemia and neutropoenia - uncommonly can include skin rash, insomnia, fever, headache, abnormalities of liver function, and particularly myopathy.