Chest Pain – R/O MI Orders
advertisement

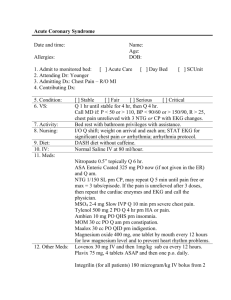
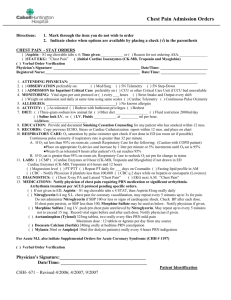
Chest Pain – R/O MI Orders Date and time: Name: Age: DOB: Allergies: 1. Admit to monitored bed: acute care 2. Attending Dr: Younger 3. Admitting Dx: Chest Pain – R/O MI 4. Contributing Dx: 5. Condition: 6. VS: 7. Activity: 8. Nursing: 9. Diet: 10. IV: 11. Meds: [ ] Stable [ ] Fair [ ] Serious [ ] Critical Q 1 hr until stable for 4 hr, then Q 4 hr. Continuous cardiac monitoring. Call MD if: P < 50 or > 110, BP < 90/60 or > 150/90, R > 25, chest pain unrelieved with 3 NTG or CP with EKG changes. Bed rest with bathroom privileges with assistance. May go to activity ad lib after 2 sets of EKGs and cardiac enzymes have been negative. I/O Q shift; weight on arrival and each am; STAT EKG for significant chest pain or arrhythmia; arrhythmia protocol (record a rhythm strip every 6 hours). Clear liquid diet until 4 hours without chest pain and then a DASH diet without caffeine. Normal Saline IV at 80 ml per hour. Nitropaste one inch applied topically Q 6 hr. ASA Enteric Coated 325 mg PO now (if not given in the ER) and Q am. NTG 1/150 SL prn CP, may repeat Q 5 min until pain free or max = 3 tabs/episode or the blood pressure drops below 100 systolic. If the pain is unrelieved after 3 doses, then repeat the cardiac enzymes and EKG and call the physician. MSO4 2-4 mg Slow IVP Q 10 min prn severe chest pain. Tylenol 500 mg 2 PO Q 4 hr prn HA or pain. Ambien 10 mg PO QHS prn insomnia. MOM 30 cc PO Q am prn constipation. Maalox 30 cc PO QID prn indigestion. Lopressor 5 mg IV q 5 minutes x 3 doses (unless the systolic blood pressure drops below 100), and then start on 50 mg, one tablet by mouth every 12 hours. Lisinopril 10 mg, one tablet by mouth every day (unless contraindicated). Magnesium oxide 400 mg, one tablet by mouth every 12 hours for low magnesium level and to prevent heart rhythm problems. 12. Other Meds: 13. Respiratory therapy: 14. Consultants: 15. Labs: 16. H&P: Oxygen at 2 liters per minute by nasal cannula (maintain SpO2 level > 92%) for 12 hours after the last episode of chest pain. Recheck a SpO2 level after removal of the O2 to ensure the SpO2 is > 90%. If it is < than 90%, then reapply oxygen to maintain a SpO2 level > 90% and daily try to retitrate the oxygen requirements of the patient on room air. Total CK, monoclonal CK-MB, troponin I on admission (if not done in ER) and 8 hr later X 2 for total of 3 times. Call if abnormal. CBC and magnesium level if not done in ER. Chem 8 and LFTs, if not done in ER. Lipid profile fasting in am. CXR (portable) if not done in ER. EKG on admission (if not done in ER) and with each cardiac enzyme panel. Please type up the H&P. ________________________________________________ Signature