Process Paper
advertisement

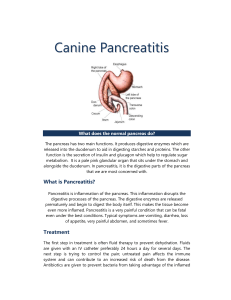
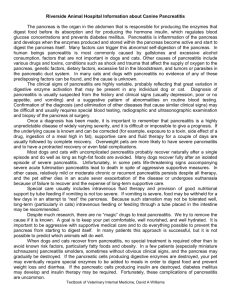
Running head: PROCESS PAPER 1 Process Paper Emily A. Dehnke NURS 30030 Nursing of Adults Professor Aller 1 November 2010 Running head: PROCESS PAPER 2 Process Paper Client Profile D.L. is a seventy-three year old white male who came into the hospital on October 3rd, 2010 with a chief complaint of epigastric and right lower quadrant pain. He has a history of Crohn’s disease with three bowel resections, hypertension, hypercholesterolemia, cholelithiasis, and a previous history of pancreatitis. He came into the hospital because while he was eating at his son’s house in Bolivar, he became dizzy, nauseous with dry heaves, and cold sweats. Then he felt severe epigastric pain radiating to the right lower quadrant. His family brought him to the hospital. His admission and primary medical diagnosis is pancreatitis. Pancreatitis, which is inflammation of the pancreas, can be acute or chronic; in this case, it is acute. Acute pancreatitis is common but can be lethal due to edema, gastric juices in the pancreas digesting the pancreas, fat necrosis, and sometimes hemorrhage (Black & Hawks, 2005). Pancreatitis in the United States is most commonly caused by alcohol use but can also be caused by gallstones, drugs, and metabolic disorders (Black & Hawks, 2005). The pancreas is a large gland behind the stomach; it secretes enzymes, or digestive juices, into the small intestine through the pancreatic duct where the enzymes join with bile, a liquid made by the liver and stored in the gallbladder, to digest food (Black and Hawks, 2005). The pancreas also releases insulin and glucagon into the bloodstream, which help regulate blood glucose (Black & Hawks, 2005). In a normal functioning pancreas, the digestive enzymes secreted by the pancreas don’t become activated until they reach the small intestine, but when the pancreas is inflamed (pancreatitis), the enzymes inside it attack and damage the tissues that produce them (Black & Hawks, 2005). How or why the enzymes become Running head: PROCESS PAPER 3 activated in the pancreas is unknown but it could be related to bile reflux or pancreatic duct obstruction (Black & Hawks, 2005). The most common sign of pancreatitis is pain and it usually starts in the middle epigastric region and hurts the most a couple hours later; most of the time, the pain radiates to the back, chest, flanks, and lower abdomen (Black & Hawks, 2005). People with gallstoneassociated pancreatitis usually experience pain after a large meal, which could have been what happened to D.L. this most recent hospital admission; his abdomen started hurting after eating lunch (Black & Hawks, 20005). Nausea and vomiting often occur with the pain because it activates the vomiting center along with gastric and intestinal hypo-motility (Black & Hawks, 2005). People with severe pancreatitis may exhibit circulatory problems such as hypotension, pallor, cool and clammy skin, hypovolemia, hypo-perfusion, and shock; hemorrhage is also a risk in pancreatitis which is manifested by Turner’s syndrome, which is bluish coloring of the left flank, and Cullen’s sign, which is bluish coloring of the periumbilical area (Black & Hawks, 2005). In July 2009, D.L. had his first case of pancreatitis. He came into the hospital with the same kind of epigastric and right lower quadrant pain he felt during his most recent hospital visit. He was in the hospital for five days on an NPO diet except for sips with medications and ice chips. He eventually started feeling better so they put him on a low fat diet and then sent home; the low fat diet is a health promotion intervention meant to reduce gallstone formation; a person eating a low fat diet will also be eating a diet lower in cholesterol (Black and Hawks, 2005). During this hospital stay, the doctors discovered that D.L. had cholelithiasis, or gallstones, which is not surprising because patients with Crohn’s Disease have an increased risk of cholelithiasis. Gallstones are crystal-like structures formed by hardening or accumulation of normal or abnormal bile components (Black & Hawks, 2005). There are three Running head: PROCESS PAPER 4 types of gallstones: cholesterol, pigment, and mixed; there are four explanations for gallstones: bile that changes what it is made up of, gallbladder stasis that leads to bile stasis, infection, and demographics and genetics (Black and Hawks, 2005). D.L. probably got gallstones as a result of the first explanation dealing with bile that changes what it is made up of; for example, cholesterol gallstones show that the bile is supersaturated with cholesterol and lacking bile salts (Black & Hawks, 2005). D.L. is most at risk for this cause of gallstones because the chance that bile becomes cholesterol-saturated increases with age and D.L. also has hypercholesterolemia, which just means he has high cholesterol levels (Black & Hawks, 2005). It is interesting to note that hypercholesterolemia is associated with a family history of heart disease and diabetes; D.L.’s mother died of coronary artery disease and his father died of diabetes complications (Black and Hawks, 2005). In November 2009, D.L. came into the hospital again with the same epigastric pain from his earlier incidence of pancreatitis. The doctors decided that the cholelithiasis was aggravating the pancreas and causing pancreatitis. Because of this, they wanted to perform a cholecystectomy, or surgical removal of the gallbladder, but they waited until December 2009 to do it. The laparoscopic cholecystectomy was done in December 2009 by Dr. Ramad. D.L. had not had any signs or symptoms of pancreatitis until Oct 3, 2010, when he again had the epigastric and right lower quadrant pain. The doctors diagnosed him again with pancreatitis by using an abdominal and pelvic CT scan. As of Oct 5, 2010, the doctors were performing more tests on D.L. such as an MRCT without contrast in order to determine the cause of the pancreatitis. Running head: PROCESS PAPER 5 The results for the MRCT were not determined before we left the floor on Oct 5, 2010, so I am not sure the cause of D.L.’s last pancreatitis episode. D.L. has a history of Crohn’s disease. He was diagnosed when he was twenty-eight years old and has had three bowel resections before 1980 because of it. Crohn’s disease is one of the chronic inflammatory disorders that characterizes inflammatory bowel disease (IBD); the other is ulcerative colitis (Baumgart, 2009). These diseases are chronic and recurrent and people are usually diagnosed between the ages of fifteen to thirty years of age; there is no cure and treatment is symptomatic (Black & Hawks, 2005). Crohn’s disease affects all layers of the submucosa, meaning it is transmural, and can affect any part of the gastrointestinal tract from the mouth to the anus, but it usually affects the intestines (Baumgart, 2009). It isn’t known why people get Crohn’s disease and the only proven risk factor is genetic; there are no preventative measures (Black & Hawks, 2005). Crohn’s disease is chronic inflammation in the bowel resulting from immune system malfunction; the bowel lumen narrows because of all the inflammation (Black & Hawks, 2005). Lesions can develop in the bowel and the tissue becomes edematous, heavy, and reddish-purple (Black & Hawks, 2005). Glanular spots, enlarged lymph nodes, and Peyer’s patches are all common in the intestines from Crohn’s as well as small superficial ulcers with granulomas and fissures, which are cracks or tears (Black & Hawks, 2005). The fissures can become abscesses and fistulas, which can release toxic substances and fluids from the intestine into the blood, abdomen, or other areas of the body (Black & Hawks, 2005). Bowel resections are often times needed in order to get rid of the damages intestine. Malabsorption, kidney stones, stomatitis, and peripheral arthritis are all problems related to Crohn’s (Black & Hawks, 2005). Common symptoms of Running head: PROCESS PAPER 6 Crohn’s disease are diarrhea, abdominal pain, fever, and blood or mucus in stool (Baumgart, 2009). Patients may have nutritional deficiencies, anorexia, weigh loss, anemia, debility, fatigue, dehydration, and metabolic imbalances (Black & Hawks, 2005). A person with Crohn’s often cannot wait a long time to use the restroom; when they feel the urge to defecate, they must find a restroom quickly. Gordon’s Functional Assessment Include client’s admission date: 10/3/2010 Occupation: Retired in 1995: was in Navy Construction Batalian. Worked at Allegheny Ludlum for 35 yrs. Diet: NPO except for ice chips and sips of water for medication Religion: Catholic Activity: Up as tolerated (no fall risk) Allergies: Magnesium, Mercaptopurine, Azathioprine, Cladribine, Fludarbine Current Medications: SCH: Carvedilol (Coreg), Cholecalciferol (Vit D), Enoxaparin (Lovenox), Ferrous sulfate, Multivitamin (Centrum), Normal Saline, PRN: Amlodipine Besylate (Norvasc), Hydromorphone HCl (Dilaudid), Ondansetron HCl (Zofran), Promethazine HCl (Phenergan) Treatments: NPO diet Past Surgeries: three bowel resections (before 1980), Nephrectomy (2006), Cholesystectomy (2009) diagnostic tests: results under the appropriate health pattern. Client Profile (summarize events leading to the day you cared for client): See previous section of paper titled “Client Profile” AREA OF HEALTH SUBJECTIVE DATA OBJECTIVE DATA INDIRECT DATA *Identify source of indirect data HEALTH/PERCEPTION D.L. said he is very happy D.L. functioned D.L. has many chronic INTERPRETATION (effective patterns or barriers/potential barriers) D.L. does have some Running head: PROCESS PAPER HEALTH MANAGEMENT General Survey, perceived health & well-being, self-management strategies, utilization of preventative health behaviors and/or services. NUTRITIONAL/ METABOLIC Patterns of food and fluid consumption, Weight, skin turgor. (Skin, Hair, Nails; Head & Neck; Mouth, Nose, Sinus; swallowing, Ht., Wt) 7 with life and is very blessed with his family. D.L. said that although he has had Crohn’s disease since he was 28, he thinks it is managed as best as it can be. D.L. said he has regular check-ups. D.L. claims not to smoke or drink. He said he is happy with his health but he just wants them to figure out what is causing his pancreatitis. independently. He was very pleasant to talk to and very knowledgeable of all his medical conditions. D.L. appears wellgroomed. Rated pain from an 8 to 2 throughout the day. V/S: 98.6 F, HR 88, BP 133/76, Resp 16, 93% Rm Air medical conditions such as hypertension, Crohn’s disease, hypercholesterolemia, etc. He has had recurrent episodes of pancreatitis. (chart) D.L. said that he is hungry because he has not eaten since coming into the hospital, but he also said he understands why he cannot eat anything. He also complained of dry mouth and being thirsty. He said he has Crohn’s disease but it is controlled well with Remicaid. D.L. did not eat anything during my shift because he is NPO except for ice chips and sips of water with medication. D.L. did not appear dehydrated despite being NPO. D.L. did eat some ice chips periodically throughout my shift. His had elastic skin turgor, He was able to swallow his pills easily. D.L. has been on an NPO diet since 10/3/2010 and has not eaten anything since that day at lunch. D.L. was on NS @ 75mL/hr to keep him hydrated. D.L. is 5’11” and 160 pounds. He is able to feed himself and order his own meals once he is allowed to eat . D.L. is also taking a multivitamin. D.L. has Crohn’s disease. Ca level is 7.9, which is low. Glucose is 157, which is a little high. D.L. is taking Cholecalciferol, ferrous sulfate, & multivitamin (chart) chronic and recurrent medical problems, but he seems very pleased with his health and is a very pleasant and kind man. The main concern right now is his pain management. D.L.’s NPO diet could contribute to dehydration and malnutrition, but being NPO is essential to performing tests and procedures that need to be done to determine what is causing the pancreatitis. NS is helping the patient keep hydrated and the multivitamin is helping to minimize malnutrition, especially since the patient has Crohn’s disease which can effect reabsorption of important vitamins and minerals. D.L.’s Ca and Running head: PROCESS PAPER ELIMINATION Patterns of excretory function & Elimination of waste; relevant labs, D.L. stated that he has had Crohn’s disease since he was 28 years old. D.L. was able to walk to the bathroom by himself. His abdomen was firm and nontender. Hypoactive BS x4. (I should have asked more questions about when he used the restroom such as: did he you just void or have a bowel movement? What did the bowel movement look like? How often do you usually have a bowel movement? D.L. was not on a strict I/O count. D.L. has Crohn’s disease and has had three bowel resections. Cholecalciferol, ferrous sulfate, multivitamin, dilaudid, & zofran could all cause constipation (chart) D.L. is independent in his elimation patterns. He can walk to the bathroom and is not incontinent. His bowel movements should be monitored to ensure his Crohn’s disease is being managed as best as possible. He should also be monitored for constipation due to his meds. D.L. said he functions independently when at home. He said he gets around fine. He also said he does not exercise, but he visits his kids and grandchildren throughout the week, which is his exercise. D.L. said that he was not moving around as much as normal due to his epigastric pain. D.L. was able to move about the room by himself without any assistance. He did not grimace or act like he was in intolerable pain while moving around. He is in very good shape for his age. He functions independently. His hand grasps were strong and equal. MAE. ROM WNL. V/S: 98.6 F, HR 88, D.L. was not a fall risk. His activity status is up as tolerated. He has walked to the bathroom to go to the restroom during his hospital stay (he hasn’t used a bedpan or bedside commode). His ADL’s are all performed by himself. He has given his own baths in the hospital. D.L. has no record of dyspnea on exertion. (chart) D.L. functions independently. He is able to move around, but keeping his pain under control should be a priority for his nurse so that his pain does not limit his movement. Medications, impacting, etc. (Abdominal - bowel and bladder) ACTIVITY/EXERCISE Patterns of exercise & daily living, self-care activities include major body systems involved. (Thoracic & Lung; Cardiac; Peripheral vascular; Musculoskeletal, vital signs) 8 Running head: PROCESS PAPER 9 BP 133/76, Resp 16, 93% Rm Air SEXUALITY/ REPRODUCTION Satisfaction with present level of Interaction with sexual partners (Breast; Testes; AbdominalGenitourinary-reproductive) SLEEP/REST Patterns of sleep, rest, relaxation, fatigue (Appearance, behavior) COGNITIVE/ PERCEPTUAL Patterns of thinking & ways of Perceiving environment, orientation Mentation, neuron status, glasses, Hearing aids, etc. D.L. stated that his first wife died of cancer. D.L. said he has three children with his first wife. D.L. said he married his second wife and that she “was a nice lady.” D.L. said that he loved his first wife very much. We did not discuss sexual relations or functioning. D.L.’s present wife was at the hospital with him for the whole day and waited in the room for him while he was getting a test done. D.L. seemed to be happy with his marriage. D.L.’s first wife died from cancer. He is remarried (chart) D.L. and I did not discuss sexuality so no conclusions can be drawn regarding this matter. However, D.L. did seem very happy with his present marriage and seemed to appreciate his wife being with him at the hospital. D.L. said that he has not gotten much sleep in the last couple of nights at the hospital because of his pain. He did say that at home he usually sleeps fine (I should have asked about how many hours he slept a night at home.) D.L. seemed very tired during my shift. When we were waiting downstairs in one of the testing areas, he was trying to take a nap while we were just waiting. (No information was obtained from indirect sources regarding sleep/rest.) D.L. told me things about the past such as storied about his kids or first wife. D.L. also recalled my name. He stated who he was, what day it was, and D.L. does not wear hearing aids or glasses. A&O x3 during my shift. D.L. could answer questions easily and D.L. has been A&O x3 during his entire hospital stay. (chart) D.L. seemed very tired due to lack of sleep from pain. It should be essential for the nurses taking care of him to manage his pain so that he is able to get more sleep. D.L. should be encouraged to take naps throughout the day even though taking naps may not be a normal event while D.L. is at home. D.L. has no problems with cognition. He Running head: PROCESS PAPER ROLE/RELATIONSHIP Patterns of engagement with others, Ability to form & maintain meaningful Relationships, assumed roles; Family communication, response, Visitation, occupation, community involvement SELF-PERCEPTION/ SELFCONCEPT Patterns of viewing & valuing Self; body image & psychological state 10 where he was easily. follow directions. Long-term & shortterm memory were intact. D.L. said he worked at a stainless steel factory in Lousiville for 35 years. He said this was his second marriage. He said he had three children with his first wife who died of cancer. He said he is remarried. He said he and his wife visit the kids and grandchildren every week. The whole family meets every Sunday for lunch after church. He said he has a boat and he and his wife like to go out on it. D.L. and his wife seemed to have a very good relationship and interacted appropriately with one another. She stayed with him throughout my whole shift. D.L.’s son came to visit him. D.L. seemed to think the world of his family because he talked about them a lot and how lucky he was to have them all live so close in proximity and have such great relationships. D.L. worked at J &L for 35 years. He retired in 1995. He was in the Navy. Married twice. Has three children. Children and wife reported as visiting D.L. often while he is in the hospital (chart) D.L. seems to have a very good support system in his family. He seems to have many diverse and meaningful relationships in his life. D.L. said despite his Crohn’s and current hospitalization, he was very happy with his health. He said his Crohn’s is wellmanaged. I observed D.L. being very pleasant and overall happy despite the pain he was in. (No information was obtained from indirect sources relating to selfperception or selfconcept) D.L. was an overall happy man who was happy with his current situation in life. He was happy with his health management. Running head: PROCESS PAPER COPING/STRESS TOLERANCE Stress tolerance, behaviors, patterns of coping with stressful events & level of effectiveness, depression, anxiety. VALUE/BELIEF Patterns of belief, values, Perception of meaning of life that guide choices or decision; includes but is not limited to religious beliefs 11 D.L. said he was doing good, but he just wishes he could get some more sleep. D.L. was dealing with being in the hospital well. He seemed happy overall. However, he did seem very tired. (I could have asked him bluntly how he was doing with being in the hospital and some ways that he copes with stress.) His wife being with him seemed to relax him. He also seemed happy to see his son when he visited during my shift. D.L. showed no signs of depression or anxiety. D.L. has no past history of depression or anxiety. His behavior since being in the hospital has been appropriate (chart) D.L. is coping with this hospitalization very well. The main concern is lack of sleep which is making the patient tired. It would be beneficial to keep allowing the family to visit. D.L. said that he attends church every Sunday. He also said he thanks God He has blessed him with such a great, supportive, and loving family. He said he wanted to participate in communion when it came around. D.L. made subtle remarks indicating a faith of some kind. He referenced God and church a couple times. He and his wife took communion together when the priest came around. Religion is listed as Catholic. D.L. is on the communion list (chart). D.L. has faith in God and is dedicated to his Catholic faith AEB communion, attending church, etc. Running head: PROCESS PAPER 12 Lab Information & Interpretation Lab Test Result 1 Normal Range Interpretation 7.9 (L) 9-11 mg/dL INR WBC 1.2 23.7 (H) 1-2 5-10,000/mm3 HGB 12.7 12-16 gm/dL Low value could be due to Ca or vitamin D deficiency as a result of poor reabsorption due to Crohn’s disease WNL High level due to inflammation, stress, & possible infection WNL HCT 37.5 35-47% WNL Ca 9 PLT 115 (L) 150-450 x10 /L RBC 4.31 (L) 4.5-6 million/mm3 MCV 87 80-95 um Low value could be from enoxaparin or bleeding from Crohn’s disease Low value could be due to enoxaparin, Crohn’s disease ( because of decreased absorption of nutrients needed to make RBC), and lack of a kidney (which produces erythropoeitin that helps bone marrow make RBC) WNL 33.9 32-36 g/dL WNL 0 0 WNL 27,740 0-160units/L AST 27 0-35 units/L Extremely high level due to acute and reoccurring pancreatitis and Crohn’s disease, which is and instestinal disease WNL ALT 46 4-36 IU/L High level could be due to pancreatitis, MCHC Troponin Lipase Running head: PROCESS PAPER 13 enoxaparin, & Ondansetron HCl Alkaline 70 30-120 u/L WNL Na K Cl 137 4.7 103 136-146 mEq/L 3.5-5 mEq/L 98-107 mEq/L WNL WNL WNL CO2 25 23-31 mEq/L WNL Glucose 157 70-110 mg/dL CREAT 1.6 0.6-1.2 mg/dL BUN 23 8-23 mg/dL High level could be result of taking Coreg, eating a big lunch before coming into the hospital, or Promethazine HCl High level could be due to impairment of the kidneys due to only having one kidney. Could also be a result WNL Calcification of tail of pancreas. Moderate inflammation & edema in region of head of pancreas. Significant surrounding fluid & soft tissue mostly in RUQ. R kidney absent. no bowel obstruction. gallbladder absent. liver and spleen normal. Findings not known (because left floor before results came back) Should yield no calcification, inflammation, or edema. Both kidneys and gallbladder should be present. Findings compatible with acute pancreatitis Liver, spleen, and pancreas should appear normal with no enlargement or edema. N/A CT scan of Abdomen and pelvis MRCT w/o contrast Running head: PROCESS PAPER 14 Medication Information & Interpretation Scheduled Medications Drug Name (generic/trade name) Carvedilol (Coreg) Cholecalciferol (Vitamin D) Enoxaparin (Lovenox) Drug classification/action Why Person Taking Patient Dose (Normal Range) -antihypertensive -beta blocker -blocks beta adrenergic receptor sites -decreases HR & BP, improves CO -treat hypertension -25 mg PO 2x/day with meals (6.25 mg 2x/d, may be increased q7-14 days up to 25 mg 2x/d) -fat-soluble vitamin -requires activation in liver & kidneys to create active form of Vit D3. -treat & prevent Vit D deficiency -needed for Ca absorption from kidney -anticoagulant -antithrombotic -prevent/treat DVT or heart attack -treat Vit D deficiency -helps promote Ca & P normal levels b/c D.L. has chronic kidney disease due to lack of one kidney -1000 U BID PO (400-1000 U/day) (HIGH dose probably due to not just treating Vit D deficiency, but also improving Ca & P normal levels) -prevent thrombus formation since D.L. is not moving around as much as -30 mg SQ QD (30 mg once daily) S/E -dizziness, fatigue, weakness, diarrhea, erectile dysfunction, hyperglycemia Nursing Implications -give with food or meals -Take apical pulse before administering: hold for pulse <60 -may cause increased BUN, K, blood glucose, etc. -monitor I/O & daily weight -monitor BP & HR -dizziness, N, V, -monitor serum Ca, anorexia, P, & alkaline constipation, phosphatase levels bone/muscle pain, periodically fatigue -monitor for vit deficiency: Rickets -monitor for vitamin toxicity: hypervitaminsosis D -bleeding, pain or -monitor for bleeding irritation at site, & hemorrhage anemia, -monitor CBC, PLT thrombocytopenia, count, and occult Running head: PROCESS PAPER 15 -prevents thrombus formation Ferrous Sulfate Multivitamin (Centrum) Na Cl 0.9% (Normal Saline) he usually would (this dose is especially for patient with decreased renal function due to lack of one kidney) -antianemic -prevent/treat Fe -iron supplement deficiency due to -prevent/treat Fe increased risk for deficiency malabsorption as a result of Crohn’s disease -multivitamin -treat/prevent -treat/prevent vitamin vitamin deficiency deficiency due to Crohn’s disease -replace Na & Cl lost -maintain patency -maintain patency of IV of IV -hydrate -hydrate N, V -325 mg PO once -hypotension, N, daily with meals constipation, dark (325 mg once daily) stools, diarrhea, epigastric pain -1 tablet PO QD (1 tablet QD) -IV 75 mL/hr (1.53L/24 hrs) -constipation, diarrhea, upset stomach, black stoole -fever, hypertension blood periodically (may cause decrease in PLT) -may cause increase in AST & ALT -alternate injection sites daily -monitor bowel function for constipation -monitor nutritional status -give on empty stomach -may give with food if GI upset occurs -use cautiously in kidney dysfunction -monitor I/O, electrolytes, & pH balance PRN Medications Drug Name (generic/trade name) Amlodipine Drug Action/ Purpose -antihypertensive Why Person Taking Normal Dose Range -treat hypertension -10 mg PO QD (5- S/E -headache, light- Nursing Implications -assess BP: hold for Running head: PROCESS PAPER 16 Besylate (Norvasc) -Ca channel blocker -causes vasodilation resulting in decreased BP 10 mg once daily) headedness, dizziness, fatigue, peripheral edema, fainting, hypotension, flushing, reflex tachycardia, change in liver/kidney function -confusion, sedation, constipation, hypotension, urinary retention, tachycardia Hydromorphon e HCl (Dilaudid) -opioid analgesic -antitussive -decrease moderate to sever pain -suppress cough -decrease pain from pancreatitis -2 mg IV push q3h prn (1.5 mg q3-4h prn, dose may be increased as needed) Ondansetron HCl (Zofran) -antiemetic - serotonin (5-HT3) antagonist -decrease nausea and vomiting -treat nausea & vomiting associated with pain and pancreatitis -4 mg IV q6h prn (4 mg q6-8 h) -headache, diarrhea, dizziness, fatigue, constipation Promethazine HCl (Phenergan) -antiemetic -antihistamine -sedative/hypnotic -treat N & V associated with pain and -12.5 mg IV q6h (12.5-25 mg q4h prn) -confusion, disorientation, sedation SBP <120 -monitor I/O & daily weight -may be given with another hypertensive drug -serum liver enzymes should be checked periodically -monitor BP, P, & Resp before and during therapy: resp <10, decrease dose by 25-50% -watch CO2 levels -antecdote: narcan -when IV, dilute with 5 mL of sterile H2O or NS -give 2 mg or less over 205 minutes -may cause increase in bilirubin, AST, & ALT levels -monitor for N, V, abdominal distension, & BS -infuse over 20 minutes -monitor BP, HR, & Running head: PROCESS PAPER -phenothiazine -relieve histamine excess, decrease N&V, and sedate 17 pancreatitis Resp -assess patient’s level of sedation -assess for N&V before & after -may cause increased glucose Nursing Care Plan I chose “acute pain” as my primary diagnosis because of the fact that D.L. was in so much severe, constant pain. I chose “impaired comfort” as my second diagnosis because of the fact that D.L. was having to endure so many uncomfortable things at one time such as pain, nausea, and hunger. I first chose “risk for impaired nutrition: less than body requirements” as my second diagnosis, but I could not think of ways to ensure he had adequate nutrition since they did not want him to have anything in his stomach so that they would be able to perform any tests or procedures on him as quickly as they could. Nursing Diagnosis 1: Acute Pain r/t epigastric and right lower quadrant pain AEB… -severe epigastric and RLQ pain -pancreatitis -pain levels ranging from 2-8 -Dilaudid ordered for pain prn Outcomes: Two Patient-centered goals 1. Client will report a pain level verbally acceptable to him by the Nursing Diagnosis 2: Impaired comfort r/t pain and inability to eat AEB… -NPO except for ice chips & sips of water for medication -has not eaten since 10/3/2010 -hypo-active BSx4 -severe pain in epigastric area -pain levels ranging from 2-8 -patient c/o being tired because of lack of sleep due to pain Outcomes: Two Patient-centered goals 1. Client wi2. Client will report decreased pain and increased Running head: PROCESS PAPER end of my shift. 2. Client will consistently report a pain level of <4/10 during hospital stay. Interventions w/Rationale 1. Assess pain level q3h and pain characteristics -identifies patient specific need of pain relief -accurate pain assessment is necessary to implement proper & efficient pain management techniques 2. Administer pain medication (Dilaudid) as scheduled/prn -pain medication given when needed and on time decreases the chance of the pain becoming severe (severe pain often take more medication and a longer time for the medication to take affect) 3. Encourage alternative pain relief measures such as repositioning, splinting abdomen with a pillow, deep breathing exercises, not sitting or standing constantly, etc. -increases patient’s sense of control -relaxation decreases muscle tension, which would decrease pain 4. Ensure quiet, comfortable, and relaxing environment by turning down lights, minimizing noise, closing the door, making sure wife is in the room, etc. -decreases anxiety and increases mood of patient EBP Citation: Black, J., & Hawks, J.H. (2005). Medical surgical nursing: clinical management for positive outcomes. (7th Ed) St. Louis, MO: Elsevier Saunders. 18 restfulness before my shift is over. Interventions w/Rationale 1. Administer pain medication (Dilaudid) as scheduled/prn -managing the client’s pain will help them to be comforted 2. Manage the client’s nausea by administering the scheduled/prn medications (Phenergan, Zofran) -Nausea is very uncomfortable and managing the nausea will help the patient to feel relieved and relaxed 3. Develop a therapeutic relationship with the patient, especially regarding pain and comfort. (Ex: encourage patient to express pain, teach self-management, provide support & understanding of pain) -a nurse who actively gets the patient involved with their own planning, interventions, and assessment of comfort and pain levels enhances the patient’s potential to be comforted 4. Explain that the reason the patient is not allowed to eat anything is so that the doctors can perform necessary tests such as an MRCP, CT scan, etc. in order to try and determine what is causing the pancreatitis so that they can better treat the problem. -a patient who understands the reasoning behind doctor’s orders they are not happy with makes it easier for them to accept and comply with the orders. It is especially important to reiterate that although the orders may not be pleasant, the overall reasoning is to help the patient. EBP Citation: Carpenito-Moyet, L.J. (2006). Nursing diagnosis: application to clinical practice. (11th Ed.) Philadelphia, PA: Lippincott. Craven, R., & Hirnle, C.J. (2007). Fundamentals of nursing: Running head: PROCESS PAPER Carpenito-Moyet, L.J. (2006). Nursing diagnosis: application to clinical practice. (11th Ed.) Philadelphia, PA: Lippincott. Craven, R., & Hirnle, C.J. (2007). Fundamentals of nursing: human health and function. (6th Ed.) Philadelphia, PA: Lippincott. Evaluation: Goal 1: Goal met. Pain level was assessed to be an 8/10. Dilaudid was administered. Patient encouraged to lie down to rest and relax. Tried to make environment as comfortable as possible: closed door to minimize noise and distraction, made sure wife was in the room, & turned down lights. Reassessed pain after 45 minutes and pain was down to a 4/10, which the patient stated was much better than before. Goal 2: Goal not met. I did not see the patient through to his discharge from the hospital, so this goal is not able to be evaluated. 19 human health and function. (6th Ed.) Philadelphia, PA: Lippincott. Evaluation: Goal 1 & 2: Goals met. Phenergan and Dilaudid were administered in order to control pain and nausea. The patient verbalized his understanding of why he wasn’t allowed to eat anything. I was able to spend a lot of time talking to him using therapeutic techniques and was able to understand his frustration and also just get to know him better. By the end of my shift, his pain level went down to a 4/10 and he was able to take a nap. Running head: PROCESS PAPER 20 Reference Baumgart, D.C. (2009). The diagnosis and treatment of Crohn’s disease and ulcerative colitis. Deutsches Arzteblatt International, 106(8), 123-33. Retrieved from Ebsco Host. Black, J., & Hawks, J.H. (2005). Medical surgical nursing: clinical management for positive outcomes. (7th Ed) St. Louis, MO: Elsevier Saunders. Carpenito-Moyet, L.J. (2006). Nursing diagnosis: application to clinical practice. (11th Ed.) Philadelphia, PA: Lippincott. Craven, R., & Hirnle, C.J. (2007). Fundamentals of nursing: human health and function. (6th Ed.) Philadelphia, PA: Lippincott. Deglin, J.H., & Vallerand, A.H. (2007). Davis’s drug guide for nurses. (11th Ed.) Philadelphia, PA: FA Davis Company.