Revenue Costs

Agenda Item 4.4.3
Appendix 1
1. DESCRIPTION
Title
Partners involved
Wrexham CAMHS Service Delivery Plan
Author Angela Roberts & Patrick Howells
Date of submission March 07
Brief description of the proposal
Outline of the developments required in order to deliver CAMH services which meet national targets (SaFF 07/08) National Service Framework
Targets for Children and Young People (CAMHS). The strategic direction is identified by the statutory organisations in Wrexham and is in line with the
Wrexham Emotional Health and Wellbeing Strategy and Implementation
Plan and includes a proposal to develop Autism Spectrum Disorder as described in the CAMHS Strategy and Action Plan.
North East Wales Trust
Wrexham Local Health Board
2. NEED
Define the Need
Strategic Context
Identify the service need(s).
Determine the expected demand (activity) including expected future demand.
SaFF Target 8
In accordance with policy ‘ Everybody’s Business’ and the NSF for
Children, Young People and Maternity Services:
(i) The CAMHS Commissioning Networks will commission Specialist
CAMHS so that: a) Primary Mental Health Workers offer consultation and advice to professionals in Tier 1 within 2 weeks. [Target date: 31 st March
2008]
(ii) Commissioners of Tier 4 services will ensure that children and young people who are referred for admission are assessed and admitted according to the following criteria: a) young people who are thought by staff from a Specialist CAMHS to require admission to a psychiatric unit for adolescents on account of their clinical needs are assessed within 2 weeks. If admission is considered necessary by that assessment, it occurs within 3 weeks.
[Target date: 31 st March 2008] b) young people who are thought by staff from a Specialist CAMHS to require immediate admission to a psychiatric unit for adolescents on account of their clinical needs are assessed within 24 hours. If immediate admission is considered necessary by that assessment, it occurs within 24 hours of the assessment. If non-immediate admission is agreed, it occurs within 3 weeks. [Target date: 31 st
March 2008]
2008/09
Angela Roberts / Patrick Howells 1
Local Context
Agenda Item 4.4.3
Appendix 1
- Waiting times from referral to treatment for routine cases of 4 months
National Service Framework for Children and Young People
(CAMHS) 2005.
Everybody’s Business (All Wales CAMHS Strategy) 2001.
Royal College of Psychiatrist guide (Building Sustaining CAMHS
Claire Lamb et al)
NICE Guidelines as they apply to the practice of CAMHS Teams.
Wrexham CAMHS Strategy (Thinking of our Future 2006)
Recent and forthcoming CAMHS inspection (HIW & Wales Audit
Office) and the office of the Childrens Commissioner.
Whilst the targets for urgent and emergency responses have a major impact on the Tier 4 services commissioned by Health Commission Wales on a
Regional basis, the processes involved require assessment by the Tier 3 service which is also the route through which referrals are directed to the
Tier 4 service. In particular the emergency cases that require immediate admission will need Tier 3 CAMHS involvement to be immediately available.
These waiting time targets along with others describing what CAMH
Services should deliver are mirrored in the National Service Framework.
In addition to the targets there are a number of areas highlighted on the
Trust corporate risk register regarding delivery of CAMHS. These include the limited provision currently available for urgent risk assessments for self-harm and the issues regarding difficulty accessing immediate therapy for some of the most urgent cases. Any delivery plan will need to incorporate the means for reducing the risks highlighted.
Finally, there has been a long standing recognised service deficit for children and young people with Autism Spectrum Disorders (ASD). These young people often present with a range of complex problems and frequently fall between existing service criteria. Whilst the current limited provision exists to provide a small number of ASD assessments there is a need to expand on this in order to meet the much greater level of demand and to provide appropriate health intervention. The lack of services within this area has been a long standing source of complaints and questions from patients, carers, Community Health Council, AM’s and MP’s. Whilst there is a considerable body of professional knowledge and skills locally within the area of ASD there is insufficient capacity to fully utilise this.
The current specialist CAMHS service has insufficient resources to meet these new targets and other drivers outlined above. In addition to new resources some fundamental changes to the way the service is configured and how it functions is required. In particular there are 4 challenges facing the service from these targets:
1. How to deliver a meaningful assessment / intervention within a short time frame
2. How to provide advice and consultation within 2 weeks of request
3. How to provide an immediate response to “emergency” referrals
Angela Roberts / Patrick Howells 2
Agenda Item 4.4.3
Appendix 1
4. How to dedicate sufficient resources to deliver a meaningful assessment and appropriate health intervention for ASD
5.
This proposal will ensure that;
Waiting times are reduced as a minimum to those identified in SaFF
07/08.
The strategic priority determined at Executive level across the LA,
LHB and Trust.
The priorities identified and agreed at Children and Young People’s
Framework Partnership Board following NSF SAAT on February 28 th
07.
The priority identified in Wrexham Health, Social Care and Wellbeing
Strategy.
The North East Wales Trust have agreed that service development in the area of CAMHS is required if we are to meet our obligation to Children and
Young People with Mental Health issues.
The proposals are supported by a wide consultation on the Wrexham
CAMHS multi-agency strategy.
The reconfiguration of service delivery and the described “new ways of working” are congruent with NICE guidelines and meet identified risk areas for both Wrexham LHB and North East Wales Trust.
Service improvements are articulated under the area of proposals.
All service changes have been discussed in partnership with CAMHS
Practitioners, Clinical Psychologists and the Joint Services
Development Manager Children’s Services.
The plan has a clear interface with multi-agency developments as described in the CAMHS Strategy document.
In terms of meeting the needs of local children and young people extensive consultation around local strategy has highlighted the need to deliver these service improvements.
Angela Roberts / Patrick Howells 3
Agenda Item 4.4.3
Appendix 1
Existing
Arrangements
3. OUTLINE PROPOSAL
Currently the CAMH service is configured so that all therapists and practitioners undertake all roles and tasks which they are trained to do.
Whilst theoretically this provides a generic multi skilled workforce in practice it is not at wholesale mental health model. Some therapists currently spend time on assessment thereby interfering with their capacity for delivering specific and targeted therapies. Reconfiguration will enable therapy time to be freed up and more appropriately targeted and divided across the team.
In addition there is a mismatch between current capacity and demand and this in benchmarked against the All Wales Guidelines which indicate that one whole time equivalent (WTE) Mental Health
Practitioner should have a capacity of 40 active cases (usually new referrals) per year.
Current demand is increasing by 9% per year resulting in increasingly lengthy waiting lists. (nationally and replicated locally)
Non recurrent Local Development Plan funding in 2006 has ensured that waiting list targets can be met and maintained only until March
2007.
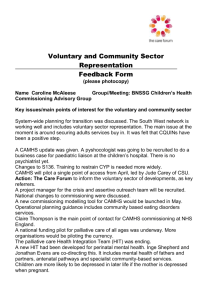
The team overall can assess and treat 380 referrals per year.
The figures below indicate the rise in referrals current and anticipated for
2006/07/08.
(A)
Active & new referrals 06
07
08
Capacity 06/07
9.5 WTE’s
380
478
520
Box A demonstrates how current capacity in the team will maintain the status quo and make a small indentation in the waiting list until March 07 and then waiting lists will increase by 9% throughout the rest of 07 and 08.
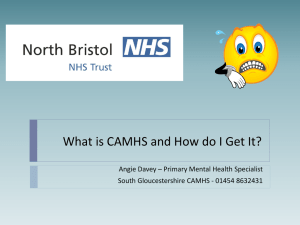
(B)
Waiting list / referrals and Capacity
Predicted waiting list without new resources
Year
2007
2008
Angela Roberts / Patrick Howells 4
Agenda Item 4.4.3
Appendix 1
2009
Current and predicted waiting list
50
58
84
Current Team Capacity
32 refs / month
32 / month
32 / month
Actual / Anticipated
(+ 9%) Referrals
38 refs / month
40 refs / month
43 refs / month
Situation at 31 st March
58 over 6 months = 0
84 over 6 months = 48
205 over 6 months = 147
Box B demonstrates the current and predicted waiting list based upon local and national epidemiological figures.
Proposal
Proposed New Service - Wrexham Only
Integrated within Tier 2/3 who have specific assessment skills.
Increased capacity in CAMHS team to address SaFF waiting list targets
Tier 2/3 Team
Creation of “Duty System approach” to ensure SaFF target for consultation, advice, training and joint working is enabled.
Historical issues regarding the delivery of an equitable service across
Wrexham and Flintshire will be resolved during the reconfiguration process in respect of the 16-18 years age group (those who are not defined as in full time education).
Creation of an Autism Spectrum Disorder Service.
Angela Roberts / Patrick Howells 5
Agenda Item 4.4.3
Appendix 1
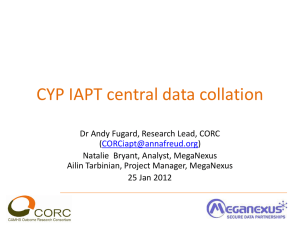
Therapy
Medical
PMHW
Component
Function
7.1 WTE
2.2 WTE
0.8 WTE Nurse Prescriber (ADHD)
Currently
3.3 WTE
Consultant vacancy of existing provision
0.05 WTE Psychiatrist funded
CAMHS Costings re Business Proposal 2007
Including staff costing changes as Agenda for Change
Month
Total in Month
Total to date
CAMH Staff / Admin + training
+ travel
+ stationary
July each but
WTE is total
Angela Roberts / Patrick Howells 6
£15,000
£15,000
1 Band 6
2 Band 5
A&C staff (1 Band 2 and 1 Band 3) & stationary etc
August
£30,298
£45,298
3 Band 6 remaining Band 5
September
£34,600
£79,898
0.5 Band 7 Clinical Psychologist
0.5 Band 7 SALT
October
£32,131
£112,029
All staff in post therefore costs stable at pay and equally divided non-pay
November
£32,131
£144,160
December
£32,131
£176,291
January
£32,131
£208,422
February
£32,131
£240,553
March
£32,131
Angela Roberts / Patrick Howells 7
Agenda Item 4.4.3
Appendix 1
Agenda Item 4.4.3
Appendix 1
£272,684
Total = £272,684
The need to make some fundamental changes to the service structure and how it operates is central to the Trust being able to meet the targets being set. Under the current service structure and in the way it operates the provision of an immediate response to an emergency referral would be very difficult to ensure. The delivery of the 4 month wait from referral to treatment would be impossible.
The initial step towards reconfiguration in order to meet the targets is to introduce a separate, internal pathway into accessing specific therapies which do not increase the waiting time. This would require the division of staff time into dedicated, specific therapy time and assessment / therapeutic intervention. Some staff would be 100% therapist others
100% assessment / intervention whilst many would have dedicated sessions within each area dependent on stills and training.
The assessment / intervention group would then become the receiving component for specialist CAMHS carrying out initial and detailed mental health assessment, commencing
CPA and deliver components of the care plan as required. This would result in the reduction of the waiting time from referral to treatment as currently a significant wait can occur between assessment and access to therapy. Whilst there is likely to still be a delay between assessment and access to some specific therapies, intervention would be commenced immediately after assessment and allow a 6 and even 4 month target to be met (with required resource allocation). The added effect of having dedicated and protected therapy time may also help improve access to many specific therapies and reduce delays in some cases.
The other deve lopment would be to introduce a “duty” system into the assessment / intervention part of the CAMHS team. Two things would be achieved by the provision of this system the first would be access to advice and consultation either via telephone or directly with a duty clinician at the earliest duty slot available. In practice staff on “duty” would perform the function of Primary Mental Health Worker available to provide information and advice by telephone or in person by arrangement. The second function the system would meet would be to take emergency calls to which the duty clinicians could respond.
The “duty” system would be an add on function of the increased provision for deliberate self-harm risk rota and in effect would become the urgent or emergency response part of the service. This would still be provided by various members of the CAMHS assessment / intervention staff on a rota basis. The introduction of this would not address issues of out of hours cover which needs to be taken forward with Tier 4 services on a N Wales basis but would significantly reduce the risk of failing to meet the target and would also succeed in removing the risk from the Corporate risk register.
To provide a meaningful level of service for ASD staff with relevant skills and experience
Angela Roberts / Patrick Howells 8
Agenda Item 4.4.3
Appendix 1 will need to be given dedicated time and responsibilities for particular areas of that ASD delivery. Some staff have specific skills and have been trained in assessment of ASD.
Some have intervention skills and experience with younger children and carers, others in developing communication and behavioural programmes for children and young people with ASD. Whilst other staff have skills and experience working with some of the associated mental health issues which may arise. Through recruiting staff to fill the capacity to meet the day to day work these staff with specific skills undertake a significant element of a dedicated ASD provision could be set up. By recruiting to a couple of specific posts in support of the existing staff identified a meaningful provision could be developed.
The following methodology is prescribed
Reconfiguration and appropriate increase of the existing team will enable more practitioners to assess and therapists to undertake specific and targeted brief therapy interventions.
Additional capacity is required to ensure that assessments are undertaken in a timely manner and in order that a care programme approach is fully embedded in the service.
This additional resource combined with the new ways of working will both increase activity to meet current demand as well as ensuring that future demand as per Box(A) is addressed.
The duty practitioner role will ensure that all Tier 1 of CAMHS service have access and joint working for consultation and advice. This will be addressed in two ways;
1. First duty practitioner will have pre-booked consultation and advice appointments.
2. Second duty practitioner will deal with all ad hoc consultation and advice requirements.
Both duty practitioners will undertake to risk assess all individuals admitted through
Accident and Emergency Unit on a daily basis (NSF requirement) and all other emergency referrals.
Consultation
Benefits
Need
Need has been evidenced locally by the noted increased demand for the service. In order to minimise the potential for severe disruption to the service very rigid referral criteria have been applied resulting in a lack of access and many complaints from Tier 1 practitioners.
Full consultation on the CAMHS strategy has identified the need to reconfigure, redesign and increase capacity within the service.
Running parallel to these proposals are a number of multi-agency initiatives which will meet the expectations of those consulted during this process, these include:
User groups
Statutory bodies
Voluntary organisations
Practitioners
General public
Service users, including current children and young people accessing services, have been involved throughout the process.
A “mental health model” service.
Follows NICE guidelines
Utilises a child centred Care Programme Approach.
Angela Roberts / Patrick Howells 9
Impact
Support
Agenda Item 4.4.3
Appendix 1
Reduces waiting list time
Improves service user outcome
Through PMHW (Duty Practitioner) role supports Tier 1.
Over long term produces early prevention benefits
Links with multi-agency developments and initiatives for early prevention and intervention.
Giv es “value for money”.
Assures targets (SaFF / NSF) are met.
1) Patient Care
Accessible service for user groups.
Improved approach to case management.
Targets appropriate interventions – improved outcome.
2) Other services
Improved access to consultation, advice and joint working.
Improved partnership working with other service providers (i.e. Team
around the Child, Flying Start and Sure Start teams).
3) Clinical Governance
Best practice adopted
NICE guidelines followed
Ability to benchmark against UK
Improved audit capability
Therapists and practitioners skills utilised appropriately.
4) Risk Management
Duty practitioner system ensures that risk is managed in responsive fashion.
Use of Care Programme approach ensures that risk is considered at all stages of assessment and intervention.
5) Health and Safety
CAMHS work is highly stressful and the increased capacity will eliminate some areas of pressure.
6) Workforce Implications
Provides a career structure through potential for moving through A4C
Band and utilises knowledge and skills framework effectively.
Ensure appropriate supervision and training in place
Requires a further 3 x Band 6 WTE (Capacity increase)
2 x Band 5 WTE (Developmental increase)
This proposal has been developed collaboratively by the Trust
Providers and LHBs as commissioners. The proposals have been discussed with the specialist Tier 2 and 3 teams and the Consultant
Psychiatrist (CAMHS).
Partners have been engaged in the CAMHS Steering group.
Framework Partnership has identified CAMHS as a priority following
NSF SAAT and from the strategic cross agency steer agreed by Chief
Executives.
Angela Roberts / Patrick Howells 10
Evaluation
Agenda Item 4.4.3
Appendix 1
Following the elected members workshop there is an agreement to work collaboratively across agencies.
There is a proposal from the Local Authority to support the use of school funding in the delivery of cohesive PMHW school attached services.
The Autism consultation paper is likely to ensure collaborative working around assessment and interventions for children and young people with autism spectrum disorder. The funding for enhanced educational provision will be directed to Local Authorities.
Discussions to link the current provision in the Local Authority with proposed provision for Autism Spectrum Disorder assessment in
CAMH are progressing.
Discussions to link the current provision in Local Authority with proposed provision for ASD assessment in CAMH are underway.
Current demand is set to outstrip our ability to provide within the SaFF targets from March 07.
Reconfiguration plus increased capacity within the service will ensure that the expected increase in demand can be met. (Refer to Box B)
Improved health outcomes will be generated as the teams will be configured to ensure that children and young people are not kept on the waiting list for assessment.
Following assessment a care co-ordinator will be allocated and therapeutic intervention commenced according to the care programme plans.
Early intervention through Primary Mental Health workers working closely with Tier 1 will ensure that early identification of developing mental health issues are addressed and treated.
Clinical Risk Reduction
Combined with other developments (Lottery funded Youth Worker in
Hospital Team) and early diagnosis of ADHD and ASD these developments will substantially reduce the clinical risks for Children and Young People.
Environmental Risk Reduction
Advice and consultation offered to Tier 1 practitioners should result in less family and school disruption.
Organisational Risk Reduction
Currently there is a considerable risk to the reputation of the Local
Health Board and Trust in North East Wales.
This has been highlighted locally through CAMHS consultation process, by practitioners and other agencies, by the Office of the
Childrens Commissioner and recently by the proposed review of
CAMH services by Health Inspectorate Wales and the Wales Audit office.
More effective use of resources
The Care Programme Approach and reconfiguration of teams and whole service will ensure a streamlined approach to care. The addition of practitioners who are able to best use their skills will speed up the assessment and reduce waiting lists enabling efficiency gains
Angela Roberts / Patrick Howells 11
Agenda Item 4.4.3
Appendix 1 and result in financial savings in the long term.
4. OPTION APPRAISAL
** This section must be completed where there is more than one solution available
Angela Roberts / Patrick Howells 12
Generate Options
Selection Criteria and Evaluation of
Options
Options Cost
Angela Roberts / Patrick Howells
Agenda Item 4.4.3
Appendix 1
Option 1: Status Quo – do nothing option
As previously described this is not an acceptable option and we risk severe criticism and the probability of external intervention.
Option 2: The sticking plaster approach
The use of non-recurring funding to reduce waiting times will cease to be effective from March 07. This approach has led to fragmented services and cannot guarantee clinical outcomes. Staff demotivation has been noted as an issue as has staff retention.
Option 3:
Introduce the Care Programme Approach and reconfigure without increased human resource separating the development of the
PMHW team from that of the increased capacity to provide Autism service. This will result in further fragmentation, demotivation and the medium of long term will be more costly both in human and financial terms.
Option 4: As described in the business proposal. This is the preferred approach.
The project team is the CAMHS Steering group and ensuring multiagency involvement and approval and willingness to pool budgets has been observed in the recent months. The options have been discussed through the CAMHS Steering group.
It was determined that the constraints identified in sections 2 and 3, in particular those linked to;
Achieving SaFF targets
NSF Standards and forthcoming audit and inspection negate the opportunity to explore alternatives. The proposals are very much aligned to the “have too” nature of CAMHS delivery in today’s climate.
N/A
13
Agenda Item 4.4.3
Appendix 1
5. COST
Provide details of the total recurring and non-recurring cost including all relevant revenue costs, capital costs and transitional costs.
All costs must include VAT where appropriate.
Angela Roberts / Patrick Howells 14
Revenue Costs
Agenda Item 4.4.3
Appendix 1
Costs for Delivering SaFF Targets only
Staff WTE 3 @ Band 6
= £93,012
Staff WTE 2 @ Band 5
= £49,606
Staff WTE 0.5 @ Band 3
= £8,399.50
Staff WTE 1 @ Band 2
= £15,107
Sub total
= £ 166,124.50
+ on costs
= £ 31,500
Sub total
= £ 197,654.50
Travel and Subsistence
= £ 10,000
Stationary
= £ 1,000
Training
= £ 3,000
= £243,154.50
With ASD included ( this is no longer an option re waiting list for ASD
TOTAL assessment and WAG directives)
Staff WTE 0.5 SALT @ Band 7
= £18,208
Staff WTE 0.5 Clinical Psychologist @ Band 7
= £18,208
Staff WTE 1 @ Band 6
= £31,004
Staff WTE 1 @ Band 5
= £24,803
A&C @ Band 3
Angela Roberts / Patrick Howells 15
Agenda Item 4.4.3
Appendix 1
= £16,799
= £ 109,022
= £ 27,250
= £ 136,272
Sub total
+ on costs
Sub total
Travel and Subsistence
= £ 1650
= £ 375
= £ 4125
Capital Costs
= £142,422
Combined Total = £385,576.50
Transitional Costs
Expenditure Profile Expenditure Profile including 3% uplift Year 2 + 3
Cost for delivering SaFF targets re Waiting Lists.
Cost
Year 1
Year 2
Year 3
Revenue
£ 141,840.12
£250,449.13
£257,962.60
Capital
N/A
N/A
N/A
Transitional
N/A
Angela Roberts / Patrick Howells 16
Stationary
Training
TOTAL
N/A
N/A
Total
£141,840.12
£250,449.13
£257,962.60
Cost for delivering SaFF target (waiting list plus ASD service)
Cost
Year 1
Year 2
Year 3
Revenue
£385,576.50
£397,143.79
£409,058.10
Capital
N/A
N/A
N/A
Transitional
Agenda Item 4.4.3
Appendix 1
N/A
N/A
N/A
Total
£224,919.62
£397,143.79
£409,058.10
Please refer to changes in figures on page 7 re Agenda for Change
Angela Roberts / Patrick Howells 17
Affordability
Sustainability
Implementation
Risks
Name
Angela Roberts
Patrick Howells
Agenda Item 4.4.3
Appendix 1
6. FEASIBILTY
Reconfiguration, redesign and combining the two proposed services increases the affordability.
This proposal provides long term sustainability as it deals with immediate waiting list concerns, develops the service and builds capacity in Tier 1 in line with Saff targets local agreements and Everybody’s Business” 2002.
Full implementation will take between four and six months.
7. IMPLICATIONS OF DOING NOTHING
As previously described in evaluation of proposal section. Risks are failure to meet SaFF target 8. Risk to reputation.
Organisation
Wrexham LHB
Wrexham NEWT
8. APPROVAL
Date:
15/03/07
15/03/07
Signature
Angela Roberts / Patrick Howells 18