FLATULENCE - DRUG THERAPY RESPONSE: The volume
advertisement

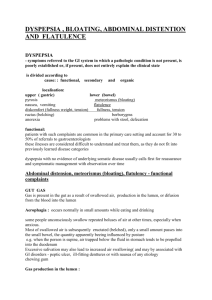
FLATULENCE - DRUG THERAPY RESPONSE: The volume, composition, and frequency of flatulence are determined by age, stress, antibiotics, diet, and other factors. Depending on age, heredity, gastrointestinal fermentation, and the degree of aerophagia, the composition of flatus will vary. Nitrogen, hydrogen, carbon dioxide, methane, and oxygen are the major components of flatus (in decreasing increments). The production of methane has not been detected in children younger than 2 years. Only 30% of individuals older than 2 years host methane-producing bacteria, such as Methobacterium remenatium. The basis of heredity for methane production is suggested by the prevalence of methane production among siblings. Diet also appears to play a role in the etiology of excessive flatulence. Nondigestable dipolysaccharides (cellulose, raffinose, and stachyose) become substrates for bacterial fermentation and increase the passage of hydrogen. Chewing gum and eating, along with stress and poor fitting dentures, can contribute to flatulence by increasing the nitrogen content. Various treatments have tried to alleviate the frequency and volume of flatulence including antibiotics, simethicone, charcoal, anticholinergies, and diet modification (Van Ness & Cattau, 1985). Generally, antibiotics have no role in therapy of flatulence, unless the patient exhibits bacterial overgrowth. Iodochlorhydroxyquin 1.5 grams/day reduced the production of flatus from 83 mL/hr to 11 mL/hr in 5 patients eating a bean diet that provided 37% of their required calories (Steggerda, 1960). Iodochlorhydroxyquin 0.5 gram three times daily reduced the release of intestinal hydrogen when added to a bean diet, as compared to the hydrogen elimination usually observed following a bean diet (Murphy & Calloway, 1972). The authors proposed the iodochlorhydroxyquin may have inhibited hydrogenproducing bacteria. SIMETHICONE is non-toxic, nonabsorbable, and works by its defoaming action by reducing surface tension and coalescing air bubbles. Simethicone doses of 40 to 80 milligrams four times daily have been shown by a number of studies to be effective in the treatment of gas (Weiss, 1974; Bernstein & Schwartz, 1974; Danhof & Stavola, 1974). Good to excellent results were reported in 152 of 200 patients treated with simethicone 40 milligrams four times daily for bloating and excessive flatus (Rider & Moeller, 1960) in a prospective, nonrandomized, uncontrolled study. Three studies have utilized a combination of PANCREATIC DIGESTIVE ENZYMES with simethicone in alleviating flatulence (Brewer, 1973; Silber, 1973, Auld, 1979). These studies reported good results with this therapy. However, no comparative control with a single agent was used and it is difficult to assess the validity of the results from these studies, since simethicone alone has been shown to be highly effective. A search of medical literature did not identify any further studies that utilized pancreatic enzymes to alleviate flatulence (RMDCC, 1988). Activated charcoal has also been utilized to reduce the number of episodes of flatus. Yatzidis (1972) administered activated charcoal 20 to 50 grams/day orally for 4 to 20 months to dialysis patients to treat gastrointestinal disturbances, without any adverse effects. Hall et al (1981) demonstrated a reduced number of episodes of flatus in 13 patients following the administration of activated charcoal with a bean meal. Anticholinergics have been promoted as effective agents to alleviate cramps and bloating associated with excessive flatulence. Snape et al (1979) observed a decrease in intracolonic pressure, colonic contractions, and cramps following the administration of clindinium 5 milligrams 90 minutes prior to a fatty meal; however, the effect of clindinium on flatus production was not investigated. It appears that diet modification will have the greatest impact on affecting flatus production. Intestinal flatus production was significantly reduced during fasting in normal subjects and in individuals with bacterial overgrowth involving the small intestine (Levitt, 1969). Avoiding the ingestion of beans (which contain cellulose, stachyose, and raffinose) can significantly reduce intestinal flatus production. Enteric bacteria are capable of fermenting up to 57% of ingested cellulose. A diet that contained 2.4 grams/day of crude fiber produced flatus at a rate of 26.7 mL/hr compared to a diet that contained 9.4 grams/day of crude fiber producing 49.4 mL/hr (Davies, 1971). Patients with lactase deficiency may produce a greater amount of flatus compared to normal individuals since lactose will become a substrate for fermentation. Lactose that is deposited into the large intestine, but not the small intestine, correlates with an increase in the elimination of hydrogen via the lungs and rectum (Levitt, 1969). The ingestion of yogurt, which contains up to 14 units of lactase, produced 33% less breath hydrogen production compared to an equal quantity of milk in lactase-deficient subjects (Kolars et al, 1984). Chlorophyllin 100 milligrams three times daily for 7 to 10 days, then 100 milligrams twice daily for a total duration of 6 months, was administered to 30 geriatric patients with excessive flatus. The authors estimated a 50% success rate with the administration of chlorophyllin for alleviated flatus. However, the evaluation of chlorophyllin was based on the daily opinions of the observers (Young & Beregi, 1980). CONCLUSION: Many modalities have been promoted to alleivate flatulence; however, data supporting their efficacy are limited. Minimizing stress and avoiding the ingestion of foods that appear to be flatulogenic for that individual may be helpful in reducing the production of flatus. Simethicone has been demonstrated to be effective in reducing flatulence. Activated charcoal may also be helpful; however, further studies are required to evaluate the efficacy of this agent. REFERENCES: 1. Auld JM: Use of a simethicone/enzyme agent in relief of gastrointestinal gas. Curr Ther Res 1979; 26:55-61. 2. Bernstein JE & Schwartz SR: An evaluation of the effectiveness of simethicone in acute upper gastrointestinal distress. Curr Ther Res 1974; 16:617. 3. Brewer RA: A study of gastrointestinal gas in the aged. Clin Med 1973; 80:18. 4. Danhof IE & Stavola JJ: Accelerated transit of intestinal gas with simethicone. Obstet Gynecol 1974; 44:148. 5. Davies PJ: Influence of diet on flatus volume in human subjects. Gut 1971; 12:713-716. 6. Hall RG Jr, Thompson H & Strother A: Effects of orally administered activated charcoal on intestinal gas. Am J Gastroenterol 1981; 75:192-196. 7. Kolars JC, Levitt MD, Aouji M et al: Yogurt - an autodigestable source of lactose. N Engl J Med 1984; 310:1-3. 8. Levitt MD: Production and excretion of hydrogen gas in man. N Engl J Med 1969; 281:122-127. 9. Murphy EL & Calloway DH: The effect of antibiotic drugs on the volume and composition of intestinal gas from beans. Am J Dig Dis 1972; 17:639-642. 10. Rider JA & Moeller HC: Use of silicone in the treatment of intestinal gas and bloating. JAMA 1960; 174:2052-2054. 11. Silber W: Pankreoflat in benign diseases of the oesophagus. a blind therapeutic trial. S Afr Med J 1973; 47:1137. 12. Snape WJ, Wright SH, Battle WM et al: The gastrocolic response: evidence for neural mechanism (Abstract). Gastroenterol 1979; 77:255. 13. Steggerda FR: Gastrointestinal gas following food consumption. Ann NY Acad Sci 1960; 150:57. 14. Van Ness MM & Cattau EL Jr: Flatulence: pathophysiology and treatment. Am Fam Physician 1985; 31:198-208. 15. Weiss J: Etiology and management of intestinal gas. Curr Ther Res 1974; 16:909. 16. Yatzidis H: Activated charcoal rediscovered. Br Med J 1972; 4:51. 17. Young RW & Beregi JS Jr: Use of chlorophyllin in the care of geriatric patients. J Am Geriatr Soc 1980; 28:46-47.