serum adenosine deaminase activity in dogs: its importance in
advertisement

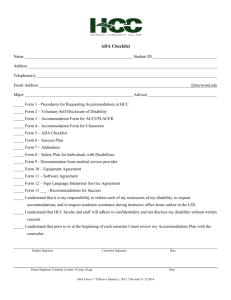
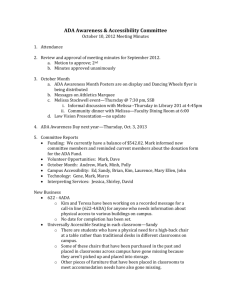
ISRAEL JOURNAL OF VETERINARY MEDICINE Vol. 55(4) 2000 SERUM ADENOSINE DEAMINASE ACTIVITY IN DOGS: ITS IMPORTANCE IN EXPERIMENTAL LIVER INTOXICATION N. Altug and Z.T. Agaoglu Department of Internal Diseases, Faculty of Veterinary Medicine, University of Yuzuncu Yil, 65080 Van, Turkey Abstract In the present study, ADA levels were investigated together with clinical, biochemical, hematological and histopathological findings in dogs experimentally intoxicated with carbon tetra chloride (CCl4) to determine its role in liver intoxications. Twenty healthy cross-breed dogs were divided in two groups of ten as acute and chronic intoxication groups. CCl4 was prepared in olive oil (1:1). Dogs in the acute group received 1.5 ml/kg CCl4 once only. Dogs in the chronic group received 0.5 ml/kg CCl 4 twice a week for 12 was adminisreted by orogastric probe after 12 hours of hunger. Clinical, haematological and biochemical analysis were made in all dogs 2 days before the experiment and on days 1, 3, 5, 7 and 9 in the acute group and four times at 21 day intervals in the chronic group. Liver biopsies were taken on days 4 and 9 from the acute group and at weeks 6 and 12 from chronic group. weeks. CCl4 During the experiment signs of inappetance, stillness, watery feces and mild dehydration in the acute group, and inappetance, weakness, light colour of feces, dark orange colour of urine and depression in the chronic group were observed. Erythrocyte and haemoglobin levels increased significantly (p<0.05) on the third day in the acute group, whereas, total leukocyte counts increased significantly (p<0.001) in the chronic group. Significantly important increases (p<0.001) were also observed in biochemical parameters (serum AST, ALT, ALP and ADA) in both groups of dogs. On histopathology, precise hepatocellular hydropic degeneration, necrosis in the centrilobular and midzonal regions and dissociation in remarc cordons were observed in the acute group. Fibrosis was observed in the portal regions and around the vena centralis in the chronic group. It is concluded that determination of ADA activity can be useful in the assesment of liver degeneration caused by toxic hepatopathy in dogs and ADA activity can be added to other routine biochemical tests employed in diagnosis of liver intoxication. Key Words: Dog, Liver toxication, CCL4, Symptoms, ADA. Introduction Adenosine deaminase (ADA) catalyses hydrolytic deamination of either adenosine or deoxyadenosine to produce inosine and deoxyinosine respectively (1). Several ADA isozymes exist, with different molecular weights, kinetic properties and tissue distribution (2). In human (1) and animals (3) ADA consist of three isoenzymes: ADA I, ADAI+ complex protein (CP) and ADA 2. ADA 2 is the main component of serum ADA activity (2), while the others (ADA I and ADA I+CP) are major components of tissues (2, 3). ADA has been found in high levels in the spleen, lungs and lymph nodes, and in low levels in the myocardium, muscles, kidneys, bladder and liver (4). It has been detected in the cell cytoplasm and nucleus (5). ADA activity has been reported to be high in lymphoid tissues and its inadequacy reported to cause immune deficiency (1, 6). On the other hand, ADA activity increases during hepatitis, tuberculosis, salmonellosis, brucellosis, toxoplasmosis, visceral leishmaniasis, rickettsiosis, infectious mononucleosis, pneumonia, rheumatoid arthritis and leukemia in humans (1, 6), enzootic muscular dystrophy in lambs (7), feline infectious peritonitis (8), hepatopathy in dogs (8) and various hepatic diseases and leukosis in cattle (9). Although ADA activity reportedly increases in acute and chronic hepatitis, hepatic fibrosis, liver cirrhosis and hepatoma (10), its importance in veterinary medicine, its state in acute and chronic liver diseases and its relationship between other routinely used biochemical tests have not been investigated. In the present study, ADA activities were investigated with clinical, biochemical, hematological and histopathological findings in dogs experimentally intoxicated with CCL4 to determine its role in liver intoxication. Materials and Methods In this study, 20 healthy cross-bred dogs aged between 1 and 6 years and weighing 15 to 28 kg were divided into two groups of ten as acute and chronic intoxication groups. CCL4 ( Merck) were prepared in olive oil (1:1) and given to the dogs by oro-gastric probe after 12 hours of hunger. Dogs in acute group received 1.5 ml/kg CCL4 only once, and the chronic group received 0.5 ml/kg twice a week over 12 week. Before and during the experiment, clinical examinations were made and the findings recorded. Ten ml of blood without anticoagulant and 5 ml blood with anticoagulant (EDTA) were taken from the animals 2 days before experiment and on days 1, 3, 5, 7 and 9 in the acute group and four times over 21 days intervals in the chronic group. Whole blood was used to assess hematological changes. For this purpose. Coulter-Maxim cell counter was used. Blood without anticoagulant was used to prepare serum samples to determine aspartate aminotransferase (AST) (Randox AS-483), alanine aminotransferase (ALT) (Randox AL- 485) and alkaline phosphatase (ALP) (Randox AP-502) levels using commercial kits. ADA activity was determined colorimetrically by a modified Martinek method (11). Liver biopsies with the guide of ultrasonography were taken on days 4 and 9 from the acute group and on weeks 6 and 12 from the chronic group for examining histopathological changes. For statistical analysies. Student's t test was used to determine the effect of CCl4 on several biochemical and histopathological parameters (12). This study was approved by the ethics committee. The dogs used in the experiment were hospitalized after the experiment at the Animal Hospital. They were fed with a controlled diet (low in protein, fat and carbohydrates) containing a balanced vitamin and mineral supplement. Diuretic and sodium restricted diet were given to one dog with submandibular oedema. All the dogs also received antibiotic and glycocorticoids for their antibacterial, antifibrotic properties respectively. The dogs were kept one month in the hospital then were donated to a dog rehabilitation center when they were clinically healthy. Results After CCL4 adminstration, non-specific liver toxicity symptoms such as anorexia, stillness and watery feces were seen in the acute group of dogs. These signs continued for 3 days and disappeared by 9 days post-inoculation. In the chronic group anorexia, weakness, light colour and muddy feces, dark orange urine and depression were observed as the number of doses increase. Furthermore, in 4 dogs low level of icterus, in 2 dogs polydypsia and in one dog with submandibular oedema were observed. On hematological examination, total leukocyte (WBC), thrombocyte and hematocrit values (PCV) were not significantly changed during the experiment compared with the preexperiment values of the acute group. However, statistically significant increases(p<0.05) were observed in erythrocyte (RBC) and hemoglobin (Hb) values only on day 3. Furthermore, RBC, Hb, PCV and thrombocyte values were not significantly different from the preexperinantal values in the chronic group. The WBC values, however, significantly increased during experiment (p<O.OOl). Serum AST, ALT, ALP and ADA levels in the acute group before and after experiment are given in Table 1. These enzymes increased significantly (p<0.001) as seen in Table 1 except for AST on day 9. During the experiment, serum enzyme activities peaked on day 1 for AST, ALT and ADA, on day 3 for ALP. Serum AST, ALT, ALP and ADA activities before and after experiment (weeks 3, 6, 9 and 12) in the chronic group are given in Table 2. All the enzyme levels increased significantly (p<0.001). The experiment was terminated at 12 weeks, when the values were still increasing. Table I : Biochemical levels in the acute intoxication group DAYS AST (U/L) X±Sx ALT (U/L) X±Sx ALP (U/L) X±Sx ADA (U/L) X±Sx 29.86±1.7 32.57±1.4 113.0±4.5 2.34±0.24 1 387.9±19* 425.4±14.0* 180.7±4.0* 5.41±0.32* 3 315.4±13* 321.6±10.6* 455.2±6.9* 5.09±0.09* 5 175.0±5.7* 222.5±7.32* 399.9±11.0* 4.83±0.10* 7 63.14±3.2* 124.4±5.0* 311.4±11.0* 3.40±0.15* 9 32.43±2.0 68.0±1.6* 268.5±6.7* 2.94±0.19* Before experient * p<0.001, n=10 Table 2 : Biochemical levels in the chronic intoxication group Weeks AST (U/L) X±Sx ALT (U/L) X±Sx ALP (U/L) X±Sx ADA (U/L) X±Sx Before experient 37.88±1.0 39.63±1.77 98.87±4.23 2.83±0.20 3 238.37±6.55* 456.5±10.0* 647.4±11.7* 13.02±0.20* 6 298.30±11.8* 490.9±11.4* 791.75±9.55* 17.56±0.33* 9 320.7±10.3* 952.9±11.3* 22.12±0.48* 12 370.8±11.9* 575.3±11.1* 626.3±11.0* 1093.1±10.4* 24.18±0.43* * p<0.001, n=10 Liver biopsies were taken on days 4 and 9 from the acute group and on weeks 6 and 12 from the chronic group. Precise hepatocellular hydropic degeneration, necrosis in centrilobular and midzonal regions, and dissociation in remarc cordons were observed in the acute group (Figure 1). Fibrosis was observed in the portal regions, around the vena centralis and paranchimous tissues in the chronic group (Figure 2). Picture 1. Histopathological appearance of a liver section from the acute intoxication group (HE x 80). Hepatocellular degeneration and necrosis (1) in centrilobular (2) and midzonal (3) regions. Picture 2. Histopathological appearance of a liver section from the chronic toxication group (HE x 80). Fibrotic areas stretching from one hepatic lobule (1) to another (2). Discussion Diagnosis of liver disease is based upon clinical history, clinical signs, biochemical assays, serum protein electrophoresis, radiography, ultrasonography and, eventually, histopathological examination (13). In the present study, clinical signs seen in the acute group were anorexia, stillness, watery defecation and mild dehydration, and for the chronic group anorexia, depression, pain in abdominal palpation (in four dogs), mild icterus (in two dogs), polydypsia (in two dogs) and submandibular oedema in one dog 6 weeks after toxication (in one dog). Similar clinical signs have been reported by other workers (14, 15). Significant increases in RBC and Hb levels could be seen only on the third day in the acute group (p<0.05). In contrast, a significant increase in WBCs could be seen throughout the experiment in the chronic group (p<0.001). These results agree with the findings of others (15, 16), but disagree with the results of another group (17). Other hematological parameters were not significantly changed in either group. Increases in RBC and Hb levels observed in the present study could be due to mild dehydration as a result of watery defecation in the acute group. Ogawa et al. (16) reported an increase in WBC intoxication group and tubuler changes caused by CCl 4 claimed to be the reason for leucocytosis. These workers also reported liver damages after CCl4 intoxication. Therefore, the leucocytosis reported in the present study could well be due to liver damage. Several experimental studies have shown that chronic administration of CCl 4 leads to hepatic cirrhosis as well as renal damage (16). The target site of the renal nephrotoxicity has been postulated as the mitochondria of the renal tubular cells (16). The dark orange colour of urine observed in the chronic toxication group could well be the result of nephrotoxicosis. All enzymes studied increased significantly (p<0.001) in the acute group (Table 1), except the value for AST obtained on day 9. During the experiment, serum enzyme reached peak levels on day I for AST, ALT and ADA,and on day 3 for ALP. These findinds are similar to those reported by others (5, 14, 18, 19) in acute hepatic liver damage. Serum AST, ALT and ALP activities increased up to 12 weeks, when the experiment was terminated (Table 2). These findings agree with other studies on chronic liver damage (15, 17, 20). Serum AST, ALT and ALP were reported to increase in chronic CCl4 toxication (20, 21), and this increase has been suggested to be positively correlate with increased liver damage. The highest increase was also observed at the end of chronic toxication by some workers (20, 21). Similarly, a simultaneous increase in these serum enzymes in the chronic group was also observed in this study. Increase in ADA levels has been reported in animals (8) and patients (22) with liver disease. Determination of ADA isoenzymes was reported to be an important clue in diagnosing liver damage (6, 23). Furthermore, determination of ADA reported to be a usefill tool especially in the differentiation of paranchymal and obstructive liver damage (24, 25). Some have also suggested that determination of serum ADA isoenzyme activities may be a new marker for liver disease (10). Ellis et al. (25) also suggested that determination of ADA activity is especially valuable in late hepatitis, since serum ADA activity does not return to normal as rapidly as that of other liver enzymes, while higher than normal activity is frequent in cirrhosis at times when other enzyme levels are normal. Serum ADA activities in the acute group increased significantly similar to AST, ALT and ALP activities (p<0.001). It reached a peak level on the first day and decreased up to the ninth day post-experiment. Similar to other enzymes, ADA also increased significantly in the chronic group (p<0.001). Similar findings were reported by several workers in serum samples obtained from animals (8, 26), and patients (1, 25) with liver damages. ADA activities has been reported to increase in acute and chronic liver damages caused by CCl4 toxication. In addition to cell damage, detection of ADA activities has been reported to be a useful clue to early diagnosis of liver diseases (5, 27). Increased ADA levlels with liver cell damage were also observed in the present study. Low levels of ADA have also been found in the kidney (4). A possible nephrotoxicity may have been developed in the chronic group in the present study. Histopathology of kidneys was not investigated in the present study, but abnormal urination in the chronic group indicates some kind of nephrotoxicity. Kurata (23) reported an increase in ADA in patients with liver damage. ADA 1 is increased in acute liver damages which arise from damaged tissues (23). Furthermore, increased ADA 2 arise from stimulated T lymphocytes (23). Although determination of ADA isoenzymes are important parameters in diagnosing liver damage, they could not be detected in the present study. Increased ADA paralleled the liver damage demonstrated histopathologically in the acute group. This result is in agreement with those of some workers (10, 23) but disagree with those of Chicuma (9). Furthermore, in the chronic group ADA increased in parallel with the severity of fibrosis and degeneration in the liver determined histopathologically. Similar findings were reported by Kobayashi et al.(10). It is concluded that, determination of ADA can be usefill in the assessment of liver degeneration caused by toxic hepatopathy. The fact that ADA levels remained high suggests a continuous liver intoxication. Furthermore, determination of ADA isoenzymes may be helpful in differentiating acute and chronic liver disease. Thus, determination of ADA activity can be added to the other routine biochemical tests that are used in the diagnosis of liver disease. References 1. Ungerer, J.P.J., Oosthuizen, H.M., Bissbort, S.H. and Vermaak, W.J.H.: Senim adenosine deammase: isoenzymes and diagnostic application. Clin. Chem. 38(7): 13221326, 1992. 2. Ratech, H., Martiniuk, F., Borer, W.Z. and Rappaport, H.: Differential expression of adenosine deaminase isozymes in acute leukemia. Blood. 72 (5): 1627-1632, 1988. 3. Rotandaro, L.: Multiple forms of adenosine deaminase in the thymus of the bovine fetus and calf. Boll. Soc. Ital. Biol. Sper. 57 (23): 2355-2360, 1981. 4. Yasuda, J., Tanabe, T., Hashimoto, A. and Too, K.: Adenosine deaminase (ADA) activity in tissues and sera from normal and leukaemic cattle. Br. Vet. J. 152 (4): 485-488, 1996. 5. Zuck, V.U. und Rotzsch, W.: Die adenosin desaminase (ADA)-biologische und medizinisch-diagnostiesche Bedeutung. Z. Med. Lab. Diagn. 31:231-238, 1990. 6. Gakis, C.: Adenosine deaminase (ADA) isoenzymes ADA I and ADA 2: diagnostic and biological role. Eur. Respir. J. 9:632-633,1996. 7. Rodriguez, J.Z. and Gonzalez, J.G.: Activities of enzymes involved in energy metabolism of Churra breed lambs and changes caused by enzootic muscular dystrophy. Annales de la Facultad de Veterinaria de Leon. 21: 409-419, 1975. 8. Tanabe, T.: Adenosine deaminase activities in the sera and tissues of animals and their clinical significance. Jpn. J. Vet. Res. 41: 1, 1993. 9. Chikuma, S.: Clinicopathological studies of serum adenosine deaminase activity in cattle. Jpn. J. Vet. Res. 45 (2): 125-126,1997. 10.Kobayashi, F., Ikeda, T., Marumo, F. and Sato, C.: Adenosine deaminase isoenzymes in liver disease. Am. J. Gastroenterol. 88 (2): 266-271, 1993. 11. Glick, D.: Enzymatic metfiods used for diagnosis. Methods of biochemical analysis. Vol. XIII, Interscience Publishers, Johnwiyeldsens. 344-345,1965. 12. Hayran, M. and …zdemir, 0.: Computer, Statistic and Medicine, Medikomat Press, Ankara, 1995. 13. Thomas, D., Simpson, J.W. and Hall, E.J.: BSAVA Manual of Canine and Feline Gasroenterology. First Ed. BSAVA. UK. 191-219,1996. 14.Polzin, D.J., Stowe, C.M., O’Leary, T.P. and Hardy, R.M.: Acute hepatic necrosis associated with the administration ofmebendazole to Dogs, JAVMA, 179 (10): 1013-1016, 1981. 15. Chapman, B.L., Hendrick, M.J. and Washabau, RJ.: Granulomatous hepatitis in Dogs: nine cases (1987-1990), JAVMA, 203 (5): 680-684, 1993. 16. Ogawa, M., Mori, T., Mori, Y., Ueda, S., Azemoto, R. et al.: Study on chronic renal injuries induced by Carbon Tetrachloride: Selective inhibition of the Nephrotoxicity by irradiation, Nephron, 60:68-73, 1992. 17. Mwanza, T., Miyamoto, T., Okumura, M., Kadosawa, T. and Fujinaga, T.: Ultrasonography, biochemical and hematological profiles in liver disease caused by lntravenous administration of dimethylnitrosamine in dogs, Jpn. J. Vet. Res., 45 (3):153-161, 1997. 18. Ronneberger, H. and Hein, B. (1984) Effect of antithrombin III on experimental hepatotoxin poisoning in dogs, Arzneimittelforschung, 34 (3): 277-279, 1984. 19. Noonan, N.E.Variations of plasma enzymes in the pony and the dog after carbon tetrachloride administration. Am. J. Vet. Res., 42(4): 674-678, 1981. 20. Dashti, H., Jeppsson, B., Hagerstrand, I., Hultberg, B., Srinivas, U. et al.: Thioacetamide and carbon tetrachloride induced liver cirrhosis, Eur. Surg. Res., 21: 83-91, 1989. 21.Yoshitake, I., Ohishi, E., Sano, J., Mori, T. and Kubo, K.: Effects of KF-14363 on liver fibrosis in rats with chronic liver injury induced by carbon tetrachloride, J. Pharmacobio-Dyn., 14: 679-685, 1991. 22. Nilius, R, Neef., L., Rath, F.W., Gatzsche, M. and Zipprich B.: Adenosine deaminase activity as indicator of inflammation in liver disease, Dtsch. Z. Verdau. Stoffwechselkr, 47 (5): 224-229, 1987. 23. Kurata, N.: Adenosine deaminase, Nippon Rinsho, 53 (5):1178-1183, 1995. <p class="MsoNormal" style="margin-top:2.85pt;text-align:justify;text-indent:" 19.85pt;line-height:150%;mso-pagination:none;mso-la