Discovering Human Sexuality
advertisement

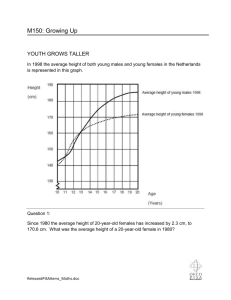
Instructor’s Manual by Amy Wisniewski to accompany Discovering Human Sexuality, Second Edition Chapter 4 Sex and Gender Differences Chapter Overview Males and females differ anatomically, physiologically, and behaviorally. How humans develop as male or female is explained at the beginning of the chapter. Disorders of sex development—or conditions in which chromosomal, gonadal, or genital sex are discordant or ambiguous—are also described. Gender, or the mental and behavioral traits attributed to males or females, is considered from both biological and social/environmental perspectives. Most likely, gender develops as a result of complex interactions between biological and social influences. Finally, transexual people possess the biology of one sex but the gender identity of the opposite sex. Chapter Outline Genes and Hormones Guide Sex Development Female and male reproductive tracts develop from different precursors Female and male external genitalia develop from the same precursors The gonads descend during development Puberty is sexual maturation The brain also differentiates sexually Sex Development May Go Awry Chromosomal anomalies affect growth and fertility The gonads or genitals may be sexually ambiguous Gender Is a Central Aspect of Personhood Gender identity might not match anatomical sex Box 4.1: Personal Points of View: My Life With Androgen Insensitivity Syndrome Women and men differ in a variety of cognitive and personality traits Differences in sexuality include attitudes toward casual sex, jealousy, and frequency of masturbation Many gender differences arise early in life Biological Factors Influence Gender Evolutionary forces act differently on females and males Experiments demonstrate a role for sex hormones Box 4.2: Biology of Sex: “Eggs at Twelve” Life Experiences Influence Gender Gender is molded by socialization Box4.3: Personal Points of View: The Boy Who Was Raised as a Girl Cognitive developmental models emphasize thought processes Gender Development Is Interactive Transgender People Cross Society’s Deepest Divide Transexuals are of more than one kind Box 4.4: Cultural Diversity: Transgenders in Cross-Cultural Perspective Changing sex is a multistage process Box 4.5: Controversies: How Should We Treat Gender-Dysphoric Children? Some transgenders do not want surgery Transgenders and transexuals struggle for awareness and acceptance Chapter Summary 1. Sex is usually determined by the sex chromosomes: The XX pattern causes female development, and the XY pattern causes male development. The key player in male development is the gene SRY on the Y chromosome, which induces the embryo’s genital ridges to become testicles. In the absence of SRY, the genital ridges become ovaries. 2. The male and female internal reproductive tracts develop from different precursors— the Wolffian and Müllerian ducts. In XY embryos, the testicles secrete anti-Müllerian hormone (AMH), which causes the Müllerian ducts to regress, and androgens, which cause the Wolffian ducts to develop further and produce the male internal anatomy. In XY embryos lacking functional androgen receptors (a condition called androgen insensitivity syndrome), neither the male nor the female reproductive tract develops. In XX embryos (normal females), the lack of AMH allows the Müllerian ducts to develop further, and the lack of androgens allows the Wolffian duct to regress, producing the female internal anatomy. 3. The external genitalia of the two sexes develop from common precursors. The urethral folds give rise to the labia minora in females and to the shaft of the penis in males. The genital swellings give rise to the labia majora in females and the scrotum in males. The genital tubercle forms the external portion of the clitoris in females and the glans of the penis in males. Male-typical development of the external genitalia requires the presence of testosterone and its conversion to 5α-dihydrotestosterone (DHT). In female fetuses that are exposed to high levels of androgens (as in congenital adrenal hyperplasia), the external genitalia are partially masculinized. 4. Some sexual differentiation of the brain occurs prenatally— high levels of androgens drive male-typical brain development, and low levels permit female-typical development. At puberty and thereafter, estrogens become important in establishing and maintaining female-typical body structure and function and also influence the brain. 5. Disorders of sex development include chromosomal anomalies such as Klinefelter syndrome (XXY) and Turner syndrome (XO), as well as genetic conditions that affect sex hormone production (e.g., congenital adrenal hyperplasia) or the body’s sensitivity to sex hormones (e.g., androgen insensitivity syndrome). The proper treatment of children with ambiguous genitalia is a subject of controversy. 6. Gender is the entire collection of mental traits that differ between women and men. Gender identity is a person’s core sense of being a woman or a man. Gender role is the social expression of gender identity. 7. Women outperform men in fine movements, verbal fluency, and some aspects of memory. Men outperform women in some cognitive traits, such as visuospatial skills. Personality differences include greater aggressiveness in men. In the area of sexuality, men and women differ in frequency of masturbation (men masturbate more frequently), attitudes toward casual sex (men are more approving), and styles of jealousy (women are more likely to experience emotional jealousy; men are more likely to experience sexual jealousy). All these gender differences show considerable overlap between the sexes, and their significance is debated. 8. Many gender differences arise early in life. Most children distinguish perceptually between males and females by 1 year of age, can identify their own sex by 2 to 3 years, and understand the immutability of sex by 3 to 4 years. Males are more active than females. Boys are more aggressive than girls. Boys and girls prefer different toys, and both prefer to associate with children of their same sex. Sexspecific interaction styles develop within these same-sex groups. Differences in other cognitive traits emerge gradually during childhood. 9. Biological factors influence gender. These include genes that have evolved to help men and women improve their reproductive success. A role for sex hormones, especially during prenatal life, is illustrated by experiments on animals, by observation of humans affected by endrocrinological disorders, and by the study of anatomical markers (such as finger-length ratios) that are correlated with gender traits. 10. Socialization influences gender. This can happen through the innumerable rewards and punishments that children receive from parents and others. Imitation is also an important mediator of gender learning. 11. A variety of cognitive developmental models stress the importance of children’s thought processes in the development of gender. The understanding of gender develops sequentially in young children. Gender schemas are frameworks of beliefs that influence perception and that tend to encourage either/or thinking about gender. In sexual script theory, gender learning involves the social negotiation of roles, such as those to be played by the man and woman in heterosexual relationships. 12. Transgender people are those whose gender identity does not match their biological sex. Transexuals are transgender people who seek to change their anatomical sex: They may transition from male to female (M-to-F) or from female to male (F-to-M). 13. All F-to-M transexuals and some M-to-F transexuals have a childhood history of strong gender nonconformity. They dislike the bodily changes induced by puberty and may attempt to conceal them. They are usually homosexual in the sense that they are sexually attracted to persons of the same birth sex as themselves. They usually do not identify as gay, however, but rather as heterosexual individuals. Some heterosexual M-toF transexuals have a different developmental history, in which the desire to change sex develops out of a wish to incorporate their sexual targets (women) into their own bodies (autogynephilia). 14. Sex reassignment is a multistage process involving living for some period in the identity of the other sex, followed by hormonal treatments and, sometimes, sexreassignment surgery. Genitals can be transformed into those of the other sex, but the procedure is expensive and, particularly in the case of F-to-M reassignment, yields imperfect results. Nevertheless, many transexuals are satisfied with the results of sex reassignment and are able to surmount the social and sexual challenges of post-transition life. 15. Other transgender people do not seek sex reassignment for a variety of reasons. Some believe that sex reassignment would be unnecessary if society could be persuaded to loosen its rigid ideas about gender. All transgender people face discrimination and the risk of violence, and most states and the federal government fail to offer them specific protections. Lecture Notes (Bulleted items are grouped as suggested slides for presentation purposes.) Genes and Hormones Guide Sex Development (Figure 4.1) Testes and ovaries form from the precursor gonads The gene that instructs the ridges to differentiate into testes is called SRY o This gene is located on the Y chromosome Male and Female Reproductive Tracts Develop from Different Precursors (Figure 4.2) Embryos of both sexes possess both Wolffian and Müllerian ducts o Wolffian ducts are precursors of the male reproductive tract o Müllerian ducts are precursors of the female reproductive tract In males, testes produce anti-Müllerian hormone (AMH) to eliminate the female ducts In females, the absence of AMH allows Müllerian ducts to persist and to develop into the oviducts, uterus, and deeper parts of the vagina. Male and Female External Genitalia Develop from the Same Precursors (Figure 4.3) Female and male external genitalia have the same developmental origin. The testicles descend during development (Figure 4.4) Most prenatal sex development occurs during weeks 8 through 24 of gestation, when testosterone levels are high in male fetuses The Brain Also Differentiates Sexually There are differences in brain structure, function, and chemistry between the two sexes o These differences are brought about by higher levels of androgens in males than in females during development Sex Development May Go Awry Chromosomal anomalies that do not fall under typical female (46,XX) or male (46,XY) chromosomal complements affect growth and fertility o Klinefelter syndrome (XXY, XXXY) o Turner syndrome (XO) o XYY syndrome o Triple-X syndrome The gonads or genitals may be sexually ambiguous o Gonadal intersexuality o Androgen Insensitivity Syndrome (AIS) (Box 4.1) o Congenital adrenal hyperplasia (CAH) (Figure 4.6) Gender Is a Central Aspect of Personhood Gender identity is the sense of which sex one belongs to. For some people, gender identity does not match anatomical sex This identity is expressed via gender role behavior Sexual orientation, cognition, and personality traits differ between men and women (Figures 4.7, 4.8A, and 4.8B) Differences in sexuality include attitudes toward casual sex, jealousy, and frequency of masturbation Many gender differences arise at a young age. o By about 3 years of age, most children show evidence of gender constancy (Figure 4.9) o By about 1 year of age, most children can distinguish between men and women o Differences in toy preferences (Figure 4.10) Biological Factors Influence Gender Evolutionary factors influence gender development (Figures 4.11). o Evolutionary factors: ▪ Cognitive differences between the sexes due to long-standing division of labor between men and women ▪ Difference in interest in casual sex between men and women. ▪ Jealousy Experiments Demonstrate a Role for Sex Hormones Girls with CAH have behavioral traits shifted in the masculine direction (Figure 4.12) Prenatal androgens influence gender (Box 4.2 and Box 4.3) The 2D:4D ratio correlates with many gendered characteristics (Figure 4.13) Life Experiences Influence Gender Life experiences influence gender development beginning early in life (Figure 4.14) o Observing socialization (Figure 4.15 A and B) o Rewards and punishments o Imitation (Figure 4.16) Cognitive models focus on thought processes. o Gender schemas (Figure 4.17) o Sexual scripts Transgendered People Cross Society’s Deepest Divide Unhappiness caused by discordance between anatomical sex and gender identity is called gender dysphoria o F-to-M transexuals (trans men) o M-to-F transexuals (trans women) ▪ Transvestism ▪ Autogynephilia o Sex-reassignment is a multistage process (Figure 4.19) o Some transexuals do not desire surgery (Figures 4.20 and 4.21) o Some medical centers treat pre-pubertal children affected by gender dysphoria (Box 4.5) o Transgenders and transexuals struggle for awareness and acceptance (Figure 4.22) Class Discussion Questions 1. People with DSD are sometimes depicted as having both male and female external genitalia. Is this biologically possible? 2. Women and men differ in their performance on some cognitive tasks. Do you think that learning or socialization contributes to these differences? Why or why not? 3. Gender development probably involves complex interactions between biology and socialization. Did both types of influences affect the development of David Reimer (Box 4.3)? Why or why not? 4. Would you consider a F-to-M transexual who is attracted to women heterosexual, homosexual, or neither? Why? 5. If a M-to-F transexual did not wish to have genital surgery, would you question their gender dysphoria? Why or why not? Teaching Suggestions/Resources 1. Eugenides, Jeffrey. (2003). Middlesex: A Novel. New York: Macmillan. 2. Bailey, J.M. (2003). The man who would be queen: The science of gender-bending and transsexualism. Joseph Henry Press. 3. Fine C. (2010). Delusions of gender: How our minds, society, and neurosexism create difference. W.W. Norton & Company, NY.