Supplemental Table 1: Exome Sequencing Consent and
advertisement

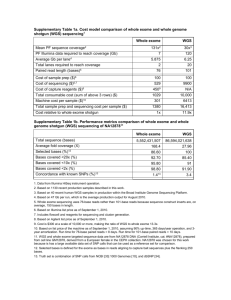
Supplemental Table 1: Exome Sequencing Consent and Secondary Findings Reporting Strategy 1 2 3 4 5 6 7 a Guideline Provide clinicians ordering exome sequencing with detailed consent form to explain complexity of whole exome sequencing, including the possibility for the identification of secondary findings. Categorization of secondary findings: A) Recessive disease carrier status; B) Cancer predisposition; C) Adult-onset disease predisposition (non-cancer); D) Earlyonset diseaseb Provide patients with the option to consent to the receipt of a secondary findings report. Reiterate technical limitations of exome sequencing with specific regard to the incomplete gene coverage to ensure that patients understand that negative secondary findings do not rule out the possibility of a mutation in a gene associated with one of the disease categories. Childrenc not offered secondary findings reports for adult-onset predisposition or recessive disease carrier status (categories A-C) Given that the impact and significance of secondary findings differs widely from that of primary results, report secondary findings separately from the primary exome report. Provide only known, disease-causing mutations in characterized genes. Do not report variants of uncertain significance. Rationale/ Support Supported by American College of Medical Genetics (ACMG) Policy Statementa: "2. Pre-test counseling should be done by a medical geneticist or an affiliated genetic counselor and should include a formal consent process…. 8. Laboratories and clinics utilizing WGS/WES should have clear policies in place related to disclosure of secondary findings. Patients should be informed of those policies and the types of secondary findings that will be reported back to them and under what circumstances." Supported by ACMG Policy Statement: "3. Prior to initiating WGS/WES, participants should be counseled regarding... the likelihood and type of incidental results that could be generated..." Supported by ACMG Policy Statement: "8. ...Patients should be given the option of not receiving certain or secondary findings." Supported by ACMG Policy Statement: "3. Prior to initiating WGS/WES, participants should be counseled regarding the expected outcomes of testing... and what results will or will not be disclosed." Standard guidelines for genetic testing in minors (eg. American Society of Human Geneticsd, American College of Medical Geneticse, AMA Code of Ethics, European Society of Human Geneticsf) . Supported by ACMG Policy Statement: "3. Prior to initiating WGS/WES, participants should be counseled regarding the expected outcomes of testing, the likelihood and type of incidental results that could be generated, and what results will or will not be disclosed." Supported by ACMG Policy Statement: "13. [Patients] should be informed of... the virtual certainty of finding variants of uncertain significance. The threshold for determining which results should be returned to individuals seeking screening should be set significantly higher than that set for diagnostic testing due to the much lower a priori chance of disease in such individuals." American College of Medical Genetics and Genomics (ACMG) Policy Statement "Points to Consider in the Clinical Application of Genomic Sequencing." e-publication: http://www.acmg.net/StaticContent/PPG/Clinical_Application_of_Genomic_Sequencing.pdf b Early-onset disease: A condition in which manifestation of clinical symptoms may occur during childhood c Children = <18 years old d American Society of Human Genetics Board of Directors, American College of Medical Genetics Board of Directors (1995). Points to consider: ethical, legal, and psychosocial implications of genetic testing in children and adolescents. AJHG 57, 1233-1241. e AMA Code of Medical Ethics’ Opinions on Genetic Testing. (2009) American Medical Association Journal of Ethics f European Society of Human Genetics (2009) EJHG 17, 720–721.