ADHD Etiology - Learning Connections Centre
advertisement

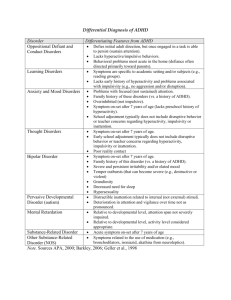
June 2001 Attention Deficit Hyperactivity Disorder – The need for a natural solution Introduction Imagine living in a fast-moving kaleidoscope, where sounds, images, and thoughts are constantly shifting because all your senses are heightened. Your world seems too bright, too loud, too abrasive and too rapidly changing for comfort. You find it difficult to filter out normal background “noise” and find it difficult to concentrate on a task. For many people, this is what it is like to have ADHD. Attention Deficit Hyperactivity Disorder (ADHD) previously known as hyperkinesis is the most common behavioural disorder in children.(1) It is estimated to affect 3 to 5 percent of schoolage children.(1) Frequently the symptoms of ADHD are commingled with learning problems, oppositional conduct, anxiety and depression. Symptoms and Extent of the ADHD problem ADHD is a diagnosis applied to children and adults who consistently display certain characteristic behaviours over a period of time. The most common behaviours fall into three categories: Inattention Hyperactivity Impulsivity ADHD, according to the “Diagnostic and Statistical Manual (DSM-IV), must appear before seven years of age, persist for at least six months and appear in the school environment as well as the home.”(2) Between 30-40% of ADHD subjects have learning disabilities.(3,4) Other neurobiological difficulties associated with ADHD include Tourette’s disorder, anger control problems (oppositional defiant disorder), anxiety and depression.(5,6) Biederman studied a large population of ADHD children and found that more than half had depression, anxiety, and conduct disorder.(6) Current Medical Management – The Ritalin controversy The first report of stimulant use to treat ADHD was in 1937.(7) The action of methylphenidate (Ritalin) is virtually identical to cocaine. It acts on the CNS with a dopamine-agonistic effect that is slower in onset, but mechanistically almost identical to cocaine and amphetamines. (8,9) Scarnati lists more than 100 adverse reactions to methylphenidate. Contraindications as stated in the MIMS include anxiety, tension, agitation, tics, Tourette’s syndrome, hyperthyroidism and arrhythmias.(10) The adverse reactions related to methylphenidate use include: System Central Nervous System Reactions Nervousness, insomnia, anorexia, headaches, drowsiness, dizziness, depressed mood, irritability, dyskinesia, blurring of vision, dependence, tolerance. Gastrointestinal Abdominal pain, nausea, vomiting, dry mouth. Cardiovascular Tachycardia, palpitations, arrhythmias, changes in BP and heart rate (usually an increase). Rash, pruritus, urticaria, fever, arthralgia, alopecia.(10) Dermatological and/or hypersensitivity reactions When methylphenidate is used with antidepressants (such as tricyclics and SSRI’s) seizures, hypertension, hypothermia and convulsions can ensue. As blood levels of the methylphenidate decrease over time, irritability can manifest as a “rebound” type of withdrawal symptom. The frequent practice of maintaining ADHD patients on methylphenidate over many years increases the potential for its abuse. In fact, it is fast becoming a “street drug” in the US. In 1991 US emergency rooms reported less than 25 Ritalin overdoses. By 1995, this number was up to 400 cases for children aged 10-14 years.(11) In 1994, US Government researchers reported that Ritalin caused liver cancer in male mice.(12) The carcinogenic doses were equivalent to just 2½ times higher than the highest human prescribed dose. The National Toxicology Program concluded methylphenidate is a “possible human carcinogen”. This revelation about methylphenidate, plus the major adverse effects, provides the clear conclusion that it is imperative that alternative modalities be implemented for the management of ADHD. ADHD Etiology ADHD is far from homogeneous, with many likely contributory factors. Some of these etiological factors generate symptomatologies that closely resemble ADHD. Among these are food sensitivities and intolerances, sensitivities to food additives, nutrient deficiencies, heavy metal toxicity and toxic pollutant burden. Underactivity of the brain linked to ADHD Initial evidence of the brain being under stimulated in ADHD patients, was first considered with the use of advanced electroencephalograms (EEG or brainwave studies). Lubar demonstrated that when ADHD children performed a concentration task there was an increased amount of slow brain wave activity in their frontal lobes, instead of the usual increase in fast brain wave activity that was seen in the majority of the control group. (13) In 1990 further research supported the notion that most ADHD people at rest, have normal activity in their brain. However, when they perform a concentration task, they experience decreased activity in the prefrontal cortex rather than the expected increased activity that is seen in a normal control group. Research using SPECT imaging (single photon emission computed tomography) which measures cerebral blood flow and metabolic activity patterns, hypothesised and correlated 5 clinical subtypes of ADHD. Sub-Type Imaging of brain ADHD Combined type Decreased activity in the basal ganglia and prefrontal cortex during a concentration task Imaging shows decreased activity in the basal ganglia and dorsal lateral prefrontal cortex during a concentration task Increased activity in the anterior cingulate gyrus and decreased prefrontal cortex activity Inattention and hyperactivity-impulsivity Tyrosine – to increase PEA (phenylethylamine) Inattention, chronic boredom, decreased motivation, internal preoccupation and low energy Tyrosine Cognitive inflexibility, difficulty with transitions, excessive worrying, argumentative behaviour Cingulate hyperactivity appears to be due to relative deficiency of serotonin. Decreased or increased activity in the temporal lobes with decreased prefrontal cortex activity Inattention and/or hyperactivity and mood instability, aggression, mild paranoia, anxiety, atypical headaches or abdominal pain, learning problems Phosphatidyl Serine – to improve memory problems Negativity, depression, sleep problems, low energy, low self esteem, social isolation dl- Phenylalanine, Tyrosine, SAME - help limbic hyperactivity ADHD primarily inattentive subtype Overfocused ADD Temporal lobe ADD Limbic ADD Increased central limbic system activity and decreased prefrontal cortex activity Symptoms Nutrients Gingko biloba Vitamin E – improves memory and muscle movement disorders From further neurobiological studies a consensus is emerging that motor and attentional functions associated with the frontal cortex, are adversely affected in ADHD. These areas of the brain are predominantly dopaminergic, and hypofunction of dopamine pathways is a consistent feature of the disorder.(13,14,15) The Serotonin Connection to ADHD In 1999, researchers at the Howard Hughes Medical Institute discovered that Ritalin and other stimulants exert their paradoxical calming effects by boosting serotonin levels in the brain. Elevating serotonin appears to restore the delicate balance between dopamine and serotonin and reduces hyperactivity.(16) Previously it was thought that the calming action of Ritalin worked through the neurotransmitter dopamine. Specifically, researchers believed that Ritalin and other stimulants interacted with the dopamine transporter protein (DAT). After a nerve impulse moves from one neuron to another, DAT removes residual dopamine from the synaptic cleft, and repackages it for future use. However, Caron’s study found that if DAT was removed then the calming effect of Ritalin still occurred. From these results it was then suspected that dopamine wasn’t the only key to understanding ADHD. The studies suggested that rather than acting directly on dopamine, the stimulants create a calming effect by increasing serotonin levels. The study concluded that the proper balance between dopamine and serotonin was the key, and that hyperactivity may develop when the relationship between dopamine and serotonin is out of balance.(17) Another key amino acid is tyrosine, which assists the body cope physiologically with stress by building the body’s store of adrenaline. Chronic stress increases the need for tyrosine and often results in an extreme reduction of brain tyrosine levels. Tyrosine with vitamin B6, zinc and magnesium helps regulate blood pressure and elevate mood by enhancing the synthesis of noradrenalin in the brain. Food Allergies, Gut Dysfunction and Gastrointestinal Parasites Food sensitivities and food allergies provoke hyperactivity through partially digested food (exorphins) entering the blood stream and scrambling the neuronal communication system. In eight out of nine studies 86% of hyperactive children had elevated eosinophils indicative of allergy or parasitic infection.(18) Data from two double blind studies indicated that 73-76% of ADHD children responded favourably to food elimination diets. Maintenance on low-antigen diets raised the success rate to 82%.(19) One study found significant quantities of bacterial pathogens, yeast organisms and protozoan parasites were in a high proportion of children with ADHD. These findings are quite suggestive that these children suffered from impairment of gut mucosal immunity. (20) Studies have shown that Candida (species) leads to an increase in tartaric acid in urine and bowel samples. Tartaric acid competes or inhibits the activity of malic acid in the Krebs cycle, thus reducing energy production. It was also found that the Candida (species) leads to an increase in arabinose in urine and bowel samples. Arabinose binds with lysine and arginine residue. This forms a penosamide cross-linking between lysine, arabinose and arginine. This cross-linking impairs catalytic sites for lipoic acid, vitamin B6 and biotin as well as initiating an autoimmune response. Crosslinking of proteins results in poor nutrient flow through cell membranes resulting in loss of bowel function. Clostridia (spore formers) cause an increase in dihydroxyphenylpropionic acid (DPPA). DPPA is a false neurotransmitter that reacts with dopamine and noradrenaline receptors. This alters the levels of dopamine and noradrenaline and may give rise to schizophrenia and behavioural problems. Thus, treatment of intestinal parasites, gut dysfunction and food allergies need to be considered in the treatment of ADHD. Nutrient Deficiencies and Imbalances Assessment of ADHD children often reveals nutrient deficiencies or imbalances which, when corrected, result in considerable behavioural and academic improvement. In a series of studies that spanned 18 years, Schoenthaler found that a vitamin-mineral supplement produced significantly less antisocial behaviour than did placebos. Cognitive performance was also significantly improved.(22) Zinc Zinc is of primary importance in ADHD, as it is an important cofactor in metabolism, relevant to neurotransmitters, fatty acids, and prostaglandins and indirectly affects dopamine metabolism.(23) Several studies conducted in different countries have found zinc to be low in ADHD sufferers.(23) Serum zinc can be markedly below normal, and urinary zinc clearance can be lower, both findings are suggestive of poor zinc intake and/or absorption. Zinc deficiency can result in weakened immune system responses and diminished digestive system function. Children who are zinc deficient are often picky eaters who will only eat a few foods – this of course worsens the zinc deficiency. Studies have also shown that children with ADHD who are unresponsive to stimulant drugs are more likely to be zinc deficient than children who respond favourably to these medications.(24) In addition zinc is an important component of the enzyme, delta 6 desaturase, which converts omega 3 fatty acids to DHA.(17) This could explain why children with low levels of zinc also have low levels of essential fatty acids in the blood. Vitamin B6 (pyridoxine) Studies have shown that pyridoxine can help ameliorate hyperactivity. (25) Vitamin B6 is an essential cofactor for a majority of the metabolic pathways of amino acids, including decarboxylation pathways for dopamine, adrenaline and serotonin. Coleman reported that B vitamins improved the behaviour of some children with ADHD in a double blind cross over comparison with methylphenidate.(25) It was also observed that high dose vitamin B6 reduced the symptoms while boosting serotonin levels into the normal range. Magnesium Another trace mineral that is highly important in ADHD is magnesium. This mineral has a multitude of uses within the body including the activation of several hundred different enzymes. Magnesium, like zinc, is a necessary cofactor required by the enzyme delta 6 desaturase. Magnesium is also a calming mineral that relaxes nerves and muscles and diminishes the effects of stress.(27) Recurrent infections, food or environment allergies and gastrointestinal parasites can all result in excessive magnesium loss.(27) Low magnesium may be associated with hyperactivity due to hyperirritability of brain neurons. Studies have shown that supplementation with magnesium can improve behaviour and cognitive performance in children with ADHD.(28) Adults with ADHD are also likely to require magnesium supplementation. Avoiding stimulants like caffeine, nicotine or amphetamines, as well as learning to manage stress and addressing physical problems such as chronic infection, allergies, gut dysfunction and parasitic infestation, are all important factors which will help to decrease further magnesium loss. Essential Fatty Acids (EFA’s) Several studies have indicated that some physical symptoms reported in ADHD are similar to symptoms observed in essential fatty acid (EFA) deficiency. One reliable symptom of EFA deficiency is excessive thirst (polydipsia) without matching polyuria.(29) An English ADHD support group reported that children with hyperactivity were significantly thirstier than children who were not hyperactive. Mitchell measured plasma fatty acids in 100 children and found hyperactive children had significantly lower concentrations of DHA, arachidonic acid and DGLA. Phosphatidyl Serine Phosphatidyl serine is clinically proven to benefit a wide range of brain functions. (30) This phospholipid occurs in the brain at far higher concentrations than it does in other organs. It is a key constituent of nerve cell synaptic membranes, which are deeply involved in the production of neurotransmitters. Ingested as a supplement, phosphatidyl serine energises the human brain, facilitating synaptic connectivity and specifically boosting dopamine transmitter functions i.e. its production, release, and post synaptic receptor actions. In a study of ADHD children aged between 4 and 19 years, dietary supplementation with phosphatidyl serine benefited greater than 90% of the cases.(32) At intakes of 100-300 mg/day of phosphatidyl serine, attention and learning were most consistently improved. Karen Donchak For additional information, please contact: Bio Concepts PO Box 1492 Eagle Farm BC, Qld 4009 References 1. Kidd PM: Attention Deficit/Hyperactivity Disorder (ADHD) in Children: Rationale for its integrative management. Alt Med. Rev. 5 (5) 2000 402-428 2. American Psychiatric Association (APA): Diagnostic and Statistical Manual of Mental Disorders (4th Edition), Washington DC APA 1994. 3. Biederman J et al: Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety and other disorders. Am. J. Psychiatry. 1991; 148:564-77. 4. Simeon JG: Pharmacotherapy of attention deficit hyperactivity disorder. Can. J. Psychiatry (1993); 38: 443-448. 5. Barkley RA: Attention Deficit Hyperactivity Disorder: A handbook for diagnosis and treatment. New York, Guilford Press; 1998. 6. Biederman J: Attention – deficit/hyperactivity disorder: a life-span perspective. J. Clin. Psychiatry 1998; 59-4-16. 7. Goldman LS et al: Diagnosis and treatment of attention deficit hyperactivity disorder in children and adolescents. J. Am. Med. Assoc 1998; 270:1100-1107. 8. Volkow ND et al: A new PET ligand for the dopamine transporter: studies in the human brain. J. Nuclear Med. 1995; 36:2162-2168. 9. Volkow ND et al: dopamine transporter occupancies in the human brain induced by therapeutic doses of oral methylphenidate. Am. J. Psychiatry 1998; 155:1325-1331. 10. Scarnati R: An outline of hazardous side effects of Ritalin (methylphenidate) Int. J. Addictions 1986; 21:837-841. 11. Indiana Prevention Resource Centre (IPRC) Factline on Non-medical use of Ritalin. Bloomington, IN: Indiana University (1998). 12. Medical Economics Company (MED) Physician’s Desk Reference, 53rd Edition Montvale, NJ: MED 1999. 13. Brucker-Davis F: Effects of environmental synthetic chemicals on thyroid function. Thyroid 1998; 8:827-856. 14. Brouwer A et al: Interactions of persistent environmental organohalogens with the thyroid hormone system: mechanisms and possible consequences for animal and human health. Toxicol Indust. Health 1998; 14:59-84. 15. Haddow JE et al: Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N. Engl. J. Med. 1999; 341:549-555. 16. Caron M: Serotonin may hold key to hyperactivity disorder. Science 1999. 17. Gant C: Complementary medicine approaches to ADHD. Presentation to Ann. Conf. American College of Advancement in Medicine (ACAM), Orlando Fl. May 1999. 18. Murray Mt et al: Encyclopedia of Natural Medicine. Rocklin. CA: Prima Publishing 1998 19. Crook WG: Sugar, yeast, and ADHD fact or fiction? Bellanti JA et al. Jackson TN International Health Foundation 1999. 20. Lyon M: Healing the Hyper Active Brain. Focus Publishing 2000 365-387. 21. Kidd PM: A review of five nutrients and botanicals in the integrative management of cognitive dysfunction. Altern. Med. Rev. 1999 4: 144-161. 22. Galland L. Nutritional supplementation for ADHD. Jackson TN: International Health Foundation 1999. 23. Bekaroglu M et al: Relationships between serum free fatty acids and zinc, and attention deficit hyperactivity disorder: a research note. J. Child. Psychol. Psychiatry 1996; 37: 225227. 24. Arnold LE et al: Dose hair zinc predict amphetamine improvement of ADD/hyperactivity? Int. J. Neurosci. 1990; 50: 103-107. 25. Coleman M et al: A preliminary study of the effect of pyridoxine. Biol. Psychiatry 1979 14: 741-751. 26. Kozielec T et al: Assessment of magnesium level in children with attention deficit hyperactivity disorder. Magnes. Res 1997; 10: 143-148. 27. Starobat-Hermelin et al The effects of magnesium physiological supplementation on hyperactivity in children with attention deficit hyperactivity disorder (ADHD). Magnes. Res. 1997; 10: 149-156. 28. Dykman KD et al: Effects of nutritional supplementation on attention deficit disorder. Integr. Physiol. Behav. Sci 1998; 33:49-60. 29. Burgess JR et al: Long chain polyunsaturated fatty acids in children with attention deficit hyperactivity disorder. Am. J. Clin. Nutr 2000 71;27-30 30. Colquhoun I et al: A lack of essential fatty acids as a possible cause of hyperactivity in children. Med. Hypotheses (1981);7:673-679. 31. Makrides M et al: Are long-chain polyunsaturated fatty acids essential nutrients in infancy? Lancet. 1995; 345:1463-1467. 32. Ryser CA: Benefits of PS (phosphatidyl serine) against attention deficit in a preliminary study. Lancet (letter in preparation). 33. Greenblatt J. Nutritional supplements in ADHD. J. Am. Acad. Child Adolesc. Psychiatry 1999; 38:1209-1210.