LW43.1: IN SITU (<5%) MANTLE CELL LYMPHOMA IN TWO PELVIC LYMPH NODES OF A
PATIENT, WITH A SMALL FOCUS OF A PROSTATIC ADENOCARCINOMA.
Patrick Browne1, Viera Nelson1 and Bharat N Nathwani2
1.Genzyme Genetics, Hematopathology, Los Angeles, USA
2.Cedars-Sinai Medical Center & University of Southern California, Hematopathology, Los Angeles, USA
patrick.browne@genzyme.com
Clinical history: 62 year old male underwent a radical prostatectomy, for rising PSA levels, that showed a
small focus of adenocarcinoma, Gleason score 3+3=6 and was staged as pT2. During the staging procedure,
he was found to have slightly enlarged bilateral peri-prostatic pelvic lymph nodes that were excised. He had
no signs or symptoms and no clinical evidence of lymphadenopathy or splenomegaly. A PET scan showed
only questionable uptake in the neck area and also questionable uptake in the right external iliac chain which
were felt to be non-specific findings. A bone marrow examination showed no flow cytometric or morphologic
evidence of involvement by lymphoma. Cytogenetic studies on the bone marrow were normal. He was felt to
be a candidate for surveillance only.
Details of biopsy: Right and left pelvic lymph nodes measured 1.8 x 1.1 x 0.3 cm and 4.5 x 3.2 x 1.8 cm
respectively and showed no metastatic carcinoma. Formalin fixation.
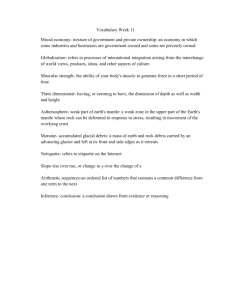
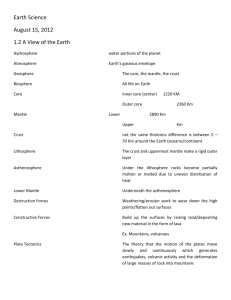
Histopathology: Both lymph nodes showed similar histologic features. More than 95% of the lymph nodes
had benign histologic features of sinus histiocytosis, multifocal hemorrhage, paracortical T-zone hyperplasia,
and scattered separated, uniform, generally round follicles whose germinal centers showed a mixture of
benign centrocytes and centroblasts, and moderate number showed polarity (photos 1,2). These germinal
centers were surrounded by well-defined mantle zones that were 10 to 25 mantle cell layer thick (photo 3).
The mantle cells were small, had round to irregular nuclei (depending on the fixation), condensed chromatin
structure and scant cytoplasm. Scattered, small mantle cell nodules present showed similar cytology to that
seen in the mantle zones.
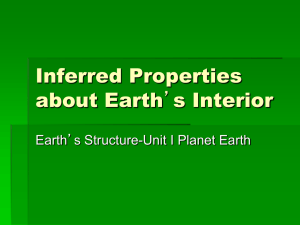
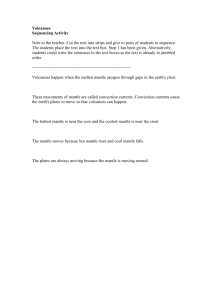
Immunohistochemistry/immunophenotype: <5% of mantle cells were Bcl-1+ (photos 4-7) and CD5+
(weakly) (photo 8). In addition, the mantle cells were also positive for PAX-5, CD20 (photo 9), IgD (photo
10,11), bcl-2, but negative for CD23, and CD3 (photo 12). Few bcl-1 positive cells were also seen immediately
outside the mantle zones and there was minimal extension inwards into the periphery of germinal centers.
Flow cytometry: The right and left pelvic lymph nodes were submitted to our laboratory for flow cytometric
analysis and both showed 4% CD5-positive monotypic B-cells with surface lambda light chain restriction in a
background of numerous polyclonal B-cells. The monoclonal B-cells also showed dim to moderate coexpression of CD23.
Genetic/molecular analysis: Cytogenetic analysis done on a bone marrow were normal.
Proposed diagnosis
In situ (<5%) mantle cell lymphoma.
Interesting feature(s) of the submitted case
1. This case, to the best of our knowledge, is the first case of an “in situ” mantle cell lymphoma in two pelvic
lymph nodes, and a small, localized adenocarcinoma in the prostate. Bcl-1 positive cells occupied <5% of the
total number of lymphoid cells by IHC in both pelvic lymph nodes, and this finding is in complete agreement
with flow cytometry results on both nodes that showed 4% monotypic B cells. Also, by flow cytometry, the
monotypic B-cells were CD23-positive in addition to CD5.
2. Without doing BCL-1 stain the diagnosis of mantle cell lymphoma could not have been made, and this stain
also showed that the malignant cells occupied < 5% of the total number of lymphoid cells which is a very small
tumor burden, hence an early stage of mantle cell lymphoma. Although there is low tumor burden, the mantle
zones of both pelvic lymph nodes were involved, due to "homing" of the Bcl-1 positive cells to the mantle
zones and to the mantle cell nodules. Occurrence of additional molecular abnormalities will result in histologic
and clinical progression, however, it cannot be predicted when they will occur.
 0
0