Inherited Disorders of the Red Cell Membrane Hereditary
advertisement

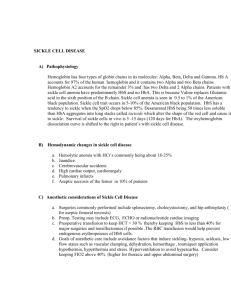
Inherited Disorders of the Red Cell Membrane Hereditary spherocytosis, transmitted as an autosomal dominant trait, is the most common inherited disorder of the red cell membrane. The disorder is a deficiency of membrane proteins (i.e., spectrin and ankyrin) that leads to gradual loss of the membrane surface during the life span of the red blood cell, resulting in a tight sphere instead of a concave disk. Although the spherical cell retains its ability to transport oxygen, it is poorly deformable and susceptible to destruction as it passes through the venous sinuses of the splenic circulation. Clinical signs are variable but typically include mild anemia, splenomegaly, jaundice, and bilirubin gallstones. A life-threatening aplastic crisis may occur when a sudden disruption of red cell production (in most cases from a viral infection) causes a rapid drop in hematocrit and the hemoglobin level. The disorder usually is treated with splenectomy to reduce red cell destruction. Hemoglobinopathies Hemoglobinopathies represent abnormalities in hemoglobin structure that can lead to accelerated red cell destruction. Two main types of hemoglobinopathies can cause red cell hemolysis: the abnormal substitution of an amino acid in the hemoglobin molecule, as in sickle cell anemia, and the defective synthesis of one of the polypeptide chains that form the globin portion of hemoglobin, as in the thalassemias. Sickle Cell Disease (Anemia). Sickle cell disease is a chronic disorder resulting in organ failure and premature death. The disorder affects approximately 50,000 (0.1% to 0.2%) black Americans. Approximately 8% of black Americans carry the trait. Sickle cell disease results from a point mutation in the β chain of the hemoglobin molecule, with an abnormal substitution of a single amino acid, valine, for glutamic acid. Sickle hemoglobin (HbS) is transmitted by recessive inheritance and can manifest as sickle cell trait (i.e., in heterozygotes with one HbS gene and one normal HbA gene) or sickle cell disease (i.e., in homozygotes with two HbS genes). In the homozygote with sickle cell disease, almost all the hemoglobin is HbS. In the heterozygote with sickle cell trait, only approximately 40% of the hemoglobin is HbS. In the homozygote, sickling occurs when the HbS becomes deoxygenated. The deoxygenated hemoglobin aggregates and polymerizes, creating a semisolid gel that changes the shape and deformability of the cell . Sickling of red cells is initially a reversible process with oxygenation. HbS returns to its normal depolymerized state. However, with repeated episodes of deoxygenation, the cells remain permanently sickled. These sickled red cells are abnormally adhesive, attach to the vessel wall, and cause accumulation of more cells that obstruct blood flow in the microcirculation, leading to tissue hypoxia. Sickled cells have a rigid and nondeformable membrane, predisposing to premature destruction and hemolysis. Thus, the life span of the sickled cells is markedly reduced. Perhaps the most important factor in promoting sickling is the amount of HbS and its interaction with other hemoglobin chains. The person with sickle cell trait who has less HbS has little tendency to sickle except during severe hypoxia and has virtually no symptoms. HbF does not interact with HbS or sickle; therefore, infants with sickle cell disease do not begin to experience the effects of the sickling until sometime after 4 to 6 months of age, when the HbF has been replaced by HbS. The factors associated with sickling and consequent blood vessel occlusion in persons with sickle cell disease include cold; stress; physical exertion; infection; illnesses that may cause hypoxia, acidosis, or dehydration; or even such trivial incidents as reduced oxygen tension induced by sleep. Chronic hemolysis produces rather severe anemia, .The hyperbilirubinemia that results from the breakdown products of hemoglobin often leads to jaundice and the production of pigment stones in the gallbladder. Children with sickle cell disease may experience growth retardation and susceptibility to osteomyelitis. Vaso-occlusion accounts for the most severe complications of sickle cell disease. An acute pain episode results from vessel occlusion and can affect almost any part of the body. Common sites obstructed by sickled cells include the abdomen, chest, bones . Acute chest syndrome is an atypical pneumonia resulting from pulmonary infarction. It affects approximately 40% of persons with sickle cell disease and is characterized by fever, chest pain, and cough. The most serious complication is stroke resulting from cerebral occlusion. The spleen is especially susceptible to damage by sickle cell hemoglobin predisposes the person to life-threatening infections by encapsulated organisms such as Streptococcus pneumoniae, Haemophilus influenzae type b, and Klebsiella species .Prophylactic penicillin should be begun as early as 2 months of age and continued until at least 5 years of age. Maintaining full immunization, including administration of H. influenzae and hepatitis B vaccines, is recommended.