Immunization Deficiencies Form
advertisement

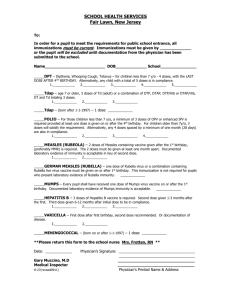
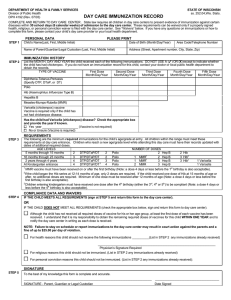
Woodbury City Public Schools School Health Office Immunization Deficiencies (Deficiencias de la inmunizacion) To the Parent/ Guardian of DOB / / Your child’s health record shows the following immunizations are incomplete. The boxes checked below indicate the dates that are missing. Vaccine Type DPT, Td Polio MMR Measles Rubella Mumps HIB Hepatitis B Mantoux Varicella Pneumococcal Vaccine (PreK) Influenza (PreK) Meningococcal Vaccine (Gr. 6) Tdap (Gr.6) Primary Series Doses ///////// ///////// ///////// ///////// First ///////// ///////// ///////// ///////// Booster 4 Year /////////////// /////////////// /////////////// /////////////// /////////////// /////////////// /////////////// Immunization Requirements (effective June 2012) DPT: Age 1-6 years: 4 doses, with one dose given on or after the 4th birthday, OR any 5 doses. Tdap: Grade 6: 1 dose Polio: Age 1-6 years: 3 doses, with one dose given on or after the 4th birthday, OR any 4 doses Measles: 2 doses of a live measles containing vaccine on or after the 1st birthday. Rubella and Mumps: 1 dose of live rubella- mumps-containing vaccine on or after the 1st birthday. Varicella: 1 dose on or after 1st birthday HIB: 1 dose after 1st birthday- (Preschool only) Hepatitis B: 3 doses Pneumococcal vaccine: Age 12-59 months- 1 dose (Preschool only) Meningococcal Vaccine: Grade 6 Influenza Vaccine: Age 12-59 months- 1 dose annually (Preschool only) Your doctor or clinic must administer the required immunization, and the confirmation of the administration must be given to the Nurse on or before ___________________________. Must show at least 1 dose of DPT, Polio & MMR for admission to school. After that date, the student will be excluded from school until the immunization is administered. Physician’s Name (print): ____________________________________________________________ Physician’s Signature: ______________________________________________________________ Physician’s Address: ___________________________________________________________________ Physician’s Phone Number: ________________________ Date of Examination_________________ 9/15