Immunization Form - Fair Lawn Schools
advertisement

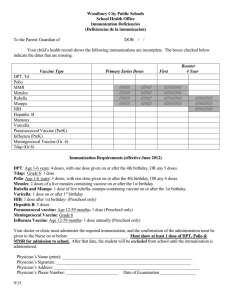
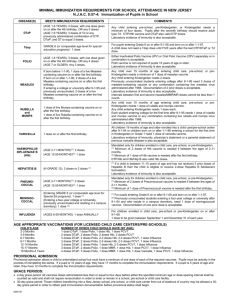
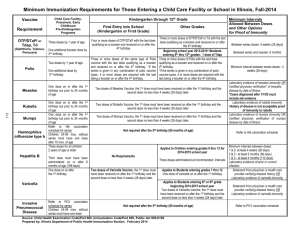
SCHOOL HEALTH SERVICES Fair Lawn, New Jersey To: In order for a pupil to meet the requirements for public school entrance, all immunizations must be current. Immunizations must be given by _____________ or the pupil will be excluded until documentation from the physician has been submitted to the school. Name_________________________ DOB_____________ School_______________ _____DPT – Diptheria, Whooping Cough, Tetanus – for children less than 7 y/o - 4 doses, with the LAST DOSE AFTER 4TH BIRTHDAY. Alternatively, any child with a total of 5 doses is in compliance. 1.____________ 2.____________ 3.____________ 4.____________ 5.____________ _____Tdap – age 7 or older, 3 doses of Td (adult) or a combination of DTP, DTAP, DTP/Hib or DTAP/Hib, DT and Td totaling 3 doses. 1.____________ 2.____________ 3.____________ _____Tdap – (born after 1-1-1997) – 1 dose ____________ _____POLIO – For those children less than 7 y/o, a minimum of 3 doses of OPV or enhanced IPV is required provided at least one dose is given on or after the 4th birthday. For children older than 7y/o, 3 doses will satisfy the requirement. Alternatively, any 4 doses spaced by a minimum of one month (28 days) are also in compliance. 1.____________ 2.____________ 3.____________ 4.____________ _____MEASLES (RUBEOLA) – 2 doses of Measles containing vaccine given after the 1st birthday, (preferably MMR) is required. The 2 doses must be given at least one month apart. Documented laboratory evidence of immunity is acceptable in lieu of second dose. 1.____________ 2.____________ _____GERMAN MEASLES (RUBELLA) – one dose of Rubella virus or a combination containing Rubella live virus vaccine must be given on or after 1st birthday. This immunization is not required for pupils who present laboratory evidence of Rubella immunity. ____________ _____MUMPS – Every pupil shall have received one dose of Mumps virus vaccine on or after the 1st birthday. Documented laboratory evidence of Mumps immunity is acceptable. ____________ _____HEPATITIS B – 3 doses of Hepatitis B vaccine is required. Second dose given 1-3 months after the first. Third dose given 6-12 months after initial dose to be in compliance. 1.____________ 2.____________ 3.____________ _____VARICELLA – First dose after first birthday, second dose recommended. Or documentation of disease. 1.____________ 2.____________ _____MENINGOCOCCAL – (born on or after 1-1-1997) – 1 dose ____________ **Please return this form to the school nurse Mrs. Frotten, RN ** Date: _____________ Gary Muccino, M.D Medical Inspector H-27(revised0911) Physician’s Signature: _____________________________________ _____________________________________ ________________________________ ________________________________ Physician’s Printed Name & Address