Pharmacology 14c – Diuretics
advertisement

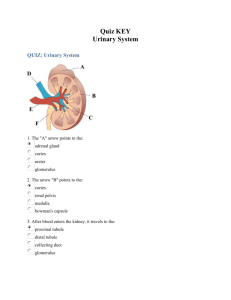
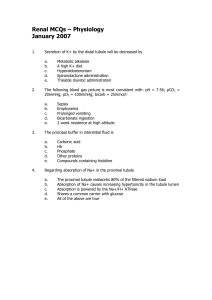
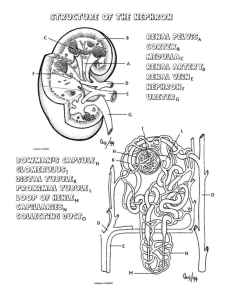
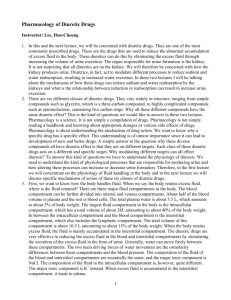
RENAL TUBULE. Pharmacology 14c – Diuretics Anil Chopra 1. 2. 3. 4. 5. Bowmans capsule Glomerular filtration Proximal tubule Distal tubule Cortex Revise the physiology of the 300 300 300 150 300 300 kidney, focusing on the mechanisms which regulate the Outer ionic composition (particularly medulla Na+, Cl- and K+), volume and 600 60 600 600 600 600 0 osmolarity of the urine. Inner Loop of Henle medulla Define the term diuretic. 1000 1000 1000 1000 1000 1000 Explain how the following 1200 1200 1200 1200 groups of diuretic drugs alter the ionic composition, volume and Collecting duct osmolarity of the urine osmotic diuretics, e.g. mannitol carbonic anhydrase inhibitors, e.g. acetazolamide loop diuretics, e.g. furosemide (frusemide) thiazides, e.g. bendroflumethiaze (bendrofluazide) potassium sparing diuretics. e.g. amiloride, spironolactone. Note that loop diuretics, thiazides and K+ sparing diuretics are clinically the most important groups of diuretics. For each of the following drugs (a) name the principal conditions for which they are used clinically, (b) list their main pharmacokinetic properties and (c) describe and explain where possible their principal adverse effects. (i) frusemide (ii) bendrofluazide (iii) amiloride (iv) spironolactone The proximal tubule is the principal site of Na, water and HCO3 absorption The ascending limb of the loop of henle is impermeable to water and so acts to increase the osmolarity of the interstitial fluid – this enables water reabsorption in the collecting duct Water reabsopriton in the collecting duct is under the control of arginine vasopressin (AVP) RENAL TUBULE. Ca reabsorption in the distal tubule Bowmans capsule is under control pf PTH (para thyroid hormone) Proximal tubule Distal Aldosterone controls Na and so Glomerular Cortex tubule filtration water reabsorption in the distal 300 300 300 150 300 300 tubule In the distal tubule as Na is Outer reabsorbed K is excreted – therefore medulla increased water excretion leads to 600 60 600 600 600 600 0 excess K excretion Inner Loop of Henle medulla Differing concentrations of filtrate 1000 1000 1000 1000 1000 1000 and interstitial fluid is shown on the 1200 1200 1200 1200 right Some things, e.g. drugs are actively Collecting duct secreted in the proximal tubule Diuretics: Drugs that act on the renal tubule to promote the excretion of Na+, Cl- and H2O. They are used to treat: - Hypertension - Salt and water overload Acute pulmonary oedema Heart Failure Liver cirrhosis and ascites Nephritic syndrome Renal Failure - Acute hypercalcaemia RENAL TUBULE. Bowman’s capsule Proximal tubule Glomerular filtration Distal tubule 1 2 HCO3Na+ 65-70% H2O 5 4 H2O Na+ Cl- Na+ Na+ Cl- Cl- H2O H2O Loop of Henle 3 1 H2O 1 Collecting duct (1) Osmotic Diuretics Names Mannitol Usage Prevent acute renal failure by increasing H2O excretion. Decrease intra-cranial pressure. Decrease intra-ocular pressure. Mode of Action It is pharmacologically inert. It is filtered by the glomerulus but not reabsorbed resulting in an increase in the osmolarity of the kidney tubule. This results in a decrease in water reabsorption in the proximal tubule, loop of Henle and collecting duct. H2 O Side Effects Can result in: dehydration hyponatraemia hypernatraemia nausea, vomiting pulmonary oedema (2) Carbonic anhydrase Inhibitors Names Acetazolamide Usage – generally weak diuretics used in: Metabolic alkalosis. Renal stones Decrease intra-ocular pressure in glaucoma. Mode of Action These act on the proximal tubule to prevent the reabsorption of HCO3- and Na+. This is results in less water being reabsorbed due to the low osmolarity of the proximal tubule cells and the intersitium. The high concentration of HCO3- in the distal tubule will also cause a reduction in K+ loss. Urine is therefore very alkaline. Side Effects Hypokalaemia Metabolic acidosis Self limiting action (3) Loop Diuretics Names - Frusemide Usage – powerful diuretics used in: Oedema – Heart failure, pulmonary, renal, hepatic, cerebral Moderate Hypertension - Piretanide Hypercalcaemia Hyperkalaemia Mode of Action It prevents the reabsorbtion of sodium and chloride ions in the ascending loop of Henle and is associated with a decrease in Ca2+ and Mg2+ reabsorption. This results in a lower osmolarity of the interstitium and hence less water will be reabsorbed in the descending limb and collecting duct. The increased Na+ in the distal tubule causes large K+ loss due to the Na+ / K+ exchange pump. Its overall effect excretion of a large amount of H20, Na+, Ca2+ and K+. Side Effects and Pharmacokinetics Administration – IV or oral Distribution – strongly bound to plasma proteins Clearance – secreted into tubular fluid, excreted unchanged T1/2 = 1-2hrs, duration of action longer - lasts 3-6hrs Hypovolaemia & Hypotension K+ loss (Ca2+/Mg2+), Metabolic Alkalosis Hypokalaemia (4) Thiazides Names Bendrofluazide (bendroflumethiazide) Usage Cardiac failure Hypertension – initially decrease blood volume/long-term = vasodilation Severe resistant oedema Idiopathic hypercalciuria - stone formation Nephrogenic diabetes insipidus (paradoxical) Mode of Action They inhibit Na+ and Cl- absorption in the early part of the distal tubule and so increase magnesium Mg2+ loss and Ca2+ reabsorption. This results in a decrease in water reabsorption in the collecting duct and therefore a moderate increase in urine volume and Na+, Cl- & K+ loss (Mg2+ loss). Other actions of thiazides: Vasodilation – due to opening of K channels Inhibition of insulin secretion (diabetogenic) – due to opening of K channels Diazoxide a non-diuretic thiazide has marked vasodilatory and diabetogenic actions Inhibition of uric acid secretion into the proximal tubule Side Effects and Pharmacokinetics Inhibits insulin secretion which can result in diabetes mellitus. The K+ loss can result in metabolic alkalosis. Uric acid retention – gout Hypokalaemia MECHANISM OF THIAZIDE ACTION Tubule lumen Interstitium 3Na+ ATPase Na+ Cl- 2K+ ClK+ - Thiazides » Admintration – well absorbed orally » Distribution – most bind to plasma proteins » Clearance – competes with uric acid for secretion into proximal tubule, excreted unchanged in urine » Onset of action 1-2hrs, duration of action 12-24hrs (5) Potassium Sparing Drugs Names Spironolactone, amiloride Usage Amiloride is used with other diuretics that result in K+ loss. Spironolactone is used in hyperaldosteronism (primary and secondary). Mode of Action They block aldosterone from binding to its receptor and amiloride inhibits the aldosterone sensitive Na+ channels, both resulting in an increase in Na+ loss, and K+ reabsorption. The osmolarity of the tubular fluid decreases causing decreased water reabsorption in the collecting duct. It also increases uric acid loss. Side Effects Hyperkalaemia, Metabolic Acidosis Spironolactone – Gynaecomastia, Menstrual disorders, Testicular Atrophy Diuretic Oral Onset Duration Excretion Other Osmotic diuretics i.v. 0.5h 1.5-3h Glom. Fil. Carbonic Anhydrase Inhibitors Good 0.5h 12h Tubular Secretion Loop diuretic Good 1h 4-6h Tubular secretion 50% unchanged 50% metab. Thiazides Good 1-2h 8-12h 24h Tubular secretion Compete with uric acid Spironolactone Good Days Canrenone Glom. Fil. Compete with uric acid Amiloride Poor 6h 24h Tubular secretion Unchanged in urine