Ocular antibiotics: a look at the past, a view of the present, and a
advertisement

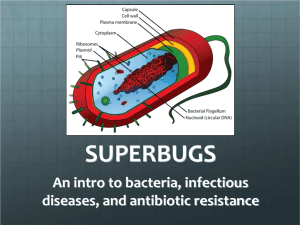
The new antibiotics: a look at the past, a view of the present, and a glance towards the future COPE ID 10146-AS Milton M. Hom, OD, FAAO. Course description (1 hour): In 1969, the US Surgeon General declared “we can close the books on infectious disease”. Unfortunately, bacteria are alive and well and sometimes even gaining on us. Is this the beginning of the end of the antibiotic era? We look at 4G and 5G fluoroquinolones, the antibiotic arms race, contact lens wear and the private lives of bacteria. A look at the past: Bacteria are 3.5 billion years old and still kicking They love us: we are the big buffet Reproduction Private lives of bacteria Bacteria have an “unembarrassed penchant for reproduction.” Francis Mah, MD Some bugs create a whole new generation every twenty minutes Adaptability The antibiotic era Began 1928 when Alexander Fleming discovered penicillin Used for World War II; general use late 1940s “We can close the books on infectious disease”. US Surgeon General, 1969 Is this the beginning of the end of the antibiotic era? Adaptability and resistance “The bugs are getting stronger-and they’re getting stronger faster” Barry Kreiswirth, New York City’s Public Health Research Institute Ten years ago: Nearly all strains of Streptococcus pneumoniae were susceptible to penicillin. Today: 45% of all strains are resistant. (Shnayerson and Plotkin, The Killers Within, Little Brown, 2002) Infrastructure: Animals and agriculture Five times as many domestic food animals as people in the United States Daily animal fecal excretion can be 5-400 times greater than humans Amount of feces excreted by a cow per day is 100 times more than a human Flies carry genetically exact antibiotic-resistant organisms from nearby animals. Ground water and streams contaminated with antibiotic-resistant bacteria Used to treat fruit trees, honeybees hives, and catfish and salmon farms. A view of the present: The arms race “The war between humans and bacteria seems like a hopeless one because of the sheer numbers of bacteria, their incredible ability to adapt, and their unembarrassed penchant for reproduction.” Francis Mah, MD (Mah FS.New antibiotics for bacterial infections. Ophthalmol Clin North Am. 2003 Mar;16(1):11-27) Pharmaceutical researcher’s chess game: Bacteria try to checkmate the best antibiotic move, the new antibiotic molecule attempts at checkmating the new bacterial strain Defenses Some succeeded in making cell walls impermeable Others created tiny pumps that vomited antibiotics out of the cell (efflux pump) Some have developed enzymes to attack the antibiotic and slice chemical rings Some antibiotics target an enzyme for attachment; bacteria have changed or replaced those enzymes Strict guidelines needed Correct dosing in specific and selected and properly diagnosed infections Correct period or duration of time Carefully selected patients The drugs: fluoroquinolones 3G fluorquinolones Ciprofloxacin (Ciloxan) 5ml $40.99 Ofloxacin (Ocuflox) 5ml $40.99 3G 4G fluorquinolones Levofloxacin (Quixin) Described in the same class as moxi and gati :American Family Physician 2000;61(9):2744. New formulation 1.5% levofloxacin 4G fluorquinolones 8-methoxy group (-OCH3) Targets both topo IV and DNA gyrase Efficacy versus 3G Moxifloxacin (Vigamox)(oral: Avelox 1999) Bulky side-chain in the C-7 position Gatifloxacin (Zymar)(oral: Tequin 1999) Dual mutations needed for resistance 2-fold to 4-fold better activity against Gram-negative ocular isolates BAK: does it really matter? Dosing (Schlech BA, et.al. Eradication of Bacteria from Infected Eyes by a Three Day BID Treatment with Moxifloxacin Ophthalmic Solution 0.5%) 140 patients with confirmed bacterial conjunctivitis Treated topically BID for 3 days Results: 81% were classified as microbiological successes. Bacterial keratitis (Laroche L, et.al. Bacterial Keratitis : Predisposing Factors, Clinical and Microbiological Review of 300 Cases) 300 cases over 20 month period Defined bacterial keratitis: Suppurative corneal infiltrate, and overlying epithelial defect. Risk factors found: Contact-lens wear 50.3% History of keratopathy 21% Trauma 15% Case report: Contact lens related infection History: 34 year-old female wanting SCL. In the past she reports a “red eye” with extended wear contact lens wear. Slit lamp evaluation: Inferior superficial punctate keratitis in both eyes, more dense in the right eye. Closer examination of the blink showed an incomplete blink. Diagnosis: Infiltrative keratitis and dryness Treatment: Use a steroid in combination (Tobradex)? 4G fluorquinolone resistance Ask patient about hospital based infections and treatments. “There will be a continual need for new antibiotics because bacteria are very adaptable. We’ve already seen some resistance to fourth-generation fluoroquinolones in some ocular isolates, mainly because they have been in the systemic world for years” “Typically antibiotics have a 7 to 10 year lifespan. We hope with the proper use this will be the case with the fourth-generation fluoroquinolones as well.” Deepinder K. Dhaliwal, MD A glance towards the future: 5G fluorquinolones: Trofloxacin (oral: Trovan) Azithromycin Linezolid