David Baldwin,Director,Environmental and
advertisement

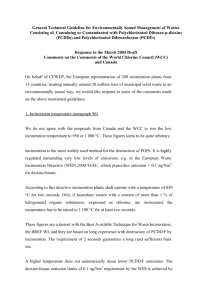
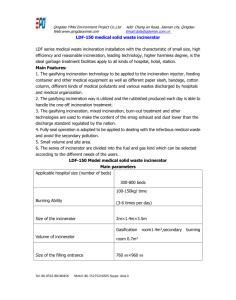
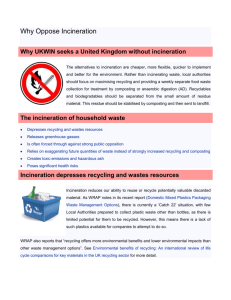
SELECTION OF HEALTH CARE RISK WASTE TREATMENT TECHNOLOGIES FOR GAUTENG Dave Baldwin Director, Environmental & Chemical Consultants, PO Box 2856, Cresta, 2118 Co-Author: Torben Kristiansen, Chief Technical Advisor, Gauteng Department of Agriculture, Conservation, Environment and Land Affairs, Rambøll, Hannemann & Hojland ABOUT THE SPEAKER Dave Baldwin graduated with a BSc Honours and PhD in chemistry from the University of Manchester Institute of Science and Technology in 1967. After three years of postdoctoral research in inorganic chemistry at the University of Washington, Seattle and University College London, he joined the Chemistry Department, University of the Witwatersrand in 1970 as a lecturer in Inorganic Chemistry and was involved in teaching and research, largely in inorganic chemistry for the next 16 years. This period included one-year sabbatical leaves at the California Institute of Technology, Pasadena in 1977and the Albert Einstein College of Medicine, New York in 1984. In 1982, Dave developed a strong interest in general and hazardous waste management and became a consultant to industry initially on all aspects of hazardous waste treatment and disposal. In 1986, he joined the CSIR as a programme manager, where he developed his interest in providing consulting services to industry in analytical chemistry, the development of chemical processes and solid and liquid waste management. He left the CSIR in 1990 to start Environmental and Chemical Consultants cc and has since provided consulting services in this area and been a director of Waste-tech (Pty) Ltd and Fraser Alexander Holdings. He was involved in the introduction of commercial “medical waste” treatment services into South Africa and developed a system for chemical waste management for small producers. He was a member of the working group that developed the Minimum Requirements for the Handling, Classification and Disposal of Hazardous Waste, which was published in 1994 and was the South African Hazardous Waste Consultant during the development of the National Waste Management Strategy in 1997 and 1999. Clients include waste management companies, the chemical and allied industries, mining industry and national, provincial and local government. ABSTRACT During the development of a Sustainable Health Care Waste Management Programme for Gauteng, a comparison was made of the environmental, health and safety impact and the advantages and disadvantages of the various treatment technologies for health care risk waste, i.e. burn technologies such as incineration, and non-burn technologies, such as microwaving and autoclaving. The costestimates are based the price level of 2002 and on South African manufactured incinerators, whereas the key technology component of non-burn treatment plants was assumed to be imported typically from the US or Europe. Furthermore, the costs are based on the environmental minimum requirements set out in the Health Care Waste Management Policy (November 2001) by the Gauteng Legislature and the current draft Health Care Waste Management Regulations that are expected to be promulgated in Gauteng in 2003. These requirements result in the need to install flue gas cleaning systems for all incinerators for the removal of acid gases, dioxins and heavy metals as well as the removal of dust, whereas the non-burn treatment plants will need to carry out detailed verification of the level of disinfection achieved. The study also included a cost comparison of the various technologies, which showed that microwaving was generally more expensive up to a capacity of 2000kg/hr. At low throughput capacities, i.e. <200kg/hr, incineration was more expensive than autoclaving but the costs became more comparable once the throughput increased above 500kg/hr. The costs of monitoring the emissions from incinerators and the sterilisation efficacy of non-burn technologies were also evaluated and will be presented. SELECTION OF HEALTH CARE RISK WASTE TREATMENT TECHNOLOGIES FOR GAUTENG INTRODUCTION South Africa has mainly used incineration as the technology of choice for the treatment of health care risk waste. However, an investigation into the status quo of health care risk waste management in Gauteng completed in 2000 (GDACEL, 2000) confirmed the general impression held by many practitioners that the management of this hazardous waste was in a parlous state. Most incinerators, particularly those in the public and private hospitals, were not operated to the required standards and, therefore, represent a significant environmental and health risk. During the subsequent development of a Sustainable Health Care Waste Management Programme for Gauteng, a comparison was made of the environmental, health and safety impact and the advantages and disadvantages of the various treatment technologies for health care risk waste, i.e. burn technologies such as incineration, and nonburn technologies, such as microwaving and autoclaving. Since, health care risk waste consists of four major waste types, i.e. infectious waste including sharps, chemical waste including pharmaceutical waste, pathological waste and radioactive waste, a waste management programme must cater for all four types of waste. A treatment technology, which is normally developed for sterilisation of the infectious component of the waste, must either be able to treat all waste streams or the different types must be separated at source. The main treatment options for health care risk waste include: Combustion Technologies, i.e. thermal treatment/combustion technologies: Incineration which includes: excess air, controlled air, rotary kiln and fluidised bed Plasma Arc and Pyrolysis Sterilisation/Disinfection Technologies, Steam sterilisation, e.g. Autoclaving Chemical sterilisation, e.g. with chlorine, glutaraldehyde Gas sterilisation, e.g. with ethylene oxide, formaldehyde Dry heat sterilisation, e.g. oil heated screw feed technology Electro-thermal deactivation (ETD), Microwave sterilisation, Irradiation sterilisation Cobalt-60 gamma rays Ultra violet Electron beam sterilisation The technologies indicated in italics are experimental or have limited commercial application internationally: UV treatment is largely effective only as surface treatment. Recent developments have resulted in the introduction of commercial non-burn facilities using Electrothermal Deactivation in Gauteng and the Western Cape, and Autoclaving in KwaZulu-Natal and a number companies are proposing the introduction of microwave facilities and a chemical sterilisation technology. Also, modern incinerators with scrubbers are being introduced or existing facilities are being modified to meet the expected more stringent gas emission standards. All of the above treatment technologies result in a residue, i.e. ash in the case of burn technologies or a sterilised/disinfected waste that has to be disposed to landfill. Note that in terms of the South African Minimum Requirements for the Handling, Classification and Disposal of Hazardous Waste, health care risk waste cannot be landfilled unless it is incinerated or otherwise sterilised. There are significant differences between burn and non-burn technologies and the most important of these are the types of health care risk waste that can be treated and the residues that are generated, as well as the type of emissions and where they occur; these are illustrated in figure 1. In the diagram it is assumed that the combustion treatment facility meets all the National and Provincial Standards and, therefore, can accept three of the major types of health care risk waste, i.e. infectious waste including sharps, chemical waste including pharmaceuticals and pathological waste, and that a gas cleaning system is used. Pathological (Anatomical) waste, which includes recognisable human parts, and chemical waste should not be handled by non-burn technologies and alternative technologies must be used for their treatment and disposal. Radioactive waste is not included in Figure 1, although selected low radioactive waste that comes from health care facilities could be treated, subject to permits. However, no radioactive waste can be treated by non-burn technologies and all must be disposed to special permitted waste landfills/depositories. Burn treatment technologies Infect waste & sharps Pathological waste Chemical waste Incineration Ash Landfill Flue gas cleaning residuals Emissions to air Leachate generation Non-burn treatment technologies Infectious waste & sharps Pathological waste Chemical waste Non-burn treatment Incineration, Cremation or Burial Treatment as a hazardous waste Noninfectious waste Landfill Ash or body parts Cemetery Waste or treatment residues to landfill Leachate generation + gas emissions to air Figure 1: Generic Differences Between Non-burn and Burn Technologies for the Treatment of Health Care Risk Waste INCINERATION/COMBUSTION TECHNOLOGY The main elements of modern incineration technology are illustrated schematically in Figure 2. Historically single chambered incinerators have been used for the treatment of health care risk waste and there are many still in use in Gauteng and the rest of the country. Further, developments included the introduction of multi-chambered incinerators, both excess air and starved air/controlled air types specifically designed and permitted for the treatment of the infectious waste stream. These incinerators are potentially capable of handling small quantities of chemical hazardous waste. An automatic feeding system is used for feeding the waste into the incinerator. The waste is combusted/pyrolysed in the primary combustion chamber with a stoichiometric deficit of air at temperatures ranging from 650oC to 1100oC. A support burner, usually fired by fuel oil or gas, is used both during start up and intermittently during operation to achieve and maintain the required temperature. The result is a bottom ash or slag and a gas stream containing combustible volatile organic compounds, particulates and potential pollutants. In the secondary combustion chamber, an excess of air is added and a secondary support burner fired by fuel oil or gas is used, if required, to maintain the temperature above 1100 oC to give complete burning of the combustible gases and solids from the primary chamber. A minimum retention time of 2 seconds is usually required. Energy can be recovered via a water/steam boiler but in South Africa this has been found to be uneconomic largely due to the small size of the incinerator and the relatively low cost of energy. The flue gas is cleaned using either wet, dry or semi-dry flue gas cleaning including a dust filter. Normally wet flue gas cleaning is not economic for health care risk waste incinerators because of their small size; hence, most plants make use of semi-dry or dry flue gas cleaning. Using flue gas cleaning systems, the strict emission limits for acid gases, particulates, heavy metals and dioxins set by many countries can be achieved. Common filters used are bag house filters or the more temperature tolerant ceramic filters. Typical neutralising agents for acid gases used are lime or bicarbonate products, possibly with activated carbon added for dioxin or heavy metal removal. Inputs: Waste Electricity, support fuel (oil/gas) & air Support fuel (oil/gas) & air Coling water (circulated) Dry process: Chemicals or Wet Process: chemicals + water Process: Feeding system Primary combustion chamber (solids and gases) Secondary combustion chamber (flue gases) Boiler/heat exchanger/cooling system Flue gas cleaning system Stack Heat and/or hot water (to be utilised) Dry process: Fly ash + used chemicals (landfilled) or Wet process: Fly ash + sludge (landfilled) and waste water (sewer system) Cleaned flue gas (to the air) Outputs: Bottom ash (landfilled) Figure 2: Flow Diagram of a Modern Incineration Plant. The typical inputs and outputs of materials and energy for the modern incineration process are also indicated in figure 2. The ash and any other solids and liquid wastes, e.g. from gas cleaning, must be classified, as required by the Department of Water Affairs and Forestry’s Minimum Requirements for the Handling, Classification and Disposal of Hazardous Waste, and disposed to an appropriate hazardous or general waste landfill. ADVANTAGES AND DISADVANTAGES OF INCINERATION The main advantages and disadvantages of incineration as a technology for the treatment of health care risk waste are listed in table 1. Table 1: Advantages and Disadvantages of Incineration Advantages of incineration Safe elimination of all infectious organisms in the waste at temperatures above ~700oC Flexible, as it can accept pathological waste and depending on the technology chemical waste. Residues are not recognisable Reduction of the waste by up to 95% by volume or 83 to 95% by mass: typically 5-17% ash is obtained. Very well proven technology No pre-shredding required No special requirements for packaging of waste Full disinfection is assumed to have occurred provided the high temperatures are maintained and the ash quantity is adequate. No monitoring of sterilisation efficiency is required. Disadvantages of incineration Normally higher investment costs required for incinerator and flue gas cleaning compared to nonburn technologies Point source immediate emissions to the air (as opposed to attenuated emission of CH4 and CO2 from landfill body over a period of decades) High cost of monitoring gas emissions and demonstrating compliance to emission standards. Solid and liquid by-products must be handled as potentially hazardous waste (may not apply to bottom ash if waste is well sorted and FGC residues handled separately) Incineration is perceived negatively by many sections of the community. PVC and heavy metals in the waste provide a significant pollutant load on the gas cleaning system (and for heavy metals on the quality of bottom ash also). Existing health care risk waste incinerators in South Africa cannot accept significant amounts of chemical waste because of refractory damage (but above you argue that modern plants can to some extent.) Separation at source is a key requirement for the correct management of health care risk waste, but incineration with flue gas cleaning is more forgiving than many other technologies, as it can accept pathological waste and, depending on the amount, the type of incinerator and its construction, chemical waste. For many of the pyrolytic dual chamber incinerators currently in use in South Africa, the amounts of chemical, including pharmaceutical waste that can be accepted is low. Thus, like normal household waste, which contains small amounts of hazardous chemical waste, the infectious waste stream must be expected to include small amounts of pharmaceuticals, chemicals used in wards, such as disinfectants, solvents, etc., even when a programme for separation at source has been instituted. An incinerator can readily accept this waste stream. However, most of the current incinerators available in South Africa should not deliberately accept chemical including pharmaceutical waste due to damage to the incinerator and significantly increased requirements for gas cleaning. ENVIRONMENTAL, HEALTH AND SAFETY IMPACT OF INCINERATION Incineration has proven to be a very effective way of sterilising health care risk and no special tests to determine the efficacy of the sterilisation process is normally required. However, in the past, most of the health care risk waste incinerators in South Africa have been poorly operated and almost all have not been fitted with emission control equipment. Tests on the emissions have shown that the incinerators are unable to meet the current DEAT Emission Guidelines for a Schedule 39 Process for some heavy metals and for HCl. Gauteng Province has decided to insist that, in future, incinerators meet the DEAT Emission Guidelines as a minimum requirement and this means that gas-cleaning equipment will be needed. With modern wet or dry gas cleaning techniques, incinerators have been able to meet the strict standards imposed in the USA and the European Union. Apart from gas emissions, incinerators produce an ash, which normally classifies as hazardous, although it can be delisted to general sites, if chemically stabilised with lime or treated by cementation; the volumes of ash generated are small. Source separation can result in reduced amounts of heavy metals being present in incinerator ash and potentially facilitate delisting of the ash, although two of the major problem metals, lead and zinc, are introduced with PVC because of the use of lead and zinc soaps during the production process. Gas cleaning can be accomplished by both wet and dry scrubbing. Dry scrubbing is generally preferred, as it is more economic for the typical HCRW incineration plant capacity, and, the resulting solid, which may be classified as hazardous, can be disposed to hazardous waste landfill, whereas the liquid wastes generated by wet scrubbing is charged a premium when disposed to landfill. Incineration is still a very common technology for health care risk waste treatment internationally, as it can meet the required strict environmental requirements, provided they are well operated and have good emission control equipment. However, in world regions with no or limited mass incineration of domestic or commercial waste steam sterilisation, microwave treatment and other non-burn technologies are fast becoming the most effective HCRW treatment technology with increasing costs of flue gas cleaning. MICROBIAL INACTIVATION USING NON-BURN TECHNOLOGIES Increasing emission requirements resulting in increasing cost of flue gas cleaning for incineration plants as well as an unfavourable perception of incineration has lead to the development of a range of sterilisation/disinfection technologies for the treatment of health care risk waste (see the introduction). Autoclaving, microwaving and ETD sterilise result in heating of the waste to moderate temperatures, 90oC to 160 oC, which results in its sterilisation, provided all the waste is subjected to the required temperatures for sufficient time. The sterilisation standards are discussed in the following paper (L Godfrey et al., 2003). Chemical treatment on the other hand uses a chemical sterilising agent to achieve equivalent treatment standards. In this paper, microwave technology will be briefly discussed as a typical non-burn technology. In the microwaving process, infectious waste is normally wetted or exposed to high-temperature steam, shredded and the moisture in the waste heated by a series of microwave generators for a specified period. The temperatures reach ~95 oC and the microorganisms are killed in the process, resulting in a residue that is confetti-like and slightly moist. Microwaving has been used to treat such items as sharps, microbiological materials, blood, and biological fluids. It is not suitable for the treatment of pathological chemically hazardous, or radioactive wastes and large quantities of metals can reduce the effectiveness of the microwaves’ penetration of the waste. Air emissions from the shredder and treatment plant are usually treated to remove moisture and volatile organic carbon compounds. The volume of the final waste product is reduced significantly by shredding and compaction of the final product, but almost no mass reduction occurs. Inputs: Waste Water (if waste is dry) Power to feed microwave generator Process: Feeding system Size reduction Heat and microwave treatment Compaction Water vapour Waste water Unloading to container/truck Transport to landfill Gas Cleaning Outputs: Gas Emissions Landfilling of treated waste Figure 2: Flow Diagram of a Typical Microwave Plant ADVANTAGES AND DISADVANTAGES OF NON-BURN STERILISATION TECHNOLOGIES The main advantages and disadvantages of autoclaving, microwaving and ETD technologies are in many ways similar and these are listed in the first row of table 2: there are some differences, however, and these are highlighted in rows 2 to 4. Table 2: Advantages and Disadvantages of Autoclave, Microwave and ETD Sterilisation Technologies Advantages Autoclaving, Microwaving ETD and DHS (Cross cutting) High sterilisation efficiency under appropriate conditions; Volume reduction depending on type of shredding/compaction equipment that has been installed Low risk of air pollution Moderate operation costs Easier to locate as generally more acceptable to communities and neighbours than incineration Recovery technologies can be used on sterilised waste Disadvantages Autoclaving Proven system that is familiar to health-care providers Relatively High Sterilisation Temperature Microwaving Low capacity units are available for small waste producers e.g. clinics and GPs Moderate investment costs Low Sterilisation Temperature may lower energy costs Electro-thermal Deactivation Low Sterilisation Temperature may lower energy costs Not suitable for pathological waste and chemical waste, including pharmaceuticals and cytotoxic compounds Good waste segregation required No or limited mass reduction Shredders are subject to breakdowns and blocking and repairs are difficult when the waste is infectious. It is not possible to visually determine that waste has been sterilised Waste is not rendered unrecognisable or unusable, if not shredded either before or after sterilisation. High monitoring costs to demonstrate compliance with sterilisation standards Treated waste must be disposed to landfill Air filtration is needed Operation requires highly qualified technicians. HEPA filters must be maintained and replaced regularly. Significant amounts of volatile organic carbon compounds produced Contaminated water must be discharged to sewer Waste and containers must have good steam permeability, especially if there is no prior shredding No waste reduction Unsuitable for very high quantities of infected metal (e.g. needles from inoculation campaigns) Low sterilisation temperature increases time required for treatment. Relatively high investment and operating costs Low sterilisation temperature increases time required for treatment. Autoclave, Microwave, ETD and DHS technologies cannot accept all the health care risk waste streams. Pathological (anatomical) waste, chemical waste and radioactive waste should be separated as well as possible at source. However, it is estimated that these components only represent 5% of the total health care risk waste stream and therefore non-burn technologies can treat the bulk of the waste stream. ENVIRONMENTAL, HEALTH AND SAFETY IMPACT OF STERILISATION TECHNOLOGIES The environmental and health impacts of the Autoclaving, Microwaving, and ETD technologies are potentially low compared to incineration, which generates large quantities of gas that is immediately emitted to the air. However, landfilling of sterilised waste results in anaerobic biodegradation of the waste, which will give methane a gas, which is a greenhouse gas with greater impact than carbon dioxide. One of the main problems is that good separation at source is required particularly to ensure that chemical including pharmaceutical wastes are not treated as the resulting sterilised waste will probably be classified as hazardous. Small amounts of gaseous emissions must be expected to be released during the sterilisation process and shredding, particularly if the waste has been poorly segregated at source, and appropriate precautions must be taken to remove these. Also, most sterilisation technologies require the waste to be shredded and, if accomplished before the sterilisation process, there are potentially significant health and safety risks for the staff, when a shredder breaks down or becomes blocked, e.g. by a large metal object. The cleaning procedure must be well defined, include the use of appropriate PPE and preferably include disinfection or sterilisation of the waste before manual cleaning and repair is undertaken. For the microwaving and ETD processes, special precautions must be taken to protect personnel against the electromagnetic radiation that is used. A COST COMPARISON OF SELECTED HCRW TREATMENT TECHNOLOGIES Financial estimates of the costs of the various health care risk waste treatment technologies were made and were based on data obtained from suppliers, and companies that are actually in the process of setting up or are operating such facilities. The data has, however, been adjusted for civil works, environmental protection measures, and should be viewed as indicative costs only: the price level used in all calculations was that pertaining in February 2002. The assumptions used were: The estimated salary costs would include all statutory contributions, holidays, shifts, sick leave, medical etc. The cost for the establishment of a new building or renovation of an existing building to house the plant is included in the estimated costs. A standard fixed amount for consultancy fees and other expenditure required to obtain an EIA authorisation from the Province plus any other legal requirements such as a Schedule 39 permit for an incinerator was included. Salaries were based on normal South African levels. The cost of equipment was based on International/South African price levels for delivery in Gauteng and was obtained from suppliers, plant operators and international publications. Incinerators include gas-cleaning equipment, i.e. lime treatment plus a ceramic filter. Note that, often, building some or all of a plant in South Africa can considerably reduce costs and the capital estimates for incinerators include this assumption. The cost of civil works and installation were based on Gauteng prices Economic life of civil works and treatment technologies: 12 years Economic life of internal storage and transportation equipment: 10 years The following costs are not included: i) Infrastructure at the generators site, ii) Establishment of public utilities used, e.g. landfills iii) Cost of administration, invoicing, marketing etc. iv) Cost of training of operators v) Cost of PPE/OSH programmes. vi) Value Added Tax. Depreciation costs are estimated as 10 years for equipment and 15 years for other capital and a real interest rate of 12% p.a. The operational hours for the plants were based on operation for 26 days per month and 12 months per year. However, the maximum operational hours were varied as follows: i) Incinerators < 200kg/hr: 12 hrs per day with manual de-ashing ii) Incinerators 200kg/hr: 20 hours per day with automatic de-ashing iii) Non-burn Technologies: 24 hours per day The costs for disposal of residues, such as the ash and gas cleaning waste from incinerators, and sterilised the waste from non-burn technologies, were estimated using current disposal costs. It was assumed that the ash from incinerators requires treatment with 2.5% lime in order to minimise its impact on the landfill. Residues from non-burn are assumed deposited at normal landfill sites, whereas residues from incinerators are assumed deposited at a Hazardous Waste Landfill site. For non-burn technologies an estimate of the costs of disposal of pathological waste and chemical waste that could not be treated by the technology was included. Table 4 gives the comparative costs estimated for microwaving, autoclaving and incineration. The data for microwaving and autoclaving technology can be taken as being illustrative of the costs expected for the other non-burn thermal technologies such as the ETD and Dry Heat Sterilisation, as the investment costs and operational costs are expected to be similar for these technologies. Table 3: Comparative Costs for Various HCRW Treatment Technologies Investment Cost, R Running Costs*, R R/kg millions millions/yr Microwaving 100 5.83 2.33 3.27 250 7.40 3.10 1.95 1000 10.61 5.09 1.08 Autoclaving 100 4.84 1.82 3.03 250 6.34 2.55 1.34 1000 9.90 5.14 1.71 Incineration 100 3.96 1.66 5.55 250 5.16 2.49 2.00 1000 7.42 4.53 0.97 * Running Costs = Interest + Depreciation on Capital + Operating Costs but cost of monitoring excluded Capacity, kg/hr The results indicated the following: a) As expected, the cost for treating a kg of waste decreases dramatically as the capacity of the plant increases. b) For incineration, there is a discontinuity that occurs below 200kg/hr due to the assumptions made, i.e. the capital cost for the larger plants is increased because automatic de-ashing is included but this is accompanied by an increase in the maximum operating hours for the larger automated plants from 12hrs per day to 20hrs per day. This increase in operating hours decreases the expected cost per kilogram significantly. c) The costs in table 3 are based on operating the facility at its maximum capacity. For example, operating the 1000kg/hr autoclaving plant for 8 hrs/day or one shift gives a treatment cost of R1.71/kg; for 16 hours or two shifts, R0.85/kg, and for 24 hours or three shifts, R0.71/kg. Clearly, the treatment facility should be operated as far as possible at full capacity, as this decreases the overall costs of treatment: a central facility handling waste from many sources will clearly be more cost effective than many small plants, particularly in urban areas, where the transport distances are relatively small. d) According to the available data, microwaving is relatively expensive compared to the other two technologies but the costs per kilogram treated become comparable with those of other technologies at higher loads. e) The investment costs for incineration appear to be relatively low compared to the other two technologies. This can, at least in part, be attributed to the fact that the cost of the incinerators are based on them being manufactured in South Africa, whereas capital costs for the other two technologies are based on imported equipment. MONITORING OF INCINERATOR EMISSIONS One of the major concerns expressed by participants in the Gauteng project was the potentially high cost of monitoring of the performance of health care risk waste treatment technologies. A study was undertaken for Department of Agriculture, Conservation, Environment and Land Affairs (Baldwin, 2003) on the costs of testing incinerator emissions and a separate study considered the cost of evaluating the sterilisation efficiency non-burn technologies (L Godfrey et al., 2003), which is considered in detail in the next paper. Until the new Air Quality Management Bill is enacted and new emission standards have been set, the current requirements in terms of schedule 2 of the Air Pollution Prevention Act (Act 45 of 1965) have been used, see table 4. An incinerator will have to undergo performance testing, where the operator demonstrates that the facility can meet the requirements set out the ROD and undergo a standard or minimum monitoring programme for at least one year. Once the facility has demonstrated that it routinely meets the requirements, it can apply for a reduction in frequency of analysis, i.e. to the minimum required programme. Note that from table 4, continuous monitoring of PM/dust, CO, O 2, water vapour, HCl and SO2 is proposed. The instrument and operating costs were obtained from a number of reputable South African suppliers of equipment and an average value taken for instruments from various sources. Note the cost of a dioxin analysis of R80000.00 includes the collection of duplicate samples by a South African company and analysis by a laboratory overseas, e.g. in Germany. Table 4: Approximate Costs for the Performance Testing and the Standard and Minimum Monitoring Programmes Minimum Requirements Performance Testing Monitoring Frequency (Permit conditions can vary) Standard Performance Standard (minimum) per Analysis, Analysis, year R R per year Minimum Analysis, R per year Units mg/Nm3 PM/dust 180 Continuous Continuous a) CO O2 Water vapour TOC Dioxin/furan (nanogram) TEQ - Continuous Continuous Continuous - Continuous Continuous Continuous - a) a) a) - 68 000 9 000 b) - 68 000 9 000 0.2 1 2(1) 80000 160 000 80 000 HCl 30 Continuous Continuous a) 100 000 100 000 HF SO2 25 Continuous Continuous a) 11 500 11 500 NOx - - - - - - NH3 - - - - - - 0.5 1 2 (1) 10000 20 000 10 000 60 720 720 90,000 868,000 1,041,000 370,000 283,000 Pb, (same for Cr, Be, Ar, As, Sb, Ba, Ag, Co, Cu, Mn, Sn, V, Ni) Cd (same for Tl) Hg LOI for ash 0.05 0.05 <5% 1 1 1 2 (1) 2 (1) 12 - Total Estimated Costs (to nearest R1000) a) b) c) Capital Cost Equipment Depreciation Cost Annual Running Costs Costs already included as continuous monitors fitted. No additional cost, as normally measured by CO analyser. Value to be confirmed with DACEL – may change. Thus, the monitoring cost for the standard programme is estimated at ~R370,000 per annum and the minimum analysis as R280,000 per annum, a reduction of ~24%. Clearly, the actual cost per kilogram of waste treated will vary significantly depending on the amount of waste that is treated in the incinerator. In order to get a better comparison of the impact of monitoring costs on the overall cost of treating health care risk waste, the values derived in table 6, were used to calculate the treatment cost per kilogram for incinerators ranging from 100kg/hr to 1000kg/hr: the results are presented in table 5. Note that the scenario is based on that used in the project feasibility study and assumes the incinerators are all working at full capacity, i.e. for a 100 kg/hr incinerator for 12 hours per day and for the larger incinerators for 20 hours per day and 26 days per month. Table 5: Cost per kilogram of waste treated Waste First Year Monitoring, Throughput, kg/hr Standard % of cost/kg* Programme, R 100 7.09 22 250 2.37 16 500 1.43 8.2 1000 1.00 7.0 * Compared to zero monitoring costs Second & Subsequent Years Minimum Programme, R 6.49 2.22 1.36 0.96 Monitoring, % of cost/kg * 14 9.0 6.2 4.0 CONCLUSIONS AND RECOMMENDATIONS Incineration and non-burn technologies have been compared both from a financial and environmental point of view and, provided all are operated within the proposed standards, there appears to be little to choose between them. Incineration is, however, more versatile since if fitted with gas cleaning equipment it can readily handle most types of health care risk waste, whereas separation of chemical and pathological waste at source must be undertaken with non-burn technologies. As might be expected, the greater the capacity of the treatment facility and the higher the operating hours, the lower the cost of treatment, which supports the provision of a few large facilities in an urban environment such as Gauteng. A study was also undertaken into the monitoring of incinerator stack emissions and continuous monitoring is proposed for the parameters, PM/dust, CO, O2, water vapour, HCl and SO2. A monitoring programme clearly increases the overall cost of treatment significantly for a small incinerator, whereas the percentage increase in cost for a large facility is relatively small. REFERENCES Baldwin D, Report “Evaluation of the Emission Monitoring Requirements for HCRW Incinerators” for Gauteng Department of Agriculture, Conservation, Environment and Land Affairs, September 2002 Gauteng Department of Agriculture, Conservation, Environment and Land Affairs, Final Report on Feasibility Study into the Possible Regionalisation of Medical Waste Treatment/Disposal Facilities in Gauteng, September 2000 Godfrey L et al, Validation and Monitoring of Non-Burn Health Care Risk Waste Treatment Facilities in Gauteng, Conference “Healthcare Waste Management in Africa Today”, Sandton Convention Centre, Sandton, South Africa, August 2003