COMMITTEE FOR PHYSICIAN`S HEALTH
advertisement

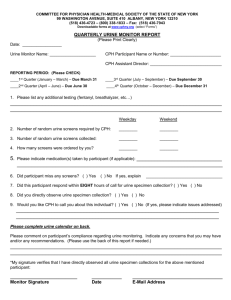
COMMITTEE FOR PHYSICIAN HEALTH-MEDICAL SOCIETY OF THE STATE OF NEW YORK 99 WASHINGTON AVENUE, SUITE 410 ALBANY, NEW YORK 12210 (518) 436-4723 – (800) 338-1833 – Fax: (518) 436-7943 Downloadable forms at www.cphny.org (select “Forms”) QUARTERLY URINE MONITOR REPORT (Please Print Clearly) Urine Monitor Name: _________________________________ CPH Participant Number: __________________ CPH Assistant Director: ___________________ REPORTING PERIOD: (Please CHECK) ____1st Quarter (January – March) – Due March 31 ____3rd Quarter (July – September) – Due September 30 ____2nd Quarter (April – June) – Due June 30 ____4th Quarter (October – December) – Due December 31 1. Please list any additional testing (fentanyl, breathalyzer, etc…) ________________________________________________________________________ ________________________________________________________________________ Weekday Weekend 2. Number of random urine screens required by CPH: ________ ________ 3. Number of random urine screens collected/ordered by you: ________ ________ 4. Please indicate medication(s) taken by participant (if applicable): _____________________________ ______________________________________________________________________ 5. Did participant miss any screens? (If yes, please explain in comment section below.) ( ) Yes ( ) No 6. Did this participant respond within EIGHT hours of call for urine specimen collection? ( ) Yes ( ) No 7. Did you directly observe urine specimen collection? ( ) Yes ( ) No 8. Would you like CPH to call you about this individual? ( ) Yes ( ) No Please comment on participant’s compliance regarding urine monitoring. Indicate any concerns that you may have and/or any recommendations. ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ Please complete urine calendar on back by circling the dates screens were collected. *My signature verifies that I have directly observed all urine specimen collections for the above mentioned participant: _____________________________ _____________ _______________________________________ Monitor Signature Date E-Mail Address Revised: 1/15/2015 Please list the testing date and requisition number (which is located in box #3 on the chain of custody form) for each sample collected. Date Date Requisition Number Requisition Number 2016 January '16 Su M Tu W Th 3 10 17 24 31 4 11 18 25 5 12 19 26 6 13 20 27 7 14 21 28 Su M Tu W Th 3 10 17 24 4 11 18 25 5 12 19 26 6 13 20 27 7 14 21 28 February '16 F 1 8 15 22 29 Sa 2 9 16 23 30 Su 7 14 21 28 M 1 8 15 22 29 Tu 2 9 16 23 F 1 8 15 22 29 Sa 2 9 16 23 30 Su 1 8 15 22 29 M 2 9 16 23 30 Tu 3 10 17 24 31 April '16 M Tu W Th 3 10 17 24 31 4 11 18 25 5 12 19 26 6 13 20 27 7 14 21 28 Th 4 11 18 25 F 5 12 19 26 Sa 6 13 20 27 Su M 6 13 20 27 7 14 21 28 Tu 1 8 15 22 29 F 6 13 20 27 Sa 7 14 21 28 Su M Tu 5 12 19 26 6 13 20 27 7 14 21 28 May '16 July '16 Su W 3 10 17 24 March '16 W 4 11 18 25 Th 5 12 19 26 Sa 2 9 16 23 30 Su 7 14 21 28 October '16 M 1 8 15 22 29 Tu 2 9 16 23 30 W 3 10 17 24 31 Th 4 11 18 25 M Tu W Th F 2 9 16 23 30 3 10 17 24 31 4 11 18 25 5 12 19 26 6 13 20 27 7 14 21 28 Sa 1 8 15 22 29 Su M 6 13 20 27 7 14 21 28 Tu 1 8 15 22 29 W 2 9 16 23 30 Th 3 10 17 24 F 4 11 18 25 Sa 5 12 19 26 W 1 8 15 22 29 Th 2 9 16 23 30 F 3 10 17 24 Sa 4 11 18 25 September '16 F 5 12 19 26 Sa 6 13 20 27 Su M Tu W 4 11 18 25 5 12 19 26 6 13 20 27 7 14 21 28 November '16 Su Th 3 10 17 24 31 June '16 August '16 F 1 8 15 22 29 W 2 9 16 23 30 F 4 11 18 25 Th 1 8 15 22 29 F 2 9 16 23 30 Sa 3 10 17 24 December '16 Sa 5 12 19 26 [42] Su M Tu W 4 11 18 25 5 12 19 26 6 13 20 27 7 14 21 28 Th 1 8 15 22 29 F 2 9 16 23 30 Sa 3 10 17 24 31