Lip Teh
Inverted Nipples
First described by Ashley Cooper 1840
2% of women have at least 1 inverted nipple
Unilateral more common than bilateral
Aetiology
1. CONGENITAL (most common)
i. Lack of dense connective tissue beneath the nipple that normally plays an
important role in maintaining its projection. Worse in association with greater
subcutaneous fat accumulation. (Schwager)
ii. A lack of smooth muscle growth into the nipple from the areolar
iii. Scarring under the nipple
iv. Arrest of the ductal system development = relative shortness of the lactiferous
ducts, which tether the nipple and prevent it projecting.
v. Abnormal fibromuscular structures encompass the lactiferous ducts and are
inserted in the nipple dermis, holding it in the inverted position. (Pitanguy)
2. Acquired i. Mastitis
ii. Macromastia
iii. Breast reduction surgery
iv. Breast carcinoma (need to exclude)
v. Scarring post breast feeding
Classification (Han and Hong 1999)
Grade I.
The inverted nipple is easily pulled out, maintains its projection fairly well without
traction. Gentle finger pressure around the areola or gently pinching the skin causes the
nipple to pop back out.
Minimal or no fibrosis. There is no soft-tissue deficiency of the nipple. The lactiferous
duct should be normal without any retraction.
Grade II.
The nipple can be pulled out manually, but not as easily as in grade I. After releasing
traction, the nipple tends to fall back and invert again.
Moderate degree of fibrosis. The lactiferous ducts are mildly retracted but do not need to
be cut for the release of fibrosis. On histologic examination, these nipples have rich
collagenous stromata with numerous bundles of smooth muscle
Grade III.
The nipple is severely inverted and retracted. It is very difficult to pull out these nipples
manually. Despite application of pressure on the nipple to force it to protrude, it
promptly retracts.
The fibrosis is remarkable and lactiferous ducts are short and severely retracted. The bulk
of soft tissue is markedly insufficient in the nipple. Histologically, there are atrophic
terminal duct lobular units and severe fibrosis
Lip Teh
Clinical Problems
1) Functional
a. Breast feeding
b. Frequent irritation and inflammation due to poor hygiene and the
inability to clean within the inversion.
2) Cosmetic/Psychological/sexual
Treatment
1) medical (for breast feeding)
a. Breast shells( milk cups, breast cups, or breast shields)
i. uses elasticity of the skin during pregnancy
ii. applying gentle constant pressure to the areola in an effort to
break the adhesions under the skin that prevent the nipple from
protruding.
iii. Ideally, shells should be worn starting in the third trimester of
pregnancy for a few hours each day.
iv. After the baby is born, these same shells can be worn about 30
minutes prior to each feeding to help draw out the nipple even
more.
v. any milk collected in them should NOT be saved.
b. Hoffman Technique.
i. Manually stretching out nipple 5x/day
c. Breastpump./Nipple suction device
i. After birth, breastpump can be helpful at drawing out a flat or
inverted nipple immediately before
ii. can be used at other times following delivery to help further break
the adhesions under the skin by pulling the nipple out uniformly
from the center.
d. Nipple stimulation.
i. After birth, if the nipple can be grasped, a mother can roll her
nipple between her thumb and index finger for a minute or two
and then quickly touch the nipple with a moist, cold cloth or ice
wrapped in cloth
e. Nipple shield.
i. flexible nipple made out of silicone that is placed over the
mother's nipple during feedings so that latch-on is possible for
the baby.
ii. To prevent the baby from becoming too addicted to nursing with
the shield, it should be removed as soon as the baby is latched-on
and nursing well.
iii. Possible problems associated with the use of nipples shields
include a drop in the mother's milk supply and insufficient
transfer of milk to the baby.
2) Surgical
a. Goals
i. restoration of an adequate projecting nipple together with an
areola
Lip Teh
ii. preservation of the lactiferous for a patient who may want to
breast-feed.
b. 2 main types
i. Ducts preserved (Grade I-II)
ii. Ducts sacrificed (Grade III)
1. Hartrampf and Schneider(1976) reported that the nipples
maintained normal sensation and erectile power
Surgical Methods
Create tightness at the neck of the inverted nipple.
1) Skin excision
Kehrer(1888), Deaver(1917)and Basch(1893) introduced methods of excising a ring of
areolar skin from around the nipple or subcutaneous myotomy of the areolar muscle.
However, these techniques are more applicable to a depressed nipple than to a truly
inverted nipple
Axford(1889) created a tight neck by excising three elliptical pieces of skin radially and
applying a purse-string suture around the nipple.
Grodsky(1937) introduced a method for creating four triangles of skin with the base on
the nipple margin and the apex toward the areola, followed by direct closure of the
defects to produce nipple projection.
DuFourmentel, (1950) expressing dissatisfaction with the techniques designed to
preserve the lactiferous ducts, introduced a technique for attaining aesthetic objectives
based on a V-Y technique that cuts all the fibrous bands but not the ducts.
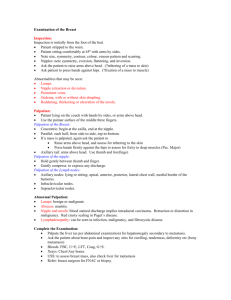
Namba technique (1966) involves the creation of a tight neck at the nipple base with
three simple half-Z-plasties without sacrificing the duct system or adding bulk to the
nipple to maintain nipple projection.( tighten the neck base and elongate the length of
the neck.)
Schematic diagram of the Namba technique. (Above, left) Preoperative design. The length of a-c is about 1
cm. The angle of acd is 30 to 45 degrees. (Above, center) Triangular flaps are elevated.
2) Purse String method
Lip Teh
Stark (1980) cut the areola to a depth of 1 cm around the nipple and placed two
horizontal mattress sutures from 6 to 12 o'clock and from 9 to 3 o'clock. This type of
suturing or a purse-string suture at the base may interfere not only with blood supply to
the nipple but also with lactation.
Peled 1999 Traction will indicate the need and success of release of the deep tissues. This is done with
the sharp edge of a regular injection needle, 18 gauge, introduced at 6 o'clock deeply at the base of the
nipple or with a microsurgical blade. By moving the needle horizontally in a fan-like movement while
pulling the traction suture, the breast ducts are divided and the skin is released. In cases of ill-defined or
missing nipples, there is no need for release. Through the same hole at 6 o'clock, a subcuticular, pursestring, 4-0 clear nylon suture is placed. The stitch takes small deep bites, exiting the skin at the marked line
every 5 to 6 mm, and entering through the same skin hole described for knifeless otoplasty. It progresses
around the entire circumference. At the completion of the subcutaneous, buried, purse-string suture, both
thread ends come out at 6 o'clock, the same hole originally entered. While pulling the traction suture, the
purse string is tied, creating the nipple mound . The knot buries spontaneously under the skin, and the hole
is left open for spontaneous healing. The wrinkling of the areolar skin at the base of the nipple improves
spontaneously in 3 weeks. Not suitable for nipple projection in scarred skin
3) Piercing (Scholten 2001)
With body jewellery
Nipple is brought out with a pair of forceps, and a holding suture of 2-0 Vicryl is used to further evert the
nipple. Gentle traction is applied until there is good projection. The nipple is pierced through the marking
points at its base with a 16-gauge Biovalve intravenous catheter needle. To achieve maximal nipple
projection, the first half of the nipple is pierced inward, whereas the second half is in a more outward
direction. The position of the needle is assessed without traction from the suture. Small adjustments at this
stage can be made if necessary. When a satisfactory position is achieved, body jewellery replaces the needle
and the polytetrafluoroethylene catheter is slowly withdrawn. I normally insert a so-called barbell, which is
a straight bar of stainless steel, tapped at both ends with balls that screw in place. For initial treatment, I
prefer to use high-quality stainless steel. However, when the piercing is completely healed, this device can
be replaced with other materials (e.g., polytetrafluoroethylene, titanium, gold, or silver). An everted nipple
with a projection of at least 9 to 10 mm could be achieved in all cases. Healing is generally complete within
2 weeks. In case of treatment in the later stages of pregnancy, the nipple will stay everted until suckling of
the newborn baby begins, at which time the body jewelry can be removed, although this is not strictly
necessary.
Should wear jewellery for at least 3 months. Recurrence rate likely to be high
Add bulk beneath the nipple
1) Elsahy (1976)
Two de-epithelialized triangular dermal flaps at 3 and 9 o'clock.
A curved circumferential incision is made around the nipple, so the pathologic fibrous
bands and lactiferous ducts are left undisturbed.
Lip Teh
Flaps wrapped around the nipple in a subcutaneous tunnel as a sling
2) Teimourian (1980)
Modification of above. Differences
a) The directions of the flaps were altered from 3 and 9 o'clock to 12 and 6 o'clock
to create less interference with the blood and nerve supply to the nipple
b) all the lactiferous ducts were cut
c) the dermal flaps were used as supportive bulk under the nipple rather than as a
sling.
Superior to Elsahy's procedure in that nipple projection is better achieved and the
recurrence rate is lower; but this technique excludes the possibility of future lactation
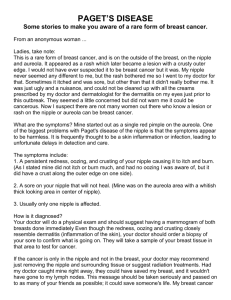
Schematic diagram of modified Teimourian technique. (Left and center) Preoperative design. The length of
a-b is 1.5 cm. The length of a-c is less than 1 cm. The length of a-d is about 1.5 cm (varies with size of
nipple). (Right) Cross-sectional view of operative method. Triangle flap a-b-d is de-epithelialized and
developed as composite flap. Dissection is continued below composite flap toward bundle of lactiferous
ducts. Shortened lactiferous ducts and associated fibrous structures are completely interrupted. Two
superior and inferior composite flaps are hinged toward dissected space and sutured together to provide
structural bulk. Points a and b are subdermally approximated to tighten nipple neck base.
4) intranipple strutting with bilateral deepithelialized dermal flaps (Lee 1998)
Lip Teh
The nipple proper is dissected free from the underlying attachment under loupe vision,
with splitting and stretching by sharp Metzenbaum dissection in the vertical plane so as
to minimize ductal injury with selective release of fibrous bands.
The deepithelialized skin flaps were positioned erect in intranipple slits, forming a strut.
The remaining proximal portion of the deepithelialized skin flaps are sutured together in
the subcutaneous tunnel.
The V-Y fashioned closure of the donor defect further accentuates nipple projection by
placing the flap base in a more centripetal direction.
Complications
1. infection
2. hematoma
3. nipple sensory change
4. loss of erectile function
5. loss of lactation
6. partial/total nipple necrosis
7. incomplete correction
8. partial/complete relapse(3-10%)
9. scarring
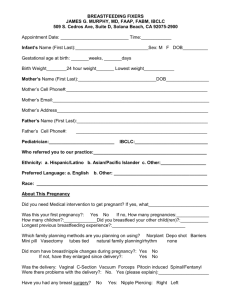
Diagram showing the most common pattern of blood supply.
Lip Teh
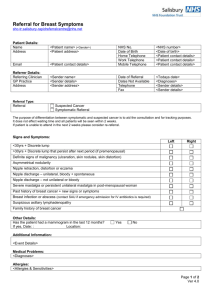
The operative technique in three grades. (Above) Grade I. The eversion of the nipple is maintained only by
purse-string suture. (Center) Grade II. The fibrosis (small x) is released, and a purse-string suture is added.
(Below) Grade III. Lactiferous ducts are cut, and the fibrosis is released. Triangular dermal flaps are turned
under the nipple and sutured together. A purse-string suture is added.
Lip Teh
 0
0