AuerFamily Homeopathy Adult Intake Form Name: Date of
advertisement

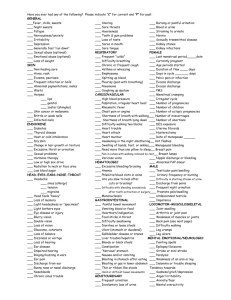
AuerFamily Homeopathy Adult Intake Form Name:__________________________________________ Date of Birth__________________ Home Address:_______________________________________________________________ City,State,Zip: ___________________________ Home Phone:__________________Cell Phone:_______________ Work Phone:____________ E-mail address:________________________________________________________________ Sex: M F Weight Height Marital status ___________________ Number of children ___________________ Employment status: Student Homemaker Disabled Retired Work full time Work part time Unemployed Other Usual Occupation: Employer:__________________________ Business/Work Address: _______________________________________________________ City, State, Zip: _______________________________________________________________ Referred by:_________________________________________________________________ Person to be contacted in case of emergency:______________________________________ Address:________________________________________ _________________________________________ Phone:_____________________ Hospitalizations -starting with the most recent (except normal pregnancies); include type of illness, month and year hospitalized, name of hospital, city and state: #1:________________________________________________________________________ #2:________________________________________________________________________ #3:________________________________________________________________________ Allergies:___________________________________________________________________ Please list any medications you are taking (Type, Dosage, Frequency):__________________ __________________________________________________________________________ __________________________________________________________________________ Medicinal Herbs, Vitamins, Teas:_________________________________________________ ___________________________________________________________________________ Do you use: Coffee: Amount __________ Cigarettes: Amount ________ Alcohol: Amount ________ Other drugs:_________ Amount ______ Tests Chest x-ray Electrocardiogram TB test GI series Kidney x-ray Barium Enema Other x-rays Year _____ _____ _____ _____ _____ _____ _____ Immunizations Year Tetanus Polio Typhoid Mumps, Measles Flu Other _____ _____ _____ _____ _____ _____ S Please check any of the following problems that have recently bothered you: frequent/severe headaches back pains neck lumps or swelling loss of balance dizzy spells blackouts/fainting wear glasses blurry vision eyesight worsening see double see halos or lights eye pains or itching watering eyes earaches hearing difficulties running ears noises in ears dental problems sore or bleeding gums sore tongue congested nose running nose sneezing spells head colds nose bleeds sore throat difficulty swallowing hoarse voice wheezing or gasping frequent coughing cough up phlegm cough up blood chest colds rapid or skipped heart beats chest pains shortness of breath swollen feet or ankles armpits or groin swelling difficulty sleeping motion sickness excessive sweating difficulty relaxing recurring indigestion frequent belching nausea vomiting pain in abdomen bloated abdomen constipation loose bowels black stools gray or whitish stools pain in rectum itching rectum blood with stools frequent urination involuntary urination burning on urination black or bloody urine weak urine stream difficulty starting urine constant urge to urinate aching muscles or joints swollen joints back or shoulder pains weakness in arms/legs painful feet trembling numbness leg cramps skin trouble scalp problems itching or burning skin bruise easily nervousness or anxiety nervous with strangers nail biting difficulty making decisions lack of concentration loss of memory lonely or depressed frequent crying hopeless outlook Comments or special problems: worry a lot scary dreams/thoughts feeling of desperation shy or sensitive dislike criticism angered easily annoyed by little things family problems problems at work sexual difficulties change of sexual energy considered suicide loss or gain in weight loss of appetite always hungry fatigue or weariness fever or chills motion sickness night sweats hot flashes warm or cold than others MALES ONLY burning or discharge swelling on testicles painful testicles FEMALES ONLY missed period menstrual problems bleeding between periods heavy bleeding bearing down feeling vaginal discharge genital irritation pain on intercourse swelling of breasts _____# of pregnancies _____# of births _____# of miscarriages _____#of premature births _____# of caesarian _____# of abortions ______________________________ __________________________________________________________ What are you most sensitive to (e.g. noise, odors, light, pain)? __________________ Describe an ideal day in terms of weather and temperature: ____________ What are your fears? ________________________ Do you have any hobbies? ____________ Favorite color? Least favorite color? Favorite book, movie or song? _____________________________________________________ (Women only) What symptoms do you experience premenstrually? __________________ Describe any recurrent dreams, important dreams in your life or recurrent themes in your dreams: How is your energy? Is there any particular time of day when it is lower or higher? ____________ How is your sexual interest/drive? ____________ What do you most like to eat or crave? __________________ What foods do you most dislike? How is your thirst? What temperature do you like fluids? ____________ ______ ____________ Are there any foods that you are sensitive to or allergic to?_______________________________ _______________________________________________________________________