Genus: Mycobacterium
advertisement

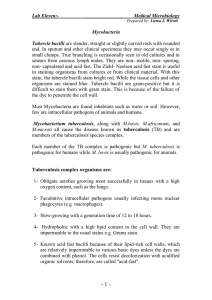
Page 1 of 3 Systematic Bacteriology Lec.(5) Genus: Mycobacterium Mycobacterium is slender, straight or slightly curved non motile rods non capsulated, none sporing and is aerobic bacilli. They don’t stain easily but once stain they resist decolorization with mineral acids. They are therefore referred to as acid fast bacilli (AFB). They are comprised obligate pathogens, opportunistic and saprophytes. Mycobacterium of clinical importance M. tuberculosis M. africanum M. bovis M. leprae M. ulcerance Habitat and mode of transmission M. bovis is found mainly as pathogenic in cattle human become infected by close contact with infected cattle M. tuberculosis is found in human transmitted to other person by inhaling cough droplets or dust particle contain tubercle bacilli and transmitted to animal that in close association with man also being reported. Pathogenicity: Tuberculosis: After inhaling infected droplets the tubercle bacilli become lodged in the lung forming small inflammatory lesion. Activated macrophage form granuloma around the site of primary infection which usually limits it (self- healing). Pulmonary Tuberculosis : This occurs when the primary infection does not heal completely and there is continued multiplication or reactivation of organism in the lung several months or years later due to poor health, malnutrition or defective immune response. An inflammatory reaction leads to a liquefied destruction of lung tissue (formation of a cavity). DR.YAGOUB HAMADT ALLAH 1 ALBAH UNIVERSITY Page 2 of 3 Systematic Bacteriology Lec.(5) Bacilli multiply in the wall of the cavity and can be found in the sputum (infectious stage) Patients with advanced infection have difficulty in breathing due to cavities in their lungs. Symptoms are include chronic cough, production of mucopurulent sputum which may contain blood in the late stages of the disease there is loss of weight, fever, night sweats, fatigue, chest pain and anemia later lung collapse. Tuberculosis meningitis: Occur more frequently in non-immune infants and young children as a complication of primary tuberculosis The condition is often fatal unless treated at an early stage Renal & urogenital Tuberculosis: Bone & joint Tuberculosis: Miliary Tuberculosis: Diagnosis: Caution: M. tuberculosis is a highly infectious pathogen (hazard group 3) we can safety cabinet Minimize the creation of aerosols Lab must be well ventilated Smear made by wooden stick which can be easily discarded and incinerated after use. Specimens: Sputum in screw-cap leak proof specimen container (must be sputum not a saliva), or urine and pus. Microscopy: By Ziehl Neelsen staining. Concentrating of AFB in sputum by centrifugation significantly increases the sensitivity of direct microscopy Fluorescence microscopy (fluoro-chrome stain) Culture: DR.YAGOUB HAMADT ALLAH 2 ALBAH UNIVERSITY Page 3 of 3 Systematic Bacteriology Lec.(5) Specimens such as sputum, urine and pus which are contain commensals require decontamination before being cultured (for routine purpose sodium hydroxide has been found to be an effective decontamination. M. tuberculosis will grow aerobically on a protein enriched media e.g Lowenstein – Jensen egg media (slow growing produce raised, dry cream colored colonies 2-3 weeks but culture should be incubated for up to 6 weeks before being discarded Identification based on Z N stain Rate of growth Temperature of growth Production of pigments Tuberculin test Mantoux test Antibiotics: Antibiotic effective for treatment of tuberculosis include isonizid, streptomycin, p-aminosalicylic acid and rifampcin Control: Adequate nutrition Well ventilated house General health education Immunoprophylaxis is achieved by BCG vaccination DR.YAGOUB HAMADT ALLAH 3 ALBAH UNIVERSITY