FACTORS ASSOCIATED WITH RECURRENT ANTERIOR CRUCIATE LIGAMENT
RUPTURES IN FEMALE INTERCOLLEGIATE SOCCER PLAYERS
A Thesis
Presented to the faculty of the Department of Kinesiology
California State University, Sacramento
Submitted in partial satisfaction of
the requirements for the degree of
MASTER OF SCIENCE
in
Kinesiology
(Movement Studies)
by
Elizabeth Ann Silva
SUMMER
2012
© 2012
Elizabeth Ann Silva
ALL RIGHTS RESERVED
ii
FACTORS ASSOCIATED WITH RECURRENT ANTERIOR CRUCIATE LIGAMENT
RUPTURES IN FEMALE INTERCOLLEGIATE SOCCER PLAYERS
A Thesis
by
Elizabeth Ann Silva
Approved by:
__________________________________, Committee Chair
Dr. David Mandeville
__________________________________, Second Reader
Heather Farwig
____________________________
Date
iii
Student: Elizabeth Ann Silva
I certify that this student has met the requirements for format contained in the University format
manual, and that this thesis is suitable for shelving in the Library and credit is to be awarded for
the thesis.
__________________________, Graduate Coordinator
Dr. Michael Wright
Department of Kinesiology
iv
___________________
Date
Abstract
of
FACTORS ASSOCIATED WITH RECURRENT ANTERIOR CRUCIATE LIGAMENT
RUPTURES IN FEMALE INTERCOLLEGIATE SOCCER PLAYERS
by
Elizabeth Ann Silva
Statement of Problem
Currently all information pertaining to recurrent Anterior Cruciate Ligament (ACL)
ruptures has been reported regarding the general female population. This study looked at
the female soccer intercollegiate population and factors associated with recurrent ACL
ruptures.
Sources of Data
Data for this study was attained using a non-validated survey using
Surveymonkey.com. This website was the most practical method for the type of
information being attained while allowing anonymity of all participants. The NATA
provided email directories of ATCs in the United States. This free directory was retrieved
once the survey request from was approved by the NATA Survey Dispersal and the
CSUS Human Subjects Committee. A contact list request form was found on the NATA
v
website. A disclaimer created by the NATA was attached to the survey to relinquish any
endorsement of the NATA.
Once all steps had been performed to allow for survey dispersal, 1000 female and
male ATCs were selected at random from the NATA contact list. The survey was
electronically sent to the subjects through the online survey methods.
Conclusions Reached
The purpose of this study was to determine the factors associated with the ACL
recurrence phenomenon. Both graft type and rehabilitation type were not found to be
associated with time to ACL recurrence. Autograft trended towards increased
survivorship as did traditional rehabilitation. Future studies are needed to determine the
optimal conditions of the initial ACL reconstruction and rehabilitation in order to avoid
recurrence for female intercollegiate soccer players.
_______________________, Committee Chair
Dr. David Mandeville
_______________________
Date
vi
DEDICATION
I would like to dedicate this thesis to my parents, Manuel and Alda Silva. They have
always believed in me and told me that anything was possible with a hard work. I am
thankful for their love and support through all these years of my educational journey.
vii
ACKNOWLEDGEMENTS
I would like to acknowledge my brother-in-law and sister Gilbert and Lucy Gutierrez
and my boyfriend Andrew Melo, who have always supported me through the good times and
bad. They listened to me complain and cry, but has always pushed me to keep going. I love
you always.
To Heather Farwig, my reader, my friend, my mentor, you motivate me to keep going
and to be a better person and better athletic trainer. I appreciate you helping me through this
process and for always believing in me. Thank you for always being there for me
educationally and personally.
Dr. Mandeville, thank you for sticking with me through this process. I know it took a
while and many revisions, but I finally finished. I really appreciate all that you have done.
Dr. Wright, thank you for always meeting with me to help me with scheduling and
finalizing my thesis. You have helped me in more ways than I can ever imagine.
viii
TABLE OF CONTENTS
Page
Dedication .............................................................................................................................. vii
Acknowledgments................................................................................................................. viii
List of Tables ........................................................................................................................... xi
List of Figures ........................................................................................................................ xii
Chapter
1. INTRODUCTION .............................................................................................................. 1
Statement of Purpose ................................................................................................... 2
Significance of the Study ............................................................................................ 2
Definition of Terms ..................................................................................................... 2
Delimitations................................................................................................................ 3
Limitations ................................................................................................................... 4
Assumptions................................................................................................................. 4
Hypotheses ................................................................................................................... 4
2. REVIEW OF LITERATURE ............................................................................................. 5
The Anterior Cruciate Ligament .................................................................................. 5
How the ACL is Injured................................................................................................ 6
Factors that Predispose an Increase in Prevalence in ACL Ruptures .......................... 6
Females Soccer Athletes at Risk for Composite Knee Injuries ................................... 8
Forces that Cause Composite Injures ........................................................................... 9
Surgery Options/Graft Selections ............................................................................... 10
Return to Play (RTP) ................................................................................................. 11
Rate of Recurrent ACL Ruptures ............................................................................... 12
Consequences of Recurrent ACL Rupture ................................................................. 13
Purpose....................................................................................................................... 15
3. METHODOLOGY ............................................................................................................ 16
Subjects ...................................................................................................................... 16
Procedures.................................................................................................................. 16
Data Acquisition ........................................................................................................ 17
ix
Data Analysis ............................................................................................................. 18
4. RESULTS ......................................................................................................................... 19
5. DISCUSSION .................................................................................................................... 22
ACL Graft Type ......................................................................................................... 22
Rehabilitation Type.................................................................................................... 23
Interpretation.............................................................................................................. 24
Limitations & Future Research .................................................................................. 25
Conclusion ................................................................................................................. 26
Appendix A. Survey: Demographics, First ACL Rupture, Second ACL Rupture ................ 28
Appendix B. Guidelines and Packet for NATA Survey Distribution .................................... 34
Appendix C. Contact Cover Letter for Survey ...................................................................... 41
References ............................................................................................................................... 43
x
LIST OF TABLES
Tables
1.
Page
Table 1 Contingency table of the association of ACL graft type and time to
ipsilateral ACL recurrence of four intercollegiate women soccer players ........... 20
2.
Table 2 Contingency table for the association of rehabilitation type and time to
ipsilateral ACL recurrence of four intercollegiate women soccer players ........... 21
xi
LIST OF FIGURES
Figures
1.
Page
Figure 1 The association of ACL graft type and time to ipsilateral ACL recurrence
of four intercollegiate women soccer players ....................................................... 20
2.
Figure 2 The association of rehabilitation type and time to ipsilateral ACL
recurrence of four intercollegiate women soccer players ..................................... 21
xii
1
CHAPTER 1
Introduction
Soccer is a well-known sport throughout the world. This sport, like many other
sports, suffers injuries. A prevalent injury among those athletes is injury to the anterior
cruciate ligament (ACL). Females have a four to six time’s higher ACL injury rate when
compared to their male counterparts while participating in soccer (Walden, Jagglund,
Werner & Ekstrand, 2010). Injury to the ACL in females has many different factors and
of those factors the most predominate, ones are anatomical and biomechanical.
Anatomical and biomechanical factors vary from a narrow intercondylar notch, Q-angle,
valgus force on the knee and ACL ligament size. Once the athlete suffers an ACL
rupture, they have to make a choice whether to continue to play or quit. Athletes that
continue to play at a high/competitive level typically decided to have surgery.
Once a patient has ACL surgery and they go through the rehabilitation phase of
recovery. Even with a successful rehabilitation, there is still a chance that they will rerupture their ACL. Some factors associated with this recurrence are ACL graft selection
and the type of rehabilitation the athlete goes through. A study performed by Wright,
Magnussen, Dunn and Spindler in 2011, showed that females have a two to six percent
chance that their ACL graft will have a recurrence of rupture. This statistic is in regards
to the general female population and not specific to intercollegiate female soccer players
that have a recurrence rate. At this time, there are no studies or statistics reported that are
in regards to the ACL recurrence rate of female intercollegiate soccer players.
2
Statement of Purpose
The purpose of this study was to assess factors associated with recurrent ACL
ruptures in female intercollegiate soccer players.
Significance of the Study
Most information regarding factors related to ACL recurrence has been reported in
regards to the general female population. This is due in part to the fact that factors
associated with recurrent ACL ruptures in female intercollegiate soccer players has not
been reported. The results of the survey created will help to determine these common
factors.
Definition of Terms
Allograft- a graft of tissue between individuals of the same species but of disparate
genotype (Dorland's illustrated medical, 1990).
Anterior Cruciate Ligament- a ligament in the knee that attaches to the anterior aspect of
the tibial plateau, restricting anterior movement of the tibia on the femur (France, 2011)
Autograft- a graft of tissue derived from another site in or on the body of the organism
receiving it (Dorland's illustrated medical, 1990).
Certified Athletic Trainer (ATC) – a professional who has attained a standard level of
competence in athletic training. The ATC is involved in the prevention, recognition, and
evaluation of injuries, and works closely with others in rehabilitation from injuries. They
have fulfilled the requirements for certification established by the National Athletic
Trainers’ Association Board of Certification, Inc. (NATABOC) (France, 2011)
Contralateral-On the other side (Prentice, 2011)
3
Intercondylar notch-situated between two condyles (Dorland's illustrated medical, 1990).
Ipsilateral- situated on the same side (Prentice, 2011)
Lateral Collateral Ligament- a ligament that attaches to the femur and he fibula;
maintains stability of the lateral aspect of the knee joint (France, 2011)
Medial Collateral Ligament- a flat longitudinal band found on the medial (inside) side of
the knee (France, 2011)
Posterior Cruciate Ligament- a ligament in the knee that attaches to the posterior aspect
of the tibial plateau, restricting posterior movement of the tibia on the femur (France,
2011)
Q-angle- is the relationship of the hip to the knee. A line from the superior iliac spine of
the hip to the mid patella forms this angle; then an imaginary line is drawn from the
middle patella to the tibial tubercle. The space between the two is known as the Q-angle
(Prentice, 2011)
Valgus- outward bending or twisting force (France, 2011)
Varus- inward bending or twisting force (France, 2011)
Delimitations
This study was delimitated to certified athletic trainers from all divisions of
women’s intercollegiate soccer. All subjects were Certified Athletic Trainers (ATC) from
all divisions of women’s intercollegiate soccer. All data acquired will be from female
intercollegiate soccer players that had a recurrent ACL from fall 2005 to spring 2012.
4
Limitations
This study was limited to ATC’s in the United States with colleges that have
intercollegiate women’s soccer programs. Only from female intercollegiate soccer,
players that have had a recurrent ACL rupture will be used for this study. The validity of
the testing instrument (non-standardized survey) and the limited answers provided for the
subjects also provided limitations to this study.
Assumptions
It was assumed that all participants would understand and answer honestly
questions stated in the survey used for this research. It was assumed that all participants
were ATC’s that had access to records pertaining information regarding female
intercollegiate soccer players that suffered two ACL ruptures and were familiar with the
survey engine .
Hypotheses
The following hypotheses were investigated:
1. It is predicted that there will be significant relationship between female
intercollegiate soccer players with a recurrent ACL rupture and accelerated
rehabilitation (H1).
2. It is predicted that there will be significant relationship between female
intercollegiate soccer players with a recurrent ACL rupture and graft selection
(H2).
5
CHAPTER 2
Review of Literature
The Anterior Cruciate Ligament (ACL) is a vital part of knee stability that is
located inside the knee within the intercondylar notch (Prentice, 2011). A highly active
athlete such as one that plays soccer needs their ACL to aid in the movements needed for
soccer such as cutting, pivoting and jumping. Soccer has a high risk to ACL injuries
relative to other sports (Alentorn-Geli, Myer, Silvers, Samitier, Romero, Lazaro-Haro &
Cugat, 2009).
Females have a four to six time’s higher ACL injury rate when compared to their
male counterparts (Walden, Jagglund, Werner & Ekstrand, 2010). Some of these factors
are due to anatomical and biomechanical factors. Looking at some of these anatomical
and biomechanical factors along with graft selection and type of rehabilitation (rehab)
will help to determine what factors lead to the phenomenon of recurrent ACL ruptures.
The Anterior Cruciate Ligament
The ACL is the most injured ligament in the body (Spindler & Wright, 2008).
Annually in the U.S., there are approximately 95,000 new ACL ruptures and about
60,000 to 75,000 surgical reconstructions of the ACL (Gammons & Schwarts, 2011).
Reconstructive surgery is recommended for individuals that are physically active.
The ACL stabilizes the knee during physical activity and is made up of three twisted
bands: the anteromedial (AM), intermediate and posterolateral (PL) bands (Prentice,
2011). These bands are interwoven together in the form of a braid for increased tensile
strength. Of these three bands, the AM and PL are the most noticeable bands. These
6
bands of the ACL prevent anterior translation of the tibia on the femur so that during
activities, the tibiofemoral joint is stabilized. The ACL restricts the tibia against
excessive internal rotation and serves as a secondary restraint for valgus and varus stress
in the presence of collateral ligament damage (Prentice, 2011). The ACL also works in
conjunction with the thigh muscles, specifically the hamstrings, to resist anterior sheer
force of the knee joint during physical activities. Without the ACL, a physically active
patient will complain of having the sensation of their knee “giving out” or feel unstable
which can potentially lead to other knee injuries.
How the ACL is Injured
A complete rupture of the ACL can occur by contact or non-contact mechanisms.
A contact mechanism occurs when either a player is struck by another player or object.
This can cause a valgus force or forced hyperextension. Hyperextension occurs when a
force great enough is delivered to the front of the knee, which translates the tibia
posteriorly and ruptures the ACL. A non-contact injury occurs without direct contact and
can be caused when the lower leg is rotated while the foot is fixed. This is typically
known as a plant and twist mechanism. Whether the rupture is contact or non-contact,
the patient will report hearing and/or feeling a “pop.” Of the two types of mechanisms of
injury, the majority of ACL ruptures are non-contact (The MARS Group, 2010).
Factors that Predispose an Increase in Prevalence in ACL Ruptures
Ninety percent of ACL tears in women and sixty percent in men occur via the
non-contact mechanism (Spindler & Wright, 2008). Although the non-contact
mechanism is extremely high in females, it is not known what causes the increased
7
prevalence. It has been reported that females have a two to three times higher ACL
injury risk compared to men (Walden, Jagglund, Werner, & Ekstrand, 2010). Studies
have shown that anatomical factors such as ligament size of the natural ACL and femoral
intercondylar notch relate to ACL rupture. Additionally postural, biomechanical,
strength and hormonal differences are thought to be risk factors for increased ACL
rupture in females (McDaniel, Rasche, Gaudet, & Jackson, 2010) (Foster, 2008)
(Prentice, 2011)
A narrow intercondylar notch may predispose females to ACL injury. The
positioning of the ACL within the notch, and a narrow notch width may cause increased
elongation of the ACL under high tension (Hewett, Myer & Ford, 2006). One potential
injury occurs when a forced rotation of the femur occurs on the fixed tibia. The forced
rotation causes a narrowing of the notch, which then impinges the ACL, possibly leading
to rupture of the ligament (Prentice, 2011). A narrower intercondylar notch may also
lead to a smaller, weaker ACL.
An additional anatomical factor related to increased ACL rupture for females is
the Q-angle. The Q-angle is a relationship of the hip to the knee. This angle is formed
by a line from the superior iliac spine of the hip to the mid patella; then an imaginary line
is drawn from the middle patella to the tibial tubercle. The space between the two is
known as the Q-angle. An excessive degree of Q-angle is thought to predispose females
to knee injuries. The normal Q-angle for males is ten degrees whereas females it is
fifteen degrees. Anything exceeding fifteen degrees is considered excessive and can lead
8
to an increase in ACL rupture (Prentice, 2011). This excessiveness in females is due to
the increased hip width that aids in childbirth.
Other risk factors for the increased prevalence of ACL rupture in females are
biomechanical differences. In females more so than males, a valgus force is placed on
the knee during jump landing. This causes an increase in the valgus angle and can lead to
increased probability for ACL injuries (Foster, 2008). ACL ligament size in females is
typically smaller, thus the increased biomechanical loads during jump landing increase
the likelihood of rupturing the ACL (Foster, 2008). All of these factors combined, can
lead to the increased stress placed on the ACL in physically active females, which may
lead to increased prevalence of ACL ruptures during sports such as soccer.
Female Soccer Athletes at Risk for Composite Knee Injuries
Females in jumping, cutting, pivoting sports have a four to six times higher ACL
injury compared to male counterparts (Walden, Jagglund, Werner & Ekstrand, 2010).
Many of these movements are combined in the game of soccer. These movements vary
from running, sprinting, jogging, pivoting, shifting, twisting and cutting. In isolation,
many of these movements do not cause injury to the ACL, but a combination of these
movements may lead to the non-contact mechanism of rupture. However, it is unknown
which movements or which position in soccer has an increase in ACL rupture prevalence.
It is known that the combinations of movement in soccer cause forces sufficient to cause
ACL rupture in females.
During soccer, the contact or non-contact mechanism of injury rarely ruptures the
ACL in isolation. Typically, an ACL injury is associated with other ligaments, cartilage
9
or bones being injured as well. A strong valgus force along with the rotation of the femur
on the tibia causes the medial aspect of the knee to be loaded with enough force to tear
the ACL, MCL and medial meniscus. This is known as the unhappy triad. When there is
enough valgus force, the MCL is also injured due to the attachment of the MCL to the
medial meniscus (Prentice, 2011). The ligament injured in association with the ACL is
usually the medial meniscus. This is due to the loading of the femur into the tibia. This
load causes the femoral notch to tear the ACL and “pinch” the medial meniscus between
the femur and the tibia.
Forces that Cause Composite Injuries
The mechanism of ACL injury is associated with certain types of forces that can
cause other injuries to the knee. Of the forces applied to the knee, there are four that can
cause injury to other ligaments of the knee. A valgus force alone can lead to injury of the
MCL; a varus force causes injury to the LCL; a force from the anterior (front) aspect of
the knee can cause injury to the ACL; and a force from the posterior (back) aspect of the
knee can cause a PCL injury along with an ACL injury (Prentice, 2011) These forces can
lead to three different degrees of injury to the ligaments. These degrees range from a
grade one to a grade three-ligament sprain. A grade three-ligament sprain is when the
ligament is completely ruptured. These forces may also lead to damage of other
components of the knee, primarily the menisci. Menisci injuries can occur with a plant
and twist mechanism or a valgus force. A plant and twist mechanism loads the medial
aspect of the knee therefore forcing the femoral condyle to press on the medial meniscus
and tearing part of it; or varus force great enough to cause not only the LCL to rupture
10
but also causing the medial femoral condyle to open up and potentially stress the medial
meniscus to tear. Once these injuries occur, the next step is to decide whether or not to
continue to live life with the injury or have surgery to repair the damage. Those that
decide to have surgery are physically active and those that do not live a sedentary life.
Surgery Options/Graft Selections
Some athletes can opt to not have surgery after a ruptured ACL and can try to
rehabilitate their leg. If their muscles are strong enough they may be able to be an active
athlete without having their ACL. As long as they do not have the sensation of instability
then they can continue with activity. However, orthopedic surgeons recommend that
athletes elect surgical reconstruction of the ACL in order to return to their high level of
activity. This is due to the fact that if a high-level athlete continues to perform without an
ACL, they predispose themselves to possibly injure other joint structures, ligaments or
muscles.
Once the athlete has decided to have their ACL repaired, there are different
options for ACL surgery. The two main types of surgeries performed to repair the ACL
are an autograft and an allograft. An autograft is tissue from the athlete themselves to
make a graft ACL and an allograft is tissue from a deceased person that donates their
body to science. The types of autografts used are bone patellar tendon bone (BPTP)
which is where the surgeon takes a piece of the athletes’ patellar tendon with bone plugs
on either end or a hamstring graft of the semitendinosus and gracilis muscle. One study
showed that bone-patellar tendon-bone for young person’s is the best graft selection and
semitendinosus and gracilis for older subjects, women and those devoted to recreational
11
sport (Garofalo, Moretti, Kombot, Moretti, & Mouhsine, 2007). The types of allografts
typically used are an achilles tendon of the ankle or posterior tibialis tendon of the ankle.
These grafts are frozen and placed in a cadaver bank until they are ready to be used.
Once ready to be used they are sized and fitted for the athlete. ACL graft selection is
determined by surgeon preference (Battaglia, Cordasco, Hannafin, Rodeo, O’Brien,
Altchek, Cavanaugh, Wickiewicz & Warren, 2007). Once surgery has been performed,
the athlete then goes through the process of rehabilitation and determining a return to
play.
Return to Play (RTP)
Recovery time of a typical ACL only reconstruction has been reported to take
between eight to twelve months (Holgum, 2005). This time frame depends upon the type
of rehabilitation. The athlete either goes through an accelerated or traditional
rehabilitation. Accelerated rehabilitation is defined as returning to full activity between
four to six months (Holgum, 2005). This type of rehabilitation can be used for those in
that participate in competitive and/or serious recreational sports. When an athlete
participates in an accelerated program, they usually begin early weight bearing. It is
believed that there are few complications from the surgery with early weight bearing.
Traditional rehabilitation is known as returning to full activity between eight to twelve
months (Holgum, 2005). This type of rehabilitation is a delayed program with the same
progressions but at a slower rate. Jogging progression to straight running is not permitted
until approximately six months whereas in an accelerated program would begin running
12
around the four month mark. During the eight to twelfth month is when the athlete will
return to full sport (Holgum, 2005).
Whether the athlete goes through an accelerated or a traditional rehabilitation,
currently there are no universal RTP criteria. To determine if the athlete is able to RTP,
the only assessments used are freedom of pain, normal strength and sport specific
exercises (Hetzler, Luke, Bushman, & Hetzler, 2009). These measurements are all
determined by each specific athlete. Even after the athlete has returned to normal
sporting activity, there is still a chance that they may re-injure their knee.
Rate of Recurrent ACL Ruptures
Females have a two to six percent chance of ACL graft rupture recurrence after
less than five years from the initial reconstruction even in successful rehabilitation
traditional or accelerated (Wright, Magnussen, Dunn & Spindler, 2011). Whether the
recurrence of the ACL rupture occurs on the contralateral (opposite) leg vs. the ipsilateral
(same) leg is approximately three percent (Wright, Magnussen, Dunn, & Spindler, 2011).
Previous reports indicate several reasons for graft failure including technical,
biological or a combination of both (The MARS Group, 2010). Technical failure refers
to as surgical error. This is can occur when the tunnel placement is to anterior/posterior
in the femur or tibia. Biological failure was defined as “lack of incorporation of the graft
as evidence by early failure without a significant traumatic episode or obvious significant
technical problems with the previous reconstruction” (The MARS Group, 2010). The
athlete will begin to function and go through rehabilitation, but over a period of time the
13
knee will feel loose or unstable. The most accurate test to perform in order to determine
a biological failure is the Lachman’s (Lam, 2011).
Another potential reason for failure can be due to decreased sensation of pain. A
decreased sensation of pain can lead to the accelerated progression of rehabilitation even
though the graft is not at its full strength. This fast progression could cause the graft to
rupture. The likelihood of this can be due to the use of an allograft instead of an
autograft. In using an allograft athletes often do not have as much pain because the tissue
is not from their own body. Common graft failure occurs in an allograft due to early pain
free exercises. Because the allograft is a foreign body in the athlete, the nociceptors are
diminished which allows the athlete to push forward with exercises. They will not feel
the normal amount sensory pain since it does take time for the body to take the allograft
to mold and adapt it to their new ACL graft. The bone plugs themselves will take a full
year to heal and the ACL graft is at its most vulnerable state in the first couple of months
after surgery.
Consequences of Recurrent ACL Rupture
The effect of the recurrent ACL rupture can negatively impact the career of the
female athlete. Due to recurrence of an ACL injury, some females are forced to quit
playing soccer. Some reasons forcing the athlete to quite are going through multiple
surgeries, increased cost of having multiple surgeries along with rehabilitation after both
repairs are made. The athlete may decide to have the ACL repaired both times but might
still suffer pain and cannot continue to compete at the level of competition that is needed.
For an athlete competing at the intercollegiate level this not only causes physical stress
14
but also mental stress. They have to think not only for the current situation but their
future.
Another factor impacting the female athlete’s career is the cost of surgical
reconstruction of not only the initial rupture but the second one as well. Along with the
surgery comes the cost of rehabilitation for the initial a secondary injury. The mean total
cost was for a surgical repair of an allograft ACL reconstruction is $5,465 and $4,872 for
autograft ACL reconstruction. An allograft ACL reconstruction was more costly than
autograft ACL reconstruction in the outpatient setting (Nagda, Altobelli, Bowdry,
Brewster & Lombardo, 2010). Some complications may occur after the secondary
rupture that leads to a more extensive surgery, which in turn leads to an increased cost of
the surgical approach along with extended rehabilitation.
The consequences may seem small initially when the female athlete contemplates
quitting playing soccer; however their knee function may be compromised in the future.
Multiple injuries and surgeries can lead to knee osteoarthritis (OA) and has an early
increased probability after ACL reconstruction. It is estimated that OA develops in fifty
percent of patients with ACL tears ten to twenty years after the injury (Spindler &
Wright, 2008). This can lead to a debilitating joint pain and thus decreases the quality of
life and eventually can then lead to a total knee replacement (TKR). What most people
do not know is that a TKR is not covered by insurance companies until the patient
reaches fifty years of age.
15
Purpose
Most information regarding the factors related to ACL recurrence has been
reported with reference to the general female population. The factors associated with
recurrence in female intercollegiate soccer players have not been previously reported.
Specifically the association of graft selection and accelerated rehabilitation factors remain
unknown. Therefore the purpose of this study is to assess factors associated with
recurrent ACL ruptures in female intercollegiate soccer players. It is predicted that
accelerated rehabilitation will be strongly correlated with recurring ACL ruptures and
additionally, it is thought that graft selection will be correlated with recurrent ACL
ruptures.
16
CHAPTER 3
Methodology
This study was designed to determine the factors that are associated with the
phenomenon of recurring ACL ruptures in female collegiate soccer players. It is hoped
that this information will help future athletes avoid recurrent ACL ruptures.
Subjects
The subject sample is comprised of Certified Athletic Trainers (ATC), who will
provide information regarding female intercollegiate soccer players with recurrent ACL
ruptures in their care. Those that will be included are ATC from NCAA division I, II &
III, NAIA and junior colleges of women’s collegiate soccer. Those that were excluded
are colleges that do not have a women’s collegiate soccer program.
Procedures
A non-validated questionnaire created by the researcher (see Appendix A) was
used to gather data. The validity and reliability of this survey has not been established
but this type of survey has been previously used and is the most appropriate method to
acquire this type of ACL re-injury data. The survey was created so as to minimize the
responses and elicited data pertaining to recurrent ACL injuries in the female collegiate
soccer players. The survey was sent to the National Athletic Trainer’s Association
(NATA) secretary for distribution. The ATC subjects completed the self-reported
multiple-choice questionnaire after accepting the informed consent that at the beginning
of the survey which has been reviewed and approved by the California State University,
Sacramento Internal Review Board (IRB).
17
A 19 questionnaire was created and disbursed with four sections of questions.
The first section of the survey addressed background information of the ATC regarding
the level of women’s soccer which they work at and if they have access to the
information needed for the survey. The second section of the survey regards information
concerning the athlete’s first ACL rupture. Questions begin with the athlete’s
demographics such as age, height and weight and then questions such as their mechanism
of injury (MOI), and all information regarding their initial ACL rupture. The third
section of the survey is designed to acquire information regarding the second ACL
rupture.
Data Acquisition
The survey was created using Surveymonkey.com. This website was the most
practical method for the type of information being attained while allowing anonymity of
all participants. The NATA provided email directories of ATCs in the United States.
This free directory was retrieved once the survey request from was approved by the
NATA Survey Dispersal (see Appendix B) and the CSUS Human Subjects Committee. A
contact list request form was found on the NATA website. A disclaimer created by the
NATA was attached to the survey to relinquish any endorsement of the NATA (see
Appendix B).
Once all steps had been performed to allow for survey dispersal, 1000 female and
male ATCs were selected at random from the NATA contact list. The survey was
electronically sent to the subjects through the online survey methods. The timeline for
this survey was dispersal on March 28, 2012 with final collection in April 14, 2012. If
18
there were not enough participants, then a follow up e-mail would be sent to the
participants not having completed the survey. After this e-mail is sent, then the survey
would remain open until April 20, 2012.
Data Analysis
Correlation analysis will be used to analyze the relationships between graft
rupture factors and ACL recurrence using Chi Square (p<0.05, SPSS Chicago, IL).
19
CHAPTER 4
Results
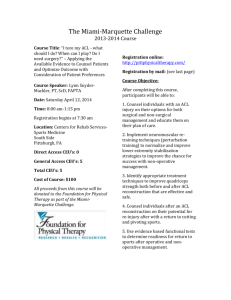
The response rate of this study was 19.7%, with one hundred and ninety seven
surveys answered. Of those, twenty responded having had an ACL recurrence. Of those
twenty, sixteen reported contralateral ACL rupture (80%) and four reported ipsilateral
ACL recurrence (20%). As this study aimed to assess the factors associated with
recurrent ACL ruptures, only the ipsilateral respondents were assessed. Thus four
subjects were used to evaluate associations between ACL graft type to time of recurrence
and rehabilitation type to time of recurrence. The responses were grouped into three
variables, ACL graft type, rehabilitation type, and time to recurrence. The ACL graft
variable was categorized as: autograft (category 1, bone-patellar tendon-bone and
hamstring,) and allograft (category 2, cadaver connective tissue). The second variable
was rehabilitation type: traditional rehabilitation (category 1, 8-12 months), and
accelerated rehabilitation (category 2, 4-6 months). The third variable, time to recurrence
was categorized as being: date of initial rupture to date of recurrence less than 12 months
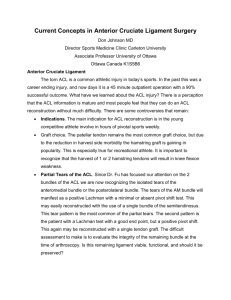
(category 1), or greater than 12 months (category 2). The results indicated that the
predominate graft type was autograft (n = 3) and rehabilitation type was traditional
rehabilitation (n = 3, Tables 1 & 2, Figures 1 & 2). Associations between the variables
were assessed using a Chi Square (x2, p < 0.05). For this test at p = .05, the critical value
for significance was x2 = 3.841. The association between graft type and time to
recurrence was found to be not significant (x2 = 0.53). The association between
rehabilitation type and time to recurrence was found to be not significant (x2 = 0.53).
20
Table 1. Contingency table of the association of ACL graft type and time to ipsilateral
ACL recurrence of four intercollegiate women soccer players.
a
b
Graft
Time to
type
recurrence
Category 1a
3
2
Category 2b
1
2
Totals
4
4
Category 1 = Autograft; Category 2 = Allograft
Category 1 = less than 1 year; Category 2 = greater than 1 year
x2= 0.53, non-significant
x2= 0.53, non-significant
Figure 1. The association of ACL graft type and time to ipsilateral ACL recurrence of
four intercollegiate women soccer players.
21
Table 2. Contingency table for the association of rehabilitation type and time to
ipsilateral ACL recurrence of four intercollegiate women soccer players.
Rehabilitation
Time to
type
recurrence
Category 1a
3
2
Category 2b
1
2
Totals
4
4
a
Category 1 = Traditional Rehabilitation; Category 2 = Accelerated Rehabilitation
b
Category 1 = less than 1 year; Category 2 = greater than 1 year
x2= 0.53, non-significant
x2= 0.53, non-significant
Figure 2. The association of rehabilitation type and time to ipsilateral ACL recurrence of
four intercollegiate women soccer players.
22
CHAPTER 5
Discussion
Most information pertaining to the factors related to ACL recurrence for non-athletic
female population has been reported with reference to the general male population.
Researchers do suggest that future studies should focus on factors related to ACL
recurrence within the female population (Foster, 2008). Currently, these factors have not
been reported for female intercollegiate soccer players. This area of study needs to be
researched due to the fact that females involved in cutting, jumping and pivoting sports
have a four to six times higher ACL injury rate compared to their males counterparts
(Walden, Jagglund, Werner, & Ekstrand, 2010). The purpose of this study was to
determine if the type of rehabilitation and the type of ACL graft were associated with
time to ACL recurrence. It was predicted that there would be a significant relationship
between accelerated rehabilitation and time to ACL recurrence for female intercollegiate
soccer players (H1). Additionally, a significant relationship was predicted between graft
type and time to ACL recurrence for female intercollegiate soccer players (H2).
Information gained from this study could be used to influence female intercollegiate
soccer players along with other sports medicine professionals in their selection of graft
and rehabilitation type in order to avoid ACL recurrence.
ACL Graft Type
The American Board of Orthopaedic Surgery lists ACL reconstructions as the
sixth most common procedure performed (Nagda, Altobelli, Bowdry, Brewster, &
Lombardo, 2010). Prior to these surgeries, the surgeon has the choice in determining the
23
type of ACL graft used (Battaglia, Cordasco, Hannafin, Rodeo, O’Brien, Altchek,
Cavanaugh & Wickiewicz, 2007). The graft type associated with increased survivorship
for ACL reconstruction continues to be an area of debate (The MARS Group, 2010). The
two types of ACL grafts primarily used for reconstruction are allograft (cadaver) and
autograft (hamstring tendon and bone-patellar tendon-bone). After the reconstruction is
performed, the ACL graft has to incorporate into the body allowing for full function of
the athlete. A study performed by Kaeding et. al., (2010) showed that allograft rupture
rates were higher than autograft ruptures in patients 10 to 19 years of age. Thus, the type
of ACL graft used may influence ACL recurrence rates; therefore this variable was used
in this study.
Rehabilitation Type
There is no universally utilized return to play (RTP) criteria for individuals
returning from ACL reconstruction (Hetzler, Luke, Bushman & Hetzler, 2009). The most
common measurements used for RTP are: freedom of pain, range of motion, normal
strength, proprioception and sports specific functionality (Hetzler, Luke, Bushman, &
Hetzler, 2009). These attributes are measured while the athlete transitions through their
respective physical therapy program. The two types of physical therapy programs are
traditional rehabilitation (returning to sport within eight to twelve months) and
accelerated rehabilitation (returning to sport within four to six months). Athletes
participating in traditional rehabilitation begin running at a later time period
(approximately month six) compared to those that are participating in accelerated
rehabilitation (approximately month four, Holgum, 2005). Often, athletes that participate
24
in intercollegiate sports participate in the accelerated rehabilitation program. It may be
likely that in athletes returning to play too soon, the ACL graft has not had the time to
incorporate into the body, which can cause graft failure. However, it is unknown if
rehabilitation type influences ACL recurrence rates.
Interpretation
Graft type was not found to be associated with time to ACL recurrence. Of the
two types of ACL grafts in this study, autograft was the predominate graft of the four
subjects (n = 3). This finding was unexpected as autograft incurs secondary surgical
trauma at the graft site. Despite this fact, surgeons chose autografts for these athletes
possibly due to the higher survival rate when compared to allograft. In this study one
subject with an autograft suffered ACL recurrence within a year which was similar to the
one subject with an allograft. The remaining two autograft subjects had recurrence
greater than one year. Based on these findings autograft appears to have increased
survivorship. Future studies are needed to substantiate these findings.
Rehabilitation type was not found to be associated with time to ACL recurrence.
Interestingly, of the two rehabilitation types studied, traditional rehabilitation was the
predominate type of the four subjects (n = 3). This was unexpected because it was
thought that athletes at the intercollegiate level would go through an accelerated
rehabilitation program in order to compete for their position on the team. The choice of
rehabilitation program that the athlete goes through is the surgeon’s, in consultation with
either the physical therapist or ATC. It may be that surgeon’s choice the conservative
rehabilitation type in order to increase graft survivorship. However, the one subject with
25
accelerated rehabilitation experienced an ACL recurrence within a year, as did one
subject with traditional rehabilitation. The remaining two subjects that went through
traditional rehabilitation had an ACL recurrence greater than one year. Although these
findings are inconclusive, traditional rehabilitation appears to have increased ACL
survivorship.
Limitations & Future Research
This study was limited to ATC’s in the United States with colleges and
universities that had intercollegiate women’s soccer programs. Only data pertaining to
female intercollegiate soccer players that have had a recurrent ipsilateral ACL rupture
were used in this study. These specific parameters may have limited the sample size. It
is likely that the limited sample size was not sufficient to power the study to avoid type II
error. Although the findings of this study are limited by a small sample, this area requires
additional research involving increased sample sizes. as studies have shown that fifty
percent of ACL injuries occur to individuals between the ages of 15-25 (Lam, 2011).
Of the survey data collected, sixteen ATC respondents had information pertaining
to female intercollegiate soccer players that had a second ACL rupture of the
contralateral knee. Future research could be expanded to include these female athletes
having suffered a second ACL rupture. If this direction is taken, then rehabilitation type
on the involved side would have to be linked to the contralateral rupture. It is more likely
that anatomical and biomechanical factors would influence a contralateral rupture.
Additionally, because females in cutting, jumping and pivoting sports have a four to six
times higher ACL injury rate compared to their male counterparts, future studies could be
26
broadened to involve other female sports that use these movements (Walden, Jagglund,
Werner, & Ekstrand, 2010).
Conclusion
The purpose of this study was to determine the factors associated with the ACL
recurrence phenomenon. Both graft type and rehabilitation type were not found to be
associated with time to ACL recurrence. Autograft trended towards increased
survivorship as did traditional rehabilitation. Future studies are needed to determine the
optimal conditions of the initial ACL reconstruction and rehabilitation in order to avoid
recurrence for female intercollegiate soccer players.
27
APPENDICES
28
APPENDIX A
Survey: Demographics, First ACL Rupture, Second ACL Rupture
29
Survey Questions
1. Do you have access to medical records from Fall 2009-Spring 2011 regarding
female intercollegiate soccer players?
Yes
No
2. Which level of college do you work at?
Division I
Division II
Division III
NAIA
Junior College
3. How many recurrent ACL ruptures did you have within the women’s soccer team
from Fall 2005-Spring 2011?
4. What was the date of the first rupture?
Athlete A_________
C___________
Athlete B___________
Athlete
Athlete D___________
F___________
Athlete E ___________
Athlete
5. What were the height, weight & age of each athlete?
Athlete A__________
C___________
Athlete B____________
Athlete
Athlete D__________
F___________
Athlete E____________
Athlete
6. What was the mechanism of injury of the initial rupture? (Contact vs Noncontact)
Contact: Struck by another player or object
Non-contact: Self injured
Athlete A__________
C___________
Athlete B___________
Athlete
Athlete D__________
F___________
Athlete E___________
Athlete
30
7. What did the initial rupture consist of (Check all that apply)?
Athlete A
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete B
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete C
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete F
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete E
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete D
____Lateral Meniscus Tear
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
____Lateral Meniscus Tear
8. Was the athlete on her menses during the initial rupture? (Yes, No, Unknown)
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E___________
Athlete F__________
9. What type of surgical approach was used for the first ACL reconstruction?
(Bone-patellar tendon-bone, Cadaver allograft, Hamstring tendon)
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E___________
Athlete F__________
31
10. What type of rehabilitation did the athlete go through? (Traditional or
Accelerated)
Traditional: returning between 8-9 months
Accelerated: returning 4-6 months
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E___________
Athlete F__________
11. Was the athlete wearing a functional brace after her first reconstruction when she
re-injured her ACL? (Yes, No, Unknown)
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E___________
Athlete F__________
12. Was the second rupture ipsilateral or contralateral?
Athlete A__________
C___________
Athlete B___________
Athlete
Athlete D__________
E___________
Athlete D___________
Athlete
13. What was the date of the second rupture?
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E ___________
Athlete F__________
14. What were the height, weight & age of each athlete?
Athlete A__________
C___________
Athlete B____________
Athlete
Athlete D__________
F___________
Athlete E____________
Athlete
15. What was the mechanism of injury of the second rupture? (Contact v Noncontact)
Athlete A__________
Athlete B___________
Athlete C__________
32
Athlete D__________
Athlete E___________
Athlete F__________
16. What did the second rupture consist of (Check all that apply)?
Athlete A
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete B
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete C
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete F
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete E
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
Athlete D
____Lateral Meniscus Tear
____Lateral Meniscus Tear
____ACL tear ____PCL tear ____MCL tear ____LCL tear
____Medial Meniscus Tear
____Lateral Meniscus Tear
17. What type was used for the second ACL reconstruction?
(Bone-patellar tendon-bone, Cadaver allograft, Hamstring tendon)
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E___________
Athlete F__________
18. Was the athlete on her menses during the second rupture? (Yes, No, Unknown)
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E___________
Athlete F__________
33
19. What position did the athlete play? (Forward, Midfield, Defense, Goal keeper)
Athlete A__________
Athlete B___________
Athlete C__________
Athlete D__________
Athlete E___________
Athlete F__________
34
APPENDIX B
Guidelines and Packet for NATA Survey Distribution
35
NATA
NATA guidelines regarding lists for members conducting surveys
NATA certified members requesting lists for research purposes will be referred to their
district secretary for approval of their project. NATA will provide address lists or
email lists for approved research projects by certified members at the lowest rate (9
cents/name) – prepayment and a signed one-time use agreement required. There is
no limit to the number of contact names a certified member can request for his/her
project. NATA does not offer an email broadcast service for certified members’
research broadcasts.
Student members sending up to 1,000 surveys can be done via email: A broadcast to a
maximum of 1,000 email addresses can be provided for student members conducting
research projects. NATA has the ability to provide a random sample of the population, if
it exceeds 1,000. NATA will transmit the cover letter (containing a link to the member's
questionnaire) via email to recipients. The transmission will be labeled as coming from
the researcher. If a follow-up reminder is desired, NATA will transmit a second letter to
the same members selected for the original broadcast.
Student member surveys of more than 1,000 will be conducted via U.S. mail: Since
email lists are not available in quantities above 1,000, member research that requires a
population greater than 1,000 is handled in the following manner. NATA can provide
name and address of the population desired so the member can send the hard copy
surveys via U.S. mail. The member must sign an agreement indicating the data will be
used only one time and only for the stated purpose. NATA will forward the data
electronically to the member, who can then print the labels for the mailing. If a follow-up
reminder is desired, the member must once again sign a “one time use” agreement for the
second mailing.
Disclaimer: The NATA Board of Directors has implemented this policy in regards to
student surveys: Graduate Student Surveys: When a graduate student asks the national
office for a mailing or email list to send a survey, s/he is referred to the relevant district
secretary. If the survey meets the District Secretaries/Treasurers Committee’s
requirements, the graduate student is given approval to receive a free list. The board was
concerned the recipients may think the surveys are NATA-sponsored. The board asked
that the graduate students be required to print a disclaimer at the beginning of the
questionnaire to alleviate this confusion. This wording was subsequently developed:
“This student 75 survey is not approved or endorsed by NATA. It is being sent to you
because of NATA’s commitment to athletic training education and research.” (6/13/02)
36
NOTE: THIS POLICY IS SUBJECT TO CHANGE WITHOUT NOTICE.
Only NATA student members may access this service.
37
Guidelines
Process:
For student members, NATA will broadcast email student surveys to a maximum of
1,000 participants. If a follow-up reminder is desired, NATA will transmit a second letter
to the same members selected for the original broadcast.
For professional members, NATA will provide address or email lists at the lowest rate
(9¢/ name). Prepayment and a signed one-time use agreement are required in addition to
the documents below. There is no limit to the number of contact names a professional
member can request for a project. NATA does not offer an email broadcast service for
professional members.
Disclaimer:
The following disclaimer is required:
“This student survey is not approved or endorsed by NATA. It is being sent to you
because of NATA’s commitment to athletic training education and research.”
Requirements:
1.
Completed application form (next page).
2.
Institutional Review Board approval - upload as part of form.
3.
Informed Consent form, if applicable - upload as part of form.
4.
Word (.doc) version of survey invitation email to participants - upload as part of
form. See Sample Cover-Letter for more information.
5.
Description / criteria identifying targeted survey participants - see 'ResearchSurvey-Criteria' document for more information.
38
Survey List Request Form
Purpose of Mailing List (check all that apply):
_ Email Survey
-Email broadcast service by National Office (max. 1000 recipients available to
student members only)
_ Is follow up Email Survey required?
_ Survey (for non students)
_ email addresses
_ postal addresses
File format:
_ Comma Delimited Text
_ Excel
Work Settings:
_College/University
_Secondary School
_Clinic
_Hospital
_Professional Sports
_Industrial/Occupational/Corporate
_Business/Sales/Marketing
_Heatlh/Fitness/Sports Clubs/
_Performance Enhancement Clinics
_Amateur/Recreational/Youth Sports
_Military/Law Enforcement/Government
_Independent Contractor
_Other
_Unemployed
_ All Member Types
_ Certified
_ Associate
_ Retired Certified
_ Certified Students
_ Non-certified Students
_ International Non-Certified
_ Certified International
To select by geographical area, please select one:
_ US only
_ All Districts
39
_ All members (Canada & International included)
To make a selection by State or District, check/circle below:
Districts
States
_1
CT, ME, MA, NH, RI, VT
_2
DE, NJ, NY, PA
_3
DC, MD, NC, SC, VA, WV
_4
IL, IN, MI, MN, OH, WI
_5
IA, KS, MO, NE, ND, OK, SD
_6
AR, TX
_7
AZ, CO, NM, UT, WY
_8
CA, NV, HI, Guam
_9
AL, FL, GA, KY, LA, MS, TN
_ 10
AK, ID, MT, OR, WA
SURVEY LIST USE AGREEMENT
I certify that the requested NATA survey list will be utilized only for the study specified
above. The list will not be duplicated, copied, or reproduced in any manner, but used one
time only.
I agree that any broadcast email will not contain other recipients’ email addresses in the
“To:” or “Cc:” field, since the email addresses provided are not to be shared among the
recipients.
To send a broadcast email from Microsoft Word, we have provided instructions in the
members-only section of the NATA Website. Go to:
https://cf.nata.org/members1/documents/mass_email_instructions_for_nata.pdf.
Members agree to abide by policies and procedures of the NATA. Failure to abide by
these requirements is a violation of such policies and may subject the user to sanctions by
the NATA Ethics Committee.
Applicant Signature________________________ Date ____________________
40
SAMPLE Contact Cover Letter for student surveys
Dear Fellow Certified Athletic Trainer:
I am a master’s degree candidate at (University Name), requesting your help to complete
part of my degree requirements. Please follow the link at the end of this letter to an online
survey titled: (Title of Project).
This student survey is not approved or endorsed by NATA. It is being sent to you
because of NATA’s commitment to athletic training education and research.
The questionnaire consists of __ demographic questions and __ Likert Scale (1-very
uncomfortable to 5 very comfortable) questions, which will take about five to seven minutes
to complete.
One thousand randomly selected certified NATA members in (Location Demographic) with
a listed email address are being asked to submit this questionnaire, but you have the right to
choose not to participate. The (University Name) Institutional Review Board has approved
this study for the Protection of Human Subjects.
This is a completely anonymous questionnaire and upon submission, neither your name nor
email address will be attached to your answers. Your information will be kept strictly
confidential.
As a fellow certified athletic trainer, your knowledge and opinions regarding this topic makes
your input invaluable. Please take a few minutes to fill out the anonymous questionnaire you
will find by clicking on this link and submit it by (Date):
(http:/__________________________________ /)
Thank you for your time and consideration.
Sincerely,
Name of Member and Credentials
Institution Name
Address
Email Address
Participants for this survey were selected at random from the NATA membership database according to
the selection criteria provided by the student doing the survey. This student survey is not approved or
endorsed by NATA. It is being sent to you because of NATA’s commitment to athletic training education
and research.
41
APPENDIX C
Contact Cover Letter for Survey
42
Dear Certified Athletic Trainer,
I am a master’s degree candidate at California State University, Sacramento
requesting your help to complete part of my degree requirements. The purpose of
this message is to request your participation in a research investigation designed to
look at Factors Associated with Recurrent Anterior Cruciate Ruptures in Female
Intercollegiate Soccer Players from Fall 2005 until Spring of 2011.
This student survey is not approved or endorsed by NATA. It is being sent to you
because of NATA’s commitment to athletic training education and research.
The questionnaire consists of 19 yes/no, check all that apply and demographic
questions which should take approximately 20-30 minutes to complete.
Participation in this study is entirely voluntary and refusal to participate involves
no penalty, neither will harm be placed by taking this survey.
As a fellow certified athletic trainer, your knowledge and opinions regarding this topic
makes your input invaluable. Please take a few minutes to fill out the anonymous
questionnaire and submit it by April 14, 2012.
The following link https://www.surveymonkey.com/s/ACL-Silva will direct you to the
questionnaire and specific instructions. Strict confidentiality will be maintained
throughout this research. If you have any questions, comments, or technical difficulties,
please contact me, Elizabeth Silva at (XXX) XXX-XXXX or xxxxxx@xxxxxxx.edu.
Thank you in advance for your time and for your assistance with this research project.
Sincerely,
Elizabeth Silva, ATC
Graduate Assistant Athletic Trainer
California State University, Sacramento
Participants for this survey were selected at random from the NATA membership database according to
the selection criteria provided by the student doing the survey. This student survey is not approved or
endorsed by NATA. It is being sent to you because of NATA’s commitment to athletic training education
and research.
43
REFERENCES
(1990). Dorland's illustrated medical dictionary. (26 ed.). Philadelphia: W. B. Saunders
Company.
Alentron-Geli, E., Myer G. D., Silvers H. J., Smaitier G., Romero, D., Lazaro-Haro, C.,
& Cugat R., (2009). Prevention of non-contact anterior cruciate ligament injuries
in soccer players. Part 2: a review of prevention programs aimed to modify risk
factors and to reduce injury rates. Knee Surg Sports Tramatol Arthrosc, 17, 859879. Doi: 10.1007/s00167-009-0823-z
Battaglia II, M. J., Cordasco, F. A., Hannafin, J. A., Rodeo, S. A., O’Brien, S. J., Altchek,
D. W., Cavanaugh, J., & Wickiewicz, T. L. (2007). Results of revision anterior
cruciate ligament surgery. The American Journal of Sports Medicine, 35(12),
2057-2066. Doi: 10.1177//0363546507307391
Foster, J B. (2008, May). ACL injury experts shift focus to extend beyond gender bias.
Biomechanics The Magazine of Body Movement and Medicine. XV (5), 11.
France, R. C. (2011). Introduction to sports medicine and athletic training. (2 ed.). New
York: Delmar.
Gammons, M. & Schwartz, E. (2011, November 2). Anterior cruciate ligament injury.
MedScape, Retrieved from http://emedicine.medscape.com/article/89442overview.
Garofalo, R., Moretti, B., Kombot, C., Moretti L., & Mouhsine E. (2007, May). Femoral
tunnel placement in anterior cruciate ligament reconstruction: rationale of the two
incision technique. Journal of Orthopaedic Surgery and Research. 2(10), 1-6.
44
Hetzler, T. M., Luke, A. L., Bushman, B. A. & Hetzler, B. S. (2009). Anterior cruciate
ligament reconstruction return to play criteria commonly utilized by certified
athletic trainers. Journal of Athletic Training, 44(3), S-33.
Hewett, T E., Myer, G D., Ford, K R., (2006). Anterior cruciate ligament injuries in
female athletes part 1, mechanisms and risk factors. The American Journal of
Sports Medicine, 34(2), 299-311. doi: 10.1177/0363546505284183
Houglum, P. A. (2005). Therapeutic exercise for musculoskeletal injuries. (2 ed.).
Champaign, IL: Human Kinetics.
Kaedinq, C. C., Aros, B., Pedroza, A., Pifel, E., Amendola, A., Andresh, J. T., Dunn, W.
R., Marx, R. G., McCarty, E. C., Parker, R. D., Wright, R. W., & Spindler, K. P.,
(2010). Allograft versus autograft ligament reconstruction predictors of failure
from a moon prospective longitudinal cohort. Sports Health A Multidisciplinary
Approach, 3(1), 73-81. doi: 10.1177/1941738110386185
McDaniel, L. W., Rasche A., Gaudet, L., & Jackson, A., (2010). Reducing the risk of
ACL injury in female athletes. Contemporary Issues In Education Research,
3(3,) 15-20.
Nagda, S. H., Altobelli, G. G., Bowdry, K. A., Brewster, C. E., & Lombardo S. R.,
(2010). Cost analysis of outpatient anterior cruciate ligament reconstruction
autograft versus allograft. Clinical Orthopaedics and Related Research, 468,
1418-1422.
45
Prentice, W. E. (2011). The knee and related structures. In M. Ryan, W. Glass & C.
Johnson (Eds.), Principles of Athletic Training A Competency-Based Approach
(14 ed., pp. 556-600). New York: McGraw Hill.
Spindler, K. P., Wright, R W., (2008). Anterior cruciate ligament tear. The New England
Journal of Medicine, 359(20), 2135-2142.
The MARS Group. (2010). Descriptive epidemiology of the multicenter acl revision
study (mars) cohort. The American Journal of Sports Medicine, 38(10), 19791986. DOI: 10.1177/0363546510378645
Walden, M, Jagglund, M, Werner, J & Ekstrand, J (2010). The epidemiology of anterior
cruciate ligament injury in football (soccer): a review of literature from a genderrelated perspective. Knee Surg Sports Traumatol Arthrosac, 19, 3-10. DOI:
10.1007/s00167-010-1172-7
Wright, R. W., Magnussen, R. A., Dunn, W. R., & Spindler, K. P. (2011). Ipsilateral graft
and contralateral acl rupture at five years or more following acl reconstruction.
The journal of bone and Joint Surgery, Incorporated, 93-A (12), 1159-1165. DOI:
10.2106/JBJS.J.00898