І- Acute Lymphoblastic Leukemia
advertisement

Molecular Biology Methods
Flowcytometric and FISH Markers in
Childhood Acute Lymphoblastic Leukemia
Dr Gihan EL Hussieny Gawish, MSc, PhD.
2
Acknowledgements
First of all, I cannot give a word to fulfill my deeps love and thanks
to (Allah) for lighting me the way not only throughout this piece of work but
also throughout my whole life.
This work is dedicated to:
My husband; Dr Hussein Al Omer and my Family
I am indebted to King Saud University for support and encouragement to
finish this work.
Also, I wish to express my deep thanks to:
Prof. Dr./ Abdelfattah M. Attalah, Professor of Genetics &
Immunology, George Washington University, USA (Former).
Director of Biotechnology Research Center, New Damietta, Egypt,
for continuous advice
Prof. Dr./ Ahmed Abd Al Salam Settin, Professor of Pediatrics &
Genetics, Faculty of Medicine, Mansoura University for his
continuous help
Finally, I am indebted to all the team of the honorable Genetics
Unit, Mansoura University Children Hospital, for their continuous
support and encouragement
Gihan El Hussieny Gawish
January 2009
3
Contents
Title
Introduction
Review of Literature
I- Acute lymphoblastic leukemia
1-Definition
2-Incidence of Leukemia
3-Types of leukemia
4-Biological Classification of ALL
5-Causing of Leukemia
6-The Signs of Leukemia
7-Stages of Childhood ALL
8-Treatment of Childhood ALL
9-Four Phases of Treatment
II- Cell cycle and apoptosis
1-Cell cycle
1-1-Cell cycle and cancer
2-Apoptosis and its markers
2-1-The mechanism of apoptosis
2-2-Apoptosis-targeted therapies for hematologica malignancies
2-3-The apoptosis promoter (p53)
2-4-The inhibitor of apoptosis
2-4-1-Bcl2 proteins
2-4-2-C-myc oncogene
III-Flow cytometry
1-Introduction
2-Principles of flow cytometric instrumentation
2-1-Fluidic system
2-2-Illumination system
2-3-Optical and electronics system
2-4-Data storage and computer control system
3-Data analysis
IV- Applications of flow cytometry
1-Cell cycle analysis
1-1-Staining procedure
Page
1
4
4
4
5
6
6
7
9
11
11
14
15
15
19
20
21
25
30
35
35
38
42
42
44
46
49
53
54
59
63
65
66
4
Page
1-2-Evaluation of DNA histogram
2-Immunophenotyping Applications
2-1-Erythrocyte analysis
2-2-HIV monitoring
2-3-Immunophenotyping of leukemias
2-4Quantification of stem cells
2-5-Platelet analysis
2-6-Testing for HLA-B27
3-Major applications of apoptosis analysis
3-1- Apoptosis light scatter
3-2-Apoptosis DNA analysis
3-3-Apoptosis cell membrane analysis
3-4-Apoptosis enzyme analysis
3-5-Apoptosis organelle analysis
4- Detection of apoptotic markers
V- Flourescence in situ hybridization
1-Introduction
2-Three different types of FISH probes
2-1-Locus specific probes
2-2-Alphoid or centromeric repeat probes
2-3-Whole chromosome probes
3-Applications of FISH
3-1-ALL investigation by FISH
3-1-1-Philadelphia
VI- References
VII- Life Flowcytometric Figures
VIII-Life FISH Pictures
67
71
72
73
73
75
75
76
76
77
78
80
82
83
83
86
86
91
91
91
92
92
96
97
106
144
147
5
List of Figure
Review of Literature
Page
Figure (2-1)
A schematic representation of the mammalian cell cycle
18
Figure (2-2)
The intrinsic or mitochondrial pathway
22
Figure (2-3)
The mechanism of apoptosis (Apoptosis triggered by
external signals: the extrinsic or death receptor path way)
24
Figure (2-4)
Diagram of the mitochondrial and death receptor pathways
of cell death
26
Figure (3-1)
Facscaliblur flow cytometry instrument
47
Figure (3-2)
Flow cytometer system (Facscalibur)
48
Figure (3-3)
Flow cytometers use the principle of hydrodynamics
focusing for presenting cells to a laser
50
Figure (3-4)
A simplified illustration of Flow Cytometry
52
Figure (3-5)
Two parameter histogram and dot plot displaying FL1-FITC
on the x axis and FL2-PE on the y axis
57
Figure (3-6)
Figure (3-7)
58
60
Figure (3-8)
FlowJo program
Analysis pulse width versus pulse height or area we can
eliminate the majority of G0 doublets that appear as G2
DNA histogram
Figure (3-9)
DNA histogram (aneuphliod population)
62
Figure (4-1)
Coeffecient of Variation (C.V.)
69
Figure (4-2)
Propidium iodide and TO-PRO-3
79
Figure (4-3)
Figure (5-1)
Sub G1 peak by propidium iodide staining
Fluoresence in situ hypridization
81
88
61
6
List of Abbreviations
AL
ALL
ALT
AO
AST
BM
CBC
CD
CML
CV
DAPI
DI
DMSO
DNA
EB
EDTA
FAB
FACS
FISH
FITC
G0/G1
G2/M
HIV
HLA
HPV
LC
MMC
MRD
PBS
PI
PS
S phase
Acute leukemia
Acut lymphoblastic leukemia
Alanine amino transaminase
Acridine orange
Aspartate amino transaminase
Bone marrow
Complete blood picture
Cluster of differentiation
Chronic myeloid leukemia
Coefficient of variation
4-6 diamino -2-2phenylindole
DNA index
Dimethylsulfoxide
Deoxyribonucleic acid
Ethedium bromide
Ethyline diamine tetraacetic acid
French American British
Flow activated cell sorter
Fluorescence in situ hybridization
Flourecien isothiocyanate
Phase represents the gap in of DNA replication time
between mitosis and the start
Phase represents the gap between the end of DNA
replication onest of mitosis
Human immunodeficiency virus
Human leukocyte antigen
Human papilloma virus
Liver cirrhosis
Mithramycin
Minimal residual disease
Phosphate buffer saline
Propidium iodide
Phosphatidylserine
DNA syntheis
7
WBC
White blood cells
Introduction
Childhood acute lymphoblastic leukemia (ALL) is a disease in
which too many underdeveloped lymphocytes are found in a child's blood
and bone marrow. Lymphocytes are infection-fighting white blood cells.
ALL is the most common form of leukemia in children, and the most
common kind of childhood cancer (Moorman et al., 2006).
Acute lymphoblastic leukemia (ALL) represents nearly one third of
all pediatric cancers. Annual incidence of ALL is about 30 cases per million
populations, with a peak incidence in patients aged 2-5 years. Although a
small percentage of cases are associated with inherited genetic syndromes,
the cause of ALL remains largely unknown (Jeffrey, 2005).
Flow cytometry can be applied in basic research and in the clinic to
identify and measure apoptotic cells. The choice of a particular flow method
depends on several variables (cell system, type of flow cytometer, type of
apoptosis inducer, type of information required) (Bogh and Duling, 2005).
The cell cycle was subdivided into four consecutive phases; G1 or
pre-synthetic phase, S, G2 or post-synthetic phase, and M phase during which
mitotic division into two daughter cells takes place. The G2 phase represents
the gap in time between the end of DNA replication and onset of mitosis. It is
possible to discrimination between G1 vs, S vs, G2 or M cells because of the
difference in their DNA content (Rabinovitch, 1993).
8
The DNA content of the cell can provide a great deal of information
about the cell cycle. The measurement of the DNA content of cells was one
of the first major applications of flow cytometry (Albro et al., 1993).
Apoptosis (programmed cell death) is a physiologic phenomenon
where in the dying cell plays an active part in its own destruction (Schuler et
al., 1994). Apoptosis plays a role in many diseases. There is a great potential
for treatment of these diseases in developing agents that can alter the
apoptotic process and change the natural disease progression. Molecules
whose roles in apoptosis have been investigated include Bcl-2 and c-myc
proteins, the p53 tumor suppressor gene and various tumor suppressor gene
products (Menendez et al., 2004).
P53 is a pro-apoptotic genes present in all cells, but has special
significance to cancer cells. It is a tumor repressor gene, meaning that its
presence reduces the occurrence of cancer tumors by promoting apoptosis in
cancer cells (Polyak et al., 1997). BCL2 is an important regulator of
apoptosis, The oncogenic activity of the Bcl2 gene is carried out via
suppression of lymphocytic apoptosis or programmed cell death (Cory &
Adams, 2002 and Roumier et al., 2002). C-Myc is widely known as a crucial
regulator of cell proliferation in normal and neoplastic cells (Wechsler et al.,
1997& Facchini and Penn, 1998).
The technology of flow cytometry and the discovery of a method to
produce monoclonal antibodies have made possible the clinical use of flow
cytometry for the identification of cell populations. Monoclonal antibodies
(tagged) with the fluorescent dye are commonly used for the identification of
cell surface antigens and fluorescent dyes that directly and specifically bind
9
to certain components of the cell (i.e. DNA) are used for cell cycle analysis
(Zhang et al., 2005).
Fluorescence in situ hybridization (FISH) allows identification of
specific sequences in a structurally preserved cell, in metaphase or interphase
(Chatzimeletiou et al., 2005). FISH is increasingly used for the identification
of ALL. FISH plays an important role in detecting chromosome changes
(Primo et al., 2003).
Almost all the chromosome abnormalities in ALL are translocations.
The most common one is Philadelphia chromosome. It is the main product of
the t(9;22) translocation. This translocation causes a rearrangement between
the proto-oncogene c-ABL and a gene called the breakpoint cluster region
(BCR). The BCR/ABL fusion gene resulting from t(9;22) translocation. FISH
is increasingly used for the identification of BCR/ABL gene rearrangements
(Rudolph et al., 2005).
10
І- Acute Lymphoblastic Leukemia
Acute lymphoblastic leukemia (ALL) is the most common form of
childhood cancer. It is a type of cancer that starts from white blood cells in
the bone marrow called lymphocytes. In most cases it quickly moves into the
blood. It can then spread to other parts of the body including the lymph
nodes, liver, spleen and central nervous system (Moorman et al., 2006).
Leukemia is a cancer of the blood cells. There are several types of
leukemia and these are classified by how quickly they progress and what cell
they affect. Acute leukemia is fast-growing and can overrun the body within
a few weeks or months. By contrast, chronic leukemia is slow-growing and
progressively worsens over years (Carolyn et al., 2002).
Normal blood cells contain white blood cells, red blood cells,
platelets and fluid called plasma. All of these products are formed in the bone
marrow, a spongy area located in the center of bones. It contains a small
percentage of cells that are in development and are not yet mature. These
cells are called blasts. Once the cell has matured, it moves out of the bone
marrow and into the circulating blood. The body has mechanisms to know
when more cells are needed and has the ability to produce them in an orderly
fashion (Carroll et al., 2003).
11
1-Incidence of Leukemia:
Acute lymphoblastic leukemia is the most common form of
childhood leukemia where it accounts for about 75% of childhood leukemia
and 25% of all pediatric cancer (Lanzkowsky, 2000). National Cancer
Institue, Cairo University, ALL represents 23.3% of all pediatric
malignancies and 75% of all pediatric leukemias. In a more recent research in
the Pediatric Heamatology/Oncology Unit, Ain Shams University Hospital,
ALL constitutes 82% of all leukemic cases (Khalifa et al., 1999).
The global incidence of leukemias is about 8 to 9 per 100,000 people
each year. Approximately 250,000 new cases occur annually worldwide.
Leukemia accounts for 2.5% of overall cancer incidence. However, its
incidence among children demonstrates its significance. Although childhood
cases (through 14 years of age) account for about 12% of all leukemias,
childhood cancer is the second biggest killer of children (after accidents) and
leukemia is the most common form of childhood cancer. The incidence of
childhood ALL in the United States has increased approximately 20% over
the past two decades, mostly in the 0- to 4-year-old age group. Over the
course of this century, leukemia rates have also generally increased (Sandler
and Ross, 1997).
Acute lymphoblastic leukemia affects slightly more boys than girls.
It occurs predominantly in children, peaking at four years of age. It is seen
more frequently in industrialized nations, and it is slightly more common
among white children and boys. Studies have suggested that patients who are
younger than thirty five years of age far better than older patients (Jeffrey,
2005).
12
2-Types of leukemia:
By considering whether leukemias are acute or chronic, and whether
they are myelogenous or lymphocytic, they can be divided into four main
types. The first one is an acute myeloid leukemia which occurs in both
children and adults. The second one is an acute lymphocytic leukemia which
is the most common type seen in children, but also seen in adult's over65.The
third one is a chronic myelogenous leukemia which occurs mostly in adults.
Chronic lymphocytic is the fourth type which is the most often seen in people
over age55, can affect younger adults, but almost never seen in children (Pui,
1995).
In acute leukemia, the bone marrow cells are unable to properly
mature. Immature leukemia cells, which are often called blasts, continue to
reproduce and accumulate. In chronic leukemia, the cells can mature but not
completely. They are not really normal. They generally do not fight infection
as well as do normal white blood cells. Of course, they live longer, build up,
and crowd out normal cells. The types of leukemia are also grouped by the
type of white blood cell that is affected, leukemia that affects lymphoid cells
is called lymphocytic leukemia, and leukemia that affects myeloid cells is
called myeloid leukemia or myelogenous leukemia (Lichtman et al., 1995).
3-Biological Classification of ALL:
Acute lymphoblastic leukemia blasts are derived from either B-cell
or T-cell lineages, as determined by cell surface and other markers. A small
percentage of the cells are either so primitive that they do not express enough
markers to identify (Ross et al., 2003 and Pullen et al., 1999).
13
Acute lymphoblastic leukemia is categorized according to a system
know as the French-American-British (FAB) Morphological Classification
Scheme for ALL. ALL1 is mature-appearing lymphoblasts (T-cells or pre-Bcells); these cells are small with uniform genetic material, regular nuclear
shape, nonvisible nucleoli, and little cytoplasm. ALL2 is immature and
pleomorphic lymphoblasts (T-cells or pre-B-cells), these cells are large,
variable in size, varaiable genetic material, irregular nuclear shape, one or
more large nucleoli and variable cytoplasm. ALL3 is lymphoblast(Bcells),these are large, genetic material is finely stripped and uniform, nuclear
shape is regular, there are one or more prominent nucleoli, and cytoplasm is
moderately abundant (Schrappe et al., 2000).
4-Causing of Leukemia:
The causes of the disease are not known, but experts believe that
ALL develops from a combination of genetic and environmental factors. A
number of genetic mutations associated with ALL have been identified.
Missing or defective genes that suppress tumors are responsible for cases of
ALL (Guo et al., 2005).
Several things have been identified as risk factors-that is, exposure
to them puts a person at a higher risk of developing leukemia, but it is not a
certainly that this exposure will lead to leukemia. These factors include
exposure to high-energy radiation, like that released from a nuclear accident
or bomb. Some genetic syndrome put a person at higher risk. People who
work with the chemical benzene over a long period of time also have a
greater chance of getting leukemia. Some scientist feel that exposure to
14
electromagnetic fields, like those that come from power lines, may put a
person to higher risk, but this has not been proven (Pui et al., 2001).
Heredity, radiation, chemical exposures, and treatment with
chemotherapeutic agents have been implicated in the development of
leukemia. Viral infection by at least one known virus, human T-cell
leukemia/lymphotropic virus type I (HTLV-1), is a well-understood cause of
adult T-cell leukemia (Franchini, 1995 and Greaves, 1997).
Another
group
of
risk
factors
includes
occupational
and
environmental exposure to radiation or chemicals. The best established cause
of leukemia among children is in utero exposure to diagnostic X-rays.
Leukemia in adults is strongly associated with occupational exposure to
ionizing radiation. There is little evidence, however, that nonionizing
radiation such as electromagnetic fields (EMF) induces leukemia. Indeed,
two recent studies have shown that EMF exposure is not a major risk factor
for leukemia in children or in adults.
Some studies have reported an
association between cancer and high levels of electromagnetic radiation
(EMR). Whether lower levels of radiation (eg, living near power lines, video
screen emissions, small appliances, cell phones) play any major role is
uncertain but probably unlikely (Linet et al., 1997 and Verkasalo, 1996).
Because most people in the general population are not exposed to
chemotherapeutic drugs or occupationally exposed to radiation or chemical
solvents, exposure to these agents cannot explain the causes of the majority
of leukemia cases diagnosed each year. We conservatively estimate that the
causes of at least 20,000 (approximately 70%) of the 28,000 new leukemia
cases that develop annually in the United States are unexplained. Thus, the
15
causes of leukemia remain largely unknown. Although some success has
been achieved in treating leukemias, especially in children, mortality rates
have remained relatively high (approximately 75% in the United States)
(Kazak et al., 1997).
Genetic predisposition may play a major role in both adult and
childhood leukemia. Although the Leukemia Society of America emphasizes
the fact that anyone may develop the disease, an increased risk exists among
Eastern European Jews, and a decreased risk exists among Asians
(differences in diet and lifestyle may play a role, however). Individuals with a
family history of leukemia or lymphoma have a 5.6-fold increased risk for
AML. Parents of children with Down syndrome also have an increased risk
of leukemia (Greaves, 1997 and Shannon et al., 1992).
Up to 65% of leukemias contain genetic rearrangements, called
translocations, in which some of the genetic material (genes) on a
chromosome may be altered, or shuffled, between a pair of chromosomes.
For example the most common genetic injury in ALL is t(12;21), which
means a translocation with a genetic shift between chromosome 12 and 21. It
is also referred to as TEL-AML1 fusion and occurs in approximately 20% of
ALL patients. Researchers believe that this translocation may occur during
fetal development in some patients. About 20% of adults and about 5% of
children with ALL have a genetic abnormality called the Philadelphia (Ph)
chromosome t(9;22). Another important chromosome translocation is t(4;11)
involving the MLL gene on chromosome II. Often occurring in children
under one year old (Khandakar et al., 2005).
16
5-The Signs and diagnosis of Leukemia:
The blast cells are unable to perform their normal function of
fighting infection, so patients may develop fevers or infections that won't go
away. As the number of immature cells (blasts) increases, the normal cells
are crowded out. This leads to low red blood cell counts and platelets (Smith
et al., 1996).
Acute lymphoblastic leukemia tends to cause symptoms more rapidly
than chronic leukemia. Some common symptoms include fever, chills,
weakness and fatigue, swollen or tender lymph nodes, liver or spleen, easy
bleeding or bruising, swollen or bleeding gums, night sweats, and bone pain.
The abnormal cells can accumulate in the brain or spinal cord, causing
headaches, vomiting, confusion, or seizures (Adachi et al., 2005).
In acute lymphoblastic leukemia, the doctor asks about medical
history and conducts a physical exam. During the exam, abnormalities such
as enlarged spleen, liver or lymph nodes may be detected, prompting further
investigation. Complete blood count would find blast cells present in the
blood, thus suggestion a diagnosis of leukemia. This test can reveal that the
patient has leukemia. A sample of bone marrow is determined the type of
leukemia (Champlin et al. 1989 and Burger et al., 2003).
A complete blood cell count is the first step in diagnosing ALL. This
test will often show various findings, including the following: The presence
of circulatory leukemic blast cells, the presence and severity of anemia and
the count of a variety of blood cell types. (A high white blood cell count
indicates a more severe disease.) These tests will not always show the
17
presence of leukemic cells. Blood tests do not always detect leukemia, and
about 10% of patients with ALL have a normal blood cell count (Adachi et
al., 2005).
If the results of the blood tests are abnormal or the physician
suspects leukemia despite normal cell counts, a bone marrow aspiration and
biopsy are the next steps (Rezaei et al., 2003).
If bone marrow examination confirms ALL, a spinal tap may be
performed, which uses a needle inserted into the spinal canal. A sample of
cerebrospinal fluid with leukemia cells is a sign that the disease has spread to
the central nervous system. In most cases of childhood ALL, leukemic cells
are not found in the cerebrospinal fluid (Vieira et al., 2005).
6-Treatment of Childhood ALL:
The treatment depends on age, the results of laboratory tests, and
whether or not the child has been previously treated for leukemia. Untreated
ALL means that no treatment has been given except to reduce symptoms.
There are too many white blood cells in the blood and bone marrow, and
there may be other signs and symptoms of leukemia. Remission means that
treatment has been given and the number of white blood cells and other blood
cells in the blood and bone marrow is normal that there no signs or symptoms
of leukemia. Recurrent disease means that the leukemia has come back after
going into remission. Refractory disease means that the leukemia failed to go
into remission following treatment (Bassan et al., 1997).
There are treatments for all patients with childhood acute
lymphoblastic leukemia. The primary treatment for ALL is chemotherapy.
18
Radiaion therapy may be used in certain cases. Bone marrow transplantation
is being studied in clinical trials (Uckun et al., 1997).
Acute lymphoblastic leukemia patients should receive chemotherapy
drugs as soon as possible after diagnosis. Chemotherapy uses strong drugs to
kill leukemia cells. The goal of chemotherapy is to achieve remission (no
symptoms of ALL) and to restore normal blood cell production. Common
chemotherapy drugs include doxorubicin, fludarabine and cyclophosphamide.
The drugs used depend on factors such as the patient's age and the number
and type of leukemia cells in the blood. Unfortunately, chemotherapy also
kills normal cells, so ALL patients receiving chemotherapy may have side
effects, including nausea, tiredness and a higher risk of infections (Balduzzi
et al., 2005).
For most patients, chemotherapy restores normal blood cell
production within a few weeks, and microscopic examinations of their blood
and marrow samples will show no signs of leukemia cells. When this
happens, the disease is in remission. Although chemotherapy often brings
long-lasting remissions in children, in adults, ALL frequently returns. If the
ALL returns, patients and their doctors can consider more chemotherapy or a
marrow or blood cell transplant. Chemotherapeutic agents kill cancer cells by
activating apoptosis, or programmed cell death. Major apoptotic pathways
and the specific role of key proteins in this response is described. The
expression level of some of these proteins, such as Bcl2, BAX, and caspase 3,
has been shown to be predictive of ultimate outcome in hematopoietic
tumors. New therapeutic approaches that modulate the apoptotic pathway are
now available and may be applicable to the treatment of childhood ALL
(Donadieu & Hill, 2001 and Nakase et al., 2005).
19
Radiation therapy uses X-rays or other high-energy rays to kill
cancer cells and shrink tumors. Radiation for ALL usually comes from a
machine outside the body (external beam radiation therapy) (Durrant et al.,
1997).
Bone marrow transplantation is a newer type of treatment. First, high
doses of chemotherapy with or without radiation therapy are given to destroy
all of the bone marrow in the body. A bone marrow transplant using marrow
from a relative or person not related to the patient is called an allogeneic bone
marrow transplant (Ulrich et al., 2001).
An even newer type of bone marrow transplant, called autologous bone
marrow transplant, is being studied in clinical trials. During this procedure,
bone marrow is taken from the patient and may be treated with drugs to kill
any cancer cells. The marrow is frozen to save it. The patient is then given
high-dose chemotherapy with or without radiation therapy to destroy all of
the remaining marrow. The frozen marrow that was saved is thawed and
given through a needle in a vein to replace the marrow that was destroyed
(Sebban et el., 1994).
Treatment outcome is dependent not only on the therapy applied, but
importantly, also on the underlying biology of the tumor and the host. Each of
these variables must be factored into initial treatment decisions, as well as
later refinements based on initial response, and several biological features. It
is recognized that with improvements in therapy, certain variables might lose
their prognostic value; therefore, risk assignment plans should be routinely
reassessed. Finally an optimal system should allow for comparison of the
20
outcomes of similar or identical patients, treated on different protocols (Choi
et al., 2005).
There are generally four phases of treatment for ALL. The first
phase, remission induction therapy, uses chemotherapy to kill as many of the
leukemia cells as possible to cause the cancer to go into remission. The
second phase, called central nervous system (CNS) prophylaxis, is preventive
therapy,
it
involves
using
intrathecal
and/or
high-dose
systemic
chemotherapy to the CNS to kill any leukemia cells present there. It is also
used to prevent the spread of cancer cells to the brain and spinal cord even if
no cancer has been detected there. Radiation therapy to the brain may also be
given, in addition to chemotherapy, for this purpose. CNS prophylaxis is
often given in conjunction with consolidation therapy. Once a child goes into
remission and there no signs of leukemia, a third phase of treatment called
consolidation or intensification therapy, is given. Consolidation therapy uses
high-dose chemotherapy to attempt to kill any remaining leukemia cells. The
fourth phase of treatment, called maintenance therapy, uses chemotherapy for
several years to maintain the remission (Attal et al., 1995).
21
II- Cell cycle and Apoptosis
1-Cell cycle:
The concept of the cycle in its current form is introduced by Howard
and Plec, (1953). They observed that DNA synthesis (S- phase) in individual
cells was discontinuous and occupied a discrete portion of the cell life and
was constant in duration. Mitotic division (M-phase) was seen to occur after
certain period of time following DNA replication. A distinct phase between
DNA replication and mitosis was also apparent (Look et al., 1996).
Cell cycle phase of G1 was historically considered to be a time cells
had little observable activity. Since this time precedes DNA synthesis, the
term Gap 1 (G1) was coined. They have diploid chromosome (2C=46
chromosome). At a certain point in the cell's life, the DNA synthetic
machinery turns on. This phase of the cell's life is labeled "S" for synthesis.
As the cell proceeds through this phase, its DNA content increases from 2C
to 4C. At the end of S, the cell has duplicated its genome and it is in the
tetraploid state. After the S phase, the cell again enters a phase that was
historically thought to be quiescent. Since this phase is the second gap region,
it is referred to as G2. In the G2 phase, the cell is producing the necessary
proteins that will play a major role in cytokinase. After a highly variable
amount of time, the cell enters mitosis (M). DNA content remains constant at
4C until the cell actually divides at the end telophase (Liblit, 1993).
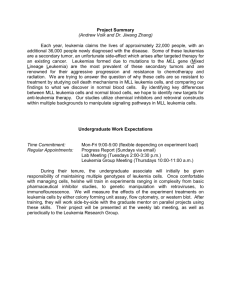
The process of replicating DNA and dividing a cell can be described
as a series of coordinated events that compose a "cell division cycle,"
22
illustrated for mammalian cells in Fig (2-1). In each cell division cycle,
chromosomes are replicated once (DNA synthesis or S-phase) and segregated
to create two genetically identical daughter cells (mitosis or M-phase). These
events are spaced by intervals of growth and reorganization (gap phases G1
and G2). Cells can stop cycling after division, entering a state of quiescence
(G0). Commitment to traverse an entire cycle is made in late G1. At least two
types of cell cycle control mechanisms are recognized: a cascade of protein
phosphorylations that relay a cell from one stage to the next and a set of
checkpoints that monitor completion of critical events and delay progression
to the next stage if necessary (Nasmyth, 1996).
The first type of control involves a highly regulated kinase family.
Kinase activation generally requires association with a second subunit that is
transiently expressed at the appropriate period of the cell cycle; the periodic
"cyclin" subunit associates with its partner "cyclin-dependent kinase" (CDK)
to create an active complex with unique substrate specificity. Regulatory
phosphorylation and dephosphorylation fine-tune the activity of CDK-cyclin
complexes, ensuring well-delineated transitions between cell cycle stages
(Elledge, 1996).
A second type of cell cycle regulation, checkpoint control, is more
supervisory. It is not an essential part of the cycle progression machinery.
Cell cycle checkpoints sense flaws in critical events such as DNA replication
and chromosome segregation. When checkpoints are activated, for example
by underreplicated or damaged DNA, signals are relayed to the cell cycleprogression machinery. These signals cause a delay in cycle progression,
until the danger of mutation has been averted. Because checkpoint function is
not required in every cell cycle, the extent of checkpoint function is not as
23
obvious as that of components integral to the process, such as CDKs (Sherr,
1996).
Figure (2-1): A schematic representation of the mammalian cell cycle
(Nasmyth, 1996).
24
25
1-1-Cell cycle and cancer:
Superficially, the connection between the cell cycle and cancer is
obvious: cell cycle machinery controls cell proliferation, and cancer is a
disease of inappropriate cell proliferation. Fundamentally, all cancers permit
the existence of too many cells. However, this cell number excess is linked in
a vicious cycle with a reduction in sensitivity to signals that normally tell a
cell to adhere, differentiate, or die. This combination of altered properties
increases the difficulty of deciphering which changes are primarily
responsible for causing cancer (Jacks and Weinberg, 1996).
The first genetic alterations shown to contribute to cancer
development were gain-of-function mutations. These mutations define a set
of "oncogenes" that are mutant versions of normal cellular "protooncogenes."
The products of protooncogenes function in signal transduction pathways that
promote cell proliferation. However, transformation by individual oncogenes
can be redundant (mutation of one of several genes will lead to
transformation) or can be cell type-specific (mutations will transform some
cells but have no effect on others). This suggests that multiple, distinct
pathways of genetic alteration lead to cancer, but that not all pathways have
the same role in each cell type (White, 1996).
More recently, the significance of loss-of-function mutations in
carcinogenesis has become increasingly apparent. Mutations in these socalled "tumor suppressor" genes were initially recognized to have a major
role in inherited cancer susceptibility. Because inactivation of both copies of
a tumor suppressor gene is required for loss of function, individuals
heterozygous for mutations at the locus are phenotypically normal. Thus,
26
unlike
gain-of-function mutations,
loss-of-function
tumor
suppressor
mutations can be carried in the gene pool with no direct deleterious
consequence. However, individuals heterozygous for tumor suppressor
mutations are more likely to develop cancer, because only one mutational
event is required to prevent synthesis of any functional gene product
(Morgenbesser et al., 1994).
It now appears that tumor suppressor gene mutations are highly
likely to promote, and may even be required for, a large number of
spontaneous as well as hereditary forms of cancer. Loss of function of the
tumor suppressor gene product pRb, for example, would be predicted to
liberate E2F transcriptional activators without requiring phosphorylation and
thus bypass a normal negative regulation controlling entry into the cycle.
Loss of the tumor suppressor gene product p16 would have a similar
consequence, liberating E2Fs by increasing pRb phosphorylation . In
addition, cell cycle progression can be halted at several points by the tumor
suppressor gene product p53, activated in response to checkpoints sensing
DNA and possibly also chromosome damage; loss of p53 would remove this
brake to cycling (Symonds et al., 1994).
2-Apoptosis and its markers:
Apoptosis and necrosis are too distinct, mutually exclusive, modes
of cell death. Apoptosis, frequently referred to as programmed cell death is
an active and physiological mode of cell death, in which the cell itself
designs and executes the program of its own demise and subsequent body
disposal. Different patterns of apoptosis (early and delayed apoptosis) many
cell types, cells of hematopoietic origin in particular, undergo apoptosis
27
rapidly, to within few hours following exposure to relatively high
concentration of cytotoxic agents (Majino and Joris, 1995).
Apoptosis can be defined as 'gene-directed cellular self-destruction''
although this is really a phenomenon where cells are programmed to die at a
particular point, e.g. during embryonic development, and even here cells may
go through an apoptotic pathway. However, apoptosis is certainly a distinct
process from other forms of oncosis leading to necrosis (Gerbaulet et al.,
2005 and Wallach et al., 1999).
Apoptosis affects individual cells, physiological induction e.g. lack
of signals, phagocytosis by macrophages or other cells and there is no
inflammatory response. Necrosis affects group of cells, non physiological
induction e.g. virus and poison, phagocytosis of macrophages and there is
inflammatory response (Wirth et al., 2005).
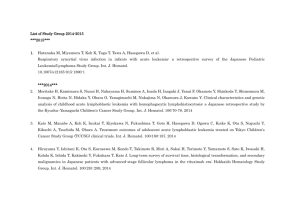
There are three different mechanisms by which a cell commits
suicide by apoptosis. In the intrinsic or mitochondarial pathway, the outer
membranes of mitochondria in a healthy cell express the protein; Bcl2 on
their surface. Bcl2 is bound to a molecule of the protein Apaf-1. Internal
damage to the cell (e.g., from reactive oxygen species) causes Bcl2 to release
Apaf-1; a related protein, Bax, to penetrate mitochondrial membranes
causing cytochrome c to leak out. The released cytochrome c and Apaf-1
bind to molecules of caspase 9 Fig. (2-2). The resulting complex of
cytochrome c, Apaf-1, caspase 9 and ATP is called the apoptosome. The
apoptosome aggregate in the cytosol (Niu et al., 2005 and Lam et al., 2005
and Kroemer& Reed 2000).
28
Figure (2-2): The intrinsic or mitochondrial pathway (Lam et al., 2005).
29
Caspase 9 is one of a family of over a dozen caspases. They are all
proteases. They get their name because they cleave proteins-mostly each
other at aspiratic acid residues. Caspase 9 cleaves and, in so doing, activates
other caspases. The sequential activation of one caspase by another creates an
expanding cascade of proteolytic activity (rather like that in blood clotting
and complement activation) which leads to digestion of structural proteins in
the cytoplasm, degradation of chromosomal DNA and phagocytosis of the
cell (Wada et al., 2005).
In the extrinsic or death receptor pathway, Fas and the TNF receptor
are integral membrane proteins with their receptor domains exposed at the
surface of the cell. Binding of the complementary death activator (FasL and
TNF respectively) transmits a signal to the cytoplasm that leads to activation
of caspase 8. Caspase 8 (like caspase 9) initiates a cascade of caspase
activation leading to phagocytosis of the cell Fig. (2-3). For example,
cytotoxic T cells recognize (bind to) their target, they produce more FasL at
their surface, this binds with the Fas on the surface of the target cell leading
to its death by apoptosis. In some cases, final destruction of the cell is
guaranted only withits engulfment by a phagocyte (Bijangi et al., 2005 and
Vega et al., 2005).
In the third way, neurons, and perhaps other cells, have another way
to self-destruct that unlike the two paths described above, doesn't use
caspase. Apoptosis- inducing factor (AIF) is a protein that is normally located
in the inter membrane space of mitochondaria. When the cell receives a
signal telling it that it is time to die, AIF is released from the mitochondrial, it
is migrates into the nucleus and binds to DNA, Which triggers the destruction
of the DNA and cell death (Urbano et al., 2005).
30
Figure (2-3): The mechanism of apoptosis (Apoptosis triggered by
external signals: the extrinsic or death receptor path way) (Bijangi et al.,
2005).
31
Defects in programmed cell death (apoptosis) mechanisms play
important roles in the pathogenesis and progression of hematological
malignancies, allowing neoplastic cells to survive beyond their normally
intended life-spans and subverting the need for exogenous survival factors.
Apoptosis defects also serve as an important complement to proto-oncogene
activation, as many deregulated oncoproteins that drive cell division also
trigger apoptosis (Evan and Littlewood, 1998).
Similarly, errors in DNA repair and chromosome segregation
normally trigger cell suicide as a defense mechanism for eradicating
genetically unstable cells, and thus apoptosis defects permit survival of the
genetically unstable
cells,
providing opportunities
for
selection
of
progressively aggressive clones (Ionov et al., 2000).
Chemotherapy and irradiation trigger apoptosis in tumor cells and an
understanding of the biochemical pathways involved in apoptosis provides an
opportunity to classify tumors based on their response to common induction
regimens. Multiple distinct signaling pathways regulate apoptosis, but two
major cell death pathways have been implicated in hematological
malignancies: the mitochondrial pathway and the death receptor pathway Fig.
(2-4) (Evans et al., 2002).
32
Figure (2-4): Diagram of the mitochondrial and death receptor pathways
of cell death (Evans et al., 2002).
33
Both of these pathways ultimately activate members of the caspase
family of proteins that are responsible for executing the terminal phases of
apoptosis. p53 protein levels rise in response to various cellular stresses
including chemotherapy. p53 induces the loss of mitochondrial membrane
potential with subsequent release of cytochrome c, which forms a complex,
the "apoptosome," with the adapter molecule Apaf-1, ATP, and caspase-9.
This complex, in turn, activates caspase-3 (Evans et al., 2002).
Another proximal pathway of cell death involves death receptor
signaling at the cell surface. Binding of CD95-L and other tumor necrosis
factor (TNF) family ligands to their death inducing receptors, CD95/APO1/FAS or TNF- and TRAIL respectively, leads to receptor trimerization and
the
recruitment
of
adapter
molecules. These
molecules
include
FADD/MORT-1 that in turn lead to recruitment and activation of caspase-8.
This initiator caspase also cleaves and activates downstream caspases,
including caspase-3. Although generally described as being distinct, these
two proximal pathways are interconnected. For example, caspase-8 cleaves
the pro-apoptotic protein BID, which results in translocation to the
mitochondria and release of cytochrome c (Kishi et al., 2003, Blom, 2000, de
Franchis et al., 2000 and Goto et al., 2001).
Several studies have examined the prognostic significance of
apoptotic protein expression in leukemia. Defects in the p53 pathway are
distinctly rare in childhood malignancies including ALL, where mutations are
detected in < 5% of cases at the time of initial diagnosis. However, relapsed
blasts may harbor mutations of p53 gene much more commonly. Further,
ALL blasts at relapse have been noted to express high levels of the Mdm-2
34
protein, which abrogates p53 signaling (Dirven et al., 1995 and Pemble et
al., 1994).
Cancer-associated
defects
in
apoptosis
play
a
role in
chemoresistance and radioresistance, increasing the threshold for cell death,
and thereby requiring higher doses for tumor killing (Tschopp et al., 1999
and Makin et al., 2000).
Melanoma (skin cancer) cells avoid apoptosis by inhibiting the
expression of the gene encoding Apaf-1. Some cancer cells, especially lung
and colon cancer cells, secrete elevated levels of a soluble (decoy) molecule
that binds to FasL, plugging it up so it cannot bind Fas. Thus cytotoxic T
cells (CTL) cannot kill the cancer cells by the mechanism of death receptor
pathway. Other cancer cells express high levels of FasL, and can kill any
cytotoxic T cells (CTL) that try to kill them because CTL also express Fas
(but are protected from their own FasL) (Meijer et al., 2005).
Apoptosis plays a role in many diseases, such as cancer, viral
infections, and autoimmune and neurodegenerative disorders. There is a great
potential for treatment of these diseases in developing agents that can alter
the apoptotic process and change the natural disease progression. Molecules
whose roles in apoptosis have been investigated include Bcl-2 and c-myc
proteins, the p53 tumor suppressor gene and various tumor suppressor gene
products, MAP kinases, and proteases (Menendez et al., 2004).
2-1-The apoptosis promoter (p53):
p53 stimulates a wide network of signals that act through two major
apoptotic pathways. The extrinsic, death receptor pathway triggers the
35
activation of a caspase cascade, and the intrinsic, mitochondrial pathway
shifts the balance in the Bcl-2 family towards the pro-apoptotic members,
promoting the formation of the apoptosome, and consequently caspasemediated apoptosis. The impact of these two apoptotic pathways may be
enhanced when they converge through Bid, which is a p53 target. The
majority of these apoptotic effects are mediated through the induction of
specific apoptotic target genes. However, p53 can also promote apoptosis by
a transcription-independent mechanism under certain conditions. Thus, a
multitude of mechanisms are employed by p53 to ensure efficient induction
of apoptosis in a stage-, tissue- and stress-signal-specific manner (Linda &
Carol, 1996 and Susan et al., 2003).
Some cancer causing viruses use tricks to prevent apoptosis of the
cells they have transformed. Several human papilloma viruses (HPV) have
been implicated in causing cervical cancer. One of them produces a protein
(E6) that binds and inactivates the apoptosis promoter p53. Binding of Fas
ligand or agonistic anti-Fas antibody to the death receptor Fas can activate a
caspase-cascade resulting in apoptosis. Fas cell surface expression was
determined by flow cytometry (Hougardy et al., 2005).
Genes involved in apoptosis are either pro-apoptotic (promote
apoptosis) or anti-apoptotic (inhibit apoptosis). P53 is a pro-apoptotic genes
present in all cells, but has special significance to cancer cells. It is a tumor
repressor gene, meaning that its presence reduces the occurrence of cancer
tumors by promoting apoptosis in cancer cells. Normally it induces apoptosis
by activating caspases 9, 8, 7, and 3. The loss of p53 decreases caspase
activation and therefore the cell will not undergo apoptosis. Mutation in the
p53 gene is the most common mutation in cancer; it is present in about half
36
of all cancer tumors, 80% in all colon cancer tumors, 50% of lung cancer
tumors, and 40% of breast cancer tumors (Polyak et al., 1997).
Under normal conditions p53 is a short-lived protein. The p53
inhibitor Mdm2 (Hdm2 in humans) is largely responsible for keeping p53 in
this state. Mdm2 inhibits the transcriptional activity of p53 and, more
importantly, promotes its degradation by the proteasome (Levine, 1997).
p53 mutants in tumours have a reduced affinity for DNA and a
reduced ability to induce apoptosis. We describe a mutant with the opposite
phenotype, an increased affinity for some p53-binding sites and an increased
ability to induce apoptosis. The apoptotic function requires transcription
activation by p53 (Elisabeth et al., 1999).
Early observations suggested that p53 may function as an oncogene,
because overexpression of p53 appeared to cause oncogenic transformation
of cells. In the late 1980s, however, several critical discoveries defined the
normal function of p53 to be anti-oncogenic. Wild-type p53 genes, when
introduced into cells, were found to be growth suppressive (Isabela et al.,
2000).
p53 plays multiple roles in cells. Expression of high levels of wildtype (but not mutant) p53 has two outcomes: cell cycle arrest or apoptosis. In
response to genotoxic stress, p53 acts as an "emergency brake" inducing
either arrest or apoptosis, protecting the genome from accumulating excess
mutations. Consistent with this notion, cells lacking p53 were shown to be
genetically unstable and thus more prone to tumors (Isabela et al., 2000).
37
p53 promotes cytochrome c release through the induction of target
genes encoding BH3-only proteins. Importantly, p53 also induces APAF-1
expression through a response element within the APAF-1 promoter (Kannan
et al., 2001)
The tumor suppressor gene product p53 is clearly a central player in
many biochemical pathways that are pivotal to human carcinogenesis. The
sequence-specific DNA binding properties of this nuclear phosphoprotein
regulate the transcription of a continually expanding number of genes, the
protein products of which regulate cell cycle progression and apoptosis
(Isabela et al., 2000).
Loss of p53 function by mutation is common in cancer. However,
most natural p53 mutations occur at a late stage in tumor development, and
many clinically detectable cancers have reduced p53 expression but no p53
mutations. It remains to be fully determined what mechanisms disable p53
during malignant initiation and in cancers without mutations that directly
affect p53. p53 mutants in tumours have a reduced affinity for DNA and a
reduced ability to induce apoptosis (Niu et al., 2005).
p53 expression has important clinical implications as an indicator of
prognosis and response to chemotherapy or radiotherapy in different human
tumor types. The common effect of p53 mutations found in tumours is to
inactivate p53 as a transcription factor. Consequently, a great deal of effort
has been expended in trying to identify transcriptional targets of p53.
Particular attention has been paid to target genes which may mediate cellcycle arrest and apoptosis (Ko and Prives, 1996 ).
38
p53 dependent G1 and G2 arrest requires induction of the p21 cyclindependent kinase inhibitor. In contrast, no single gene can explain p53induced apoptosis. Many p53 target genes have been identified which
function in known apoptotic pathways, regulate survival factor signalling,
induce apoptosis when over expressed or are involved in biochemical events
linked to apoptosis (Buckbinder et al., 1997 , Miyashita and Reed, 1995 ,
Owen-Schaub et al., 1995, Polyak et al., 1997, Varmeh-Ziaie et al., 1997,
McCurrach et al., 1997 and Rampino et al., 1997).
p53 can activate target genes through a non-canonical sequence. The
first such example is in the p53-induced gene 3 (PIG3), which has been
implicated in the accumulation of reactive oxygen species and apoptosis
induction (Polyak et al., 1997). Another recently described example is the
gene encoding the pro-apoptotic phosphatase PAC1, which is induced
through binding of p53 to a novel palindromic binding site (Yin et al., 2003).
A novel insight into the interplay between p53 and its family
members, p63 and p73, in the induction of apoptosis has been recently
revealed (Flores et al., 2002). The effect of p63 and p73 on p53
transcriptional activity, using a selection of knockout mouse embryo
fibroblasts (MEFs), defined two distinct classes of target gene. Whereas p53
alone is sufficient for the induction of p21 and Mdm2, the induction of the
apoptotic genes PERP, Bax and Noxa requires p53 together with p63 and
p73. This finding demonstrates an essential role for both p63 and p73 in the
efficient induction of apoptotic target genes by p53. The mechanism of this
cooperation is currently unknown, but it may involve an enhanced binding to
and/or stabilization of the transcription complex on the promoters of p53
39
apoptotic target genes by the cooperative action of all three members (Urist
and Prives, 2002).
In addition to the contribution of p63 and p73 to the apoptotic
function of p53, they play an important role in the precise control of cell
death during normal mouse development. p73 also plays a role in the
induction of cell death in response to DNA damage, a process involving
cooperation between the Abl tyrosine kinase and p73 (Shaul, 2000).
Immunohistochemical (IHC) detection of p53 expression has been
established as a relatively easy and straightforward method for fresh and
archival tissues. Available monoclonal antibodies recognize both wild-type
and mutant forms, but there may be a selective detection of the latter owing to
the very short half-life of the former (Porter et al., 1992 and Soussi et al.,
1994).
p53 is a tumor suppressor that is rarely mutated in ALL patients
but whose function is frequently altered by mutations to genes that code for
proteins that regulate p53 function. Activation of p53 occurs in response to
cells that have acquired DNA damage that may be engaged in aberrant cell
proliferation. Mutations to proteins that regulate p53 function, like HDM2,
p14, and p21, are frequent findings in ALL (Roman et al., 2002).
Bovine papillomavirus type 1 (BPV-1)-transformed mouse fibroblast
cell lines were analyzed via flow cytometry (FCM) for expression of p53
protein along with their DNA content. Significantly elevated levels of the p53
protein was present in some but not all of the transformed cell lines.
Quantitation of p53 protein in cell lines containing BPV-1 DNA revealed that
40
the tumorigenic cell lines expressed higher levels of the p53 protein
(Agrawal et al., 1994).
The correlation between p53 abnormalities and DNA aneuploidy and
that analysis of p53 protein is useful for prediction of clinical course in
esophageal squamous cell carcinoma (Goukon et al., 1994).
Liu et al., (2004) evaluated changes in apoptotic proteins expression
that occur in response to chemotherapy in pediatric cases with acute leukemia
just prior to and 1, 6 and 24 hours following the administration of multiagent
chemotherapy. They found great heterogeneity in the patterns of apoptotic
protein expression in the initial response to chemotherapy among individual
patient samples. Importantly, no increases in p53, p21 or Mdm-2 protein
expression were seen in leukemic blasts from the standard risk patients whose
initial treatment consisted of the non-p53-dependent drugs, vincristine and
prednisone.
In the subgroup of children who received at least one p53 dependent
drug, patients could be segregated into two groups, one group that showed
up-regulation of p53 protein and its target p21, and another group that
showed no increase following therapy, thus identifying at least two distinct
pathways leading to apoptosis (Chen et al., 1996).
2-2-Bcl2 proteins
Members of the Bcl-2 protein family play pivotal roles in the
decision and execution phases of apoptosis in the mitochondrial pathway. To
date, 24 Bcl-2 family members have been identified as either pro- (e.g., Bax,
41
Bak, Bcl-XS, Bid, Bad, and Noxa) or anti- (e.g., Bcl-2 and Bcl-XL) apoptotic
proteins. Bcl-2 proteins form homo- and heterodimeric complexes to regulate
mitochondrial channel formation and subsequent release of cytochrome c
from the mitochondria (Kishi et al., 2003, Blom, 2000, de Franchis et al.,
2000, Goto et al., 2001 and Cryns et al., 1999).
The Bcl2 family proteins are the central regulators of the
mitochondrial pathway. Bcl2 is an inhibitor of apoptosis. Bcl2 and its human
homolog introduce a new category of oncogenes that act by decreasing cell
death. Over expression of Bcl2 promotes oncogensis by repressing cell death
and extending cell life. However, overexpression can also lead to retardation
of cell cycling via prolongation of the G1 phase of the cycle (Webb et al.,
2005 and Green & Reed, 1998).
The Bcl2 family of intracellular proteins is the central regulator of
caspase activation, and its opposing factions of anti- and pro-apoptotic
members arbitrate the life-or-death decision. The oncogenic activity of the
Bcl2 gene is carried out via suppression of lymphocytic apoptosis or
programmed cell death. (Cory & Adams, 2002 and Roumier et al., 2002).
BCL2 is an important regulator of apoptosis, first identified from its
involvement in follicular B cell lymphoma, where the common t(8:14)
translocation causes the activation of the BCL2 oncogene. BCL2 is now
recognised as a survival factor for many types of cell, notably neurons.
Expression of BCL2 is widespread during embryogenesis but is restricted to
long-lived cells in the adult. A critical mediator of BCL2 apoptosis is
interleukin-1 beta-converting enzyme (ICE) a cysteine protease that
processes IL-1 beta during the inflammatory response (Roumier et al., 2002).
42
BCL2 is a member of a multigene family (highly conserved
evolutionarily with viral homologues). Other proteins in the family (BCLX,
BAD, BAX, BAD etc) antagonise inhibition of apoptosis by binding to
BCL2. Hence the balance of various members of the BCL family determines
the extent to which cell death is promoted or prevented. This model is
consistent with the findings of high levels of BCL2 in a variety of solid
tumours (Jiang and Milner, 2003).
Apoptosis can also be induced by a variety of cytokines e.g. TGF
beta family, which inhibit the proliferation of a wide variety of cell types that
may undergo concomitant cell death. TGF beta induced apoptosis is blocked
in myeloblastic leukaemia cells by BCL2 expressed at a level that does not
block but merely delays p53-induced apoptosis. This may reflect the fact that
both TGF beta and p53 suppress BCL2 but only p53 has the ability to
activate BAX, thus deflecting the expression pattern towards apoptosis
(Seckin et al., 2002).
Active cell suicide (apoptosis) is induced by events such as growth
factor withdrawal and toxins. It is controlled by regulators, which have either
an inhibitory effect on programmed cell death (anti-apoptotic) or block the
protective effect of inhibitors (pro-apoptotic). Many viruses have found a
way of countering defensive apoptosis by encoding their own anti-apoptosis
genes preventing their target-cells from dying too soon. All proteins
belonging to the Bcl-2 family contain either a BH1, BH2, BH3, or BH4
domain. All anti-apoptotic proteins contain BH1 and BH2 domains, some of
them contain an additional N-terminal BH4 domain (Bcl-2, Bcl-x (L), Bclw), which is never seen in pro-apoptotic proteins, except for Bcl-x(S). On the
other hand, all pro-apoptotic proteins contain a BH3 domain (except for Bad)
43
necessary for dimerization with other proteins of Bcl-2 family and crucial for
their killing activity, some of them also contain BH1 and BH2 domains (Bax,
Bak). The BH3 domain is also present in some anti-apoptotic protein, such as
Bcl-2 or Bcl-x (L). Proteins that are known to contain these domains include
vertebrate Bcl-2 (alpha and beta isoforms) and Bcl-x (isoforms (Bcl-x(L) and
Bcl-x(S)) (Poliseno et al., 2002).
Antiapoptotic B cell leukemia/lymphoma (BCL2) family
proteins are expressed in many cancers, but the circumstances under which
these proteins are necessary for tumor maintenance are poorly understood. A
novel functional assay that uses Bcl2 homology domain (BH3) peptides to
predict dependence on antiapoptotic proteins was exploiteded , a strategy,
BH3 profiling. BH3 profiling accurately predicts sensitivity to Bcl2
antagonist ABT-737 in primary chronic lymphocytic leukemia (CLL) cells.
BH3 profiling also accurately distinguishes myeloid cell leukemia sequence 1
(MCL1) from Bcl2 dependence in myeloma cell lines. It was shown that the
special sensitivity of CLL cells to Bcl2 antagonism arises from the
requirement that Bcl2 tonically sequester proapoptotic BIM in CLL. ABT737 displaced BIM from Bcl2's BH3-binding pocket, allowing BIM to
activate BAX, induce mitochondrial permeabilization, and rapidly commit
the CLL cell to death. It was demonstrated that Bcl2 expression alone does
not dictate sensitivity to ABT-737. Instead, Bcl2 complexed to BIM is the
critical target for ABT-737 in CLL. An important implication is that in
cancer, Bcl2 may not effectively buffer chemotherapy death signals if it is
already sequestering proapoptotic BH3-only proteins. Indeed, activator BH3only occupation of Bcl2 may prime cancer cells for death, offering a potential
explanation for the marked chemosensitivity of certain cancers that express
44
abundant Bcl2, such as CLL and follicular lymphoma (Del Gazio et al.,
2007).
The relationship between gene expression of Bcl 2 and Bax and the
therapeutic effect in oral cancer patients had investigated. A significant
correlation between Bcl-2/Bax gene expression ratio in the peripheral blood
mononuclear cells (PBMCs) from the patients, and the therapeutic effect of
radiation therapy These findings suggested that Bcl-2 and Bax gene
expression in PBMCs may be useful as a prognostic factor in oral cancer
patients (Oshikawa et al., 2006).
Epstein-Barr virus (EBV), the cause of mononucleosis and cause of
Burkitt's lymphoma produces a protein similar to Bcl2 and produces another
protein that causes the cell to increase its own production of Bcl2. Both these
actions make the cell more resistant to apoptosis (thus enabling the cancer
cell to continue to proliferate). Even cancer cells produced without the
participation of viruses may have tricks to avoid apoptosis (Lu et al., 2005).
Some B-cell leukemias and lymphomas express high levels of Bcl2,
thus blocking apoptotic signals they may receive. The high levels result from
a translocation of the Bcl2 gene into an inhancer region for antibody
production (Menendez et al., 2004).
Bcl2-L12 contributes to the classical tumor biological features of
Glioblastoma (GBM) such as intense apoptosis resistance and florid necrosis,
and may provide a target for enhanced therapeutic responsiveness of this
lethal cancer (Stegh et al., 2007).
2-3C-myc oncogene:
45
The c-myc gene was discovered as the cellular homolog of the retro
viral v-myc oncogene 20 years ago. The c-myc proto-oncogene was
subsequently found to be activated in various animal and human tumors. It
belongs to the family of myc genes that includes B-myc, L-myc, N-myc, and
s-myc; however, only c-myc, L-myc, and N-myc have neoplastic potential
(Wechsler et al., 1997 and Facchini & Penn, 1998). Targeted homozygous
deletion of the murine c-myc gene results in embryonic lethality, suggesting
that it is critical for development. Homozygous inactivation of c-myc in rat
fibroblasts caused a marked prolongation of cell doubling time, further
suggesting a central role for c-myc in regulating cell proliferation (Mateyak
et al., 1997).
Bovine papillomavirus type 1 (BPV-1)-transformed mouse
fibroblast cell lines were analyzed via flow cytometry (FCM) for expression
of c-myc protein along with their DNA content. Significantly elevated levels
of the c-myc protein was present in some but not all of the transformed cell
lines. Quantitation of c-myc protein in cell lines containing BPV-1 DNA
revealed that the tumorigenic cell lines expressed higher levels of the c-myc
protein (Agrawal et al., 1994).
The role of c-Myc in the cell cycle has been a confusing area due to
the collection of data from different experimental models, although it is well
established that c-myc is an early serum response gene. It should be noted
that models of serum or growth factor stimulation of starved cells primarily
address the G0/G1 and G1/S transitions. Therefore, early studies implicated cMyc in the G0/G1 transition. In cycling cells, however, the participation of cMyc in the cell cycle may be different. Furthermore, in anchorage-dependent
46
cell growth, c-Myc may affect other components of the cell cycle (Amati et
al., 1998).
It is proposed that c-Myc induces apoptosis through separate 'death
priming' and 'death triggering' mechanisms in which 'death priming' and
mitogenic signals are coordinated. Investigation of the mechanisms that
underlie the triggering steps may offer new therapeutic opportunities
(Prendergast, 1999).
The antiapoptotic effect of Epstein-Barr virus (EBV) was associated
with a higher level of Bcl-2 expression and an EBV-dependent decrease in
steady-state levels of c-MYC protein. Although the EBV EBNA-1 protein is
expressed in all EBV-associated tumors and is reported to have oncogenic
potential, enforced expression of EBNA-1 alone in EBV-negative Akata cells
failed to restore tumorigenicity or EBV-dependent down-regulation of cMYC. These data provide direct evidence that EBV contributes to the
tumorigenic potential of Burkitt lymphoma and suggest a novel model
whereby a restricted latency program of EBV promotes B-cell survival, and
thus virus persistence within an immune host, by selectively targeting the
expression of c-MYC (Ingrid et al., 1999).
Much recent research on c-Myc has focused on how it drives
apoptosis. c-Myc is widely known as a crucial regulator of cell proliferation
in normal and neoplastic cells, but until relatively recently its apoptotic
properties, which appear to be intrinsic, were not fully appreciated. Its deathdealing aspects have gained wide attention in part because of their potential
therapeutic utility in advanced malignancy, where c-Myc is frequently
deregulated and where novel modalities are badly needed. Although its exact
47
function remains obscure, c-Myc is a transcription factor and advances have
been made in characterizing target genes which may mediate its apoptotic
properties (Hermeking, 2003).
Ectopic expression of c-Myc (Myc) in most primary cell types
results in programmed cell death, and malignant transformation cannot occur
without additional mutations that block apoptosis. The development of Mycinduced lymphoid tumors was studied. Myc can be upregulated in acute
myeloid leukemia (AML), but its exact role in myeloid leukemogenesis is
unclear. To study its role in AML, a murine stem cell virus (MSCV)
retroviral gene transfer/transplantation system was used to broadly express
Myc in the bone marrow of mice either alone or in combination with
antiapoptotic mutations. Myc expression in the context either of Arf/Ink4a
loss or Bcl-2 coexpression induced a mixture of acute myeloid and acute
lymphoid leukemias (AML+ALL). In the absence of antiapoptotic mutations
however, all mice transplanted with MSCV-Myc developed AML exclusively.
MSCV-Myc-induced AML was polyclonal, readily transplantable, possessed
an intact Arf-p53 pathway, and did not display cytogenetic abnormalities by
spectral karyotyping analysis. Lastly, it was found that Myc preferentially
stimulated the growth of myeloid progenitor cells in methylcellulose. These
data provided the first direct evidence that Myc is a critical downstream
effector of myeloid leukemogenesis and suggested that myeloid progenitors
are intrinsically resistant to Myc-induced (Hui et al., 2005).
48
III-Flow cytometry
Flow cytometry is a laser-based technology that is used to measure
characteristics of biological particles. This technology is used to perform
measurements on whole cells as well as prepared cellular constituents such as
nuclei and organelles (Melamed et al., 1990, Tileney et al., 1996 and
McCoy, 2002).
The flow cytometer is an instrument for measuring scattered and
fluorescent light from single particles. The physics of the interaction of light
with single particles provides the scientific foundation for the design and
49
operation of the flow cytometer and for the critical evaluation of flow
cytometric data (Scornik et al., 1994).
Flow cytometry uses the principles of light scattering, light excitation,
and emission of fluorochrome molecules to generate specific multi-parameter
data from particles and cells in the size range of 0.5um to 40um diameter.
Cells are hydro-dynamically focused in a sheath of phosphate buffer saline
(PBS) before intercepting an optimally focused light source. Lasers are most
often used as a light source in flow cytometry (Talbot, 1993).
The technology of flow cytometry and the discovery of a method to
produce monoclonal antibodies have made possible the clinical use of flow
cytometry for the identification of cell populations. Light scatter is utilized to
identify the cell populations of interest, while the measurement of
fluorescence intensity provides specific information about individual cells.
Monoclonal antibodies (tagged) with the fluorescent dye are commonly used
for the identification of cell surface antigens and fluorescent dyes that
directly and specifically bind to certain components of the cell (i.e. DNA) are
used for cell cycle analysis (Reckenwald, 1993 and Shapiro, 1995).
Cells or particles are prepared as single-cell suspension for flow
cytometric analysis. This allows them to flow single file in a liquid stream
past a laser beam. As the laser strikes the individual cells. First light
scattering occurs that is directly related to structural and morphological cell
features. Second, fluorescence occurs if the cells are attached to a fluorescent
probe. Fluoresent probes are typically monoclonal antibodies that have been
conjucated to fluorochromes; they can also be fluorescent stains reagents that
50
are not conjugated to antibodies (Parks and Herzenberg, 1989 and
Rechenwald et al, 1993).
Fluorescent probes are reacted with the cells or particles of interest
before analysis; therefore, the amount of fluorescence emitted as a particle
passes the light source is proportional to the amount of fluorescent probe
bound to the cell or cellular constituent (Radcliff and Jaroszeski, 1998).
After acquisition of light scattering and fluorescence data for each
particle, the resulting information can be analyzed utilizing a computer and
specific software that are associated with the cytometer (Rose et al,. 1992
and Longobardi-Given, 1992).
There are two distinct types of flow cytometers that can be used to
acquire data from particles. One type can perform acquisition of light
scattering and fluorescence only. The other type is capable of acquiring
scattering and fluorescence data but also has the powerful ability to sort
particles. Both types function in a similar manner during acquisition, for
example FACScan (Becton Dickinson), this equipped with an air –cooled 15
mw argon ion laser emitting at 488 nm. Three fluorescence channels can be
measured as well as two light scatter parameters. The FACScan is also
equipped with a doublet discrimination module allowing the analysis of the
cell cycle. The FACScan is user-operated (after instruction) and is available
for use 24 hours per day (Kandathil et al., 2005).
However, sorting instruments have the powerful ability to physically
separate particles based on light scattering and/or fluorescent emission
characteristics. Cytometers were originally designed to sort, for example
FACS caliber 1, 2 (Becton Dickison), this used for analysis only. Unlike the
51
FACScan which is a dual laser system. The primary laser is an air-cooled 15
mw argon ion laser emitting at 488 nm thus allowing two light scatter
parameters and three fluorescence channels to be measured. The second laser
is ared diode laser emitting at 635nm. Thus allowing for the excitation of
other dyes such as allophycocyanin or to-pro-3 with power Macintosh G4
running system 9.0 and cell Quest v 3.3. Thus, cytometers that perform
acquisition without sorting are the most common of the two types (Rose et
al., 1992).
1-Principles of flow cytometric instrumentation:
Flow cytometers are very complex instruments that are composed of
four closely related systems. The fluidic system transports particles from a
suspension through the cytometer for interrogation by an illumination
system. The resulting light scattering and fluorescence is collected, filtered,
and converted into electrical signals by the optical and electronics system.
The data storage and computer control system saves acquired data and is also
the user interface for controlling most instrument functions. These four
systems provide a very unique and powerful analytical tool for researchers
and clinicians. This is because they analyze the properties of individual
particles, and thousands of particles can be analyzed in a matter of seconds.
Thus, data for a flow cytometric sample are a collection of many
measurements instead of a single bulk measurement (Radcliff and
Jarosezeski, 1998)..
Histograms are the simplest modes of data representation.
Histograms allow visualization of a single acquired parameter. Mean
fluorescence and distributional statistics can be obtained based on markers
52
that the user can graphically set on the plot. Multiple histograms can be
overlaid on one another to depict qualitative and quantitative differences in
two or more samples. Two-parameter data plots are somewhat more
complicated than histograms; however, they can yield more information.
Two-parameter dot plots of FSC vs SSC allow visualization of both lightscattering parameters that are important for identifying populations of
interest. Bivariate fluorescent plots allow discrimination of dual-labeled
populations that might remain hidden if histograms were used to display
fluorescent data. Two-parameter plots that combine one light-scattering
parameter and a fluorescent parameter are useful for analyzing control
samples to elucidate the origin of nonspecific binding. Data analysis is very
graphically oriented. Experience and pattern recognition become important
when using two-parameter data plots for qualitative as well as quantitative
analysis. The technique of gating or drawing regions on dual parameter lightscatter plots allows one to exclude information and examine the population
of interest by disallowing particles that might confound or interfere with
analysis. This is one of the fundamental uses for gating (Radcliff and
Jarosezeski, 1998).
Flow cytometers can be described as four interrelated systems which
are shown in Fig. (3-1). these four basic systems are common to all
cytometers regardless of the instrument manufacturer and whether or not the
cytometer is designed for analysis or sorting (Melamed et al., 1990 and
Longobardi-Given, 1992 Owens & Loken, 1995).
1-1-Fluidic system:
The fluidic system is the heart of a flow cytometer and is responsible
for transporting cells or particles from a prepared sample through the
53
instrument for data acquision Fig. (3-2). The primary component of this
system is a flow chamber. The fluidic design of the instrument and the flow
chamber determine how the light from the illumination source ultimately
meets and interrogates particles. Typically, a diluent, such as phosphate
buffered saline, is directed by air pressure into the flow chamber. This fluid is
referred to as sheath fluid and passes through the flow chamber after which it
is intersected by the illumination source. Then, the sample under analysis, in
the form of a single particle suspension, is directed into the sheath fluid
stream prior to sample interrogations. The sample then travels by laminar
flow through the chamber (Ormerod, 1994).
54
Figure (3-1): Facscaliblur flow cytometry instrument.
55
Figure (3-2): Flow cytometer system (Facscalibur) (Ormerod, 1994).
56
The pressure of the sheath fluid against the suspended particles
aligns the particles in a single file fashion. This process is called
hydrodynamic focusing and allows each cell to be interrogated by the
illumination source individually while traveling within the sheath fluid
stream (Radcliff and Jaroszeski, 1998).
The flow cell is the functional core of the fluidic system because it
presents cells in a single file for interrogation by the cytometer illumination
system. A typical flow cell Fig. (3-3) consists of a converging nozzle in
which sample is introduced at low flow rates into a larger laminar flow of
isotonic saline or sheath fluid. The cells in the sample follow the converging
streamlines and are hydrodynamically focused into alignment. The sample is
injected into the center of a sheath flow. The combined flow is reduced in
diameter, forcing the cell into the center of the stream. This the laser one cell
at a time. This schematic of the flow chamber in relation to the laser beam in
the sensing area (Philip, 2002).
1-2-Illumination system:
Flow cytometers use laser beams that intersect a cell or particle that
has been hydro dynamically focused by the fluidic system. Light from the
illumination source passes through a focusing apparatus before it intersects
the sample stream. This apparatus is a lens assembly that focuses the laser
emission into a beam with an elliptical cross-section that ensures a constant
amount of particle illumination despite any minor positional variations of
particles within the sample stream (Zimmermann and Truss, 1979).
57
Laser options
Figure (3-3): Flow cytometers use the principle of hydrodynamics
focusing for presenting cells to a laser (Philip, 2002).
58
Light and fluorescence are generated when the focused laser beam
strikes a particle within the sample stream. These light signals are then
quantitated by the optical and electronics system to yield data that is interprêt able by the user (Shapiro, 1995).
Two systems are used in flow cytometry to focus the illuminating
light to the point at which it intersects the cell stream. One type of system
uses a spherical lens to give a focal spot size of 30- 60 µm. The second
system uses a pair of crossed cylindrical lenses to focus the light to a sheet
about 120 µm wide and 4-7 µm deep (Cledat et al., 2004).
Most flow cytometers utilize a single laser, however, some systems
support the simultaneous use of two or more different lasers. The most
commonly used laser is an argon ion laser that has been configured to emit
light in the visible range of the spectrum. A 488- nm. Laser emission is used
for most standard applications. The majority of fluorochrom that are
available on the market today can be excited using this wavelength. Thus,
laser is excellent excitation sources because they provide a single wavelength
beam that is also stable, bright, and narrow. Some type of lasers present in
flow cytometers can be turned to U.V. or other wavelengths. If the exiting is
not tunable, then another laser source that emits the desired wavelength is
required. At the measuring point in a typical flow cytometer the stream of
cells intersects a beam of light from a laser or arc lamp Fig. (3-4). When light
interacts with biological particles some of the light is scattered out of the
incident beam and this scattered light may be collected over a range of angles
by detectors positioned around the measuring point (Gerstner et al., 2005).
59
Figure (3-4): A simplified illustration of Flow Cytometry (Gerstner et al.,
2005).
60
1-3-Optical and electronics system:
The excitation optics consists of the light source and the optical
components that serve to interrogate or excite the hydrodynamically focused
sample stream in the flow cell. The 488 nm line of the argon laser is used as a
light source in many commercially available cytometers, but any light source
that provides the requisite intensity, e.g. , the mercury vapor or the xenon are
lamp can be used. Optical components are used to expand, shape and focus
the light which then interacts with the sample in the flow cell. The flow cell
is usually made of quartz and is designed to minimize diffraction and to
maximize the collection of the optical signals. The light source is often a
laser. Laser is used because they provide a very concentrated and intense
beam of monochromatic character of the light is especially important in
making fluorescence measurements (Telford, 2004).
The amount of light that is scattered by a cell is a complex function
of its size, shape and refractive index. The sensitivity of light scattering to
each of these factors is dependent upon the range of angles over which the
scattered light. The light scattered at small angles (i.e. forward light scatter)
could be successfully used to determine relative volume distributions for
populations of cells (Wang et al., 2004).
Light scattered and emitted in all directions (360º) after the laser
beam strikes an individual cell or particle that has been hydrodynamically
focused. The optical and electronics system of a typical flow cytometer is
responsible for collecting and quantitating at least five types of parameters
from this scatter light and emitted fluorescence. Two of these parameters are
light scattering properties. Light that is scattered in the forward direction (in
the same direction as the laser beam) is analyzed as one parameter, and light
61
scattered at 90º relative to the incident beam is collected as a second
parameter. Forward-scattered (FSC) light is a result of diffraction. Diffracted
light provides basic morphological information such as relative cell size that
is referred to as forward angle light scatter (FSC). Light that is scattered at
90º to the incident beam is the result of refracted and reflected light. This
type of light scatters is referred to as side-angle light scatter (SSC). This
parameter is an indicator of granularity within the cytoplasm of cell as well
as surface membrane irregularities to topographies (Philip, 2002).
Most current laboratory bench-top flow cytometers are capable of
detecting fluorescence from three different regions of the visible spectrum.
Cutometers are optically conquered to detect a narrow range of wave lengths
in each region. Fluorescence emission is detected simultaneously along with
FSC and SSC data; therefore, up to five parameters can be simultaneously
measured for each analyzed sample (Longobardi- Given, 1992)
Fluorescence is detected using networks of mirrors, optics, and beam
splitters that direct the emitted fluorescent light toward highly specific optical
filters. The filters collect light within the range of wave lengths associated
with each of the three fluorescent channels. Filtered light is directed toward
photo multiplier tubes or PMTs for conversation into electrical signals
(Telford, 2004).
1-4-Data storage and computer control system:
After light scattering and fluorescence is converted to electrical
signals by the optical and electronics system, the information is converted
into digital data that the computer can interpret. The signals generated from
62
cells or particles are referred to as events and are stored by the computer
(Rose et al., 1992).
After the different signals or pulses are amplified they are processed
by an Analog to Digital Converter (ADC) which in turn allows for events to
be plotted on a graphical scale (One Parameter, Two parameter Histograms).
Flow cytometry data outputs are stored in the form of computer files
(Radcliff and Jaroszeski, 1998).
Histogram files can be in the form of one-parameter or twoparameter files. Histogram files consist of a list of the events corresponding
to the graphical display specified in your acquisition protocol. A oneparameter histogram is a graph of cell count on the y-axis and the
measurement parameter on x-axis. All one-parameter histograms have 1,024
channels. These channels correspond to the original voltage generated by a
specific "light" event detected by the PMT detector. In other words, the ADC
assigns a channel number based on the pulse height for individual events.
Therefore, brighter specific fluorescence events will yield a higher pulse
height and thus a higher channel number when displayed as a histogram. A
graph representing two measurement parameters, on the x- and y-axes, and
cell count height on a density gradient. This is similar to a topographical
map. You can select 64 or 256 channels on each axis of two-parameter
histograms. Particle counts are shown by dot density or by contour plot. Fig.
(3-5) (Roederer et al., 2004).
List-mode files consist of a complete listing of all events
corresponding to all the parameters collected, as specified by your acquisition
Protocol. This file follows a format specified by the FCS 3.0 standard. Raw
63
list-mode data files can be opened or replayed using any program designed
for analysis of flow cytometry data. You should keep in mind that a Protocol
serves as a template. It allows you to collect specified Parameters (i.e. FLS,
FL1, FL2, etc.), and how these parameters are displayed. Protocols also serve
to determine how the data is gated, and contains all the Regions from which
your statistics will be generated. In addition, Protocols contain other specific
information that serves as direct interface between the computer workstation
and the cytometer. These pertain to high voltage settings for the PMT
detectors, gains for amplification of linear parameters, sample flow rates,
fluorescence compensation, discrimination settings, etc. Once your data has
been collected and written into a list-mode file you can replay the file either
using the specific Protocol used for collection or any other program
specifically designed for analysis of flow cytometry data. However, you
should keep in mind that you can only adjust Regions, Gating, and
Parameters to be displayed. Settings such as amplification, fluorescence
compensation, etc., can not be modified. Therefore, when collecting data
make sure that your instrument settings are correct. Finally, if you open your
listmode files using a programs such as FlowJo Fig. (3-6), WINMIDI, and/or
ExPO you will have to specify parameter displays, and create Regions and
Gating corresponding to the Protocol used for collecting the data (McCoy,
2002).
64
Figure (3-5): Two parameter histogram and dot plot displaying FL1FITC on the x axis and FL2-PE on the y axis (Roederer et al., 2004).
65
Figure (3-6): FlowJo program (McCoy, 2002).
66
The number of events acquired for each sample is always determined
before analysis and is usually set using software designed to control
cytometer operation. A conventional acquisition value is 100.000 events per
sample. However this value may vary and range upward of events per sample
depending on the experimental objective (Melamed et al., 1990).
2-Data analysis:
Data analysis is a very critical part of any experiment that utilizes
flow cytometry. Data is analyzed using a computer and software is usually
specific to flow cytometric data and is often part of the same computer
system that is used to control the instrument during acquision. The most
common display is a histogram. A typical histogram data plot is shown in
Fig. (3-7, 3-8) (Abu- Absi et al., 2003).
It is also possible to display two parameters simultaneously such as
FSC vs SSc or FL1 vs FL2. For two parameter plots, data from a population
of individual particles can be displayed in the form of dots or as contours
shown in Fig. (3-9) (Parks and Henzenberg, 1989).
Contour density plots display the data from a population of cells as a
series of concentric lines that correlate to different cell or particle densities
within the axes. Dot-plots are probably the most common type of twoparameter plots, and they are also the easiest to understand (Robinson, 1993).
67
Figure (3-7): Analysis pulse width versus pulse height or area we can
eliminate the majority of G0 doublets that appear as G2 (Abu- Absi et al.,
2003).
68
Figure (3-8): DNA histogram (Abu- Absi et al., 2003).
69
Figure (3-9): DNA histogram (aneuphliod population) (Parks and
Henzenberg, 1989).
70
IV- Applications of flow cytometry
Flow cytometers are very complex instruments that are composed of
four closely related systems. They provide a very unique and powerful
analytical tool for researchers and clinicians. Therefore, the flow cytometer is
widely used in research as well as in clinical immunology and hematology to
perform rapid immunophenotyping, cell sorting, and DNA analysis
(Longobardi-Given, 1992 and Bogh & Duling, 2005).
Flow cytometry is used for immunophenotyping and DNA content of
a variety of specimens including whole blood, bone marrow, serous cavity
fluids, cerebrospinal fluid, urine and solid tissues. Characteristics that can be
measured include cell size, cytoplasmic complexity, DNA or RNA content,
and a wide range of membrane-bound and intracellular portents and sorting
the cells (Rechtnwald, 1993, Ormerod, 1994 and Assuncao et al., 2005).
The use of flow cytometry in the clinical laboratory has grown
substantially in the past decade. This is attributed in part to the development
of smaller user friendly, less expensive instruments and a continuous increase
in the number of clinical applications as shown in Table (4-1) (Brown and
Wittwer, 2000).
71
Flow cytometry provides rapid analysis of multiple characteristics of
single cells. The information obtained is both qualitative and quantitative.
Where as in the past flow cytometers were found only in larger academic
centers, advances in technology now make it possible for community
hospitals to use this methodology (Orfao et al., 1995 and McCoy, 2002).
Table (4-1): Common clinical uses of flow cytometry (Brown and
Wittwer, 2000).
Field
Immunology
Oncology
Hematology
Clinical application
Common characteristic
measures
Histocompitability crossmatching
IgM, IgG
Transplantation rejection
CD3, CIRCULATING OKT3
HLA-B27 detection
HLA-B27
Immunodeficiency studies
CD4, CD8
DNA content and S phase of tumors
DNA
Measurements of profilation markers
Ki-67, PCNA
Leukemia and Lymphoma phenotyping
Leukocyte surface antigens
Identification of prognostically important
Tdt, MPO
subgroups
Hematopiotic progenit or cell enumeration
CD34
Diagnosis of systematic mastocytosis
CD25,CD69
Reticylocyte enumeration
RNA
Autoimmuneand alloimmune disorders
Antiplatelats disorders
IgG, IgM
Anti-neutrophils antibodies
IgG
Immune complexes
Complement, IgG
Feto-maternal hemorrge quantification
Hemoglobin F, rhesus D
Immunohematology
Erthrocyte surface antigens
Assessment of leukocyte contamination of blood
Forward AND Side scatter
products
Genetic
disorders
PNH
CD55,CD59
72
Functions of cells can be defined through the application of
fluorochrome dyes that have an affinity for cellular components.
Traditionally, common clinical applications are immunophenotyping of cells
of the hematopoietic system with fluorescent-labeled antibodies raised
against specific cell surface proteins (Davis et al., 2002).
Other approaches have been used to elucidate changes in cell
function and DNA content. Examples of clinical applications in equine
patients include immune-mediated hemolytic anemia, immune-mediated
thrombocytopenia (IMT), chronic inflammatory disease, and neoplasia
(Davis et al., 2002).
The great advantage of flow cytometry is that its applications are
highly amenable to standardization. The efforts that have been made for flow
cytometric applications in four major fields of clinical cell analysis: CD4+ Tcell enumeration, CD34+ hematopoietic stem and progenitor cell
enumeration, screening for the HLA-B27 antigen and leukemia/lymphoma
immunophenotyping (Keeney et al., 2004).
The diagnosis of many primary immunodeficiency diseases requires
the use of several laboratory tests. Flow cytometry is applicable in the initial
73
workup and subsequent management of several primary immunodeficiency
diseases (Illoh, 2004).
1- Cell cycle analysis:
The measurement of the DNA content of cells was one of the first
major applications of flow cytometry and is still one of the biggest
applications in this laboratory today (Albro et al., 1993).
Flow cytometry offers the possibility to study several parameters
simultaneously, e.g. cell cycle modulation, mode of cell death, activity of
mitochondria. The phases of the cell cycle were determined and the induction
of apoptosis and necrosis was demonstrated by annexin binding, analysis of
mitochondrial membrane potential and DNA strand breaks (Tusch and
Schwab, 2005).
DNA ploidy and proliferative activity (S-phase fraction) are the two
biological parameters commonly measured by DNA flow cytometric
analysis. The prime purpose of most studies is the investigation of the
prognostic value of DNA flow cytometry in addition to the information
provided by conventional clinicopathological factors known to affect disease
prognosis. The general statement, for tumors in the same histopathological
stage of the disease, is that diploid and/or low proliferative tumors have a
more favourable prognosis than aneuploid and/or high proliferative tumors,
suggesting an important role of DNA flow cytometry in the assessment of
tumor behaviour and in the outcome evaluation of the disease. (Pinto et al.,
2002).
74
1-1-Staining procedure:
The preparation and staining of cell suspension are the major factors
determining the validity and reproducibility of flow cytometric analysis.
There is no flow cytometric staining procedures which is universally
accepted and a number of different protocols have been advocated. All of the
DNA specific stains and the phenanthridinium dyes have been used for total
DNA staining of chromosomes. The former group has the potential
disadvantage that UV excitation is required but this constitutes no problem
for mercury arc lamp based system or those with a laser tunable to UV lines
(Hartwell, 1998).
The DNA fluorochromes in current use were classified into groups.
Stains that intercalate with double stranded nucleic acid and include (PI),
(EB) and (AO);and DNA specific stains that have a particular specificity for
moieties
in
DNA
and
include
mithramiycin
(MMC),
ethedium
bromide/mithramicin (EB/MMC), a bisbenzimidazole derivative and 4-6
diamino-2- phenylindole (DAPI) (Taylor and Mithorpe, 1980).
Propidium iodide is bound to polynucleotide both by means of
intercalation. This is only affected to a limited extent by high ionic strengths
and electrostatically to secondary binding sites. The binding contents of these
later sites are greatly depending on the ionic strength of the medium and can
be eliminated by using sufficiently high ionic strengths. And also have
optimal excitation at a 488 nm laser and produce good results with RNAse
treatment (Hartwell, 1998).
1-2-Evaluation of DNA histogram:
75
The
DNA
histogram
is
a
very simple
data
set
which
characteristically contains two peaks separated by a trough Fig.
(4-1). The first peak, which is usually the larger, corresponds to cells with
G0/G1 DNA content and the second, which should be at double the
fluorescence intensity of the first, corresponds to cells with G2+M DNA
content. Any cell scored in the trough has a DNA content intermediate
between G1 and G2+M and these usually represent cells in S-phase. In a
perfect data set, which doesn't exist, all G1 and G2+M cells would be scored
in single channels and any cells between or immediately adjacent to these
would be in S- phase (Henderson, 1998).
Since the cell material always contained normal diploid cells such as
leukocytes or normal kidney cells, these were used as an internal standard
and regarded as diploid (2C) (Tribukati, 1984).
When in doubt, lymphocytes should be added to establish the diploid
DNA value. Human Ficol-prepared lymphocytes, fixed in ethanol, were used
as external standard. The magnitude of the signal was adjusted so as to have
the standard diploid peak in a certain channel. In necessary the illumination
was adjusted so that the coefficient of variation (CV) of the resulting
lymphocyte diploid peak was less than 3% Fig. (4-1). All cell population
with G1 maximum deviating less than 10% form the standard value were
regarded as diploid (Gustafson, 1982).
Only G0/G1 peak is observed in DNA diploid. A broad peak
described by a large coefficient of variation may obscure a second peak. The
coefficient of variation of the G0/G1 peak must be less than 5% for single
cell suspensions prepared from fresh/ frozen tissues, and less than 8% for
76
nuclear suspension prepared from fixed, paraffin embedded specimens.
Where a diploid peak only is observed, one should ensure that tumor cells are
present in the clinical sample analyzed (Weinberg, 1996).
77
Full width at half maximum(c-a)
C.V. = × ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ42.5%
Peak (or mean) channel(b)
Figure (4-1): Coeffecient of Variation (C.V.) (Gustafson, 1982).
An aneuploid cell population was considered to be present when a
distinct peak was found constituting at least 2.5% of the total cell material
and deviating more than 10% from the diploid standard. DNA aneuploid is
reported when at least two separate G0/G1 peaks are demonstrated. For some
samples the diploid normal peak might be almost non existent; hence care
should be taken to assign peaks (Ormerod, 1994).
The degree of ploidy of this cell line was calculated by relating the
G1 maximum of these cells to DNA of the diploid G1 cells which are always
present. These diploid cells can be leukocytes, fibroblasts, normal urothelial
cells.
2 channel of aneuploid peak
Degree of ploidy= ————————————
Channel number of diploid peak
The degree of aneuploid was determined also by the DNA index
which represents the ratio of fluorescence intensity of aneuploid cells to the
diploid cells. The DNA index of a diploid tumor is 1.0, whereas, aneuploid
78
tumors are designated by progressively higher indices (Götte, 2001 and
Gorden et al., 2003).
Estimation of the proportion of G1, S and G2+M cells made by
automatic integration of the cells in corresponding channels in the multi
channel analyzer. The values are corrected for background noise. To estimate
the proportions of cells in the S-phase of aneuploid tumor cell lines where
cells from the cell line coincide, the normal cell lines are subtracted.
Calculation of the phase distribution requires a minimum of about 1000 cells
combined with a low background noise resulting from cell fragments. These
calculations may also be rendered more difficult when the peaks for the
deploid or aneuploid cell population, partially or completely overlap. On the
other hand, there is no ambiguity in any of these cases to establish an
aneuploid cell line. An additional proof of the existence of an aneuploid
hyperdiploid cell line is the existence of a G2 peak occurs to the extreme
right of the histogram without interfering with the normal cell population
(Brown and Wittwer, 2000).
An aneuploid cell population with a tetraploid amount of DNA was
considered to exist when a peak exceeded the G2+ M peak found in normal
cells by three standard deviations or more. To quantitate the number of nuclei
normally found in the 4C or G2/ M peak, a number of control tissues were
studied. The mean percentage of nuclei in the 4C peak were 2.74+ 1.41
(standard deviation) for nuclei extracted from fresh normal lymphocyte.
These control data provide a firm basis for using greater than 10% of nuclei
in the 4C peak as a criterion for DNA polyploidy in the specimens
(Rabinovitch, 1994).
79
2- Immunophenotyping Applications:
The most common applications of flow cytometry are measurement
of DNA content in tumors and immunophenotyping of haematopoietic
malignancies. Flow cytometry has shown to be a suitable method for
immunophenotyping of canine lymphomas (Culmsee and Nalte, 2002).
Immunophenotyping of abnormal cells is now considered a
fundamental tool to establish the cell lineage assignment and to obtain a more
precise
identification
of
hematopathology depends
immunophenotyping
and
the
on
various
the
cell
applications
immunohistochemical
subtypes.
of
flow
Diagnostic
cytometric
immunophenotyping
combined with the cytomorphology and histologic features of cases. The
availability of monoclonal antibodies directed against the surface proteins
permits flow cytometric analysis of erythrocytes, leukocytes and platelets
(Brown & Wittwer, 2000, Chianese, 2002 and Dunphy, 2004).
Multiparameter flow cytometry with optimally selected antibody
combinations has expanded the use of this technique beyond traditional
applications in hematopathology. By analyzing qualitative patterns of antigen
expression on discrete populations
or "clusters," one can detect
immunophenotypic aberrancy in specific cell populations relative to normal
and reactive populations. Evaluation of patterns of antigen expression can
also be used to supplement conventional methodologies in the diagnosis and
subclassification of certain types of hematologic neoplasia. Finally, the
diagnosis of some congenital disorders affecting the hematolymphoid system
can be facilitated by the detection of characteristic immunophenotypic
changes (Kroft, 2004).
80
2-1-Erythrocyte analysis:
Tests that appear to have the greatest potential for routine
application of flow cytometry include reticulocyte and reticulated platelet
enumeration,
detection
of
erythrocyte-bound
immunoglobulin,
immunophenotyping of leukemias and lymphomas, and bone marrow
differential cell counting (Brown and Wittwer, 2000 , Weiss, 2002).
Flow cytometric methods were first applied to laboratory
hematology with the improvement in reticulocyte counting and the creation
of the immature reticulocyte fraction for better anemia evaluation and
therapeutic monitoring (Davis, 2001).
81
2-2-HIV monitoring:
More than 35 million people in developing countries are living with
HIV infection. While drug prices have dropped considerably, the cost and
technical complexity of laboratory tests essential for the management of HIV
disease, such as CD4 cell counts, remain prohibitive. New, simple, and
affordable methods for measuring CD4 cells that can be implemented in
resource-scarce settings are urgently needed (Dieye et al., 2005, Walker et
al., 2005 and Pattanapanyasat & Thakar, 2005).
2-3-Immunophenotyping of leukemias:
Immunophenotyping has become common in the diagnosis and
classification of acute leukemias and is particularly important in the proper
identification of cases of minimally differentiated acute myeloid leukemia.
To evaluate the immunophenotype of adult AML, cases were studied by
cytochemical analysis and by flow cytometry with a panel of antibodies
(Khalidi et al., 1998).
Characterization of leukemias by immunotyping is particularly
helpful when the morphology is difficult to interpret. The major advantage of
using immune markers by flow cytometry is the identification of particular
leukemia subtype, not recognized by morphologic criteria, which may have
prognostic significance (Rezaei et al., 2003).
Flow cytometric immunophenotypic analysis allowed to establish
diagnosis in cytomorphologically unclassified cases, identify acute mixedlineage leukemias (AMLL) with a frequency similar to that reported in other
series, and confirm the heterogeneity of acute leukemia (AL) (Piedras et al.,
1997 and Götte, 2001).
82
Flow cytometry may be used to detect minimal residual disease
(MRD) in acute lymphoblastic leukemia because leukemic cells often display
aberrant phenotypes when compared to normal cells. Flow cytometry is a
sensitive and specific method for detecting MRD of childhood ALL, and
could predict the coming relapse (Zhang et al., 2005).
With the advent of monoclonal antibodies and a uniform
nomenclature system defining antibody reactivity in terms of clusters of
differentiation (CD), an independent means of characterizing acute leukemias
using cellular antigen expression has evolved. Immunophenotyping is usually
performed using immunofluoresence technique and is complementary to the
light microscopic based morphologic classification. This is especially true of
the lymphoid leukemias where morphology and cytochemistry cannot
distinguish among different lineage of lymphoid cells, such as B versus T
cells. With Immunophenotyping lineage is assigned using a panel of
monoclonal antibodies that identify the expression of cell surface antigens.
The panel of monoclonal reagents must include antibodies reactive with both
myeloid and lymphoid cells to distinguish between the two most important
groups. The reactivity pattern of the leukemia cells for all reagents is then
examined for the final assignment of lineage: B- lymphoid, T- lymphoid,
myeloid or undifferentiated (Maslak et al., 1994).
Comparative studies of cell surface antigen expression between
normal and leukemic cells indicate that most if not all leukemias express
phenotypes that are not observed in most normal maturing cells. This
aberrant expression of cellular antigens suggests that leukemias are not
proliferations of cells arrested at one state of normal maturation; rather
leukemic cells maintain a genetic program that can produce expression of
83
antigens
of
any
lineage.
Nearly
all
laboratories
performing
immunofluoresence analysis use different reagents (Terstappen et al., 1991).
2-4-Quantification of stem cells:
100 years ago, hematopoietic stem cells were postulated as blood
lymphocyte-like cells. Within the last 20 years, the frequency of autologous
and allogeneic transplantation of hematopoietic stem cells has increased.
Hematopoietic growth factors allow the stem cells' mobilization from the
bone marrow into the peripheral blood. Quantification of these hematopoietic
stem cells by means of flow cytometry can be achieved within hours
(Goldschmidt et al., 2003).
Flow cytometry has become the major technique for the quality
control of stem cell-containing products such as apheresis concentrates, bone
marrow or cord blood (Grieson et al., 1995). Stem cells can be easily
identified with flow cytometry due to their unique characteristics. They
demonstrate a medium level of CD34 expression, a low level of CD45
expression and a low forward side scattered (Jennings & Foon, 1997 and
Maslak et al., 1994).
2-5-Platelet analysis:
The analysis of platelets by flow cytometry is becoming more
common in both research and clinical laboratories. Platelet-associated
immunoglobulin assays by flow cytometry can be direct or indirect assays,
similar to other platelet-associated immunoglobulin immunoassays. In
autoimmune thrombocytopenic purpura, free serum antibodies are not found
as frequently as platelet-bound antibodies (Ashman et al., 2003).
84
Immunofluorescent flow cytometry was used to measure the
percentage of activated platelet populations (CD62P, CD63), the percentage
of plt-monocyte aggregates (pma) (CD41/CD45), and activated monocytes
(CD11b, CD14, CD16) in the blood (Panasuik et al., 2005).
2-6-Testing for HLA-B27:
Human
leukocyte
antigen
B27
(HLA-B27)
is
a
major
histocompatibility complex class 1 molecule that is strongly associated with
the disease ankylosing spondylitis. The performance of the two flow
cytometric antigen assays depends on the antibody used and the positive
cutoff values assigned (Seipp et al., 2005). A flow cytometric HLA-B27 test
is much faster than the classical microcytoxicity test (Jennings and Foon,
1997 and Götte, 2001).
A biannual external quality assurance scheme for flow cytometric
typing of the HLA-B27 antigen is operational in The Netherlands and
Belgium since 1995. For flow cytometry, the most widely monoclonal
antibody used was FD705, followed by GS145.2 and ABC-m3. The majority
of laboratories used more than 1 anti-HLA-B27 monoclonal antibody for
typing (Seipp et al., 2005).
3- Major applications of apoptosis analysis:
There are many ways of detecting apoptosis by flow cytometry.
Apoptotic cells can be recognized by a characteristic pattern of
morphological (cell shrinkage, cell shape change, condensation of cytoplasm,
nuclear envelope changes, nuclear fragmentation, loss of cell surface
85
structures, apoptotic bodies, cell detachment and phagoctosis of remains),
biochemical and molecular changes (free calcium ion rise, bcl2/Bax
interaction, cell dehydration, loss of mitochondrial membrane potential,
proteolysis, phosphatidylserine externalization, lamin B proteolysis, DNA
denaturatuin, 50-300kb cleavage, intranucleosomal cleavage and protein
cross-linking (Hubank et al., 2004 and Liu et al., 2004).
The methods of detecting apoptosis by flow cytometry are based on
the measurement of light scatter, the detection of changes in the plasma
membrane, the analysis of cell organelles or the sensitivity of DNA to
denaturation (Sedlak et al., 1999).
3-1-Apoptosis light scatter:
As cells die or become apoptotic the refractive index of the internal
cytoplasm becomes more similar to that of the extracellular medium this
manifests itself as a reduction in forward scatter signal. At the same time,
intracellular changes and invagination of the cytoplasmic membrane lead to
an increase in side (or orthogonal or 90º) scatter. If a dead cell discriminatory
dye is added, cells that have become permeable can be identifying. In this
way low level resolution of dead and apoptotic cells can be get. A number of
dead cell dyes are available for use and the one used will depend on any other
fluorochromes that are being measured. Some examples are; Sytox Green
(488nm excitation; green fluorescence emission), Propidium Iodide (488nm
excitation; orange/red fluorescence emission), 7-Aminoactinomycin-D (7AAD) (488nm excitation; red fluorescence emission) and TO-PRO-3 (633nm
excitation; red fluorescence emission) (Cohen and Al-Rubeai, 1995).
86
3-2-Apoptosis DNA analysis:
During apoptosis, calcium and magnesium dependent nucleases are
activated which degrade DNA. This means that within the DNA there are
nicks and fragmentation. We can detect these in three ways using DNA
analysis to look at the sub G1 peak, using strand break labeling (TUNEL) to
detect broken DNA or using Hoechst binding to detect DNA conformational
changes (Majino and Joris, 1995).
The sub-G1 Fig. (4-2) method relies on the fact that after DNA
fragmentation, there are small fragments of DNA that are able to be eluted
following washing in either PBS or a specific phosphate-citrate buffer. This
means that after staining with a quantitative DNA –binding dye, cells that
have lost DNA will take up less stain and will appear to the left of the G1
peak. The advantage of this method is that it is very rapid and will detect
cumulative apoptosis and is applicable to all cell types (Darzynkiewicz,
1997).
However in order to be seen in the sub G1 area, a cell must have lost
enough DNA to appear there, so if cells enter apoptosis from the S or G2/M
phase of the cell cycle or if there is an aneuploid population undergoing
apoptosis, they may not appear in the sub G1 peak (Schwartz and Osborne,
1993).
87
Figure (4-2): Sub G1 peak by propidium iodide staining (Darzynkiewic,
1997).
88
Also cells that have lost DNA for any other reason e.g. death by some
other form of oncosis, will appear in the sub G1 region so we have to be
careful about how we define the sub G1 peak (Nicoletti et al., 2001).
3-3-Apoptosis cell membrane analysis:
In normal cells, phosphatidylserine (PS) residues are found in the
inner membrane of the cytoplasmic membrane. During apoptosis, the PS
residues are translocated in the membrane and are externalized. In general
though not always, this is an early event in apoptosis and is though to be a
signal to neighboring cells that a cell is ready to be phagocytosed (Robinson,
1993).
Annexin-V is a specific PS-binding protein that can be used to detect
apoptotic cells. Annexin V- is available conjugated to a number of different
fluorochromes. Early apoptotic cells are annexin positive but PI negative.
Because the cells aren't fixed we can exclude dead cells and it is possible to
add further markers if the cytometer set up are appropriate. As with all live
cell assays, we have to remember that we are only looking at a snapshot of
the cells as they are at time of analysis and generally all apoptotic
experiments should be performed over a time course; Fig. (4-3) (Telford et
al., 2004, Homburg et al., 1995 and Vermes at al., 1995).
89
Figure (4-3): Early apoptotic cells are annexin positive but (in this case)
PI (negative) (Telford et al., 2004).
90
Hoechst 33342 is a DNA-binding dye that is able to quantitatively
stain the DNA of live cells. However it has also been found that if the
concentration of Hoechst is low, the apoptotic cells take up the Hoechst more
rapidly. If we also add PI or TO-PRO-3 we can specifically identify the dead
cells. This is a rapid and quantitative method but requires the use of a UV
laser. The advantage of using TO-PRO-3 is that cell phenotyping using
FITC- and PE-labelled antibodies is also possible. Thymocytes labelled with
CD4-PE and CD8-FITC can be assessed for apoptosis using Hoechst and
TO-PRO-3 (Koopman et al., 1994).
A third way of assessing the membrane changes in apoptosis is to use
YO-PRO-1 (Molecular Probes). As this fluorochrome emits in the green, it
can be combined with propidium iodide to identify dead cells. The rationale
here is that cells in early apoptosis are unable to pump out YO-PRO-1 but are
still not permeable to other dead cells discriminatory dyes (Koopman et al.,
1994).
3-4-Apoptosis enzyme analysis:
Two genes (ced-3 and ced-4) were crucial to the process of
apoptosis. The ced-4 gene product has homologues in mammalian cells,
especially a family of cysteine proteases that are now known as caspases.
There are a number of caspases in mammalian cells that have been shown to
be involved in the early stages of apoptosis e.g. (caspase2, caspase3, caspase
6, caspase 9 and caspase 10). The functions of these enzymes are not yet
entirely clear but it appears that after an initial signal to the cell to undergo
apoptosis, they may be responsible for the activation, amplification and
execution of the apoptotic cascade (Cohen and Al- Rubeai, 1995).
91
Because of the central importance of the caspases in apoptosis, their
detection by flow cytometry has become widespread. We can detect the
activity of enzymes implicated in apoptosis in three ways; by detecting the
active form of the enzyme using a specific antibody (Smolewski et al., 2002),
by using a fluorochrome labelled peptide that binds to the active site of the
enzyme (Pozarowski et al., 2003) and by using a non-fluorescent substrate
for the enzyme which yields a fluorescent product if the enzyme is active
(Telford et al., 2004).
3-5-Apoptosis organelle analysis:
During apoptosis there is often a collapse of the mitochondrial
membrane potential. This can be detected in a number of ways by flow
cytometry. Two dyes in particular are useful- CMXRos (also known as Mito
tracker Red from Molecular probes) and LDs-751 (from Exction). CMXRos
has
a
chloromethyl
group
which
allows
accumulation
in
active
mitochondria. Live cells that have active mitchondria are able to take up
CMXRos but in cells that are undergoing apoptosis, the mitochondrial
membrane potential decreases which means less dye accumulates in the
mitchondria leading to a decrease in fluorescenc (Chapman et al., 1995).
4- Detection of apoptotic markers:
Determination of p53 expression by immunohistochemistry (IHC)
has been incorporated into routine practice and its reliability has been
consolidated. However, flow cytometric (FCM) analysis might represent an
important objective and rapid approach. FCM may provide important
information about p53 protein expression in the different subpopulations and
92
cell cycle phases. In most breast, lung, and colon aneuploid tumors (77%),
p53-positive cells were detected only in the subpopulations with abnormal
DNA content (Elvira et al., 1998).
Bovine papillomavirus type 1 (BPV-1)-transformed mouse fibroblast
cell lines were analyzed via flow cytometry (FCM) for expression of p53 and
c-myc proteins along with their DNA content. At least 9,000-10,000 p53 or
c-myc protein molecules per cell were detected in the transformed
tumorigenic cell lines. These results show that quantitative FCM can be
reliably used to detect very low levels (3,000 molecules per cell) of specific
protein, and FCM is a useful tool to study the virus-induced changes in the
levels of nuclear proteins within a cell population and in tumorigenesis
(Agrawal et al., 1994).
In human follicular lymphoma, Analysis of transgenic Bcl2
expression used biotinylated Bcl2-100 monoclonal antibody for the surface
phenotyping of hematopoietic cells by flow cytometry. Cells (106 per
analysis) were stained with relevant antibodies labeled with fluorochromes
(fluorescein isothiocyanate [FITC], phycoerythrin [PE], or cyanin 5 [Cy5]) or
biotin using 1% normal rat serum to block Fc receptors. Streptavidin
conjugated to FITC or PE was used as a secondary reagent for biotinylated
antibodies. Analyses were performed on a Life Sciences Research (LSR) or a
FACStar II flow cytometer (Becton Dickinson, San Jose, CA) (Alexander et
al., 2004).
The expression of bcl-2 was examined by multicolor flow
cytometry in samples including lymph node or other tissue biopsy specimens
93
containing follicular lymphoma (FL), reactive hyperplasia (RH), or other
malignant lymphomas, as well as bone marrow aspirates. For all of the
aforementioned reasons, a reliable flow cytometric assay for expression of
bcl-2 would be a useful additional technique for establishing a diagnosis of
FL. However, the measurement of bcl-2 by flow cytometric techniques has
received only scant attention. It was described a 2-color flow cytometric
assay using antibodies against bcl-2 that demonstrated promise in the
recognition of FL. (James et al., 2003).
94
V-Flourescence in situ hybridization
1-Introduction:
FISH provides researchers with a way to visualize and map the
genetic material in an individual's cells, including specific genes or portions
of genes. This is important for understanding a variety of chromosomal
abnormalities and other genetic mutations. Unlike most other techniques used
to study chromosomes, FISH does not have to be performed on cells that are
actively dividing. This makes it a very versatile procedure. The first step is to
prepare short sequences of single-stranded DNA that match a portion of the
gene the researcher is looking for. These are called probes. The next step is to
label these probes by attaching one of a number of colors of fluorescent dye
(Schröck et al., 1996 and Fox et al., 1996).
DNA is composed of two strands of complementary molecules that
bind to each other like chemical magnets. Since the researchers' probes are
single-stranded, they are able to bind to the complementary strand of DNA,
wherever it may reside on a person's chromosomes. When a probe binds to a
chromosome, its fluorescent tag provides a way for researchers to see its
location (White et al., 1995 and Bloom, 2005).
Fluorescent in situ hybridization (FISH) represents a modem
molecular pathology technique, alternative to conventional cytogenetics
(karyotyping). Fluorescence in situ hybridization (FISH) allows identification
95
of specific sequences in a structurally preserved cell, in metaphase or
interphase (Kontogeorgos, 2004 and Celedaet al., 1994).
The probe, bound to the target, will be developed into a fluorescent
signal. The fact that the signal can be detected clearly, even when fixed in
interphase, improves the accuracy of the results, since in some cases it is
extremely difficult to obtain mitotic samples Fig. (5-1) (Muhlmann, 2002).
The power of in situ hybridization can be greatly extended by the
simultaneous use of multiple fluorescent colors. Multicolor fluorescence in
situ hybridization (FISH), in its simplest form, can be used to identify as
many labeled features as there are different fluorophores used in the
hybridization. By using not only single colors, but also combinations of
colors, many more labeled features can be simultaneously detected in
individual cells using digital imaging microscopy (Raap et al., 1995).
Fluorescence, a phenomenon whereby a chemical excited at one
light wavelength emits light at a different and usually longer wavelength, is
used throughout the life sciences to study a wide variety of structures and
intracellular activities. Advances in probe and microscope technology have
led to the rapid development of techniques for fluorescence over the past
decade (Trask, 1991).
The accuracy of cytogenetic diagnosis in the management of
hematological malignancies has improved significantly over the past 10
years. Fluorescence in situ hybridization (FISH), a technique of molecular
cytogenetics, has played a pivotal role in the detection of unique submicroscopic chromosomal rearrangements that helped in the identification of
96
chromosomal loci, which contain genes involved in leukemogenesis (Amare
et al., 2001).
Figure (5-1): Fluoresence in situ hypridization (Muhlmann, 2002).
97
98
The use of FISH is growing rapidly in genomics, cytogenetics,
prenatal research, tumor biology, radiation labels, gene mapping, gene
amplification, and basic biomedical research. In principle, the technique is
quite straightforward (Attarbaschi et al., 2004).
The hybridization reaction identifies, or labels, target genomic
sequences so their location and size can be studied. DNA or RNA sequences
from appropriate, chromosome-specific probes are first labeled with reporter
molecules, which are later identified through fluorescence microscopy. The
labeled DNA or RNA probe is then hybridized to the metaphase
chromosomes or interphase nuclei on a slide. After washing and signal
amplification, the specimen is screened for the reporter molecules by
fluorescence microscopy (Hohman and Gundlach, 1994).
FISH probes are commonly used to detect the presence of specific
DNA sequences either when DNA is condensed into metaphase
chromosomes or dispersed in non dividing interphase cells. The fact that
hybridization of probes to metaphase chromosomes is visualized in two
dimensions while interphase targets are three dimensional has implications
for both validations of assays and the development of baseline reference
ranges (Pauletti et al., 1996).
Metaphase applications generally yield clear yes/no answers while
interphase applications commonly require reportable reference ranges before
interpreting of results. In addition to determining the presence or absence of
particular sequences in the genome, FISH is useful in assessing gene copy
number in some disorders (Massod et al., 1998).
99
Analytical uncertainty over DNA probe assays also may stem from
issues related to inherent population variation. The use of some repeat
sequence probes has been discontinued because of inability to detect targeted
sequences in individuals who possess very few repeats, leading to insufficient
probe label in the targeted region which precludes visualized of the signal.
Such probes have been eliminated (Myrata et al., 1997 and Bossuyt et al.,
1995).
FISH allows very precise spatial resolution of morphological and
genomic structures. The technique is rapid, simple to implement, and offers
great probe stability. The genome of a particular species, entire
chromosomes,
chromosomal-specific
regions,
or
single-copy
unique
sequences can be identified, depending on the probes used (Attarbaschi et
al., 2004).
Until recently, FISH was limited by the hardware, software,
reagents, probe technology, and cost involved in implementing the technique.
Commercially available microscope hardware optimized for multicolor FISH
was not available until the mid-1990s. Prior to that, microscopes had to be
customized for FISH applications. Most microscope optics was not designed
to detect the low light levels inherent in FISH signals. As the genomic
resolution of the technique has increased dramatically, the requirements on
microscope optics have further increased. Chromatic aberrations among
multiple wavelengths have been a problem. For multicolor analysis in
particular, all lenses, including the collector lens, had to be chromatically
corrected. In addition, epi-fluorescence light sources were difficult to align
for uniform illumination (Amare et al., 2001).
100
Analysis of multicolor FISH images requires isolation of the various
signals either with individual filter cubes; or utilization of an excitation filter
wheel with multipass dichroic and barrier filters. Recent developments in
filter technology corrected some of the previous problems encountered
through optical misalignments caused by mechanical switching of individual
filter cubes. Excitation filter wheels used with multi-pass dichroic and barrier
filters can be used effectively for up to three colors by employing separate
excitation filters for each color with no registration shift. But, for more than
three colors, single-pass filters still had to be used (Racevskis, 2005, Iarovaia
et al., 2005 and Iourov et al., 2005).
2-Three different types of FISH probes:
2-1-Locus specific probes
They bind to a particular region of a chromosome. This type of
probe is useful when scientists have isolated a small portion of a gene and
want to determine on which chromosome the gene is located (Hjalmar, 2005
and Wang et al., 2005).
2-2-Alphoid or centromeric repeat probes
They are generated from repetitive sequences found in the middle of
each chromosome. Researchers use these probes to determine whether an
individual has the correct number of chromosomes. These probes can also be
used in combination with "locus specific probes" to determine whether an
individual is missing genetic material from a particular chromosome
(Edward et al., 2005).
101
2-3-Whole chromosome probes
They are actually collections of smaller probes, each of which binds
to a different sequence along the length of a given chromosome. Using
multiple probes labeled with a mixture of different fluorescent dyes,
scientists are able to label each chromosome in its own unique color. The
resulting full-color map of the chromosome is known as a spectral karyotype.
Whole
chromosome
probes
are
particularly useful
for
examining
chromosomal abnormalities, for example, when a piece of one chromosome
is attached to the end of another chromosome (Dugan et al., 2005).
3-Applications of FISH:
The clinical uses of FISH were considered in three main areas;
diagnosis of individuals with birth defects and mental retardation, prenatal
diagnosis and screening, and identification and monitoring of acquired
chromosome abnormalities in leukemia/ cancer. In each area the critical
consideration remains a clear understanding of the capabilities and
limitations of a test to provide useful information (Bossuyt et al., 1995 and
Pauletti et al., 1996).
Traditional cytogenetic analysis, detecting deletions, duplications,
rearrangement and the identifications of unknown material of marker or
derivative chromosomes, in individuals with birth defects and/or mental
retardation has led to an understanding of the etiology of a number of
syndromes. The clinical utility and limitations of these tests are both general
and disease specific (Ledbeteer et al., 1987, Callen et al., 1992, Ribeiro et
al., 1997 and Cassidy et al., 1998).
102
Prenatal applications of FISH testing include both screening tests
and diagnostic tests. Technical issues are few, and clinical utility raises
questions as to the intended use of FISH in testing. The application of FISH
to prenatal screening for common autosomal trisomies and sex chromosome
anomalies is becoming increasingly common. The primary considerations
involve differing clinical sensitivity between the abnormalities detected by
classical cytogenetic versus these detected by FISH based assays (Evans et
al., 1991 and Klinger et al., 1992).
Among cases ascertained via ultrasonographically identified fetal
anomalies, some may be conclusive for a syndromes diagnosis and may be
approached by a (diagnostic) FISH test. Families in which subtle or
submicroscopic chromosomal abnormalities, detectable by FISH, are known
to segregate will benefit greatly from prenatal FISH studies (Kontogeorgos et
al., 2000 and Lewin et al., 2000).
Fluorescence in situ hybridization (FISH) has become one of the
major techniques in environmental microbiology. The original version of this
technique often suffered from limited sensitivity due to low target copy
number or target inaccessibility (Zwirglmaier, 2005).
The reagents and probes themselves were not sufficient for all
applications. For instance, the efficiency of hybridization site detection
decreased with decreasing probe size, creating significant limits to what
could be observed via fluorescence microscopy. The number of differently
colored fluorescent dyes was limited, and the photostability of the dyes was
poor. But new developments in fluorescent dye technology and spin-off
technology from the federally funded Human Genome Project are now
103
having an impact. There are probes for all the human chromosomes and a
growing number of new gene-specific probes are available. In situ
hybridization kits and fluorescently labeled probes are commercially
available from several companies (Sarrate et al., 2005).
The ability of FISH to rapidly test interphase and metaphase
chromosome defects makes it especially useful in the study of cancer. In
solid tumors, conventional cytogenetics is rarely used because obtaining
metaphases is difficult and those cells that do proceed to mitosis may not be
representative of the tumor. Other molecular techniques, such as PCR and
Southern, Northern, and Western analysis, require extraction of the tissue.
Extraction procedures net both normal and abnormal cells, so sensitivity is
lower and quantitation less reliable than with FISH probes (Bosch et al.,
2005).
FISH allows cell-by-cell analysis and thus provides for a more
sensitive and reliable assessment of chromosomal aneuploidy, gene
amplifications and deletions, and chromosome translocations. A reliable
determination of whether a gene is amplified in a specimen is often possible
with evaluation of only 20 to 50 cells (Ogilvie et al., 2005).
The accuracy of cytogenetic diagnosis in the management of
hematological malignancies has improved significantly over the past 10
years. FISH has played a pivotal role in the detection of unique submicroscopic chromosomal rearrangements that helped in the identification of
chromosomal loci, which contain genes involved in leukemogenesis (Amare
et al., 2001).
104
FISH was performed with specific probes to make the rapid prenatal
diagnosis of Down syndrome. FISH was performed respectively with locusspecific probe (LSI) and centromeric probe (CEP) X/Y on the uncultured
amniotic fluid. FISH is a rapid and reliable method to detect Down syndrome
in uncultured amniotic fluid (Wang et al., 2005)
Fluorescence in situ hybridization assay and to correlate the genetic
findings with the pathologic grade and stage were used to investigate the
chromosomal abnormalities present in bladder carcinoma (Placer et al.,
2005).
A novel application of FISH to isolated nuclei is described. The
method detects gene amplification and chromosome aneuploidy in extracted
nuclei from paraffin-embedded tissue of human cancer with greater
sensitivity and specificity than existing FISH methods. The method is applied
to signal detection of the HER-2/neu (c-erbB-2) gene, whose amplification is
one of the most common genetic alterations associated with human breast
cancer (Rossi et al., 2005).
Tumor-specific chromosomal abnormalities are attracting a large
interest owing to the diagnostic, prognostic, and therapeutic importance. The
development of FISH has improved the detection of specific chromosomal
abnormalities in chronic lymphocytic leukemic (CLL). By using FISH, the
problem with tumor cells with low mitotic rate is avoided since this method
readily detects clonal aberrations also in nondividing, interphase cells. Three
different types of probes are used centromeric probes for numerical
chromosome abnormalities, whole chromosome paints, and locus-specific
105
probes for numerical chromosome abnormalities, whole chromosome paints,
and locus-specific probes. (Hjalmar, 2005)
FISH of DNA-DNA or DNA-RNA using post-mortem brain samples
is one approach to study low-level chromosomal aneuploidy and selective
expression of specific genes in the brain of patients with neuropsychiatric
diseases. FISH could be applied to extended studies of chromosomal
aneuploidy, abnormal patterns of chromosomal organization and functional
gene expression in situ in the neurons of the brain in different psychiatric and
neurodevelopmental diseases (Yurov et al, 2001).
3-1-ALL investigation by FISH:
To investigate patients with acute lymphoblastic leukemia (ALL) for
TEL/AML1 fusion, BCR/ABL fusion, MLL gene rearrangements, and
numerical changes of chromosomes 4, 10, 17 and 21 by fluorescence in situ
hybridization (FISH) and to determine the relationship and the significance of
those findings (Zhang et al., 2003).
Interphase fluorescence in situ hybridization (iFISH) is increasingly
used for the identification of BCR/ABL gene rearrangements in chronic
myeloid leukemia (CML) and acute lymphoblastic leukemia (ALL). FISH
plays an important role in detecting chromosome changes, especially in some
cryptic chromosome translocations and patients with culture failures (Primo
et al., 2003 and Zhang et al., 2003).
ALL blasts
routinely contain
somatically acquired
genetic
abnormalities that provide insight into pathogenesis and strongly influence
prognosis. Approximately one third of cases of ALL show an increase in the
106
modal chromosome number (e.g., hyperdiploid, > 47 chromosomes, and
"high" hyperdiploid, > 50 chromosomes) blasts make up a unique biologic
subset associated with increased in vitro apoptosis and sensitivity to a variety
of chemotherapeutic agents (Heerema et al., 2000 and Trueworthy et al.,
1992).
Almost one third of ALL blasts show chromosomal translocations in
the absence of changes in chromosome number. Four major translocations
have been observed, and each defines a unique biological subset of patients.
The t(1;19)(q23;q13) is a hallmark of some pre-B (cytoplasmic µ+) ALL, and
is characterized by fusion of the E2A and PBX genes (Uckun et al., 1998).
Despite the adverse prognostic impact of this translocation in older
studies, recent intensification of therapy has resulted in an improved survival
for these children. Translocations between the mixed lineage leukemia (MLL)
gene at 11q23 and over 30 different partner chromosomes characterize 6% of
ALL cases. MLL translocations, most commonly t(4;11)(q21;q23), are seen in
the vast majority of infant patients with ALL. A recent, large series
demonstrates that any rearrangement of 11q23 is associated with a worse
prognosis (e.g., 20% to 25%) (Pui et al., 2002).
3-1-1-Philadelphia
The presence of the t(9;22)(q34;q11) translocation, commonly
known as Philadelphia chromosome (Ph), in about 3% to 5% of all children
with ALL is considered as one of the molecular markers associated with a
particularly high risk for treatment failure (Ribeiro et al., 1987, Crist et
al.,1990, Pui et al., 1990, Fletcher et al., 1991, Reiter et al., 1994, and
Chessells et al., 1995) .
107
This
translocation causes
a
rearrangement
between
the
protooncogene c-ABL and a gene called the breakpoint cluster region (BCR).
Whereas the breaks in c-ABL occur mainly in the same region (between the
exons a1 and a2) on chromosome 9, two different ones affect the breakpoint
cluster region on chromosome 22: the more frequent one (approximately in
2 of 3 of all cases) shows a break in the minor breakpoint cluster region (mBCR) between the exons e1 and e2. This is predominant in ALL. In 1 of 3 of
all Ph+ ALL cases, the major (M-) BCR found between exons b2 and b3 or
exons b3 and b4 is affected. M-BCR is also found in nearly all patients with
chronic myelogenous leukemia (CML). Chimeric proteins of 210 kD (p210)
and 190 kD (p190) result from the M-BCR/ABL and m-BCR/ABL
rearrangements, respectively (Kantarjian et al., 1991).
These fusion proteins cause a deregulation of protein tyrosine kinase
activity. Both forms of the chimeric gene (BCR/ABL) can be detected by
polymerase chain reaction (PCR) and fluorescent in situ hybridization.
(Maurer et al., 1991, Dewald et al., 1993, Schlieben et al., 1996).
Most patients with Philadelphia (Ph)-positive acute lymphoblastic
leukemia (ALL) show evidence of secondary chromosome aberrations that
may influence the course of disease and response to treatment. To better
understand how these secondary chromosomal aberrations occur and to
investigate whether the p185/p190 BCR-ABL fusion protein may directly
induce an increased chromosomal instability and subsequently the
appearance of clonal chromosome aberrations, three BRC-ABL (p185/
p190)-transduced mouse pre-B cell lines were analyzed by spectral
karyotyping and fluorescence in situ hybridization. The human wild-type
108
BCR-ABL gene was expressed at a level comparable with that in human Phpositive leukemias at diagnosis. All BCR-ABL-transduced cell lines acquired
similar clonal chromosomal aberrations. Trisomy 5 was always present,
followed by loss of the Y chromosome, trisomy of chromosomes 12 and 18,
and an unbalanced translocation between chromosomes X and 12. Thus,
ectopic p185/p190 BCR-ABL expression, such as p210 BCR-ABL, PMLRARA, or C-MYC transduction, may induce an increased chromosomal
instability leading to clonal karyotypic evolution, which may mimic
secondary chromosome aberrations in human Ph-positive ALL (Rudolph et
al., 2005).
The Philadelphia (Ph) chromosome, the main product of the
(9;22)(q34;q11) translocation, is the cytogenetic hallmark of chronic myeloid
leukemia (CML), a clonal myeloproliferative disorder of the hematopoietic
stem cell; the Ph chromosome is also found in a sizeable portion of acute
lymphoblastic leukemia (ALL) patients and in a small number of acute
myeloid leukemia (AML) cases. Three different breakpoint cluster regions
are discerned within the BCR gene on chromosome 22: M-bcr, m-bcr, and
mu-bcr (Drexler et al., 1999).
Nearly all Ph + ALL cell lines have the m-bcr e1-a2 fusion gene
(only two ALL cell lines have a b3-a2 fusion) whereas all CML cell lines, but
one carry the M-bcr b2-a2, b3-a2 or both hybrids. The mu-bcr e19-a2 has
been detected in one CML cell line. Four cell lines display a three-way
translocation involving chromosomes 9, 22 and a third chromosome.
Additional Ph chromosomes (up to five) have been found in four Ph + ALL
cell lines and in 18 CML cell lines; though in some cell lines the extra Ph
chromosome(s) might be caused by the polyploidy (tri- and tetraploidy) of
109
the cells. Another modus to acquire additional copies of the BCR-ABL fusion
gene is the formation of tandem repeats of the BCR-ABL hybrid as seen in
CML cell line K-562. Both mechanisms, selective multiplication of the
der(22) chromosome and tandem replication of the fusion gene BCR-ABL,
presumably lead to enhanced levels of the fusion protein and its tyrosine
kinase activity (genetic dosage effect). The availability of a panel of Ph + cell
lines as highly informative leukemia models offers the unique opportunity to
analyze the pathobiology of these malignancies and the role of the Ph
chromosome in leukemogenesis (Drexler et al., 1999).
Treated children with acute lymphoblastic leukemia were analysed
for chromosomal abnormalities with conventional G-banding, spectral
karyotyping (SKY) and interphase fluorescent in situ hybridisation (FISH)
using probes to detect MLL, BCR/ABL, TEL/AML1 rearrangements and
INK4 locus deletions. Three novel TEL partner breakpoints on 1q41, 8q24
and 21p12 were identified, and a recurrent translocation t(1;12)(p32;p13) was
found. In addition, two cases displayed amplification (7-15 copies) of AML1.
Results were demonstrated the usefulness of SKY and interphase FISH for
the identification of novel chromosome aberrations and cytogenetic
abnormalities that provide prognostically important information in childhood
ALL (Nordgren et al., 2002).
The BCR/ABL and MLL/AF4 fusion genes--resulting from
t(9;22)(q34;q11) and t(4;11)(q21;q23) translocations, respectively--are
considered as a high risk prognostic factors in children with acute
lymphoblastic leukaemia (ALL). Their presence in malignant cells indicates
patient for the most intensive antileukaemic therapy regardless of the other
criteria. In contrast, the most common non-random chromosomal aberration
110
in paediatric ALL--translocation t(12;21)(q12;q22)--is associated with a
favourable prognosis. The examination of these rearrangements is important
for the stratification of patients to the risk groups and also provides the most
sensitive and specific tool for minimal residual disease (MRD) follow-up
(Trka et al., 1999 and Poplack, 1993).
VI- References
Abu-Absi NR, Zamamiri A, Kacmar J, Balogh SJ, Srienc F, (2003).
Automated flow cytometry for acquisition of time-dependent
population data. Cytometry A., 51(2):87-96.
Adachi A, Sato S, Sasaki Y, Ghazizadeh M, Maeda M, Kaizu K, Liu XL,
Fukunaga Y, (2005). Electron microscopic studies on the
occurrence of activated neutrophils in peripheral blood of children
with acute leukemias. J Submicrosc Cytol Pathol., 37(1):13-8.
Agrawal RS, Agrawal YP, Mantigarvi RA, (1994). Flow cytometric
quantitation of C-myc and P53 proteins in bovine papillomavirus
type 1-transformed primary mouse fibroblasts. Cytometry,
1;17(3):237-45.
Albro J, Bauer KD, Hitchcock CL, Wittwer CT, (1993). Improved DNA
content histograms from formaline-fixed Paraffin embedded liver
tissue by protinase K digestion. Cytometry, 14:673-678.
111
Alexander E, Alan W, Mary L, (2004). VavP-Bcl2 transgenic mice
develop follicular lymphoma preceded by germinal center
hyperplasia. Blood, 103(6): 2276-2283.
Amare PS, Baisane C, Saikia T, Nair R, Gawade H, Advani S, (2001).
Fluorescence in situ hybridization: a highly efficient technique of
molecular diagnosis and predication for disease course in patients
with myeloid leukemias. Cancer Genet Cytogenet., 131(2):12534.
Amati B, Alevizopoulos K, Vlach J, (1998). Myc and the cell cycle. Front
Biosci., 3:D250–D268.
Aricò M, Valsecchi MG, Camitta B, (2000). Outcome of treatment in
children
with
Philadelphia
chromosome-positive
acute
lymphoblastic leukemia. N Engl J Med., 342 (14): 998-1006.
Ashman N, Macey MG, Fan SL, Azam U, Yaqoob M, (2003). Increasedplateletmonocyte aggregates and cardiovascular disease in endstage
renal
failure
patients.
Nephrol
Dial
Transplant.,
18(10):2088-96
Assuncao P, Diaz R, Comas J, de Galarreta CM, Gonzalez-Llamazares OR,
Poveda JB, (2005). Evaluation of Mycoplasma hyopneumoniae
growth by flow cytometry. J Appl Microbiol., 98(5):1047-54.
Attal M, Blaise D, Marit G, (1995). Consolidation treatment of adult acute
lymphoblastic
comparing
leukemia:
allogeneic
a
prospective,
versus
autologous
randomized
bone
trial
marrow
transplantation and testing impact of recombinant Ll-2 after
autologous bone marrow transplantation. Blood, 86(4): 16191628.
112
Attarbaschi A, Mann G, Konig M, Dworzak MN, Trebo MM, Muhlegger N,
Gadner H, Haas OA, (2004). Austrian Berlin-Frankfurt-Munster
cooperative study groupIncidence and relevance of secondary
chromosome abnormalities in childhood TEL/AML1+ acute
lymphoblastic leukemia: an interphase FISH analysis. Leukemia,
18(10):1611-6.
Balduzzi A, Valsecchi MG, Uderzo C, De Lorenzo P, Klingebiel T, Peters C,
Stary J, Felice MS, Magyarosy E, Conter V, Reiter A, Messina
C, Gadner H, Schrappe M, (2005). Chemotherapy versus
allogeneic transplantation for very-high-risk childhood acute
lymphoblastic leukaemia in first complete remission: comparison
by genetic randomisation in an international prospective study.
Lancet; 366(9486):635-42.
Bassan R, Lerede T, Di Bona E, (1997). Granulocyte colony-stimulating
factor (G-CSF, filgrastim) after or during an intensive remission
induction therapy for adult acute lymphoblastic leukemia: Affects,
role of patient pretreatment characteristics, and costs. Leuk.
Lymphoma, 26(1-2): 153-161.
Benn DE and Robinson BG, (1996). Peripheral blood mononuclear cells are
a reliable internal standard for the flow cytometric DNA analysis
for frozen malignant brast biopsies. Cytometry, 15 (26) 161-165.
Bijangi-Vishehsaraei K, Saadatzadeh MR, Werne A, Wilson McKenzie KA,
Kapur R, Ichijo H, Haneline LS, (2005). . Enhanced TNF{alpha} induced apoptosis in Fanconi anemia type C deficient
cells is dependent on apoptosis signal-regulating kinase 1. Blood,
18 (23):543-6.
113
Blom HJ, (2000). Genetic determinants of hyperhomocysteinaemia: the roles
of
cystathionine
beta-synthase
and
5,10-
methylenetetrahydrofolate reductase. Eur J Pediatr., 159(3):S208–
S212.
Bloom K, (2005). Chromosome segregation: seeing is believing. Curr Biol.,
15(13):R500-3.
Bogh LD and Duling TA, (2005). Demonstration of a germinal center
immunophenotype in lymphomas by immunocytochemistry and
flow cytometry. Methods Mol Med., 115:65-91.
Bosch P, Catalina F, Corrales T, Peinado C, (2005). Fluorescent probes for
sensing processes in polymers. Chemistry, 11(15):4314-25.
Bossuyt P, Van Tienen M, Dumon J, (1995). Incidence of low fluorescence
alpha satellite region on chromosome21 escaping detection of
aneuploidy at interphase by FISH . Cytogenet Cell Genet., 68:
203-206.
Brown M and Wittwer C, (2000). Flow cytometry: Principles and clinical
applications in Hematology. Clincal Chem., 46:1221-1229.
Buckbinder L, (1997). The p53 tumor suppressor targets a novel regulator of
G protein signaling. Proc Natl Acad Sci USA., 94; 7868–7872.
Burger B, Zimmermann M, Mann G, (2003). Diagnosis cerebrospinal fluid
examination in children with acute lymphoblastic leukemia:
significance of low leukocyte count with blasts or traumatic
lumber puncture. J Clin Oncol., 21(2):184-188.
Burn JH, Finney DT, Goodwine LG, (1952). Biological standardization. 2nd
ed. University Press Oxford, p.32
114
Callen D, Eyre H, Yip M, Freemantle C, Haan E, (1992). Molecular
cytogenetic and clinical studies of 42 patients with marker
chromosomes. Am J Med Genet; 43: 709-715.
Carolyn S, Richard G, Samuel M, Mark S, Mel F, Roger C, Sally H,
(2002). Detecting Small-Area Similarities in the Epidemiology of
Childhood Acute Lymphoblastic Leukemia and Diabetes BMJ;
324:283–7
Carroll L, Deepa B, Dong-Joon M, Elizabeth R, Mary R, Stella D, James
R, Ceryl L, John C, (2003). Pediatric Acute Lemphoblastic
Leukemia. Hematology., (1):102-131
Cassidy S, Schwartz S, (1998). Prader- Willi and Angelman syndromes
disorders of genomic imprinting. Medicin, 77: 140-151.
Celeda D, Aldinger K, Haar FM, Hausmann M, Durm M, Ludwig H,
Cremer C, (1994). Rapid fluorescence in situ hybridization with
repetitive DNA probes: quantification by digital image analysis.
Cytometry, 17(1):13-25.
Champlin R and Gale R, (1989). Acute lymphoblastic leukemia. Recent
advances in biology therapy. Blood, 73:2051-2066.
Chapman RS, Chresta CM, Herberg AA, (1995). Further characterization
transferase (TdT) assay for the flow cytometric analysis of
apoptosis in drug resistant and drug sensitive leukemic cells.
Cytometry, 20:245-256.
Charrin C, Thomas X, Ffrench M, (2004). A report from the LALA-94 and
LALA-SA groups on hypodiploidy with 30 to 39 chromosomes
and near-triploidy: 2 possible expressions of a sole entity
conferring poor prognosis in adult acute lymphoblastic leukemia
(ALL). Blood 104 (8): 2444-51.
115
Chatzimeletiou K, Makrydimas G, Sotiriadis A, Paraskevaidis E, Nicolaides
KH, (2005). Aneuploidy screening in coelomic samples using
fluorescence in situ hybridisation (FISH). Prenat Diagn, 15;
(3)196-202.
Chen CL, Liu Q, Relling MV, (1996). Simultaneous characterization of
glutathione S-transferase M1 and T1 polymorphisms by
polymerase chain reaction in American whites and blacks.
Pharmacogenetics, 6:187–191.
Chessells JM, Bailey C, Richards SM, (1995). Intensification of treatment
and survival in all children with lymphoblastic leukaemia: results
of UK Medical Research Council trial UKALL X. Medical
Research Council Working Party on Childhood Leukaemia.
Lancet, 345 (8943): 143-8.
Chessells JM, Harrison CJ, Watson SL, (2002). Treatment of infants with
lymphoblastic leukaemia: results of the UK Infant Protocols 19871999. Br J Haematol, 117 (2): 306-14.
Chianese R, Brando B, Gratama JW, (2002). European Working Group on
Clinical Cell AnalysisDiagnostic and prognostic value of flow
cytometric immunophenotyping in malignant hematological
diseases. J Biol Regul Homeost Agents, 16(4):259-69.
Choi SJ, Lee JH, Lee JH, Kim S, Lee YS, Seol M, Ryu SG, Lee JS, Kim
WK, Jang S, Park CJ, Chi HS, Lee KH, (2005). Treatment of
relapsed acute lymphoblastic leukemia after allogeneic bone
marrow transplantation with chemotherapy followed by G-CSFprimed donor leukocyte infusion: a prospective study. Bone
Marrow Transplant, 36(2):163-9.
116
Cledat D, Batta S, Mokrinin R, Cardot P, (2004). Rice starch granule
characterization
by
hyphenated with
flow
cytometry
scattering
techniques
sedimentation field-flow fractionation. J
Chromatogr A, 1049(1-2):131-9.
Cohen J and Al-Rubeai M, (1995). Apoptosis- targeted therapies the next
big thing in biotechnology?Trends.Biotechno.,13:281-283.
Cory S and Adams JM, (2002). The Bcl2 family: regulators of the cellular
life-or-death switch. Nat Rev Cancer, 2(9):647-56.
Crist W, Carroll A, Shuster J, Jackson J, Head D, Borowitz M, Behm F,
Link M, Steuber P, Ragab A, Hirt A, Brock B, Land V, Pullen J
(1990). Philadelphia chromosome positive childhood acute
lymphoblastic leukemia: Clinical and cytogenetic characteristics
and treatment outcome. A Pediatric Oncology Group study.
Blood, 76:489-499
Cryns V and Yuan Y, (1999). Proteases to die for. Genes Dev., 12:1551–
1570.
Culmsee K and Nolte I, (2002). Flow cytometry and its application in small
animal oncology. Methods Cell Sci., 24(1-3):49-54.
Darke CH and Dyer P, (1992). Clinical HLA typing by cytoxicity. In:
"Histocomptability testing-A practical Approach" (Dyer P and
Middleton D. eds.) Oxford University Press, p, 51-80
Darzynkiewicz Z, (1997). Cytometry in cell necrobiology: analysis of
apoptosis and accidental cell deth (necrosis).Cytometry, 27:1-20.
Davis BH, (2001). Diagnostic utility of red cell flow cytometric analysis.
Clin Lab Med., 21(4):829-40.
Davis EG, Wilkerson MJ, Rush BR, (2002). Flow cytometry: clinical
applications in equine medicine. J Vet Intern Med., 16(4):404-10.
117
Dean PN, (1985). Recent advances in high performance liquid affinity
chromatography columns. Biochem Soc Trans., 13(6): 1055-8.
Dean PN and Jett JH, (1974). Mathematical analysis of DNA distributions
derived from flow microfluorometry. J. Cell. Biol., 60:52.
de Franchis R, Fermo I, Mazzola G, (2000). Contribution of the
cystathionine beta-synthase gene (844ins68) polymorphism to the
risk of early-onset venous and arterial occlusive disease and of
fasting hyperhomocysteinemia. Thromb Haemost., 84:576–582.
Del Gazio V, Brown J, Certo M, Novina C, Letai A, (2007). Chronic
lymphocytic leukemia requires BCL2 to sequester prodeath BIM,
explaining sensitivity to BCL2 antagonist ABT-737. J Clin
Invest., 117(1):112-21.
Dewald GW, Schad CR, Christensen ER, (1993). Fluorescence In Situ
Hybridization with X and Y Chromosome Probes for Cytogenetic
Studies
on
Bone
Marrow
Cells
after
Opposite
Sex
Transplantation. Bone Marrow Transplantation, 12:149154.
Dieye TN, Vereecken C, Diallo AA, Ondoa P, Diaw PA, Camara M, Karam
F, Mboup S, Kestens L, (2005). Absolute CD4 T-cell counting in
resource-poor settings: direct volumetric measurements versus
bead-based clinical flow cytometry instruments. J Acquir Immune
Defic Syndr., 39(1):32-7.
Dirven HA, Megens L, Oudshoorn MJ, Dingemanse MA, Van Ommen B,
van Bladeren PJ, (1995). Glutathione conjugation of the
cytostatic drug ifosfamide and the role of human glutathione Stransferases. Chem Res Toxicol., 8:979–986.
118
Donadieu J and Hill C, (2001). Early response to chemotherapy as a
prognostic factor
in childhood acute lymphoblastic leukemia
methodological review. Br J Haematol., 115(1): 34-35.
Dördelmann M, Reiter A, Borkhardt A, (1999). Prednisone response is the
strongest predictor of treatment outcome in infant acute
lymphoblastic leukemia. Blood, 94 (4): 1209-17.
Drexler HG, MacLeod RA, Uphoff CC, (1999). Leukemia cell lines: in vitro
models for the study of Philadelphia chromosome-positive
leukemia. Leuk Res., 23(3):207-15.
Dugan LC, Pattee MS, Williams J, Eklund M, Sorensen K, Bedford JS,
Christian
AT,
(2005).
Polymerase
chain
reaction-based
suppression of repetitive sequences in whole chromosome
painting probes for FISH. Chromosome Res., 13(1):27-32.
Dunphy
CH,
(2004).
Applications
of
flow
cytometry
and
immunohistochemistry to diagnostic hematopathology. Arch
Pathol Lab Med., 128(9):1004-22.
Durrant I, Prentico H, Richard S, (1997). Intensification of treatment for
adults with acute lymphoblastic Leukemia: results of U.K.
Medical Research Council randomized trial UKALL XA. Medical
Research Council Working Party on Leukemia in Adults. Br J
Haematol., 99(1): 84-92.
Duque RE, Andreeff M, Braylan BC, Diamond LW, Peiper SC, (1993).
Consensus review of the clinical utility of DNA flow cytometry in
neoplastic hematopathology. Cytometry, 14:492-496.
Edward NS and Murray AW, (2005). Identification of xenopus CENP-A and
an associated centromeric DNA repeat. Mol Biol Cell.,
16(4):1800-10.
119
Elisabeth S, Edward T, Michele B, Michèle O, Anne E, David H, (1999).
Increased apoptosis induction by 121F mutant p53. The EMBO
Journal; 18: 4424-4437.
Elledge S, (1996). Cell cycle. Science 274: 1664-1672.
Elvira B, Aurora C, Gabriella A, Rosella S, (1998). p53 Expression in
Human Carcinomas: Could Flow Cytometry Be an Alternative to
Immunohistochemistry.
Journal
of
Histochemistry
and
Cytochemistry, 46: 41-48
Evan G and Littlewood T, (1998). A matter of life and cell death. Science,
281:1317–1322.
Evans M, Ebrahim S, Beery S,Holzgreve W, Isada N, Quintero R, Johnson
M, (1991). Fluorescence in situ hybridization utilization for- high
risk prenatal diagnosis: a trade-off among speed, expense, and
inherent limitations of chromosome specific probes. Am J Obstet
Genycol., 1055-1057.
Evans WE, Pui CH, Campanan D, (2002). Childhood acute lymphoblastic
leukaemia--current status and future perspectives. Lancet Oncol.,
(10):597-607.
Facchini LM and Penn LZ, (1998). The molecular role of Myc in growth
and transformation: recent discoveries lead to new insights.
FASEB J., 12:633–651.
Fadok VA, Voelker DR, Campbell PA, Cohen JJ, Bratton DL, Henson PM,
(1992). Exposure of phosphatidylserine on the surface of
apoptotic lymphocytes triggers specific recognition and removal
by macrophages. J. Immunol. 148: 2207.
Fatih M, Uckun M, Zhiwen Y, Harland S, Peter S, James N, Bruce B, Lisa
C, Mireille S, Onur Ek, Tamer Z, David T, Gregory R, and Paul
120
G, (1997).
Cellular
Oncoprotein
in
Expression
Newly
of
Antiapoptotic
BCL-2
Childhood
Acute
Diagnosed
Lymphoblastic Leukemia: A Children's Cancer Group Study
Blood, 89 (15): 3769-3777.
Fletcher JA, Lynch EA, Kimball VM, Donnelly M, Tantravahi R, Sallan
SE, (1991). Translocation (9;22) is associated with extremely
poor prognosis in intensively treated children with acute
lymphoblastic leukemia. Blood, 77:435.
Flores ER, Tsai KY, Crowley D, Sengupta S, Yang A, McKeon F, Jacks T
(2002). p63 and p73 are required for p53-dependent apoptosis in
response to DNA damage. Nature 416: 560-564.
Fouad M, Maher R, Hala A, Amal Z, Saed S, (2002). Flow cytometric
analysis of nuclear DNA ploidy and proliferative activity in acute
lymphoblastic leukemia. J. Egyptian Nat. Cancer Inst., 14(4):303310.
Fox JL, Hsu P-H, Legator MS, (1995). "Fluorescence In Situ Hybridization:
Powerful Molecular Tool for Cancer Prognosis. Clin Chem.,
41:15541559.
Franchini
G,
(1995).
Molecular
mechanisms
of
human
T-cell
leukemia/lymphotropic virus type I infection. Blood, 86:36193639.
Frankel LS, Ochs J, Shuster JJ, (1997). Therapeutic trial for infant acute
lymphoblastic
leukemia:
the
Pediatric
Oncology
Group
experience (POG 8493). J Pediatr Hematol Oncol., 19 (1): 35-42.
Gala JL, Vermylen C, Cornu G, Ferrant A, Michaux JL, Philippe M,
Martiat P, (1994) High expression of bcl-2 is the rule in acute
lymphoblastic
leukemia,
except
in
Burkitt's
subtype
at
121
presentation, and is not correlated with the prognosis. Ann
Hematol, 69:17.
Gascoyne RD, Adomat SA, Krajewski S, Krajewski M, Horsman DE,
Ticher AW, O'Reilly SE, Hoskins P, Coldman AJ, Reed JC,
Connors JM, (1997): Prognostic significance of BCL2 protein
expression and BCL2 gene rearrangement in diffuse aggressive
non-Hodgkin's lymphoma. Blood, 90:244.
Gerbaulet A, Hartmann K, Mekori Y, (2005). A Mast cell apoptosis.
Methods Mol Biol., 315:407-24.
Gerstner AO, Tarnok A, Bootz F, (2005). Slide-based multi-parametric
cytometry in ENT HNO, 53(2):134-41
Goldschmidt H, Egerer G, Fruehauf S, Ho AD, (2003). Stem cells in
hematology and oncology. Med Klin (Munich), 98 (l 2):11-4.
Gorden KM, Duckett L, Dual B, Petri HT, (2003). A simple method for
detecting up to five immuno fluorescent parameters together with
DNA staining for cell cycle or viability on a bench top flow
cytometry. J. Immunol. Methods, 275:113-121.
Goto Y, Yue L, Yokoi A, (2001). A novel single-nucleotide polymorphism in
the 3'-untranslated region of the human dihydrofolate reductase
gene with enhanced expression. Clin Cancer Res., 7:1952–1956.
Götte R, (2001). Clinical applications of flow cytometry. Clinical lab.,
brassels, Belgim, C.L.I., p.12-13.
Goukon Y, Sasano H, Nishihira T, Nagura H, Mori S (1994). p53
overexpression in human esophageal carcinoma: a correlation
with tumor DNA ploidy and two parameter flow cytometric study.
Anticancer Res., 14:1305-1312
Greaves MF, (1997). Aetiology of acute leukaemia. Lancet 349:344-349.
122
Green DR, Reed JC, (1998). Mitochondria and apoptosis. Science,
281:1309–1312.
Grierson H, Wooldridge T, Hess M, Ratashak A, Bast M, Armitage J,
Sanger W, (1995). Comparison of DNA content in non-Hodgkin's
lymphoma as measured by flow cytometry and cytogenetics.
Cancer Genet. Cytogenet, 80:124-128.
Guo J, Luan P, Li ZQ, (2005). Clinical analysis of 120 cases of
malignancies with nosocomial infections. Di Yi Jun Yi Da Xue
Xue Bao., 25(7):802-4.
Gustafson H, (1982). DNA analysis by flow cytometry in carcinoma of the
urinary bladder. Cytometry, 12(3):224-32
Hann I, Vora A, Harrison G, (2001). Determinants of outcome after
intensified therapy of childhood lymphoblastic leukaemia: results
from
Medical
Research
Council
United
Kingdom
acute
lymphoblastic leukaemia XI protocol. Br J Haematol 113 (1):
103-14.
Hartwell EA, (1998). Use of RH immune globulin: ASCP practice
parameter. Am. J. Clin. Pathol., 110: 281-92.
Hecker S, Sauerbrey A, Volm M, (1994). p53 expression and poor prognosis
in childhood acute lymphoblastic leukemia. Anticancer Res.,
14(6B):2759-61
Heerema NA, Sather HN, Sensel MG, (2000). Prognostic impact of
trisomies of chromosomes 10, 17, and 5 among children with
acute lymphoblastic leukemia and high hyperdiploidy (> 50
chromosomes). J Clin Oncol., 18(9):1876–1887
Heerema NA, Harbott J, Galimberti S, (2004). Secondary cytogenetic
aberrations in childhood Philadelphia chromosome positive acute
123
lymphoblastic leukemia are nonrandom and may be associated
with outcome. Leukemia, 18 (4): 693-702.
Henderson LO, Marti GI, Gaigalas A, Hannon WH, Vogt JR-RF, (1998).
Termenology and nomenclature for standardization in quantitative
fluroscence cytometry. Cytometry, 33(2):97-105.
Hermeking H, (2003). The MYC oncogene as a cancer drug target. Curr
Cancer Drug Targets., 3(3):163-75.
Hermine O, Haioun C, Lepage E, dÕAgay MF, Briere J, Lavignac C, Fillet
G, Salles G, Marolleau JP, Diebold J, Reyas F, Gaulard P,
(1996) Prognostic significance of bcl-2 expression in agressive
non-Hodgkin's lymphoma. Groupe d'Etude des Lymphomes de
l'Adulte (GELA). Blood 87:265.
Hjalmar V, (2005). Sequential fluorescence in situ hybridization analysis for
trisomy 12 in B-cell chronic lymphocytic leukemia. Methods Mol
Med., 115:231-40.
Hohman B and Gundlach H, (1994). Multichannel fluorescence microscopy
and optoelectronic imaging. Biomedical Products, 13: 42-44.
Homburg CH, de Haas M, von dem Borne AE, Verhoeven AJ,
Reutelingsperger CP, Roos D, (1995). Human neutrophils lose
their surface Fc gamma RIII and acquire Annexin V binding sites
during apoptosis in vitro. Blood, 85: 532.
Hougardy BM, van der Zee AG, van den Heuvel FA, Timmer T, de Vries
EG, de Jong S, (2005). Sensitivity to Fas-mediated apoptosis in
high-risk HPV-positive human cervical cancer cells: relationship
with Fas, caspase-8, and Bid. Gynecol Oncol., 97(2):353-64.
124
Hubank M, Bryntesson F, Regan J, Schatz D, (2004). Cloning of apoptosisrelated genes by representational difference analysis of cDNA.
Methods Mol Biol., 282:255-73.
Hui L, Qing L, Julie O, Friederike K, Michelle M, Michael H, (2005). cMyc rapidly induces acute myeloid leukemia in mice without
evidence of lymphoma-associated antiapoptotic mutations. Blood,
106(7): 2452-2461.
Iarovaia OV, Akopov SB, Nikolaev LG, Sverdlov ED, Razin SV, (2005).
Induction of transcription within chromosomal DNA loops
flanked by MAR elements causes an association of loop DNA
with the nuclear matrix. Nucleic Acids Res., 26; 33(13):4157-63.
Illoh OC, (2004). Current applications of flow cytometry in the diagnosis of
primary immunodeficiency diseases. Arch Pathol Lab Med.,
128(1):23-31.
Ingrid K, Paul W, Hui Yang, Corina M, Lindsey M, John L, Jeffery T,
(1999). Epstein-Barr Virus Regulates c-MYC, Apoptosis, and
Tumorigenicity in Burkitt Lymphoma. Mol Cell Biol., 19(3):
1651–1660.
Ionov Y, Yamamoto H, Krajewski S, Reed JC, Perucho M,(2000).
Mutational inactivation of the pro-apoptotic gene BAX confers
selective advantage during tumor clonal evolution. Proc Natl
Acad Sci USA., 97:10872–10877.
Iourov IY, Soloviev IV, Vorsanova SG, Monakhov VV, Yurov YB, (2005).
An approach for quantitative assessment of fluorescence in situ
hybridization (FISH) signals for applied human molecular
cytogenetics. J Histochem Cytochem, 53(3):401-8.
125
Isabella A, Murali R, Paul S, William D, (2000). Calpain Inhibitor 1
Activates p53-dependent Apoptosis in Tumor Cell Lines. Cell
Growth & Differentiation, 11: 247-253.
Jacks T and Weinberg R, (1996). Cell-cycle control and its watchman.
Nature 381: 643-644.
James R, Fiona E, Steven H, (2003). bcl-2 Expression by Multicolor Flow
Cytometric Analysis Assists in the Diagnosis of Follicular
Lymphoma in Lymph Node and Bone Marrow. Am J Clin Pathol.,
119(1):145-151
Jaroszeski MJ and Radcliff GF, (1999). Fundamentals of flow cytometry.
Mol Biotechnol., 11(1):37-53.
Jeffrey M, (2005) Acute lymphoblastic leukemia. Am J Clin Pathol.,
124:445-452
Jennings C and Foon K, (1997). Recent advances in flow cytometry.
Application to the diagnosis of hematologic malignancy. Blood,
90:2863-2892.
Jiang M and Milner J, (2003). Regulation of Bcl-2 expression by
dihydrotestosterone in hormone sensitive LNCaP-FGC prostate
cancer cells. J Urol., 169(4):1553-7.
Kannan K, Kaminski N, Rechavi G, Jakob-Hirsch J, Amariglio N, Givol D,
(2001). DNA microarray analysis of genes involved in p53
mediated apoptosis: activation of Apaf-1. Oncogene 20, 34493455.
Kantarjian HM, Talpaz M, Dhingra K, Estey E, Keating MJ, Ku S, Trujillo
J, Huh Y, Stass S, Kurzrock R, (1991). Significance of the P210
versus P190 molecular abnormalities in adults with Philadelphia
chromosome-positive acute leukemia. Blood, 78:2411.
126
Kandathil AJ, Kannangai R, David S, Nithyanandam G, Solomon S,
Balakrishnan P, Abraham OC, Subramanian S, Rupali P,
Verghese VP, Pulimood S, Sridharan G, (2005). Comparison of
Microcapillary Cytometry Technology and Flow Cytometry for
CD4+ and CD8+ T-Cell Estimation. Clin Diagn Lab Immunol.,
(8):1006-9.
Kazak AE, Barakat LP, Meeske K, Christakis D, Meadows AT, Casey R,
Penati B, Stuber ML, (1997). Posttraumatic stress, family
functioning, and social support in survivors of childhood leukemia
and their mothers and fathers. J Consult Clin Psychol., 65:120129.
Khalidi HS, Medeiros LJ, Chang KL, Brynes RK, Slovak ML, Arber DA,
(1998). The immunophenotype of adult acute myeloid leukemia:
high frequency of lymphoid antigen expression and comparison of
immunophenotype, French-American-British classification, and
karyotypic abnormalities. Am J Clin Pathol., 109(2): 211-20.
Khalifa AS, El-Kardani TA, Fayek MH, Abd El-Ghaffar AA, Sabry F,
Nossair O, (1999). Flow cytometric study childhood acute
lymphoblastic leukemia immunophenotyping and DNA analysis.
The Egypt. J Haematol., 22(1,2): 1-23.
Khandakar MR, Roy K, Mukherjee S, Talukdar A, (2005). Philadelphia
chromosome positive essential thrombocythemia with dilated
cardiomyopathy. J Assoc Physicians India., 53:568-70.
Keeney M, Barnett D, Gratama JW, (2004). Impact of standardization on
clinical cell analysis by flow cytometry. J Biol Regul Homeost
Agents, 18(3-4):305-12.
127
Kishi S, Griener JC, Cheng C, (2003). Homocysteine, pharmacogenetics,
and neurotoxicity in children with leukemia. J Clin Oncol.,
21:3084–3091.
Klinger K, Landes G, Shook D, Harrey R, Lopez L, Locke P, Lerner T,
Osathanadh R, Leverone B, Houseal T, Pavelka K, Dackowski
W, (1992). Rapid detection of chromosome aneuploidies in
uncultured amniocytes by using fluorescence in situ hybridization
(FISH). Am J Hum Genet., 51: 55-65.
Ko LJ and Prives C, (1996). p53: puzzle and paradigm. Genes Dev. 10:
1054–1072.
Kontogeorgos G, (2004). Molecular cytogenetics of pituitary adenomas,
assessed by FISH technique. Front Horm Res., 32:205-16.
Kontogeorgos G, (2000). The Art and Applications of Fluorescence In Situ
Hybridization in Endocrine Pathology. Endocr Pathol. Summer,
11(2):123-136.
Koopman G, Reutelingsperger P, Kuijten M, Keehne J, Pals T, and van
Oers M (1994). Annexin V for flow cytometric detection of
phosphatidylserine expression on B cells undergoing apoptosis.
Blood, 84: 1415.
Kramer M, Hermans J, Wijburg E, Philippo K, Geelen E, Krieken J,
Maartense E, Schuuring E, and Kluin P (1998). Clinical
Relevance of BCL2, BCL6, and MYC Rearrangements in Diffuse
Large B-Cell Lymphoma Blood, 92 (9) 3152-3162.
Krawczuk-Rybak M and Wysocka J, (2005). Renal function during and after
treatment for acute lymphoblastic leukemia in children. Padiatr
Nephrol., 20(6): 782-5.
128
Kroemer G, Reed JC, (2000). Mitochondrial control of cell death. Nat Med.,
6:513–519.
Kroft SH, (2004). Role of flow cytometry in pediatric hematopathology. J
Clin Pathol., 122 Suppl:S19-32.
Lam HK, Chik KW, Yan M, Liu M, Liu VC, Li CK, Fok TF, Ng PC, Shing
MM, (2005). Arsenic trioxide mediates intrinsic and extrinsic
pathways of apoptosis and cell cycle arrest in acute leukemia. Int J
Oncol., 27(2):537-45
Lanzkowsky P, (2000). Leukemia in Manual of Pediatric Hematology and
oncology, Academic press, London, 3:359-409.
Ledbetter D, Greenberg F, Hohn V, Cassidy S, (1987). Conference report;
Second Annual Prader-Willi Scientific conference. Am J Med
Genet., 28:779-798.
Levine AJ (1997). p53, the cellular gatekeeper for growth and division. Cell,
88: 323–331.
Lewin P, Kleinfinge R, Bazin A, Mossafa H, Szpiro-Tapia S, (2000).
Defining the efficiency of FISH on uncultured amniocytes on a
retrospective cohort of 27,407 prenatal diagnosis. Prenat. Diagn.,
20:1-6.
Liblit RL, (1993). Guidelines for implementation of clinical DNA cytometry.
Cytometry, 14:472.
Lichtman MA, (1995). Acute myelogenous leukemia. In: Williams
Hematology (Beutler E, Lichtman MA, Coller BS, Kipps TJ, eds).
New York:McGraw-Hill., 272-298.
Lin HP, Ng SM, Ariffin WA, Zainab AK, Lam SK, Chan LL , (2000). Age,
sex, haemoglobin level, and white cell count at diagnosis are
important prognostic factors in children with acute lymphoblastic
129
leukemia treated with BFM-type protocol. J Trop Pediatr.,
46(6):338-43.
Linda J and Carol P, (1996). p53: puzzle and paradime. Genes &
Development, 10: 1054-1072.
Linet MS, Hatch EE, Kleinerman RA, Robison LL, Kaune WT, Friedman
DR, Severson RK, Haines CM, Hartsock CT, Niwa S, (1997).
Residential exposure to magnetic fields and acute lymphoblastic
leukemia in children. N Engl J Med., 337:1-7.
Liu H, Lin N, Tu Y, Liu Z, Huang C, (2004). Correlation between the
expression of Fas, Bcl-2 in peripheral blood lymphocytes and the
level of IFN-gamma, IL-4 in serum of patients with condyloma
acuminate. J Huazhong Univ Sci Technolog Med Sci., 24(1):90-1.
Look AT, Roberson PK, Williams DL, Rivera G, Bowman WP, Pui CH,
Ochs J, Dahl G and Kawinsky D, (1986). Prognostic importance
of blast cell DNA content in childhood acute lymphoblastic
leukemia. Blood, 65: 1079-1086.
Look AT, Melvin SL, Williams DL, Brodeur GM, Dahl GV, Kalwinsky DK,
Murphy SB, Mauer AM, (1996). Aneuploidy and percentage of
S-phase cells determined by flow cytometry correlate with cell
phenotype in childhood acute leukemia. Blood, 60:959- 68.
Longobardi-Given A, (1992). Flow cytometry. 1st ed wiley Liss, New York.
Lu ZX, Ye M, Yan GR, Li Q, Tang M, Lee LM, Sun LQ, Cao Y, (2005).
Effect of EBV LMP1 targeted DNAzymes on cell proliferation
and apoptosis. Cancer Gene Ther., 12(7):647-54.
Majino G and Joris, (1995). Apoptosis, oncosis and necrosis. An Overview
of cell death. Am.J. Pathol., 146:3-16
130
Makin G, Hickmann J, (2000). Apoptosis and cancer chemotherapy. Cell
Tissue Res., 301:143.
Malempati S, Tibbits D, Akkari Y, Oslan S, Fan G (2006). Aberrant
stabilization of c-Myc protein in some lymphoblastic leukemias.
Leukemia, 20(9):1572-81.
Martin C, Richard G, Nozomu T, Vivette D, Marie T, (2002). c-myc induced
Apoptosis in Polycystic Kidney Disease Is Independent of
FasL/Fas Interaction. Cancer Research, 62: 2210-2214.
Maslak P, Hegewisch-Becker S, Godfret L, AndreefM, (1994). Flow
cytometric determination of the multidrug-resistant phenotype in
acute leukemia. Cytometry, 17:84-93.
Massod S, Bui M, Yung J , Mark H and yang S, (1998). Reproducibility of
LSIHER-2/neu Spectrum Orange and CEP 17 spectrum Green
dual color deoxy ribonucleic acid probe kit. Ann Clin Lab Sci.,
28: 215-223.
Mateyak M K, Obaya A J, Adachi S, Sedivy J M, (1997). Phenotypes of cMyc-deficient rat fibroblasts isolated by targeted homologous
recombination. Cell Growth Differ., 8:1039–1048.
Maung ZT, MacLean FR, Reid MM, Pearson ADJ, Proctor SJ, Hamilton
PJ, Hall AG, (1994) The relationship between bcl-2 expression
and response to chemotherapy in acute leukemia. Br J Haematol
88:105.
Maurer J, Janssen JWG, Thiel E, van Denderen J, Ludwig W-D, Aydemir
Ü, Heinze B, Fonatsch C, Harbott J, Reiter A, Riehm H,
Hoelzer D, Bartram CR (1991). Detection of chimeric BCR/ABL
genes in acute lymphoblastic leukaemia by the polymerase chain
reaction. Lancet, 337:1055.
131
McCoy JP, (2002). Basic principles of flow cytometry. Hematol Oncol Clin
North Am., 16(2):229-43.
McCurrach ME, Connor TM, Knudson CM, Korsmeyer SJ and Lowe SW
(1997). bax-deficiency promotes drug resistance and oncogenic
transformation by attenuating p53-dependent apoptosis. Proc Natl
Acad Sci USA., 94: 2345–2349.
Meijer AE, Jernberg AR, Heiden T, Stenerlow B, Persson LM, Tilly N,
Lind BK, Edgren MR, (2005). MRDose and time dependent
apoptotic response in a human melanoma cell line exposed to
accelerated boron ions at four different LET. Int J Radiat Biol.,
81(4):261-72.
Melamed MR, Lindmo T and Mendelsohn M, (1990). Flow cytometry and
sorting, 2nd edition New York: Wiley-Liss.
Menendez P, Vargas A, Bueno C, Barrena S, Almeida J, De Santiago M,
Lopez A, Roa S, San Miguel JF, Orfao A, (2004). Quantitative
analysis of bcl-2 expression in normal and leukemic human B-cell
differentiation. Leukemia, 18(3):491-8.
Miyashita T and Reed JC (1995). Tumor suppressor p53 is a direct
transcriptional activator of the human bax gene. Cell, 80: 293–29.
Moorman AV, Richards SM, Martineau M, (2003). Outcome heterogeneity
in childhood high-hyperdiploid acute lymphoblastic leukemia.
Blood, 102 (8): 2756-62.
Moorman AV, Richards SM, Robinson AH, Strefford HJ, Gibson BE,
Harison
JC, (2006).
lymphoblastic
Prognosis
leukaemia
(ALL)
of
children with
and
acute
intrachromosomal
amplification of chromosome 21 (iAMP21) Blood, 9:153-9
132
Morgenbesser S, Williams B, Jacks T, DePinho R, (1994). p53-dependent
apoptosis produced by Rb-deficiency in the developing mouse
lens. Nature 371: 72-74
Motyka B, Korbutt G, Pinkoski MJ, (2000). Mannose 6-phosphate/insulinlike growth factor II receptor is a death receptor for granzyme B
during cytotoxic T cell-induced apoptosis. Cell, 103:491–500.
Muhlmann M, (2002). Molecular cytogenetics in metaphase and interphase
cells for cancer and genetic research, diagnosis and prognosis.
Application in tissue sections and cell suspensions. Genet Mol
Res., 1(2):117-27.
Myrata H, Kusuzaki K, Hirasawa Y, Inazawa J, Abe T, Ashihara T, (1997).
Ploidy
analysis
in
paraffin-embedded
malignant
fibrous
histiocytoma by DNA cytofluorometry and flourescence in situ
hybridization. Cancer Lett., 118(1):123-8.
Nakase K, Tsuji K, Nagaya S, Tamaki S, Tanigawa M, Ikeda T, Miyanishi
E, Shiku H, (2005). Acute interstitial pneumonitis during
chemotherapy for haematological malignancy. Eur J Cancer Care
(Engl), 14(4):336-41.
Nasmyth K, (1996). The cell cycle Science 274:1643-1645.
Nicoletti I, Mannucci R, Riccardi C, Grignani F, (2001). Common method
for measuring apoptotic cell death by flow cytometry. Purdue
cytometry CD-ROM series, 3: 1-9
Niu G, Wright KL, Ma Y, Wright GM, Huang M, Irby R, Briggs J, Karras
J, Cress WD, Pardoll D, Jove R, Chen J, Yu H, (2005). Role of
Stat3 in Regulating p53 Expression and Function. Mol Cell Biol.,
25(17):7432-40.
133
Nordgren A, Heyman M, Sahlen S, Schoumans J, Soderhall S,
Nordenskjold M, Blennow E, (2002). Spectral karyotyping and
interphase
FISH
reveal
abnormalities
not
detected
by
conventional G-banding. Implications for treatment stratification
of childhood acute lymphoblastic leukaemia: detailed analysis of
70 cases. Eur J Haematol. Jan; 68(1):31-41.
Norusis MJ, (2006). Statistical package for social sciences (SPSS) bare 12.0
for windows users Gide. Chicago IL:SPSS.
Ogilvie CM, Braude PR, Scriven PN, (2005). Preimplantation genetic
diagnosis--an overview. J Histochem Cytochem., 53(3):255-60.
Orfao A, Ruiz-Arguelles A, Lacombe F, Ault K, Basso G, Danova M,
(1995). Flow cytometry. Its applications in
hematology.
Hematologica, 80: 69-81.
Ormerod MG, (1994). Flow cytometry: A practical Approach. 2nd ed. IRI
Press Oxford UK.
Ormerod MG, Tribukait B, Giarretti W, (1998). Consensus report of the task
force on standardization of DNA flow cytometry in clinical
pathology. Anal. Cell Pathol., 17:103-110
Oshikawa T, Okamato M, Ahmed S, Tano T, (2006). The relationship
between gene expression of Bcl-2 and Bax and the therapeutic
effect in oral cancer patients. Cancer, 33(12):1723-5.
Owens MA and Loken MR, (1995). Flow cytometric principles for clinical
laboratory practice. Wiley-Liss New York.
Owen-Schaub LB et al. (1995). Wild-type human p53 and a temperaturesensitive mutant induce Fas/APO-1 expression. Mol Cell Biol.,
15: 3032–3040.
134
Panasiuk A, Zak J, Kasprzycka E, Janicka K, Prokopowicz D, (2005).
Blood platelet and monocyte activations and relation to stages of
liver cirrhosis. World J Gastroenterol., 11(18): 2754-8.
Parikh PV, Ashokkumar MS, Pai SK, Redkar A, Chopra HK, Barbhya SA,
Gopal R, Mittra I and Advani SH, (1995). Prognostic
significance of DNA index by flow cytometry in acute
lymphoblastic leukemia. J. Med. Res., 102:24-27.
Parks D and Henzenberg L, (1989). Flow cytometry and fluorescence
activated cell sorting . In: fundamental immunology (Paul, W.,
ed), Raven, New York.
Pattanapanyasat K and Thakar MR, (2005). MRCD4+ T cell count as a tool
to monitor HIV progression & anti-retroviral therapy. Indian J
Med Res., 121(4):539-49.
Pauletti G, Godolphin W, Press M, Slamon J, (1996). Detection and
quantitation of HER-2/neu gene amplification in human breast
cancer archival material using FISH. Oncogene, 13:63-72
Pemble S, Schroeder KR, Spencer SR, (1994). Human glutathione Stransferase theta (GSTT1): cDNA cloning and the characterization
of a genetic polymorphism. Biochem J., 300:271–276.
Pezzella F, Tse AGD, Cordell JL, Pulford KAF, Gatter KC, Mason DY,
(1990). Expressionof the bcl2 oncogene protein is not specific for
the 14;18 chromosomal translocation. Am J Pathol., 137: 225-32.
Philip J, (2002). Basic principles of flow cytometry. Hematol Oncol Clin
North Am., 16(2): 229-34.
Piedras
J,
Lopez-Karpovitch
X,
Cardenas
MR,
(1997).
Cellular
immunophenotypes in 97 adults with acute leukemia. Rev Invest
Clin., 49(6):457-64.
135
Pietilainen T, Lipponen P, Aaltomaa S, Eskelinen M, Kosma VM, Syrjanen
K, (1995). Expression of c-myc proteins in breast cancer as related
to established prognostic factors and survival. Anticanc Res.,
15:959.
Pinto AE, Fonseca I, Soares J, (2002). DNA flow cytrometry in solid
tumors. Acta Med Port., 15(2):133-42.
Placer J, Espinet B, Salido M, Sole F, Gelabert-Mas A, (2005). Correlation
between histologic findings and cytogenetic abnormalities in
bladder carcinoma: a FISH study. Urology, 65(5):913-8.
Poliseno L, Mariani L, Collecchi P, Piras A, Zaccaro L, Rainaldi G,
(2002). Bcl2- negative MCF7 cells overexpress p53: implications
for the cell cycle and sensitivity to cytotoxic drugs. Cancer
Chemother Pharmacol., 50(2):127-30.
Polyak K, Xia Y, Zweier JL, Kinzler KW and Vogelstein B (1997). A model
for p53-induced apoptosis. Nature, 389: 300–305.
Poplack DG, (1993). Acute lymphoblastic leukemia. In: Principles and
Practice of Pediatric Oncology (Pizzo PA, Poplack DG, eds).
Philadelphia:J.B., 431-481.
Porter PL, Gown AM, Kramp SG, Coltrera MD (1992). Widespread p53
overexpression in human malignant tumors. Am J Pathol 140:145153.
Pozarowski P, Huang X, Halicka DH, Lee B, Johnson G, Darzynkiewicz Z,
(2003). ZInteractions of fluorochrome-labeled caspase inhibitors
with apoptotic cells: a caution in data interpretation. Cytometry
A., 55(1):50-60.
Prendergast G, (1999). Mechanisms of apoptosis by c-myc. Oncogene.,
18(19):2967-87.
136
Primo D, Tabernero MD, Rasillo A, Sayagues JM, Espinosa AB, Chillon
MC, Garcia-Sanz R, Gutierrez N, Giralt M, Hagemeijer A, San
Miguel JF, Orfao A, (2003). Patterns of BCR/ABL gene
rearrangements by interphase fluorescence in situ hybridization
(FISH) in BCR/ABL+ leukemias: incidence and underlying
genetic abnormalities. Leukemia, 17(6):1124-9.
Pui CH, (1995). Childhood leukemias. N Engl J Med 332:1618-1630.
Pui CH, Boyett JM, Relling MV, (1999). Sex differences in prognosis for
children with acute lymphoblastic leukemia. J Clin Oncol., 17 (3):
818-24.
Pui CH, Campana D, Evans WE, (2001). Childhood acute lymphoblastic
leukaemia–current status and future perspectives. Lancet Oncol., 2
(10): 597-607.
Pui CH, Chessells JM, Camitta B, (2003). Clinical heterogeneity in
childhood
acute
lymphoblastic
leukemia
with
11q23
rearrangements. Leukemia, 17 (4): 700-6.
Pui CH, Crist WM, Look AT (1990). Biology and clinical significance of
cytogenetic abnormalitites in childhood acute lymphoblastic
leukemia. Blood, 76:1449.
Pui CH and Evans WE, (1998). Acute lymphoblastic leukemia. N Engl J
Med., 339 (9): 605-15.
Pui CH, Gaynon PS, Boyett JM, (2002). Outcome of treatment in childhood
acute lymphoblastic leukaemia with rearrangements of the 11q23
chromosomal region. Lancet., 359(9321):1909–1915.
Pullen J, Shuster JJ, Link M, (1999). Significance of commonly used
prognostic factors differs for children with T cell acute
lymphocytic leukemia (ALL), as compared to those with B-
137
precursor ALL. A Pediatric Oncology Group (POG) study.
Leukemia, 13 (11): 1696-707.
Raap T, (1995). Editorial: Cytometry for CGH, Cytometry, 19; 1-3.
Racevskis J, (2005). Molecular diagnosis of cancer: methods and protocols,
second edition. Med Oncol., 22(3):325-6.
Radcliff G, Jaroszeski MJ, (1998). Basics of flow cytometry. Methods
MolBiol., 91:1-24
Rabinovitch H, (1993). Practical consideration for DNA content and cell
cycle analysis. In: "Clinical flow cytometry: Principles and
applications" Baltimore. Williams and Wilkins, p. 77-142
Rampino N, Yamamoto H, Ionov Y, Li Y, Sawai H, Reed JC and Perucho
M, (1997). Somatic frameshift mutations in the BAX gene in
colon cancers of the microsatellite mutator phenotype. Science,
275; 967–969
Rautonen J, Siimes MA, (1988). Elevated serum transaminase activity at
diagnosis is associated with rapidly progressing disease in
children with acute lymphoblastic leukemia Cancer, 61(4):754-7.
Reaman GH, Sposto R, Sensel MG, (1999). Treatment outcome and
prognostic factors for infants with acute lymphoblastic leukemia
treated on two consecutive trials of the Children's Cancer Group. J
Clin Oncol., 17 (2): 445-55.
Reckenwald D, (1993). Introduction to flow cytometry: principles
fluorochromes instrument setup, calibration. J. Hematother., 2:
387-410.
Reed JC, (1995). Bcl2 family proteins: Regulators of chemoresistance in
cancer. Toxicol Lett., 82:155.
138
Reid T, Baldini A, Rand T, Ward D, (1992). Simultaneous visualization of
seven different DNA probes by in situ hybridization using
combinatorial fluorescence and digital imaging microscopy,
Proceedings of the National Academy of Sciences (PNAS), 89:
1388-1392.
Reiter A, Schrappe M, Ludwig WD, Hiddemann W, Sauter S, Henze G,
Zimmermann M, Lampert F, Havers W, Niethammer D,
Odenwald E, Ritter J, Mann G, Welte K, Gadner H, Riehm H
(1994). Chemotherapy in 998 unselected childhood acute
lymphoblastic leukemia patients. Results and conclusions of the
multicenter trial ALL-BFM 86. Blood, 84 (9): 3122-33.
Rezaei A, Adib M, Mokarian F, Tebianian M, Nassiri R, (2003). Leukemia
markers expression of peripheral blood vs bone marrow blasts
using flow cytometry. Med Sci Monit., 9(8):CR359-62.
Ribeiro RC, Abromowitch M, Raimondi SC, Murphy SB, Behm F,
Williams DL (1987). Clinical and biologic hallmarks of the
Philadelphia chromosome in childhood acute lymphoblastic
leukemia. Blood, 70:948.
Ribeiro RC, Broniscer A, Rivera GK, (1997). Philadelphia chromosomepositive acute lymphoblastic leukemia in children: durable
responses to chemotherapy associated with low initial white blood
cell counts. Leukemia, 11 (9): 1493-6.
Robinson JP, (1993). Hand Book of Flow cytometry Methods. Wiley-Liss
New York.
Roederer M Rodriguez WR, Christodoulides N, Floriano PN, Graham S,
Mohanty S, Dixon M, Hsiang M, Peter T, Zavahir S, Thior I,
Romanovicz D, Bernard B, Goodey AP, Darzynkiewicz Z, Parks
139
DR, (2004). Guidelines for the presentation of flow cytometric
data. Methods Cell Biol., 75:241-56.
Roman J, Castillejo JA, Jimenez A, (2002). 5' CpG island hypermethylation
is
associated
with
transcriptional
silencing
of
the
p21
(CIPl/WAFl/SDIl) gene and confers poor prognosis in acute
lymphoblastic leukemia. Blood, 99:2291-6
Rose N, Macrio E, Fhey J, Friedman H, Penn G, (1992). Manual of clinical
laboratory. Immunologu American Society for Microbiology
Washington DC., pp 156-200
Ross E, Zhou X, Song G, (2003). Classification of pediatric acute
lemphoblastic leukemia by gene expression profiling. Blood.,
102:2951-2959.
Rossi E, Ubiali A, Balzarini P, Cadei M, Alpi F, Grigolatoi PG, (2005).
High level detection of gene amplification and chromosome
aneuploidy in extracted nuclei from paraffin embedded tissue of
human cancer using FISH a new approach for retrospective
studies. Eur J Histochem., 49(1): 53-8.
Rozovzkaia T, Ravid-Amir O, Tillib S, (2003). Expression profiles of acute
lymphoblastic
and
myeloblastic
leukemias
with
ALL-1
rearrangement. Proc Natl Acad Sci U S A., 100:7853-7858.
Roumier T, Vieira HL, Castedo M, Ferri KF, Boya P, Andreau K,
Druillennec S, Joza N, Penninger JM, Roques B, Kroemer G,
(2002). The C-terminal moiety of HIV-1 Vpr induces cell death
via a caspase-independent mitochondrial pathway. Cell Death
Differ., 9(11):1212-9.
140
Rubin CM and Le Bea MM, (1991). Cytogenetic abnormalities in childhood
acute lymphoblastic leukemia. Am. J. Pediater. Hematol. Oncol.,
13:202-209.
Rudolph C, Hegazy AN, von Neuhoff N, Steinemann D, Schrock E,
Stripecke R, Klein C, Schlegelberger B, (2005). Cytogenetic
characterization of a BCR-ABL transduced mouse cell line.
Cancer Genet Cytogenet., 161(1):51-6.
Sainger N, Shal M, Desai A, Shukla S, (2006).Clinical significance of serum
p53 antibodies in oral cancer.Tumori., 92(2):134-9.
San-Miguel
G, Garica-Sanz
R, Gonzalez M,
Orfao A,
(1995).
Immunophenotype and DNA content in multiple myelpma.
Bailieres Clin. Haematol., 8: 735-759.
Sandler DP and
Ross JA, (1997). Epidemiology of acute leukemia in
children and adults. Semin Oncol., 24:3-16.
Sarrate Z, Blanco J, Anton E, Egozcue S, Egozcue J, Vidal F, (2005). FISH
studies of chromosome abnormalities in germ cells and its
relevance in reproductive counseling. Asian J Androl., 7(3):22736.
Schlieben S, Borkhardt A, Reinisch I, Ritterbach J, Janssen JWG, Ratei R,
Schrappe M, Repp R, Zimmermann M, Kabisch H, JankaSchaub G, Bartram CR, Ludwig W-D, Riehm H, Lampert F,
Harbott J, (1996). Incidence and clinical outcome of children
with BCR/ABL-positive acute lymphoblastic leukemia (ALL). A
prospective RT-PCR study based on 673 patients enrolled in the
German pediatric multicenter therapy trials ALL-BFM 90 and
CoALL-05-92. Leukemia, 10:957.
141
Schrappe M, Aricò M, Harbott J, (2000). Philadelphia chromosome-positive
(Ph+) childhood acute lymphoblastic leukemia: good initial
steroid response allows early prediction of a favorable treatment
outcome. Blood, 92 (8): 2730-41.
Schrappe M, Reiter A, Zimmermann M, (2000). Long term results of four
consecutive trials in childhood ALL performed by the ALL-BFM
study group from 1981 to 1995.Berlin-Frankfurt-munster.
Leukemia, 14 (12):2205-2222.
Schröck E, du Manior S, Veldman T, (1996). Multicolor Spectral
Karyotyping of Human Chromosomes. Science, 273:494497.
Schuler D, Szende B, Borsi JD, Marton T, Bocsi J, Magyarossy E, Koos R,
Csoka M, (1994). Apoptosis as a possible way of destruction of
lymphoblasts after glucocorticoid treatment of children with acute
lymphoblastic leukemia. Pediatr Hematol Oncol., 11(6):641-9.
Schwartz M and Osborne B, (1993). Programmed cell death apoptosis and
killer genes. Immunol. Today, 14:582.
Scornik JC, Brunson ME, Schaub B, Howard RJ, Pfaff WW, (1994). The
crossmatch in renal transplantation. Evaluation of flow cytometry
as a replacement for standard cytotoxicity. Transplantation, 57:
621-625
Sebban C, Leoage E, Vernant J, (1994). Allogeneic bone marrow
transplantation in adult acute lymphoblastic leukemia in first
complete remission: a comparative study. French Group of
Therapy of Adult Acute Lemphoblastic Leukemia. J Clin Oncol.,
12(2): 2580-2587.
Seckin D, Demirhan B, Karakayali H, Akgun S, Erdal R, Turan M, (2002).
Immunohistochemical expression of p53, Bcl-2, Bax, and Fas
142
proteins in squamous cell carcinomas from immunosuppressed
renal transplant recipients and immunocompetent individuals.
Transplant Proc., 34(6):2139-40.
Sedlak J, Hunakova L, Duraj J, Sulikova M, Chovancova J, Novotny L,
Chorvath B, (1999). Detection of apoptosis in a heterogenous cell
population using flow cytometry. Gen Physiol Biophys., 147-54.
Seipp MT, Erali M, Wies RL, Wittwer C, (2005).
HLA-B27 typing:
evaluation of an allele-specific PCR melting assay and two flow
cytometric antigen assays. Cytometry B Clin Cytom., 63(1):10-5.
Shannon KM, Turhan AG, Rogers PC, Kan YW, (1992). Evidence
implicating heterozygous deletion of chromosome 7 in the
pathogenesis of familial leukemia associated with monosomy 7.
Genomics, 14:121-125.
Shapiro HM, (1995). Practical flow cytometry, 3rd ed, Chap.7:154-156, New
York:Wiley-Liss.
Shaul Y, (2000). C-Abl: activation and nuclear targets. Cell Death Differ. 7:
10-16.
Sherr C, (1996). Cancer cell cycles. Science, 274: 1672-1677.
Shuster JJ, Wacker P, Pullen J, (1998). Prognostic significance of sex in
childhood B-precursor acute lymphoblastic leukemia: a Pediatric
Oncology Group Study. J Clin Oncol., 16 (8): 2854-63.
Sikorska-Fic B, Wasik M, Rokicka-Milewska R, (1998). DNA index
determined
by
flow
cytometry
in
children
with
acute
lymphoblastic leukemia as an additional diagnostic and prognostic
element. Wiad Lek., 51(4): 103-106.
143
Smith M, Arthur D, Camitta B, (1996). Uniform approach to risk
classification and treatment assignment for children with acute
lymphoblastic leukemia. J Clin Oncol., 14 (1): 18-24.
Smith MA, Ries LA, Gurney JG, (2005). Cancer incidence and survival
among children and adolescents: United States SEER Program
1975-1995. Bethesda, Md: National Cancer Institute, SEER
Program, 1999. NIH Pub.No. 99-4649.
Smolewski P, Grabarek J, Lee BW, Johnson GL, Darzynkiewicz Z, (2002).
Kinetics of HL-60 cell entry to apoptosis during treatment with
TNF-alpha or camptothecin assayed by the stathmo-apoptosis
method. Cytometry, 47(3):143-9.
Soussi T, Legros Y, Lubin R, Ory K, Schlichtholz B (1994). Multifactorial
analysis of p53 alteration in human cancer: a review. Int J Cancer,
57:1-9.
Stary J, Hrodek O, Hausner P, Petrakova A, Goetz P and Kreuger A
(1990). The importance of blast cell DNA content for prognosis of
childhood acute lymphoblastic leukemia. Neoplasma, 37 (3): 293299.
Stegh A, Kim H, Bnchoo R, Forlony K, Zhand J, Louis D, Chin L, (2007).
Bcl2L12 inhibits post-mitochondrial apoptosis signaling in
glioblastoma. Genes Dev., 21(1):98-111.
144
Susan H, Michael B, Zehavit G, Ygal H, (2003). Apoptosis - the p53
network. Journal of Cell Science 116: 4077-4085.
Symonds H, Krall L, Remington L, Saenz-Robles M, Lowe S,
Jacks
T,
Van T,
(1994).
p53-dependent
apoptosis
suppresses tumor growth and progression in vivo. Cell 78:
703-711
Synold TW, Relling MV, Boyett JM, (1994). Blast cell methotrexatepolyglutamate accumulation in vivo differs by lineage, ploidy, and
methotrexate dose in acute lymphoblastic leukemia. J Clin Invest.,
94 (5): 1996-2001.
Szende B, (2004). The occurrence and significance of apoptosis in tumors
Magy Onkol., 48(3):215.
Talbot D, (1993). The flow cytometric crossmatch in perspective. Transplant
Immunol., 1: 155-162.
Taylor IW and Mithorpe BK, (1980). An evaluation of DNA fluorochrome
staining techniques and analysis for flow cytometry. J. Histochem.
Cytochem., 28:1224.
Telford WG, Komoriya A, Packard BZ, (2004). Detection of localized
caspase activity in early apoptotic cells by laser scanning
cytometry. Cytometry, 47(2):81-8.
Terstappen L, Konemann M, Loken M, (1991). Flow cytometric
characterization of acute myeloid leukemia. Part1. Significance of
light scattering properties. Leukemia, 5:315-321.
Tie LJ, Gu LJ, Chen J, Dong L, Pan C, Ye H, Xue HL, Tang JY, Wang YP,
(2006). Correlation between karyotypic characteristics and
treatment outcome in childhood acute lymphoblastic leukemia
Zhonghua Xue Ye Xue Za Zhi., 27(5):339-43.
145
Tileney N, Strom T, Paul L, (1996). Cellular and molecular aspects.
Transplantation Biology, 6: 257-261.
Tkachuk D, Pinkel D, Kuo W-L, Weier H, Gray J, (1991). Clinical
applications of fluorescence in situ hybridization, GATA, 8: 6774.
Trask B, (1991). Fluorescence in situ hybridization: applications in
cytogenetics and gene mapping. Trends in Genetics, 1388-1392.
Tribukati B, (1984). Clinical DNA flow cytometry. Med. Oncol. Tumor
Pharmacothwe, 1:211.
Trka J, Zuna J, Haskovec C, Brabencova A, Kalinova M, Muzikova K,
Paukertova R, Hrusak O, Zemanova Z, Michalova K, Stary J,
(1999). Detection of BCR/ABL, MLL/AF4 and TEL/AML1
hybrid genes and monitoring of minimal residual disease in
pediatric patients with acute lymphoblastic leukemia. Leukemia,
138(1):12-7.
Trueworthy R, Shuster J, Look T, (1992). Ploidy of lymphoblasts is the
strongest predictor of treatment outcome in B-progenitor cell
acute lymphoblastic leukemia of childhood: a Pediatric Oncology
Group study. J Clin Oncol., 10(4):606–613.
Tschopp J, Martinon F, Hofmann K, (1999). Apoptosis: silencing the death
receptors. Curr Biol., 9: 381–384.
Tusch H and Schwab CE, (2005). CEThe use of flow cytometric methods in
acute and long-term in vitro testing. Toxicol In Vitro., 223-227
Uckun F, Sather H, Gaynon B, (1997). Clinical features and treatment
outcome of children with myeloid antigen positive acute
lymphoblastic leukemia: a report from the c Children's Cancer
Group. Blood., 90(1):28-35.
146
Uckun FM, Sensel MG, Sather HN, (1998). Clinical significance of
translocation t(1;19) in childhood acute lymphoblastic leukemia in
the context of contemporary therapies: a report from the
Children’s Cancer Group. J Clin Oncol., 16(2):527–535.
Uckun FM, Yang Z, Sather H, Steinherz P, Nachman J, Bosrom B, Crotty
L, Sarqis M, EKk O, Zeren T, Tubergen D, Reaman G, Gaynon
P, (2000). Cellular Expression of antiapoptotic Bcl2 oncoprotein
in newly diagnosed childhood acute lymphoblastic leukemia: a
Children's Cancer Group Study. Blood, 89(10): 3769-77.
Ulrich C, Yasui Y, Storb R, (2001). Pharmacogenetics of methotrexate:
toxicity among marrow transplantation patients varies with the
methylenetetrahydrofolate
reeducates
C677T
polymorphism.
Blood, 98:231-234.
Urbano A, Lakshmanan U, Choo PH, Kwan JC, Ng PY, Guo K,
Dhakshinamoorthy S, Porter A, (2005). AIF suppresses chemical
stress-induced apoptosis and maintains the transformed state of
tumor cells. EMBO J., 24(15):2815-26.
Urist M and Prives C, (2002). p53 leans on its siblings. Cancer Cell. 1: 311313
Varmeh-Ziaie S, Okan I, Wang Y, Magnusson KP, Warthoe P, Strauss M
and Wiman KG (1997). Wig-1, a new p53-induced gene encoding
a zinc finger protein. Oncogene, 15: 2699–2704.
Vega MI, Huerta-Yepez S, Jazirehi AR, Garban H, Bonavida B, (2005).
Rituximab (chimeric anti-CD20) sensitizes B-NHL cell lines to
Fas-induced apoptosis. Oncogene. 15: 2844-2848.
Verkasalo PK, (1996). Magnetic fields and leukemia--risk for adults living
close to power lines. Scand J Work Environ Health, 22(2):1-56.
147
Vermes, I, Haanen, C, Steffens-Nakken H, Reutelingsperger C, (1995). A
novel assay for apoptosis - flow cytometric detection of
phosphatidylserine expression on early apoptotic cells using
fluorescein labelled Annexin V. J. Immunol. Meth., 184: 39.
Vieira Pinheiro JP, Wenner K, Escherich G, Lanvers-Kaminsky C,
Wurthwein G, Janka-Schaub G, Boos J, (2005). Serum
asparaginase activities and asparagine concentrations in the
cerebrospinal fluid after a single infusion of 2,500 IU/m(2) PEG
asparaginase in children with ALL treated according to protocol
COALL-06-97. Pediatr Blood Cancer, 234-238
Vindelov LL, (1977). Flow microfluorometric analysis of nuclear DNA in
cells from solid tumors and cell suspensions. Virchows Arch. (cell
Patho.), 24: 227-242
Vojtesek B, Bartek J, Midgley CA, Lane DP, (1992). An immunochemical
analysis of the human nuclear phosphoprotein
p53. New
monoclonal antibodies and epitope mapping using recombinant
p53. J Immunol Mehods, 151:237-44
Wada T, Pippin JW, Marshall CB, Griffin SV, Shankland SJ, (2005).
Dexamethasone Prevents Podocyte Apoptosis Induced by
Puromycin Aminonucleoside: Role of p53 and Bcl-2-Related
Family Proteins. J Am Soc Nephrol., 323-327
Walker BD, McDevitt JT, (2005). A microchip CD4 counting method for
HIV monitoring in resource-poor settings. PLoS Med., 2(7):e182
Wallach D, Varfolomeev EE, Malinin NL, (1999). Tumor necrosis factor
receptor and Fas signaling mechanisms. Ann Rev Immunol.,
17:331–367.
148
Wang Z, El-Ali J, Gotsaed T, Perch-Nielson IR, Mogensren KB,
Snakenborg D, Kutter JP, Wolff A, (2004). Measurements of
scattered light on a microchip flow cytometer with integrated
polymer based optical elements. Lab Chip., 4(4):372-7.
Wang M, Li QF, Qiao FY, (2005). Application of fluorescence in situ
hybridization to prenatal diagnosis of Down syndrome. Zhonghua
Yi Xue Yi Chuan Xue Za Zhi, 22(3):317-9.
Webb LM, Vigorito E, Wymann MP, Hirsch E, Turner M, (2005). T Cell
Development
p110{gamma}
Requires
and
the
Combined
p110{delta}
Activities
Catalytic
of
the
Isoforms
of
Phosphatidylinositol3-Kinase. J. Immunol., 175(5):2783-7.
Wechsler D S, Shelly C A, Petroff C A, Dang C V, (1997). MXI1, a putative
tumor suppressor gene, suppresses growth of human glioblastoma
cells. Cancer Res., 57:4905–4912
Weiss DJ, (2002). Application of flow cytometric techniques to veterinary
clinical hematology. Vet Clin Pathol., 31(2):72-82.
Wenberg RA, (1996). How cancer arises. Scientific American, 275:62-66.
White DM, Crolla JA, Ross FM, (1995). Detection of Minimal Residual
Disease in Childhood Acute Lymphoblastic Leukaemia Using
Fluorescence In-Situ Hybridization. Brit J Haematol., 91: 10191024.
White E, (1996). Life, death, and the pursuit of apoptosis. Genes Dev. 10: 115
Wirth T, Kuhnel F, Fleischmann-Mundt B, Woller N, Djojosubroto M,
Rudolph KL, Manns M, Zender L, Kubicka S, (2005).
Telomerase-dependent virotherapy overcomes resistance of
hepatocellular carcinomas against chemotherapy and tumor
149
necrosis factor-related apoptosis-inducing ligand by elimination of
Mcl-1. Cancer Res., 65(16):7393-402.
Yin Y, Liu YX, Jin YJ, Hall EJ, Barrett JC, (2003). PAC1 phosphatase is a
transcription target of p53 in signalling apoptosis and growth
suppression. Nature. 422: 527-531
Yurov YB, Vostrikov VM, Vorsanova SG, Monakhov VV, Iourov IY,
(2001). Multicolor fluorescent in situ hybridization on postmortem brain in schizophrenia as an approach for identification of
low-level chromosomal aneuploidy in neuropsychiatric diseases.
Brain Dev., 23 Suppl 1:S186-90.
Zhang LP, Cheng YF, Liu GL, Lu AD, Liu YR, Wang H, (2005). The
clinical significance of detecting minimal residual disease in
childhood B-lineage acute lymphoblastic leukemia with flow
cytometry. Zhonghua Er Ke Za Zhi., 43(7):481-5.
Zhang L, Parkhurst JB, Kern WF, Scott KV, Niccum D, Mulvihill JJ, Li S,
(2003). Chromosomal changes detected by fluorescence in situ
hybridization in patients with acute lymphoblastic leukemia. Chin
Med J., 116(9):1298-303.
Zimmerman A and Truss F, (1979). Flow through cytophotometry. Urol.
Res., 7:1
Zwirglmaier K, (2005). Fluorescence in situ hybridisation (FISH) the next
generation. FEMS Microbiol Lett., 246(2):151-8.
150
VII- LIFE FLOWCYTOMETRIC FIGURES
(A)
Figure (1):
Flow
(B)
cytometric
analysis
of
c-myc
expression
on
M2
M1
mononuclear cells showing diagram (A) and dot plot (B) of positively
stained cells in relation to negative ones.
(A)
(B)
R2
M2
M1
R1
Figure (2): Flowcytometric analysis of p53 expression on mononuclear
cells showing histogram (A) and dot plot (B) of positively stained cells in
relation to negative ones.
151
Diploid: 100.00%
Dip G0-G1: 93.93 % at 33.49
Dip G2-M: 4.57 % at 61.69
Dip S: 1.50 % G2/G1: 1.84
Dip %CV: 2.84
Diploid: 100.00%
Dip G0-G1: 90.43 % at 35.31
Dip G2-M: 7.84 % at 65.30
Dip S: 1.73 % G2/G1: 1.85
Dip %CV: 3.17
Figure (3): Histogram showing cell cycle parameters (diploid) using flow
cytometer FACS caliber program modfit.
152
Diploid: 85.25 %
Dip G0-G1: 100.00 % at 38.52
Dip G2-M: 0.00 % at 77.05
Dip S: 0.00 % G2/G1: 2.00
Dip %CV: 3.42
Aneuploid 1: 14.75 %
Aneup G0-G1: 65.14 % at 69.75
Aneup G2-M: 28.72 % at 104.73
Aneup S: 6.13 % G2/G1: 1.50
Aneup %CV: 3.31
Aneup DI: 1.81
Diploid: 62.08 %
Dip G0-G1: 100.00 at33.10
Dip G2-M: 0.00 % at 66.21
Dip S: 0.00 % G2/G1:2.00
Dip %CV: 3.16
Aneuploid 1: 37.92 %
Aneup G0-G1: 95.37 % at45.19
Aneup G2-M: 1.76 % at 73.95
Aneup S: 2.88 % G2/G1: 1.64
Aneup %CV: 3.43
Aneup DI: 1.37
Figure (4): Histogram showing cell cycle parameters diploid and
aneuploid using flow cytometer FACS caliber program modfit.
153
VIII- LIFE FISH PICTURES
Figure A
Figure B
Figure C
Figure D
Figure (A,B,C and D): Each childhood acute lymphoblastic leukemia
case shows red signal which is ABL on chromosome 9 and green signal
which is the breakpoint cluster region (BCR) on chromosome 22 for
children with Philadelphia negative acute lymphoblastic leukemia (Ph‾
ALL).
154
Figure E
Figure F
Figure (E and F): Each childhood acute lymphoblastic leukemia case
shows red signal which is ABL on chromosome 9, green signal which is
the breakpoint cluster region (BCR) on chromosome 22 and pale orange
signal which is the fusion (BCR/ABL) for children with Philadelphia
positive acute lymphoblastic leukemia (Ph+ ALL).