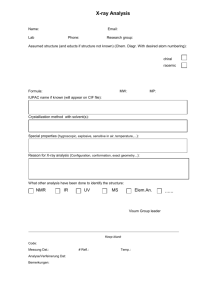
transfusion reaction report form
advertisement

KEMH/PMH PATHOLOGY CSU HMF:0900 A/0 28/04/2000 Authorised by: Dr L Marshall Haematology KING EDWARD MEMORIAL HOSPITAL FOR WOMEN AND PRINCESS MARGARET HOSPITAL FOR CHILDREN TRANSFUSION REACTION REPORT FORM ___________________________________________________ PATIENT IDENTIFICATION LABEL ________________________________________________ Ward ________________________ Consultant ________________________ Registrar ________________________ RMO ________________________ Reaction Date: ___________ Time:________ Diagnosis/Reason for transfusion: ____________________________________________________________ Component (Whole blood, etc) _______________________________ Volume given: __________________ Donation number of offending unit(s): SYMPTOMS: __________ Please fill in All boxes YES NO Pyrexia ________C Chills/Rigors Urticaria Tachycardia Chest pain ________________ ________________ ________________ ________________ ________________ ________________ Nausea/Vomiting Dyspnoea Lumbar Pain Burning around vein Hypotension Haemoglobinuria Excessive Bleeding Jaundice Shock x Other symptoms: ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------. Treatment given: ---------------------------------------------------------------------------------------------------------------Result: --------------------------------------------------------------------------------------------------------------- Previous Transfusion: _________________________ Reactions: __________________________________ Pregnancies: Known Antibodies: ___________________________ _________________________ Date: _______________ Time: ________________ BLOOD BANK REPORT: Request received: Clerical labelling error: Pre-transfusion sample blood group Post-transfusion sample blood group Medical Officer’s Signature: __________________________________ Date:______________ ___________________ ____________________ ____________________ Time:__________________ Antibody screen: _____DAT____ Antibody screen: _____DAT____ Investigation of blood bag and all units previously given: Bag No. Blood Group Compatibility Pre-trans Post-transfusion serum – jaundice or haemaglobinaemia: Urine: D:\116101881.doc Post-trans DAT Patient’s cells against plasma (if available)