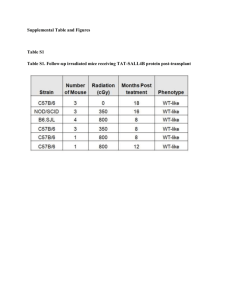
cancer from bmdc - plaza
advertisement

Cancer from Bone Marrow. Cogle, et al Bone Marrow Can Be A Primary Source Of Cancer Running title: Cancer from Bone Marrow Christopher R. Cogle1, Neil D. Theise2, DongTao Fu1, Sean Lee4, Steven M. Guthrie1, Marda L. Jorgensen1, Doug Smith1, Swan N. Thung3, Diane Krause4*, Edward W. Scott1* 1 Program in Stem Cell Biology and Regenerative Medicine, University of Florida, Gainesville, FL, USA 2 Departments of Medicine and Pathology, Beth Israel Medical Center, Albert Einstein College of Medicine, New York, NY, USA 3 4 Mount Sinai School of Medicine, New York, NY, USA Department of Laboratory Medicine, Yale University School of Medicine, New Haven, CT, USA * Authors contributed equally. Correspondence: Christopher R. Cogle, M.D., University of Florida, 1600 SW Archer Road, ARB R4-252, P.O. Box 100277, Gainesville, FL 32610-0277, Telephone: 352-392-3058, FAX: 352-392-8530, Email: c@ufl.edu 1 Cancer from Bone Marrow. Cogle, et al SUMMARY Bone marrow cells exhibit the ability to remodel distant organs. Here we show that marrow also participates in the development of epithelial neoplasias of the small bowel, colon and lung. The hematopoietic stem cell (HSC), in particular, demonstrates capability to participate in cancer development. Furthermore, this marrow involvement in epithelial cancer does not display fusion. Previous reports have highlighted chronic inflammation as critical to marrow participation in cancer. Extending these findings, we found SDF-1, a powerful HSC chemoattractant, intensely expressed in the epithelia of intestinal neoplasias containing marrowderived cells, suggesting that SDF-1 may be involved in HSC/marrow homing to cancer. Finally, we present human data demonstrating marrow as a source of epithelial neoplasias, underscoring the clinical relevance of these findings. Marrow participating in cancer development may be as a direct seed or as developmental mimicry. Future endeavors will need to distinguish between the two. Nevertheless, these findings expose new strategies for cancer prevention and treatment. 2 Cancer from Bone Marrow. Cogle, et al INTRODUCTION Bone marrow derived cells (BMDCs) can remodel remote organs (Alison et al., 2000; Cogle et al., 2004; Krause et al., 2001; Theise et al., 2000). In particular, transplantation studies in animals and humans have demonstrated that BMDCs contribute to epithelial layers of a variety of tissues (Brittan et al., 2002; Korbling et al., 2002; Krause et al., 2001; Okamoto et al., 2002). The origin of these epithelial cells could be from a single hematopoietic stem cell (HSC),(Krause et al., 2001) though other contributing marrow-derived cells may also play a role in this process. Moreover, BMDC engraftment in the gastrointestinal tract occurs by direct differentiation without evidence of cell fusion (Harris et al., 2004). The remodeling of distant organs by bone marrow cells occurs at very low levels in everyday physiology (Wagers et al., 2002). However, contribution from marrow is enhanced in settings of injury or disease, which is likely related to the homing effects of inflammation (Grant et al., 2002; Krause et al., 2001; Lagasse et al., 2000; Theise et al., 2002; Theise et al., 2000). A recent murine study suggested that BMDCs may contribute to cancer arising from the stomach lining (Houghton et al., 2004). Transplantation studies performed in mice with chronic gastritis due to bacterial infection show that resultant gastric carcinomas contained glands of marrow origin. This study emphasizes the importance of chronic inflammation in recruiting BMDCs. Whereas the authors purport that the recruited BMDCs then go on to serve as a source of gastric carcinoma, another explanation for these findings is “developmental mimicry” whereby local physical or chemical factors in the neoplastic environment influence morphologic changes in the immigrating, multipotent BMDCs. The distinction is important. BMDCs participating as a seed 3 Cancer from Bone Marrow. Cogle, et al of epithelial cancer would clearly be a malignant process, radically changing our perspectives on how we prevent and treat epithelial cancers. On the other hand, BMDCs participating via developmental mimicry would initially be a benign process of recruitment and differentiation; however, once incorporated, these multipotent developmental mimics may encourage the growth of surrounding malignant cells with tumor growth factors, immune evasion, pro-angiogenic factors and mobilization factors for metastasis. Developmental mimicry would also have significant therapeutic implications, exposing new strategies to prevent and treat cancer. Furthermore, based on in vitro cell culture in this study, it was proposed that the mesenchymal stem cell is the cell responsible for participating in gastric carcinoma. However, this was not tested with in vivo experimental techniques. This study also was restricted to animal studies, and leaves to question the clinical relevance of marrow contributing to cancer. These studies prompted us to more rigorously investigate the marrow contribution to epithelial cancers. First, we present data from transplantation experiments in mice demonstrating that bone marrow can contribute to spontaneously arising intestinal adenomas and carcinomas. We then directly address the question of the marrow cell responsible for contributing to cancer by presenting a murine lung cancer model, demonstrating that the HSC participates in cancer growth. We also address the clinical relevance of these findings by presenting human data which shows donor marrow contribution to secondary cancers after hematopoietic cell transplantation. Because the chemokine, stromal derived factor 1 (SDF-1), is a potent chemoattractant of hematopoietic stem cells and is widely expressed in many tissues during development and injury (Aiuti et al., 1997; Butler et al., 2004; McGrath et al., 1999), we further hypothesized that SDF- 4 Cancer from Bone Marrow. Cogle, et al 1 chemoattraction may be at least partly responsible for the homing and migration of BMDCs into these neoplastic environments. Here, we show that, indeed, SDF-1 is upregulated in the epithelial layers of intestinal neoplasias in both mice and humans. RESULTS Bone Marrow Contributes to Intestinal Adenomas in Mice and Humans In order to evaluate marrow contribution to intestinal neoplasias we performed transplantation experiments using APCmin mutant mice, which are prone to spontaneously develop adenomas and carcinomas in the small bowel and colon. Female mice (n=4) harboring the min mutation of the APC gene were transplanted with whole bone marrow from male APCmin mice. Three months post-transplant, the mice were sacrificed and small bowels and colons were resected. Adenomas and carcinomas were detected throughout the intestines of all animals. To address the question of whether the adenomas were of host or donor origin, we utilized a combination technique of IHC and FISH to identify neoplastic cells of donor (male) origin. Analysis of the stained intestinal tissues demonstrated donor derived colonocytes in the adenomas and carcinomas of all small bowel and colon specimens (Figure 1). These donor-derived adenoma cells were identified by being cytokeratin positive, CD45RB (lymphocytes) negative, and F4/80 (granulocytes/macrophages) negative. Importantly, this triple surface protein analysis, DAPI nuclear staining and FISH for Y chromosomes were performed on the same slide, ensuring no false positive interpretation due to overlapping leukocyte nuclei. The evaluation of over 20,000 adenoma cells from 16 intestinal samples demonstrated that a mean 2.5% of the cells were of bone marrow origin (range 0.2 – 12%). Furthermore, these donor-derived adenoma epithelial cells occurred in clusters and closely approximating pockets of cytokeratin-negative donor cells 5 Cancer from Bone Marrow. Cogle, et al located in the lamina propria. To address the question of whether the donor-derived adenoma cells represented fusion events between BMDCs and adenoma cells, we performed karyotype analyses using confocal microscopy. None of the donor-derived adenoma cells contained a fusion karyotype (XXY, XXXY), suggesting that fusion is an unlikely explanation (Figure 2). At our center we also identified two women with neoplasias involving the colon after hematopoietic cell transplantation (Table 1). The colorectal adenomas were found shortly posttransplant during colonoscopic evaluations for diarrhea. No infectious etiologies were found to explain the diarrhea; however, graft versus host disease (GVHD) was found in surrounding tissues, and colonic adenomas were identified and resected. Given the reports of marrow plasticity, we questioned whether these adenomas were of host or donor origin. Because the adenomas were found shortly after transplant, and considering the long latency period of adenomas, it is likely that the adenomas were present in the colon before transplant and they were expected to be entirely of host composition. Thus, we sectioned and stained the adenomas for the presence of donor-derived cells. As expected, the neoplastic tissues demonstrated donorderived (CD45 positive, Y chromosome positive) leukocytes, which were predominantly located in the lamina propria. To our surprise, however, the adenomas also contained donor-derived colonocytes in the adenoma epithelial layers (Figure 1). The donor cells had lost their hematopoietic surface protein, CD45 (leukocyte common antigen), and had adopted surface protein expression typical of the surrounding adenoma epithelial cells (cytokeratin and mucin) (Figure 1). Moreover, the bone marrow derived colonocytes in the adenomas were located in the basal strata of adenoma epithelia, suggesting recent immigration. In total, over 1000 adenoma epithelial cells were evaluated, demonstrating 1 – 4% of epithelial cells originating from donor 6 Cancer from Bone Marrow. Cogle, et al BMDCs. Information regarding the donors’ personal adenoma histories is unavailable. We further questioned whether these marrow-derived colonic adenoma cells were a result of fusion. In order to address this question we performed karyotype analysis. Confocal microscopy performed to enumerate X and Y chromosomes within each donor cell nucleus showed no evidence of a fusion sex chromosome karyotype (i.e., XXY or XXXY) (Figure 2). Bone Marrow As a Primary Source of Skin Cancer The observation that bone marrow incorporates into intestinal neoplasias then led us to consider whether BMDCs can contribute to other epithelial malignancies. To evaluate other epithelial malignancies we identified a woman who had a history of basal cell skin carcinoma 26 days prior to hematopoietic cell transplant and 4 years after hematopoietic cell transplant from her brother (Patient 1, Table 1). The multiparous patient was originally diagnosed with acute myelogenous leukemia. To eradicate her leukemia she elected to undergo non-myeloablative allogeneic hematopoietic cell transplant. Her brother donated mobilized peripheral blood cells and his personal history of cancer is unavailable. She achieved full donor hematopoietic engraftment three months after transplant; however had a relapse of her leukemia one year after transplant, requiring reinduction chemotherapy and donor leukocyte infusion (DLI) from her brother. Full hematopoietic chimerism was re-established three weeks subsequent to DLI. Post-transplant the patient developed GVHD of the skin only. As expected, prior to transplant her basal cell skin carcinoma was entirely female in origin (Figure 3). Although multiparous, this pre-transplant analysis suggests that no male fetal microchimerism was evident. Her post-transplant course was complicated by acute and chronic graft-versus-host-disease of the skin. Approximately four years after transplant she developed another basal carcinoma involving the forehead. Biopsy of 7 Cancer from Bone Marrow. Cogle, et al the post-transplant lesion demonstrated that the epithelial malignancy was 100% male origin (Figure 3). Furthermore, there is no evidence of fusion karyotype (i.e., XXY, XXXY) using confocal microscopy (Figure 3). The Hematopoietic Stem Cell Contributes to Lung Cancer in Mice and Humans This same woman with history of skin cancer who had received a hematopoietic cell transplant from her brother also developed lung cancer over four and one half years post-transplant (Patient 1, Table 1). She was afflicted briefly with pulmonary aspergillosis, and this was treated definitively with antifungal therapy. Again, we questioned whether the patient’s lung cancer was of host or donor origin. To address this question we sectioned and stained the patient’s lung cancer with the combination techniques of immunohistochemistry for cytokeratin and FISH for X and Y chromosomes. The lung cancer demonstrated donor origin as evidence by male cells co-expressing cytokeratin (Figure 4). We also used confocal microscopy to perform karyotype analysis. The donor-derived lung cancer cells demonstrated no evidence of a fusion karyotype (i.e., XXY, XXXY) suggesting that a multipotent bone marrow derived cell from the donor migrated to the lung and then underwent neoplastic changes (Figure 4). Previous reports of marrow as a source of gastric cancer used in vitro testing to determine if the hematopoietic stem cell (HSC) or the mesenchymal stem cell (MSC) is the primary source of cancer. Given the limitations of in vitro systems, it was important for us to use an in vivo experimental model to more rigorously examine HSC contribution to cancer. Thus, we transplanted single, GFP tagged HSC into (primary) mice (n=120) and then after hematopoietic chimerism was achieved (n=3) we sacrificed these mice and transplanted their bone marrow into 8 Cancer from Bone Marrow. Cogle, et al secondary recipients (n=30). All secondary recipient mice achieved GFP-hematopoietic chimerism. Secondary recipient mice (n=9) were then injected with murine lung cancer intramuscularly in the hind limbs. As expected, analysis of the lung cancers after 14 days of growth demonstrated a prominent display of green intratumoral cells of HSC origin (Figure 5). These cells were presumed to be inflammatory cells (progeny from the single green HSC). However, staining of the lung cancer tissues for the pan-leukocyte protein CD45 only found small pockets of donor leukocytes; the majority of these intratumoral cells were CD45 negative (data not shown). Given the plasticity potential of the HSC, we questioned whether these HSCderived cells were contributing to the lung cancer. Thus, we evaluated the cells for evidence of cytokeratin surface protein expression. Indeed, the tumors demonstrated HSC-derived (GFP+, green) cells co-expressing cytokeratin (red) (Figure 5). To determine whether these doublelabeled cells (i.e., GFP and cytokeratin) were the result of fusion, karyotype analysis was performed. All host mice and the lung cancer had a female kartyotype, allowing us to use FISH to track the male HSC and its progeny (Figure 5). Karyotype analysis of these donor-derived, cytokeratin positive cells found none with a fusion karyotype (i.e., XXY, XXXY) (Figure 5). SDF-1 Expression in Neoplastic Environments of BMDC Incorporation Based on recent rodent model findings that inflammation precedes BMDC incorporation and eventual gastric carcinoma development (Houghton et al., 2004), we questioned whether human BMDCs migrate to adenomas in reaction to inflammatory cues. Specifically, we hypothesized that the powerful chemoattractant stromal derived factor 1 (SDF-1) may be at least partly responsible for the homing and migration of bone marrow cells to the neoplastic environment (Aiuti et al., 1997). To test this hypothesis, murine (n=4) and human (n=2) adenomas which 9 Cancer from Bone Marrow. Cogle, et al contained marrow derived adenoma epithelial cells were immunohistochemically stained for SDF-1. Adenomas in mice and humans demonstrated intense and patchy SDF-1 expression. Surprisingly the rich SDF-1 expression was located predominant in the epithelial layers of the adenomas rather than in stroma or blood vessels of the lamina propria (Figure 6). DISCUSSION We have previously shown that the BMDCs can remodel distant organs (Cogle et al., 2004; Krause et al., 2001; Theise et al., 2000). Whereas this BMDC incorporation is minimal in daily physiology (Wagers et al., 2002), it becomes more apparent in settings of injury and repair, likely reflecting the response to inflammation (Butler et al., 2005; Grant et al., 2002; Krause et al., 2001; Lagasse et al., 2000; Theise et al., 2002; Theise et al., 2000). Indeed, recent reports have highlighted the role of chronic inflammation in promoting marrow incorporation into cancer (Houghton et al., 2004). Given these findings, we aimed to define the role of BMDC participation in epithelial cancers. The present studies confirm and extend previous reports, and is the first to raise the possibility that the HSC within the bone marrow is the responsible cell in cancer development. The murine transplantation studies utilizing the APCmin mutation mice provide the initial insights into bone marrow contributing to epithelial neoplasia. Spontaneous adenomas and carcinomas in the small bowels and colons of transplant recipient mice demonstrated adenoma cells of bone marrow origin. Several considerations should be made. First, bone marrow incorporation into the intestinal adenomas occurred closely approximating bone marrow derived cells located in the lamina propria, suggesting recent immigration. Another consideration is that these BMDCs in 10 Cancer from Bone Marrow. Cogle, et al the neoplasia may represent phagocytic events between the BMDC and resident adenoma cells. If this were true then resultant cells should display hematopoietic surface proteins as well as hyperdiploidy. However, using immunohistochemistry plus FISH, we show that these adenomas demonstrated differentiated donor cells that expressed cytokeratin and lost expression of hematopoietic surface proteins (CD45RB and F4/80). In addition, karyotype analysis demonstrated no evidence for fusion (i.e., XXY, XXXY). Given the plasticity potential of the HSC we further questioned if this particular marrow cell participates in cancer development. Lung cancer grown in mice which were serially transplanted from single HSC donor mice demonstrated cytokeratin positive cells of HSC origin. Our immediate consideration was that these HSC-derived cells incorporating into lung cancer represented phagocytosis between the HSC or its progeny and a cancer cell. To our surprise karyotype analysis found no evidence of fusion. It has been suggested that cells which arise as fusion products may undergo “reduction division”, dividing back into diploid cells. While that might still be an explanation for these findings, it should be noted that in models where fusion events have been described, most, if not all, of the fused cells persist in the tissues, without complete “resolution” (Wang et al., 2003). Thus, direct differentiation of HSC-derived cells into lung cancer, rather then absolutely complete and perfect resolution of every fusion event is the most likely explanation of our current findings. These results are the first to suggest that the HSC contributes to cancer, challenging the previous report which speculates that the mesenchymal stem cell compartment of the bone marrow contributes to carcinomas (Houghton et al., 2004). 11 Cancer from Bone Marrow. Cogle, et al There are two possibilities to explain HSC/marrow incorporation into cancer. As a recent study suggests, marrow derived cells may act as a direct source of cancer (Houghton et al., 2004). In this case, BMDCs serving as a seed of cancer likely require an antecedent environment of inflammation leading to BMDC immigration. Our study extends these findings by raising the possibility that SDF-1 may be involved in the homing and migration of BMDCs into epithelia. Given the potency of the SDF-1/CXCR4 axis, we report the findings that colonic neoplasias indeed over-express SDF-1 in the epithelial layers of mouse and human adenomas, suggesting that SDF-1 is an important signaling molecule in the recruitment of circulating marrow stem/progenitor cells. These results also fit with the broad findings of SDF-1 in a number of injury models (Butler et al., 2004; Hatch et al., 2002). These findings also confirm a recent report indicating SDF-1 as a key cytokine in breast cancer growth [WEINGBERG REFERENCE]. However, in contrast to the recent breast cancer study by Weinberg, et al, our results found SDF-1 in the epithelial layers of intestinal adenomas and carcinomas. The variation in location of SDF-1 expression (stromal fibroblasts versus neoplastic epithelia) may be due to differences in sites of cancer or degree of marrow contribution to cancer. In the model pathway of marrow as a direct source of cancer, after immigration into the inflamed epithelial space, the multipotent BMDCs through constant exposure to inflammatory cytokines and/or toxins (e.g., oral toxins, UV sunlight, tobacco smoking, irradiation, chemotherapy) undergo genetic transformation events promoting self-renewal and unchecked proliferation – that is, cancer development. However, the previous report did not consider a second possibility that we would call “developmental mimicry.” In this situation HSC/marrow are called into a neoplastic 12 Cancer from Bone Marrow. Cogle, et al environment and then through subjection to growth factors and cell-cell contact undergo changes in cell fate, mimicking the surrounding neoplastic cells. Given the self-renewal and high proliferative potential of BMDCs, these marrow cells could go on to act as paracrine regulators, providing growth factors and immune evasion for the surrounding tumor. Whichever route most accurately describes marrow participation in cancer, both represent a malignant process, revealing several new strategies to prevent and treat cancer. To address the clinical relevance of these findings, we also studied cancer specimens from patients treated at our center. The risk of developing a new cancer after blood or marrow transplantation is estimated to be up to eight times higher than in aged-matched controls (Curtis et al., 1997). Predisposing risk factors such as radiation, chemotherapy and use of immunosuppressants have been recognized. However, another factor in the post-transplant setting may be that multipotent donor marrow cells incorporate into inflamed epithelia, due to GVHD or other inflammatory process, and then undergo pathologic changes resulting in a new cancer. Indeed, in the human studies presented here, donor hematopoietic grafts participated in epithelial malignancies involving the lung, colon and skin of transplant recipients. It should be noted that preceding the neoplasias in the skin and colon specimens, GVHD was found. These results confirm, extend and answer the clinical relevance of the previous report showing the importance of precedent chronic inflammation (Houghton et al., 2004). One consideration is that cancers found in the patients may have been engulfed by donor-derived bone marrow cells, such as monocytes or macrophages. This theory of a myeloid-cancer hybrid cell has been put forth recently by Pawelek, et al (Pawelek, 2005). These investigators studied a renal cell carcinoma 13 Cancer from Bone Marrow. Cogle, et al developing after hematopoietic cell transplantation and discovered that the tumors contained donor DNA in addition to trisomy 17, which is a characteristic cytogenetic abnormality for this neoplasia (Yilmaz et al., 2005). Possibilities explaining this discovery is that a cell from the hematopoietic graft fused with a renal carcinoma creating a +Y, +17 situation or a marrow derived cell transdifferentiated into a renal cell carcinoma. The studies presented here found no evidence of fusion between marrow-derived cells and neoplastic cells, supporting the latter argument. To address the question of reduction division, we scored a total of 40 Y positive colonic adenoma cells with no evidence of hyperdiploidy. In the liver, where cell fusion has been demonstrated in severe disease stress states, it has been postulated that 28% of donorderived hepatocytes are due to reduction division, resulting in diploid daughter cells (Wang et al., 2003). Based on the probability of binomial distribution, the chance that we would find 40 out of 40 diploid donor-derived colonic adenoma cells amidst a background fusion resolution rate of 28% is one in 1x1022. Thus, direct differentiation of human marrow cells, rather then absolutely complete and perfect resolution of every fusion event, is the most likely explanation of our current findings. These results have strong implications for oncology, as well as stem cell biology. Our findings – demonstrating that bone marrow cells, and specifically the HSC, incorporate into epithelial cancers – suggest that a transplantable hematopoietic cell responds to inflammatory cues (such as SDF-1), activates tissue-specific differentiative genetic programming and is susceptible to further neoplastic changes. Future studies are aimed at making the important distinction between marrow as a seed of cancer versus marrow as a developmental mimic of cancer. However, in the meantime it appears that human BMDCs, much like their murine counterparts, may play a role in 14 Cancer from Bone Marrow. Cogle, et al epithelial cancer growth and development. With the findings presented here, new doors have been opened to identify novel strategies for preventing and treating cancer. EXPERIMENTAL PROCEDURES Animals Mice with genetic mutations in the APC gene (APCmin) and transgenic mice with ubiquitous GFP expression (STRAIN INFO) were obtained from Jackson laboratories (Bar Harbor, Maine). Wild-type C57BL/6 female mice were obtained from Charles River Laboratories (Wilmington, Massachusetts). The institutional animal care and use committees of Yale University and University of Florida approved all animal procedures. Human Subjects Paraffin embedded neoplastic tissues were obtained from female patients who received hematopoietic cell transplantation from male donors, following IRB approval by the University of Florida Health Science Center. Murine Hematopoietic Cell Transplantation Studies For the mouse adenoma experiments, bone marrow was harvested from a male APCmin mutant mouse and 1x106 cells were injected intravenously into recipient female APCmin mutant mice (n=4). To prepare recipients, APCmin female mutant mice received total body irradiation (1.1 Gy total from a 137cesium source) followed by marrow transplantation. All recipient mice were sacrificed 3 months post-transplant and intestines removed for fixation and staining. 15 Cancer from Bone Marrow. Cogle, et al For single HSC transplants Sca-1+c-kit+Lin- HSCs were enriched by FACS sorting before individual HSC selection with micromanipulators via fluorescent microscopy. Individual Gfp+ HSCs were then mixed with 2x105 non-Gfp+ BM cells that had been depleted of Sca-1+ cells by magnetic beads before transplant into irradiated (0.95 Gy total, 137cesium source) hosts. For the serial transplants, 1x103 bone marrow cells were transplanted into irradiated (0.95 Gy total) secondary, female C57BL/6 recipients. Mouse Adenoma Immunohistochemistry Isotype, serum, and no primary antibody controls were included for each sample in the immunostaining protocols. Negative and positive control tissues were processed in each staining run. For Y FISH, CD45 and cytokeratin, 3 µm sections were deparaffinized, hydrated, incubated in BD Biosciences Retrievagen A solution for 15 min at 100°C and then 20 min at room temperature, and incubated in 0.2 M HCL for 12 min and 1 M NaSCN at 80°C for 20 min. Y FISH was performed as described previously with digoxigenin-labeled Y chromosome probe and anti-digoxigenin-rhodamine antibody (Roche Molecular Biochemicals) [NEED REFERENCE FROM DIANE]. After Y FISH, slides were incubated in 1:20 anti- CD45RB (Santa Cruz Biotechnology), 1:100 F4/80 (eBioscience, San Diego, CA) 1 h at room temperature, incubated with anti-rat alexa 647 (Molecular Probes), fixed in 2% PFA in 1x PBS for 8 min, digested with 0.5 trypsin for 1 min at 37°C, washed with 5% FCS to inactivate the trypsin, incubated with 1:200 anti-pankeratin (DAKO) overnight at 4°C, incubated in 1:500 anti-rabbit-FITC (Molecular Probes) for 1 h at 37°C, and coverslipped by using vectashield DAPI (Vector Laboratories). Immunohistochemistry on human specimens and mouse lung cancer 16 Cancer from Bone Marrow. Cogle, et al Zinc formalin-fixed, paraffin-embedded adenoma sections were cut at 4 – 6 m and air-dried overnight. After deparaffinization and rehydration, endogenous peroxidase activity was quenched by application of 3% hydrogen peroxide in methanol for 10 minutes at room temperature. Tissues to be stained for CD45 (leukocyte common antigen, LCA DakoCytomation, Carpinteria, CA) were antigen retrieved using Trilogy unmasking solution (Cell Marque, Hot Springs, AK). Sections stained for CK20 (cytokeratin 20, DakoCytomation, Carpinteria, CA) were sequentially retrieved with citrate buffer (DakoCytomation,Carpinteria, CA) and trypsin (Digest-all 2, Zymed laboratories, San Francisco CA). Endogenous biotin was blocked with a kit (Dako, Carpinteria, CA), and primary antibody was then applied for one hour at room temperature (1:50 for CD45 and 1:25 for CK20). Primary antibody was detected using an LSAB2-HRP kit (DakoCytomation, Carpinteria, CA) and Diaminobenzidene (DAB). Isotype-matched negative controls were run with each of the antibodies, finding no non-specific binding. An appropriate positive control slide was also stained with each staining run. SDF-1 Immunostaining For SDF-1 staining, adenoma blocks were cut into 5 µm sections, deparaffinized and then incubated with mouse anti–human SDF-1 Ab K15C at 1:400. Overnight incubation at 4°C was followed by incubation with biotin-labeled rabbit anti-mouse IgG (1:100; Dako Corp.) for 30 minutes at room temperature. The sections were then incubated with ABC complex (Vector Laboratories Inc.) and developed with DAB as substrate. They were then counterstained in hematoxylin and covered with coverslips. 17 Cancer from Bone Marrow. Cogle, et al FISH Probing for X and Y Chromosomes Slides were treated to two rounds of a five-minute incubation in Lugol’s solution (Sigma, St. Louis, MO) followed by destaining in 2.5 M sodium thiocyanate. Tissue was further prepared by incubation in 0.2 N hydrochloric acid for 30 minutes at room temperature, and incubation in 1 M sodium thiocyanate for 30 minutes at 85 °C. Pretreatment concluded with a digestion in pepsin at 4 mg/mL (Sigma, St. Louis, MO) in 0.9% sodium chloride, pH 2.0 for up to 60 minutes at 37 °C. Slides were next rinsed with distilled water and equilibrated in 2x saline sodium citrate (SSC). After serial dehydration in ethanol, slides were placed on the heat plate of a Hybrite oven (Vysis Inc, Downers Grove, IL). CEP probes for X and Y chromosomes (Vysis Inc, Downers Grove, IL) were added to the sections and coverslips were sealed over the slides with rubber cement. Tissue sections and probes were co-denatured at 75 °C for 6 minutes before being hybridized overnight at 37 °C. Slides were then washed in 50% formamide in 2x SSC at 46 °C thrice for 7 minutes each, followed by 2x SSC at 46 °C for 5 minutes, and the 4x SSC + 0.1% Igepal (Sigma, St. Louis, MO) at 46 °C for 5 minutes. Slides were air dried in the dark and then mounted with Vectashield containing 4,6-daminidino-2-phenylidole (DAPI) (Vector Laboratories, Burlingame, CA). Tissue Analysis Slides were analyzed using a Leica laser scanning spectral confocal microscope (Leica Microsystems, Bannockburn, IL). DAB staining for tissue specific antigens and characteristic cellular morphology were used to specifically classify cells. Paraffin-embedded adenoma blocks were sectioned and immunohistochemically stained with specific antibodies to identify epithelial 18 Cancer from Bone Marrow. Cogle, et al neoplastic tissues (cytokeratin) and leukocytes (CD45). Basal cell skin cancer appeared below the epidermis. Neoplastic adenoma cells appeared elongated and large, with an epithelial orientation and positive staining with anti-cytokeratin antisera and periodic acid Schiff (PAS) staining. Squamous cell lung carcinoma cells were detected by their atypia, large size, angulated nuclei, evidence of keratinzation and invasion below the basement membrane. Leukocytes appeared small and round with positive anti-CD45 antisera staining. Y chromosome signal was punctate, green and regularly at the nucleus perimeter. X chromosome signal was similarly nuclear and punctate, but red. 19 Cancer from Bone Marrow. Cogle, et al REFERENCES Aiuti, A., Webb, I. J., Bleul, C., Springer, T., and Gutierrez-Ramos, J. C. (1997). The chemokine SDF-1 is a chemoattractant for human CD34+ hematopoietic progenitor cells and provides a new mechanism to explain the mobilization of CD34+ progenitors to peripheral blood. J Exp Med 185, 111-120. Alison, M. R., Poulsom, R., Jeffery, R., Dhillon, A. P., Quaglia, A., Jacob, J., Novelli, M., Prentice, G., Williamson, J., and Wright, N. A. (2000). Hepatocytes from non-hepatic adult stem cells. Nature 406, 257. Brittan, M., Hunt, T., Jeffery, R., Poulsom, R., Forbes, S. J., Hodivala-Dilke, K., Goldman, J., Alison, M. R., and Wright, N. A. (2002). Bone marrow derivation of pericryptal myofibroblasts in the mouse and human small intestine and colon. Gut 50, 752-757. Butler, J. M., Guthrie, S. M., Caballero, S., Brooks, L., Mames, R., Grant, M. B., and Scott, E. W. (2004). SDF-1 is both necessary and sufficient to produce proliferative retinopathy. J Clin Invest In press. Butler, J. M., Guthrie, S. M., Koc, M., Afzal, A., Caballero, S., Brooks, H. L., Mames, R. N., Segal, M. S., Grant, M. B., and Scott, E. W. (2005). SDF-1 is both necessary and sufficient to promote proliferative retinopathy. J Clin Invest 115, 86-93. Cogle, C. R., Yachnis, A. T., Laywell, E. D., Zander, D. S., Wingard, J. R., Steindler, D. A., and Scott, E. W. (2004). Bone marrow transdifferentiation in brain after transplantation: a retrospective study. Lancet 363, 1432-1437. Curtis, R. E., Rowlings, P. A., Deeg, H. J., Shriner, D. A., Socie, G., Travis, L. B., Horowitz, M. M., Witherspoon, R. P., Hoover, R. N., Sobocinski, K. A., et al. (1997). Solid cancers after bone marrow transplantation. N Engl J Med 336, 897-904. Grant, M. B., May, W. S., Caballero, S., Brown, G. A., Guthrie, S. M., Mames, R. N., Byrne, B. J., Vaught, T., Spoerri, P. E., Peck, A. B., and Scott, E. W. (2002). Adult hematopoietic stem cells provide functional hemangioblast activity during retinal neovascularization. Nat Med 8, 607-612. Harris, R. G., Herzog, E. L., Bruscia, E. M., Grove, J. E., Van Arnam, J. S., and Krause, D. S. (2004). Lack of a fusion requirement for development of bone marrow-derived epithelia. Science 305, 90-93. Hatch, H. M., Zheng, D., Jorgensen, M. L., and Petersen, B. E. (2002). SDF-1alpha/CXCR4: a mechanism for hepatic oval cell activation and bone marrow stem cell recruitment to the injured liver of rats. Cloning Stem Cells 4, 339-351. Houghton, J., Stoicov, C., Nomura, S., Rogers, A. B., Carlson, J., Li, H., Cai, X., Fox, J. G., Goldenring, J. R., and Wang, T. C. (2004). Gastric cancer originating from bone marrow-derived cells. Science 306, 1568-1571. Korbling, M., Katz, R. L., Khanna, A., Ruifrok, A. C., Rondon, G., Albitar, M., Champlin, R. E., and Estrov, Z. (2002). Hepatocytes and epithelial cells of donor origin in recipients of peripheralblood stem cells. N Engl J Med 346, 738-746. Krause, D. S., Theise, N. D., Collector, M. I., Henegariu, O., Hwang, S., Gardner, R., Neutzel, S., and Sharkis, S. J. (2001). Multi-organ, multi-lineage engraftment by a single bone marrowderived stem cell. Cell 105, 369-377. Lagasse, E., Connors, H., Al-Dhalimy, M., Reitsma, M., Dohse, M., Osborne, L., Wang, X., Finegold, M., Weissman, I. L., and Grompe, M. (2000). Purified hematopoietic stem cells can differentiate into hepatocytes in vivo. Nat Med 6, 1229-1234. 20 Cancer from Bone Marrow. Cogle, et al McGrath, K. E., Koniski, A. D., Maltby, K. M., McGann, J. K., and Palis, J. (1999). Embryonic expression and function of the chemokine SDF-1 and its receptor, CXCR4. Dev Biol 213, 442456. Okamoto, R., Yajima, T., Yamazaki, M., Kanai, T., Mukai, M., Okamoto, S., Ikeda, Y., Hibi, T., Inazawa, J., and Watanabe, M. (2002). Damaged epithelia regenerated by bone marrow-derived cells in the human gastrointestinal tract. Nat Med 8, 1011-1017. Pawelek, J. M. (2005). Tumour-cell fusion as a source of myeloid traits in cancer. Lancet Oncol 6, 988-993. Theise, N. D., Henegariu, O., Grove, J., Jagirdar, J., Kao, P. N., Crawford, J. M., Badve, S., Saxena, R., and Krause, D. S. (2002). Radiation pneumonitis in mice: a severe injury model for pneumocyte engraftment from bone marrow. Exp Hematol 30, 1333-1338. Theise, N. D., Nimmakayalu, M., Gardner, R., Illei, P. B., Morgan, G., Teperman, L., Henegariu, O., and Krause, D. S. (2000). Liver from bone marrow in humans. Hepatology 32, 11-16. Wagers, A. J., Sherwood, R. I., Christensen, J. L., and Weissman, I. L. (2002). Little evidence for developmental plasticity of adult hematopoietic stem cells. Science 297, 2256-2259. Wang, X., Willenbring, H., Akkari, Y., Torimaru, Y., Foster, M., Al-Dhalimy, M., Lagasse, E., Finegold, M., Olson, S., and Grompe, M. (2003). Cell fusion is the principal source of bonemarrow-derived hepatocytes. Nature 422, 897-901. Yilmaz, Y., Lazova, R., Qumsiyeh, M., Cooper, D., and Pawelek, J. (2005). Donor Y chromosome in renal carcinoma cells of a female BMT recipient: visualization of putative BMTtumor hybrids by FISH. Bone Marrow Transplant 35, 1021-1024. 21 Cancer from Bone Marrow. Cogle, et al Table 1. Patient Characteristics Patient Age at Primary transplant Disease (years) 1 59 AML 2 3 55 28 Transplant GVHD 2nd Cancer N/A PBSC PBSC Basal cell carcinoma Basal cell carcinoma Squamous cell carcinoma of the lung Colonic adenoma Colonic adenoma N/A Yes No Days Post Transplant Percent Donor in Neoplasia – 26 days 0% 1491 days 100% 1651 days 20% AML BM Yes 47 days 1% Hodgkin’s PBSC Yes 30 days 4% Lymphoma GVHD, graft versus host disease; AML, acute myelogenous leukemia; PBSC, mobilized peripheral blood stem cell; BM, bone marrow; N/A, not applicable 22 Cancer from Bone Marrow. Cogle, et al Figure Legends Figure 1. Intestinal neoplasias of bone marrow origin. (A – C) Intestinal adenomas and carcinomas from the small bowels and colons of female APCmin mutant mice. (A) Micrograph of CD45 (brown) immunostaining demonstrating few leukocytes within the adenoma (bar represents 100 µm). (B) Micrograph of cytokeratin (brown) immunostaining displaying adenomas with intense cytokeratin expression (bar represents 100 µm). (C) Fluorescent micrograph of an adenoma section stained for cytokeratin (green), leukocytes (pink), nuclei (blue) and FISH for Y chromosome (red). Arrows indicate marrow-derived cells within adenoma epithelia. (D – F) Colonic adenomas from women who received hematopoietic cell transplantation from male sibling donors. (D & E) Sections of the adenoma demonstrate a Y chromosome (green) within the nucleus (blue) of a colonocyte expressing cytokeratin (brown) and mucin (magenta). (F) Furthermore, donor-derived adenoma cells (Y chromosome, green; nuclei, blue) were CD45 (brown) negative. Figure 2. No evidence of fusion in bone marrow derived cells incorporated within murine intestinal neoplasias. Intestinal adenoma spontaneously arising in a female mouse with APCmin mutation after having received a bone marrow transplant from a male APCmin mouse. Adenomas were stained for cytokeratin (magenta), nuclei (blue) and FISH for X (red) and Y (green) chromosomes. Movie of serial z-steps through a murine intestinal adenoma. Arrows indicate marrow-derived intestinal epithelial cells demonstrating no evidence for fusion (i.e., XXY, XXXY). 23 Cancer from Bone Marrow. Cogle, et al Figure 3. No evidence of fusion in bone marrow derived cells incorporated within human colonic adenoma. Colonic adenoma found post-transplant in a woman who received hematopoietic cell transplantation from her brother demonstrates adenoma cells of male donor origin (X chromosome, red; Y chromosome, green). Movie of serial z-steps through human intestinal adenoma. Arrows indicate marrow-derived intestinal epithelial cells incorporating within the adenoma and displaying no evidence for fusion (i.e., XXY, XXXY). Figure 4. Human epithelial cancers from bone marrow origin without evidence of fusion. Basal cell skin carcinoma found pre-transplant and post-transplant in a woman who received hematopoietic cell transplantation from her brother. (A) Fluorescent micrograph of basal cell skin carcinoma found before transplant. As expected, skin cancer demonstrates that the entire specimen is of female origin (nuclei, blue; X chromosome, red). (B) Four and one half years after transplantation, skin cancer arose again and biopsy reveals that cancer is entirely of male origin (nuclei, blue; X chromosome, red; Y chromosome, green). Confocal micrograph demonstrates skin cancer cells with nuclei (blue) of male origin (Y chromosome, green) and no evidence of fusion (i.e., XXY, XXXY). (C & D) Secondary lung cancer found in a woman who received hematopoietic cell transplantation from her brother demonstrates lung cancer from donor hematopoietic cell origin. (C) Fluorescent micrograph showing immunostaining for cytokeratin (intense red) and FISH for Y (green) chromosomes (magnification 63X). (D) Confocal micrograph of bone marrow derived lung cancer cells stained with cytokeratin and FISH for X (red) and Y (green) chromosomes demonstrating no evidence of fusion. Arrows indicate donor-derived cells. 24 Cancer from Bone Marrow. Cogle, et al Figure 5. The hematopoietic stem cell contributes to lung cancer without evidence for fusion. Lung cancers in female mice which received secondary transplants from a single-HSC (GFP+,green) transplanted donor. (A) Fluorescent micrograph of lung cancer immunostained for cytokeratin (red) (bar represents 100 µm). Lung cancers show HSC derived cells (green) coexpressing cytokeratin (red) with a merged color of yellow. Arrows indicate HSC-derived lung cancer cells. (B) Confocal micrograph of lung cancer demonstrating non-fusion karyotype of HSC-derived lung cancer cells. Thick sections (10 µm) of lung cancer were stained for cytokeratin (magenta), nuclei (blue) and FISH for X (red) and Y (green) chromosomes. Arrows indicate HSC-derived lung cancer cells expressing cytokeratin. These cells on cofocal analysis demonstrated no evidence of fusion karyotype (i.e., XXY, XXXY). Figure 6. SDF-1 expression in neoplastic environments. Normal and neoplastic tissues of the intestines in mice and humans. (A & C) Normal intestines in mice and humans do not display expression of SDF-1 (brown) in the epithelial layers. (B & D) However, adenomas in mice and humans demonstrate intense and patchy expression of SDF-1 (brown) in the neoplastic epithelia. 25