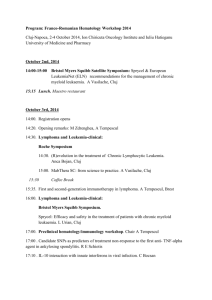
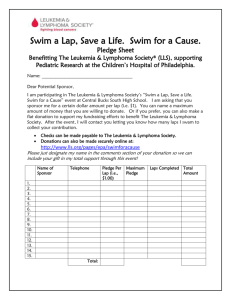
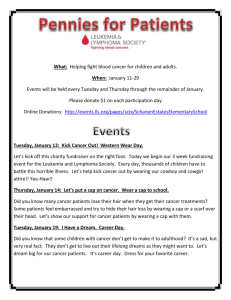
Integrated Hematology Exam:
advertisement

Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ Integrated Hematology: Pathophysiology/Pharmacology/Pathology (BI350/BI279) CASE 1: (Questions 1-3) A 65 year-old gentleman presents to your office with a chief complaint of headache. He states that he has had intermittent headaches for the last month or two. The headaches are typically relieved by Tylenol. He also notices that he develops itching, especially after he takes a warm shower. He has tried taking Benadryl, but with only partial improvement. His wife notices that his complexion has become increasingly ruddy over the last several months. The patient has for the most part enjoyed good health. He does not smoke. He has no known cardiac or respiratory problems. Review of systems is positive only for some soreness in his left upper quadrant. Physical exam: Vital signs are normal. HEENT reveals erythematous conjunctiva. There is no abnormal adenopathy. Lungs clear. Heart: S1, S2 normal; no murmurs, rubs or gallops. His abdomen is soft and non-tender. He has a 2-fingerbreadth spleen. The liver is not palpable. Examination of his extremities is unremarkable. His hemoglobin is 19 gm/dl, hematocrit 58, white count 12,000, platelet count 560,000. His peripheral smear reveals an increased number of platelets, but is otherwise unremarkable. 1. This patient most likely has a: A. Bcr/abl translocation. B. High erythropoietin level. C. JAK-2 mutation. D. Proliferation of clonally-related fibroblasts. E. Hypercellular marrow due to an infectious process. 2. If this patient had a splenectomy for another reason (such as trauma from a motor vehicle accident), the histology of the spleen would most likely: A. Appear to be normal. B. Demonstrate an increased number of plasma cells. C. Be infiltrated by sheets of myeloblasts. D. Demonstrate myeloid metaplasia (extramedullary hematopoiesis). E. None of the above. Note that the correct answer is D. Myeloid metaplasia would be the expected finding in the spleen of a patient with P.Vera. However, splenic congestion (E. “None of the Above”) would be an appropriate answer as well for a patient in the early (Erythrocytotic Phase of P.Vera) – so we will accept answer E. as well. This patient was treated appropriately and did well for the next 8 years. He now presents to his physician with symptoms of shortness of breath and dyspnea on exertion. He is found to be anemic with a Hb of 8, Hct 24. His bone marrow aspirate is shown below in Figure 1. Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ Figure 1. (BM biopsy on left; reticulin stain on right). 3. This marrow demonstrates: A. Disease transformation to a DLBCL (Richter’s syndrome). B. Disease progression to myelofibrosis. C. Metastatic carcinoma unrelated to the initial diagnosis. D. Transformation to Acute Lymphoblastic Leukemia. E. Adequate cellularity, suggesting peripheral red cell destruction as an explanation for the anemia. CASE 2. (Questions 4 & 5) A 55 year-old lawyer who has enjoyed excellent health presents to your office complaining of easy bruising. He has noted that over the last few weeks he always seems to have an ecchymotic lesion somewhere on his extremities or his trunk. There was no known trauma. Additionally, he states that he is fatigued more easily than is his norm. An avid golfer, he finds it difficult to walk 18 holes. He often notes shortness of breath with exertion and occasional palpitations. On examination, vital signs are normal. HEENT: conjunctival pallor, extensive swelling of the gums (see Figure 2A below) and palatal petechiae. No abnormal adenopathy. Lungs are clear. Heart: S1, S2 normal, I/VI systolic murmur. Abdomen is soft, non-tender, no masses. His extremities are negative except for a diffuse petechial rash on both lower extremities below the knee. . Figure 2A. 2 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ Figure 2B. Laboratory Studies: CBC: WBC 17,000 with 15% polys, 10% lymphs, 5% monos, 70% blasts; Hb 7.8 gm/dl; MCV 85; platelet count 20,000. PT and PTT are normal. The peripheral smear is shown in Figure 2B. 4. The most likely diagnosis is: A. Follicular lymphoma with extramedullary hematopoiesis. B. Acute lymphoblastic lymphoma/leukemia. C. Chronic Myelogenous leukemia. D. Acute Myelogenous leukemia, M4 or M5. E. Mature B-cell leukemia/lymphoma. 5. Further diagnostic studies are required to make a diagnosis. Based on the information presented thus far, which of the following is likely in this case? A. Non-specific esterase staining would be negative. B. The patient needs to undergo bone marrow aspiration and biopsy to confirm the diagnosis. C. The patient should have a lymph node biopsy. D. Results of cytogenetics studies may have prognostic significance. E. Analysis of TCR gene rearrangements would detect clonality. 3 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ CASE 3. (Questions 6-9) A patient with a similar presentation to the one described in Case 2 (above) was found to have the following cells on peripheral smear (Figure 3). Figure 3. 6. Which of the following molecular defects would be most likely in this disorder? A. Chromosomal translocation involving a CBF (Core Binding Factor). B. Overexpression of cyclin D1. C. t(8;14) D. t(14;18) E. t(9;22) 7. In an adult patient with this disease, which drug is considered essential to treatment: A. Chlorambucil (leukeran) B. Vincristine C. Cytarabine (Ara-C) D. Bleomycin E. Methotrexate 8. If flow cytometry were done, which of the following would likely be positive? A. CD20 B. CD4 C. CD5 D. CD33 E. CD15 and CD30 9. Which of the following monoclonal antibody targeted-therapies could be used to treat this patient? A. Rituximab (Rituxan) B. Tositumomab (Bexxar) C. Alemtuzumab (Campath) D. Ibritumomab tiuxetan (Zevalin) E. Gentuzumab ogozamicin (Mylotarg) 4 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ CASE 4: (Questions 10-13) A 60 year-old man presents to your office complaining of a mass in his left axilla. He states that he noticed a golf ball sized mass under his arm while he was showering. At first he thought it was an inflamed gland, but when it did not disappear over the next month, he decided to come to you for advice. He otherwise feels entirely well. He denies fevers, night sweats or weight loss. He has not been exposed to any infections, nor is he aware of any trauma to his arm. He specifically denies being scratched by a cat. Examination reveals normal vital signs. He has a 2 cm right supraclavicular node, a 2 cm left axillary node and a 1 cm right inguinal node. Lungs clear. Heart: S1, S2 normal; no murmurs, rubs or gallops. Abdomen soft, non-tender, no masses, no organomegaly. His extremities are negative. His CBC, differential and platelet count are normal. A lymph node biopsy was performed from the right supraclavicular node; representative sections are shown in Figure 4. Immunohistochemical studies revealed that the nodal cells expressed kappa (not lambda) light chain, as well as CD19, CD20, CD22, and surface Ig. Figure 4A (low magnification) Figure 4B (high magnification) 10. What is the most likely diagnosis? A. Diffuse Large B Cell Lymphoma B. Follicular hyperplasia C. Burkitt’s Lymphoma D. Follicular Lymphoma E. Lymphoblastic Lymphoma 11. Which of the following would be NOT be consistent with the diagnosis? A. A lack of constitutional symptoms. B. Presentation with Stage III or IV disease. C. Blasts in the peripheral blood. D. Small cleaved cells. E. A low Ki-67. 5 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 12. Which statement most accurately reflects the natural history of this disease? A. This is an aggressive disease, with an untreated life expectancy measured in weeks to months. B. This is an indolent disease, with median survival in advanced stage disease of between 7 and 10 years. C. This disease is complicated by renal failure due to the high cell turnover (uric acid nephropathy). D. Release of lysozyme from malignant cells results in renal failure. E. This disease transforms to an aggressive malignancy within a median of 2 years. 13. Which of the following accurately reflects the pathophysiological basis of this disease? A. It is associated with the t(14;18), resulting in overexpression of bcl-2. B. It is associated with the t(9;22) resulting in the bcr/abl fusion protein. C. It is associated with the t(8;14) resulting in overexpression of c-myc. D. It is due to a translocation involving core binding factor (CBF). E. It is due to a mutation in FLT-3, a tyrosine kinase receptor important in signal transduction. FREE-STANDING QUESTIONS: 14. A patient with a Non-Hodgkin’s lymphoma is treated with a chemotherapy regimen. Six months after completing her treatment, she develops symptoms of shortness of breath and is found to have rales on lung exam, and elevated JVD (jugular venous distention). CXR is consistent with congestive heart failure. This could represent a toxic effect of: A. Doxorubicin B. Vincristine C. Rituximab D. Fludarabine E. Cyclophosphamide. 15. The three most common types of Non-Hodgkin’s lymphoma in children (in the U.S.) are: A. Lymphoblastic lymphoma, Follicular lymphoma, DLBCL B. Lymphoblastic lymphoma, DLBCL, Burkitt’s lymphoma C. Follicular lymphoma, Small Cell Lymphocytic Lymphoma, DLBCL D. Burkitt’s lymphoma, Peripheral T Cell lymphomas, Mantle Cell lymphoma E. Follicular lymphoma, Marginal Zone lymphomas, Burkitt’s lymphomas. 16. The two most common types of Non-Hodgkin’s lymphoma in adults in the U.S. are: A. DLBCL and Small Cell Lymphocytic Lymphoma B. Follicular lymphoma and DLBCL C. Mantle cell lymphoma and Burkitt’s lymphoma D. Marginal Zone lymphoma and DLBCL E. Hodgkin’s lymphoma and DLBCL. 6 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 17. A 34 year old woman with Acute Myelogenous Leukemia underwent induction chemotherapy and is now in remission. Cytogenetic studies revealed that she was at a high risk of relapse. She is now considering consolidation treatment with High Dose chemotherapy & stem cell transplantation. Which of the following describes the properties of hematopoietic stem cells? They: A. Can repopulate the marrow with all cell lineages including hematopoietic and stromal supporting cells. B. Are metabolically indolent ie not highly proliferative cells. C. Express CD33. D. Express B-cell and T-cell specific markers, since they can differentiate into lymphoid or myeloid cells. E. Are easily identifiable in bone marrow aspirates. 18. Which of the following is NOT typically due to a disorder of pluripotential stem cells or multipotential progenitors? A. Aplastic anemia B. Myelodysplastic syndromes (MDS) C. CML D. P.Vera E. Multiple Myeloma 19. A 29 year old woman who complains of fatigue is found to have a hemoglobin of 9.9 g/dl (normal 12-16), a low MCV and a low MCHC. Which of the following is the most appropriate drug therapy? A. Cyanocobalamin B. Epoetin C. Ferrous gluconate D. Filgrastin E. Folic acid NOTE: QUESTIONS 20 & 21 ARE RELATED. 20. A 68 year old man presents with severe thoracic back pain, fatigue and weight loss. Laboratory studies: Hb 8.0 gm/dl, Hct 24, wbc 6,000 with normal differential & platelet count. Peripheral smear shows rouleaux formation. Serum creatinine is 5.0 (normal 1.0). Which of the following tests would be most useful in making a diagnosis? A. Bone scan. B. Urine analysis and dip stick for protein (light chains). C. Serum Fe, TIBC, ferritin levels. D. Measurement of serum viscosity. E. Serum and urine protein electrophoresis. 21. The anemia in this patient may respond which of the following medications? A. Ferrous sulfate B. Filgrastim C. Ferrous gluconate D. Cyanocobalamin E. Epoetin 7 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 22. A patient is found to be anemic, and the astute clinician orders a reticulocyte count (in addition to other studies). Which of the following disorders would typically have a low reticulocyte count? A. Autoimmune hemolytic anemia B. GI hemorrhage (8 days after the event) C. Anemia of chronic disease D. B12 deficiency 1 week into treatment with B12 E. None of the above. Dropped 23. A patient with liver disease is found to have the following peripheral blood smear (Figure 5). Figure 5. Which of the following statements regarding these cells is NOT correct? A. They are slightly larger cells (higher MCV) than normal rbcs. B. They are more resistant to osmotic lysis than normal cells. C. Their inability to change shape leads to splenic trapping. D. This type of cell may be seen in a variety of hemoglobinopathies. E. It is a manifestation of excess membrane. This smear shows target cells that are typically seen in liver disease and in thalassemias and hemoglobinopathies. This rbc shape is due to excess membrane (E is a true statement). Excess membrane would result in slightly larger cells (A is a true statement) that are less likely to undergo osmotic lysis (ie there is more room inside the cell to take in water before lysis – so they are more resistant to osmotic lysis) (B is a correct statement). Increased splenic trapping occurs in cells that are less flexible and unable to change shape to navigate the microcirculation. The classic example we gave you of this was Hereditary Spherocytosis where there is a decrease in the membrane:hemoglobin ratio, less rbc flexibility, and more splenic trapping with rbc destruction. 24. A 16 year old boy with a known hemoglobinopathy presents in the ER because of severe deep, sharp pain in his legs unresponsive to oral pain medication. His peripheral smear is shown in Figure 6. Dropped Figure 6. 8 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ In this disorder: A. Patients are expected to have a normal lifespan. B. There is an imbalance of and chains due to a deletion in the globin gene. C. There is often an impaired ability to concentrate urine. D. Splenomegaly is a common finding in adults. E. There is no increase in thrombotic risk because platelets are normal. This is a case of a patient with Sickle Cell disease. Patients with SS have a shortened life expectancy (Answer A is false). There is a single point mutation in the globin chain (B is false – there is no deletion, and no “imbalance” as in the thalassemias). Answer C is correct. Sickle cell patients typically have an impaired ability to concentrate urine (the acidic and hypertonic environment in the renal medulla results in sickling with microinfarcts). Splenomegaly is NOT a common finding in adults with SS disease because of splenic infarction which reduces the size of the spleen by the time of adolescence (“autoinfarction”). Remember that sickle patients are at increased risk of infections with encapsulated organisms because of this complication. Finally, there is an increased thrombotic risk but not because of normal platelets! 25. Examination of peripheral blood smears may identify rbc abnormalities that may trigger a physician to consider a particular diagnosis. Which association is INCORRECT? A. Spherocytes warm autoantibodies B. Rouleaux cold agglutinin disease C. Schistocytes DIC D. Howell-Jolly bodies splenectomy E. Basophilic stippling lead poisoning 26. A patient presents with a Hb of 8.5, Hct of 26, and a normal wbc and platelet count. You suspect iron deficiency anemia because she reports heavy menses. Which of the following would be consistent with this diagnosis? A. Decreased Fe, decreased TIBC, decreased ferritin. B. Decreased Fe, increased TIBC, increased ferritin. C. Decreased Fe, increased TIBC, decreased ferritin. D. Decreased Fe, MCV of 95, and decreased ferritin. E. Decreased expression of DMT-1. 27. A 40 year old man presents with symptoms of fatigue and weakness. He has had arthritis for many years. On exam, his skin is found to have a bronze discoloration, and he has moderate hepatomegaly. He has a large extended family, and a second cousin is known to have hereditary hemochromatosis. He is suspected to have this disorder and is undergoing further evaluation. Which of the following is true of this condition? A. In most cases, it is associated with a mutation leading to down-regulation of DMT-1. B. Fe deposition in the pancreas can lead to diabetes mellitus. C. Treatment is best accomplished with iron chelating agents. D. Ferritin level is always low in untreated cases. 9 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ E. Mutation of HFE results in decreased Fe absorption from the G.I. tract. 28. A 40 year old woman is determined to have a hemolytic anemia. Which of the following laboratory tests confirms hemolysis as intravascular rather than extravascular? A. Elevated urinary urobilinogen B. Decreased haptoglobin C. Increased LDH D. Positive serum free hemoglobin E. Peripheral smear showing spherocytes Many of you answered B. While ABSENT haptoglobin is consistent with intravascular hemolysis, a modest reduction of haptoglobin can occur in extravascular hemolysis, so a decreased haptoglobin is not diagnostic. 29. A 59 year old woman had an ischemic stroke 5 years ago, and is on clopidogrel (Plavix) to decrease her risk of subsequent ischemic events. This drug functions as an antiplatelet drug via which mechanism? It: A. Inhibits cyclooxygenase. B. Inhibits the GpIIb/IIIa reaction. C. Inhibits the ADP reaction. D. Inhibits GpIb. E. All of the above. 30. A 60 year old Italian man presents to the ER with profound fatigue and hemoglobinuria after enjoying Easter dinner (which included fava beans). Hb 6.0, Hct 18; wbc and platelet counts were normal; LDH 1200, Bili 4.0, Direct Bili 1.0, Retics 26%; Coombs direct and indirect negative. He most likely has: A. Cold autoantibodies. B. Increased levels of red cell oxidized glutathione. C. Heinz bodies on Wright stain. D. Ineffective erythropoiesis. E. Increased or normal serum haptoglobin. Remember that although Heinz bodies are present in G-6-P-D hemolytic episodes (which this case describes), they are only visualized by staining with Supravital stains (they are not seen on routine Wright stains.) 31. In a patient with a megaloblastic anemia, an abnormal Part I of the Schilling Test, associated with a normal part II is consistent with: A. Strict vegan diet. B. Gastrectomy state. C. Bacterial overgrowth. D. Crohn’s disease. E. Dietary folate deficiency. 10 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ NOTE: QUESTIONS 32 and 33 ARE RELATED. 32. A patient with Rheumatoid Arthritis presents with Hb 8, retic count 12%, normal wbc & platelet count. LDH 800, indirect bili 2.4. Her peripheral smear is shown in Figure 7. Figure 7. She most likely has: A. Positive urinary hemosiderin. B. Acrocyanosis. C. Positive Heinz body prep with supravital stain. D. Positive Direct Coombs test utilizing Anti IgG. E. Increased life span of circulating red blood cells. 33. The initial treatment of choice for this patient is: A. Steroids. B. Plasmapheresis. C. Avoidance of cold. D. An immunosuppressive drug such as azathioprine (Imuran) E. Rituximab. 34. A 72 year old woman presents to the ER with fatigue. Her only other complaint is numbness and tingling of her hands and feet. Laboratory studies reveal Hb 5.0, Hct 15, MCV 120, wbc 4,000 with normal differential, platelet count 150K. She most likely will have: A. Elevated homocysteine, normal methylmalonyl CoA B. Diminished BM cellularity C. Increased reticulocyte count D. Increased LDH E. Increased lifespan of circulating rbc. 35. Patients with homozygous -thalassemia major: A. Typically have normal or only slightly elevated hematocrits. B. Have ineffective erythropoiesis secondary to chain excess. C. Severe Fe deficiency secondary to chronic intravascular hemolysis with resultant iron loss. D. Have increased HbF levels in blood. E. Are typically symptomatic at birth. 11 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ Dropped 36. A patient develops fever and chills one hour into administration of packed red blood cells. The patient likely has a(n): A. IgA deficiency. B. Major hemolytic reaction. C. Leukoagglutination reaction. D. Reaction to plasma proteins. E. Reaction known as TRALI. This case describes a non-hemolytic febrile transfusion reaction. These are thought to be due to antibodies formed against donor wbcs or platelets (leukoagglutination reaction), as well as cytokines formed during blood storage. This is not a major hemolytic reaction, which would present with symptoms occurring after only a small amount of blood has been transfused and almost always before the unit is transfused completely. Though the symptoms may include fever and chills (and thus may initially be difficult to distinguish from a non-hemolytic transfusion reaction), there may also be symptoms of nausea, chest tightness, restlessness, apprehension, joint pain, back pain. The patient may develop tachycardia, tachypnea, hypotension, and oliguria. Major transfusion reactions are typically due to ABO incompatibility reactions. Again, these occur more quickly than do the non-hemolytic febrile reactions. Anaphylactic reactions can occur in patients who are IgA deficient and have developed IgA antibodies. When they are exposed to donor IgA in the blood product, they can have an anaphylactic reaction. Proteins in donor plasma can cause minor allergic reactions (these would be “anaphylactoid” and might present with urticaria or skin manifestations in addition to fever and chills). TRALI refers to “transfusion-associated lung injury” and symptoms begin suddenly while the blood product is being transfused or up to 6 hours after transfusion. The presenting symptom is DYSPNEA. 37. Patients with -thalassemia who have a one gene deletion will have: A. A mild microcytosis without anemia. B. Elevated levels of HbH throughout adult life. C. Elevated levels of Hb Barts throughout adult life. D. Splenomegaly because of chronic low levels of hemolysis. E. None of the above. Either A or B is an acceptable answer. Dropped 38. A physician on the wards is trying to decide if it is appropriate to give cryoprecipitate to a patient who is bleeding. In making this decision, it will be helpful to remember that cryoprecipitate does NOT contain which of the following factors: A. Fibrinogen B. Factor XIII C. Factor VIII D. Factor V 12 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ E. vonWillebrand factor The correct answer is D. Cryoprecipitate contains the high molecular weight factors: fibrinogen, factor XIII, factor VIII, and vonWillebrand factor, but does not contain factor V. 39. With fibrinolytic therapy, the goal is to directly or indirectly enhance the generation of which enzyme? A. Factor VIIa B. Thrombin C. Plasmin D. Factor Xa E. Fibrinogen 40. A 30 year old woman presents with easy bruising. She is on no medications. Her physical exam is normal except for petechiae on her legs. Hb, wbc with differential, PT & PTT are all Dropped normal. Platelet count is 3,000. Renal function is normal. She most likely has: A. Decreased megakaryocytes in the bone marrow. B. Platelet plugs in small blood vessels. C. Large platelets on peripheral smear. D. Abnormal expression of GpIIb/IIIa receptors on the platelet surface. E. A normal bleeding time. This was a case of ITP, and large platelets can be seen on peripheral smear in ITP. In ITP there is an increase in megakaryocytes, not a decrease. Platelet plugs in small vessels would be a description of TTP (Thrombotic Thrombocytopenic Purpura). Abnormal expression of GpIIb/IIIa receptors would not result in thrombocytopenia – just platelet dysfunction. The bleeding time in ITP would be abnormal because of the low platelet count. Note that this is NOT a case of DIC – the PT and PTT are normal. It is not TTP or HUS – renal function is normal. 41. A 20 year old medical student cuts himself while shaving. He notes that the bleeding stops immediately (due to vasoconstriction). However, he will soon begin to bleed if he is not able to initiate hemostasis with adhesion of platelets to damaged endothelium. This step is facilitated by the presence of: A. GP Ib receptors. B. Gp IIb/IIIa receptors. C. Fibrinogen. D. Thrombopoietin. E. None of the above. 42. A patient who has had an aortic valve replacement is on therapeutic doses of warfarin (coumadin). She will most likely have a normal level of which factor? A. Factor VII B. Protein C C. Factor V D. Factor X E. Protein S 13 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 43. A 26 year old woman presents with a deep venous thrombosis after flying to Australia. Though she has a predisposing factor (prolonged immobilization), you plan to evaluate her for the presence of a Factor V Leiden mutation because of her young age. Which of the following is true? A. Factor V Leiden is a rare disorder. B. It is more likely that the patient would be deficient in ATIII, Protein C or Protein S. C. Factor V Leiden is only associated with arterial thromboses, not venous thromboses. D. Factor V Leiden is associated with the abnormal function of factor VIII. E. Factor V Leiden is associated with resistance of the factor V molecule to Activated Protein C. 44. A 68 year old man with no history of excessive bleeding (football player, multiple dental extractions) presents for elective gallbladder surgery. He has a normal CBC, normal platelet count, normal PFA and a normal PT, but his PTT is 60 seconds (normal 30 sec). He most likely has: A. Factor XII deficiency B. Factor VIII deficiency C. Factor IX deficiency D. vonWillebrand’s disease E. Factor VII deficiency 45. A patient in the ICU is being treated for hypotension due to bacterial sepsis, and is suspected to have DIC. Which of the following patterns is consistent with this diagnosis? A. Spherocytes, decreased platelet count, increased fibrin degradation products. B. Schistocytes, hypofibrinogenemia. C. Decreased platelets, increased fibrin degradation products, increased fibrinogen. D. Spherocytes, hypofibrinogenemia, long PT and PTT. E. Schistocytes, normal platelet count, increased fibrin degradation products. NOTE: Questions 46 and 47 are related. 46. A 20 year old woman undergoes extraction of her impacted wisdom teeth. The normal hemostatic process should result in the formation of a blood clot and control of bleeding at the site of extraction. The final step in this normal hemostatic process is the conversion of soluble fibrin to insoluble fibrin, which is mediated by: A. Factor II (Thrombin). B. Factor XIII. C. Factor VIII. D. Tissue stabilizing factor. E. Factor XII. 47. If a patient has a deficiency of this factor, what type of bleeding pattern would you expect? A. Immediate bleeding during the extraction. B. Bleeding several hours after the extraction. C. Delayed bleeding (3-4 days later). D. No bleeding. E. You would not expect to see bleeding – you would expect thrombosis. 14 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 48. A 35 year old man comes into the ER with severe crushing substernal chest pain. He is found to have ST elevation across the precordial leads and is taken to the cath lab, where he will receive an infusion of Alteplase (tPA). There is a significant risk of bleeding with this therapy, yet it mimics the physiological process of fibrinolysis. What are the protective mechanisms in physiological fibrinolysis that limit bleeding? A. tPA works best when it is bound to fibrin. 2antiplasmin binds free tPA when it is no longer bound to fibrin. C. Endothelial cells produce PAI-1. D. Endothelial cells produce tPA in a localized fashion at the site of injury. E. All of the above. The vast majority of the class got this answer right based on the intent of the question (Answer E). However, it is true that there is an error in B. 2antiplasmin binds to PLASMIN when it is no longer bound to fibrin. So in reality, it may have been difficult to answer E. Since A, C, and D were all correct, it is difficult to say which is more correct. All answers will be accepted to this question because of this error. 49. A patient has been given an anticoagulant. Which of the following suggests that she has been treated with warfarin and not heparin? A. Anticoagulation is being monitored by measuring the prothrombin time (PT). B. Anticoagulation was achieved within 1 hour of drug administration. C. The anticoagulant’s effects are reversed by administering protamine. D. The anticoagulant was administered intravenously. E. The drug acts via binding to antithrombin III. ANSWER TRUE OR FALSE FOR QUESTIONS 50-52. (These questions are related). A patient is newly diagnosed with a deficiency of factor VIII. In this disorder, 50. The most common bleeding site is the elbow. A. True B. False 51. The number of bleeds per year directly correlates with severity of factor deficiency. A. True B. False 52. The treatment of choice for this disorder is fresh frozen plasma. A. True B. False 53. A 15 year old boy is brought in for evaluation of recurrent severe nosebleeds. He has had no surgical procedures or dental extractions. Laboratory analysis reveals that he has Classic (Type I) vonWillebrand’s disease. Which of the following is most likely? A. He would be expected to have normal factor VIII levels, but decreased vonWillebrand factor and decreased vonWillebrand antigen. B. He should have a proportionate decrease in factor VIII, vonWillebrand factor and vonWillebrand antigen. C. He would have impaired platelet GpIIb/IIIA function. D. He would be expected to have little or no response to DDAVP. E. He would have an elevated prothrombin time (PT). 15 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 54. Which of the following anti-platelet agents is a GpIIb/IIIa inhibitor: A. Aspirin B. Clopidogrel (Plavix) C. Eptifibatide (Integrilin) D. Dipyridamole (Persantine) E. None of the above. 55. You are asked to evaluate an 80 year old woman for multiple ecchymoses. She has had a joint infection and has been on antibiotics for 3 weeks. CBC, platelet count is normal. Dropped PT 25 sec (normal 11 sec). PTT 45 sec (normal 30 sec). She most likely has: A. DIC B. Factor V deficiency C. Low level of Protein C D. Factor X inhibitor E. None of the above. The key here was recognizing that a major source of Vitamin K is endogenous production by bacteria in the G.I. tract. Eradication of normal gut flora because of prolonged treatment with antibiotics can lead to Vitamin K deficiency. As you know, Vitamin K is needed for the synthesis of factors II, VII, IX, and X as well as Protein C and Protein S. Thus the correct answer is C. Note that the patient cannot have DIC – she has a normal platelet count. 56. A surgeon plans to prophylactically treat a patient who has undergone knee replacement surgery with heparin to decrease the risk of deep venous thrombosis. Which of the following statements concerning heparin and low molecular weight heparin is correct? A. Both need frequent monitoring with aPTT to ensure proper therapeutic level. B. In correct therapeutic dose, both have equal antiXa activity. C. Both have comparative risk of patient developing HIT. D. LMW heparin has a longer half-life than unfractionated heparin. E. Enoxaparin is the trade name for unfractionated heparin. 57. Which of the following statements regarding warfarin is correct: A. Blocks gamma-carboxylation of factors II, VII, V, and X. B. In initial 48 hours of starting the drug, patients can become hypercoagulable. C. Unlike heparin, it does not cross the placenta. D. Patients on antibiotics will typically need an increase in the dosage of warfarin to maintain therapeutic effect. E. It has a broad therapeutic window. 16 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 58. A 5 year old boy with no previous medical history is brought to the ER by his mother because he accidentally ingested a large dose of warfarin (coumadin). He is conscious, but appears quite agitated. On PE, his BP is 110/70 mm Hg, and pulse is 90/min. In order to decrease his risk of bleeding, which of the following is the most appropriate pharmacotherapy? A. Activated Protein C B. N-acetylcysteine C. Protamine D. Atropine E. Vitamin K 59. A 48 year old smoker with a deep venous thrombosis is given heparin. Heparin achieves its anticoagulant activity by binding to which of the following substances? A. 2 antiplasmin B. 2 macroglobulin C. Antithrombin III D. Factor VIII E. Prothrombin NOTE: QUESTIONS 60 and 61 are related. 60. A 4 year old boy with a 3 week history of fevers and lack of energy is found to have severe anemia, moderate thrombocytopenia, and a wbc of 12,000 cells/mm3 with 30% blasts, 40% lymphs, 20% polys, 10% monocytes. Physical exam reveals no lymphadenopathy. CXR is normal. A bone marrow biopsy would most likely reveal: A. Acute lymphoblastic leukemia (ALL). B. Acute myeloblastic leukemia (AML). C. Chronic lymphocytic leukemia. D. Chronic myeloid leukemia. E. Hairy cell leukemia. 61. Which of the following statements is true about this disease? A. It is most often a T-cell malignancy in children. B. A good prognosis would be associated with the t(9;22) translocation. C. A good prognosis would be associated with hyperdiploidy. D. The CNS is rarely affected in this disease. E. Oral alkylating agent chemotherapy is highly effective in this disease. NOTE Questions 62-64 are related. A 55 year old woman presents to her physician with fatigue and dyspnea on exertion. On physical exam, she is pale, has no lymphadenopathy or hepatosplenomegaly. CBC reveals an elevated wbc of 25,000, hb 9.5, hct 28.5; platelet count 15 K. Her peripheral blood smear is shown in Figure 8. 17 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ Figure 8. 62. Which of the following is the most likely diagnosis in this patient? A. Acute Lymphoblastic Leukemia B. Hodgkin’s disease with marrow involvement C. Acute Myelogenous Leukemia, M3 D. ITP E. Chronic Myelogenous Leukemia 63. Which of the following chromosomal translocations would you expect to find in this patient? A. t(9;22) B. t(8;14) C. t(15;17) D. t(11;14) E. t(14;18) 64. Which of the following statements is NOT true about this disease? A. It is associated with a significant risk of DIC. B. It is responds well to ATRA (All-trans retinoic acid). C. The molecular defect in this disease is at the transcriptional level. D. Thalidomide is approved for the treatment of this disease. E. Arsenic has been used as a differentiating agent in this disease. NOTE: Questions 65-67 are related. 65. A 25 year old woman presents to her physician after finding a large lump in the right side of her neck which has been present for the past month. She also complains of fevers, frequent drenching night sweats, and a 10 pound weight loss over the past 4 months. On exam, she is found to have an enlarged supraclavicular lymph node and enlarged nodes in the left lower posterior cervical chain and axillary regions. There is no evidence of hepato or splenomegaly. 18 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ Lymph node biopsy reveals the presence of Reed-Sternberg cells with lacunae surrounding the nuclei of these cells. Which of the following variants of Hodgkin disease is most likely present? A. Lymphocyte-Depleted B. Lymphocyte Predominance C. Mixed Cellularity D. Nodular Sclerosis E. Lymphocyte-Rich 66. The remainder of this patient’s workup is negative for additional sites of disease, including a bone marrow aspiration and biopsy. What is her disease stage? A. IA B. IB C. IIA D. IIB E. IIIB 67. This patient completed treatment for Hodgkin lymphoma 1 month ago. She now presents with increasing dyspnea and a non-productive cough. Physical exam is remarkable for fine rales at the lung bases. Arterial blood gases show hypoxia. CXR shows pulmonary fibrosis. Which of the following chemotherapeutic agents most likely produced these effects? A. Bleomycin B. Cyclophosphamide C. Doxorubicin D. Etoposide E. Vincristine 68. Which type of Hodgkin’s lymphoma does NOT have “Classical” CD15+ and CD30+ Reed-Sternberg cells? A. Lymphocyte-Depleted B. Lymphocyte Predominance C. Mixed Cellularity D. Nodular Sclerosis E. Lymphocyte-Rich Dropped 69. A 63 year old patient is diagnosed with a myelodysplastic syndrome. An approved drug for treatment of this disease is: A. Cyclophosphamide B. Methotrexate C. Doxorubicin D. 5-azacytidine E. Bleomycin D. is the correct answer. This was covered by Dr. Mega in the lecture on MDS. However, 5-azacytidine was not listed on the pharmacology drug list. 19 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 70. A 57 year old man presents with painless swelling in his neck. Physical examination is remarkable for a 2 cm cervical lymph node & splenomegaly. Biopsy of the cervical node reveals a neoplasm containing small, cleaved cells that recapitulate the normal follicular architecture of lymph nodes. Which of the following mechanisms is most likely involved in the development of this patient’s neoplasm? A. Amplification of L-myc B. Homozygous loss of p53 C. Overexpression of bcl-2 D. Point mutation in ras decreasing its GTPase activity E. Reciprocal translocation between chromosome 9 and 22. 71. A 67 year old man presents with progressive pruritic erythroderma, exfoliation, and lymphadenopathy. Examination of the peripheral blood smear reveals lymphocyte-like cells with cerebriform nuclei. These cells are CD4+. Which of the following is the most likely diagnosis? A. Burkitt lymphoma B. Diffuse Large B Cell lymphoma C. Lymphoblastic lymphoma D. Hodgkin’s lymphoma E. Sezary syndrome 72. A 70 year old man presents to the ER with a fever of 101, CXR revealing pneumonia and the following CBC: Hb 5, Hct 15, platelet count 30,000, wbc 15,000 with 10% polys, 80% blasts, and 10% lymphocytes. He most likely has: A. A chromosomal translocation resulting in over-expression of c-myc. B. Maturation arrest of myeloid series in the bone marrow. C. Leukemoid reaction secondary to infection. D. Bone marrow fibrosis. E. Chronic Lymphocytic Leukemia. 73. A 70 year old man was recently diagnosed with myelodysplastic syndrome. The data which will be most helpful to you in determining which prognostic group a patient with MDS falls into would be: A. Degree of anemia B. Size of spleen C. Presence of Philadelphia chromosome D. Number of cell lines involved. E. Degree of thrombocytopenia. 74. A 60 year old woman is receiving chemotherapy for Non-Hodgkin’s lymphoma. Several days after a treatment, she notices blood in her urine. Which of the following chemotherapeutic drugs is most likely responsible for this side effect? A. Bleomycin B. Cisplatin C. Cyclophosphamide D. Doxorubicin E. Vincristine 20 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ The correct answer to this was C. Cyclophosphamide, which causes hemorrhagic cystitis. However this point was not emphasized by Dr. Lazo in his antineoplastics pharmacology lecture, and it is clear that many of you answered B. Cisplatinum because of its associated renal failure. Though hematuria is not a typical presentation of cisplatinum renal toxicity, this is not something you might know. Therefore we did accept answers B and C for this question. NOTE: QUESTIONS 75-77 are related. A 62 year old man presents to his physician for his annual physical exam. He is found to have an elevated white blood cell count, with a normal Hb and platelet count. His peripheral blood smear is shown in Figure 9. Figure 9. 75. What is the most likely diagnosis based on the presentation and peripheral blood smear? A. Chronic Lymphocytic Leukemia B. Hairy cell leukemia C. Non-Hodgkin’s lymphoma D. Richter’s syndrome E. Sezary syndrome 76. Which of the following pattern of markers would be most consistent with this diagnosis? A. CD4 and CD3 positivity B. CD5, CD23, and CD20 positivity C. CD33 positivity D. Tdt positivity E. CD19 positive, CD20 positive, CD5 negative 77. Which of the following statements about this disease is true? A. It is staged using the Rai or Binet Staging classifications. B. This disorder arises solely from cells that have unmutated Ig heavy chain variable region genes. C. It is treated aggressively using combination chemotherapy and Rituximab with an aim for cure. D. Chromosomal translocations are not found in this disorder. E. Patients with this disease invariably die from progression to acute leukemia. 21 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 78. Drug “sanctuaries” are potential problems for curative treatment with anticancer drugs. One common physiological cause for the development of drug sanctuaries is: A. Protein binding. B. Hypothermia C. Alopecia D. Hypoxia E. Pancytopenia 79. An 80 year old male has been followed for two years with a hemoglobin of 10, MCV 102, wbc 3000 with 40% polys, 40% lymphocytes and 20% monocytes. Platelet count 40,000. Retic count 1%. An iron stain of his bone marrow aspirate is shown in Figure 10. Bone marrow smear, Iron stain, 1000x Figure 10. He most likely has: A. B12 deficiency. B. Myelodysplasia. C. CLL. D. Autoimmune hemolytic anemia and thrombocytopenia (Evan's syndrome). E. Iron overload due to hemochromatosis. 80. A 35 year old man has been followed for 4 years with a diagnosis of Idiopathic Hypereosinophilic Syndrome. Which of the following is NOT true of this disorder? A. Dramatic responses have been seen with imatinib (Gleevec). B. This disease may be due to a chromosomal alteration that results in constitutive activation of a tyrosine kinase. C. It is defined by a sustained high-grade eosinophilia without a definable secondary cause. D. It presents with clinical and laboratory similarities to CML. E. There is no effective treatment for this disease. 81. A 64 year old man presents with progressive weakness, recurrent fever, and night sweats. On physical examination, he is found to have multiple enlarges lymph nodes in the lateral cervical region. A lymph node biopsy demonstrates diffuse effacement of the nodal 22 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ architecture by uniform sheets of large atypical lymphoid cells with frequent mitoses. Which of the following is the most likely diagnosis? A. Diffuse Large B Cell Lymphoma B. Hodgkin lymphoma C. Follicular lymphoma D. Small Cell Lymphocytic Lymphoma (SLL/CLL) E. Reactive follicular hyperplasia. NOTE: Questions 82 and 83 are related. A 50 year old man presents with fatigue. He is found to have a palpable spleen and a wbc of 50,000, Hb 9, and a platelet count of 400K. His peripheral blood smear is shown in Figure 11. Figure 11. 82. He most likely has: A. A clonal disorder affecting wbc, rbc, platelets, and fibroblasts. B. A clonal proliferation of the committed myeloid precursor. C. Decreased basophils on bone marrow. D. An abnormal tyrosine kinase affecting myeloid maturation. E. A leukemoid reaction. Although this question might have been written more clearly, the key point here was that CML is a clonal disorder of the PLURIPOTENTIAL stem cell – not the committed myeloid precursor. Answer B should be incorrect because the defect lies in the pluripotential stem cell – not in the committed myeloid precursor. However, one could argue that there is a clonal proliferation of the myeloid precursor as a result of the clonal proliferation of the pluripotential stem cell. For this reason, we will accept answer B in addition to answer D. 83. Other laboratory findings that would be consistent with this diagnosis include which of the following: A. Elevated Leukocyte Alkaline Phophatase Score (LAP) B. Normal cytogenetics. C. An M:E ratio in the bone marrow of 1:3. D. An M:E ratio in the bone marrow of 20:1. E. Presence of all stages of myeloid development except the myeloblast. 23 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 84. An acceptable treatment for a patient with P.Vera who has a platelet count of 1.2 million is: A. Phlebotomy only B. Hydroxyurea C. Alkylating agents D. Prednisone E. Rituximab 85. Methotrexate is one of the chemotherapeutic agents which is active against Acute Lymphocytic Leukemia. What is it’s mechanism of action? A. Topoisomerase II inhibitor. B. Alkylating agent. C. Blocks tubulin polymerization. D. Inhibits ribonuclotide reductase. E. Inhibits dihydrofolate reductase. 86. A 65 year old man complains of weakness, weight loss, and bone pain. He reports having progressive difficulty seeing. Physical exam is significant for hepatosplenomegaly and lymphadenopathy. Serum protein electrophoresis reveals an M-protein spike, with an elevated serum IgM level. Bone marrow aspiration shows plasmacytoid lymphocytes. Which of the following is the most likely diagnosis? A. Heavy chain disease B. Monoclonal gammopathy of undetermined significance C. Multiple Myeloma D. Plasmacytoma E. Waldenstrom’s Macroglobulinemia NOTE QUESTIONS 87 and 88 are related. 87. A 70 year old man presents with left sided abdominal pain. He is found to have moderate splenomegaly. CBC: wbc 80,000 with 4% blasts, 12% promyelocytes, 15% myelocytes, 12% metamyelocytes, 9% bands, 8% polys, 23% lymphocytes, 14% monocytes, 3% basophils. The treatment of choice in this patient would be: A. Leukopheresis. B. Hydroxyurea. C. Alpha Interferon. D. Imatinib mesylate (Gleevec) E. Rituximab (Rituxan) 88. Which of the following statements is true about this treatment: A. It results in the highest rate of cytogenic responses (with the exception of bone marrow transplantation). B. It is administered intravenously because it has a short half-life. C. It has a high rate of side effects and “intolerance”. D. It is a relatively inexpensive form of therapy. E. There is no evidence of resistance to this treatment regimen. 24 Integrated Hematology Exam 11/21/06 Dropped Name:_______________________ID#:___________ 89. Novel therapies that are being used in Multiple myeloma include all of the following except: A. Melphalan and prednisone B. Velcade (Bortezomib) C. Thalidomide D. Revlimid (Lenolidomide) E. Tandem stem cell transplants. Melphalan and prednisone have been in use for 30+ years. The other treatments are all new therapies for MM. 90. A patient was recently diagnosed with Diffuse Large B Cell Lymphoma. Which of the following is NOT a significant prognostic factor in this disease? A. Age B. Serum LDH C. Performance Status D. Gene expression profiling E. Chromosomal abnormalities 91. Anticancer drugs are frequently classified by their mechanism of action. Cyclophosphamide is an example of a/an: A. Alkylating agents B. Topoisomerase II inhibitor C. Antimetabolite D. Antisignaling agent E. Intercalating agent 92. Which of the following statements is NOT true regarding radiation biology? A. The amount or quantity of radiation is expressed in terms of absorbed dose. B. 1 Gray (Gy) is equivalent to 100 rad. C. Fractionation gives normal cells a chance to repair during the time between treatments. D. The most characteristic lethal DNA lesion after a dose of ionizing radiation is the single base pair deletion. E. Greater doses of radiation are required under hypoxic conditions than in oxic conditions to provide equivalent cell killing. 93. Irradiation of water can produce harmful products such as hydroxide radicals. Of the total cell weight, water represents: A. 5-7% B. 22-27% C. 30-35% D. 50-55% E. 80-85% 94. The “4R’s” of radiation biology include all of the following, EXCEPT: A. Repair B. Revascularization C. Repopulation D. Reoxygenation E. Redistribution 25 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 95. Which tissues are affected most by each of the “4Rs”? A. Normal early responding tissues. B. Normal late responding tissues. C. Tumor cells. D. Hypoxic cells. 96. A 67 year old patient with an L4 lytic lesion due to multiple myeloma is undergoing radiation therapy. Which of the following statements are true? A. Fibrosis may be an acute toxicity that will limit delivery of full doses of radiation. B. Effects are most evident in rapidly dividing tissues such as lung. C. Toxicities do not resolve, and are dose-limiting. D. A smaller dose per fraction causes more damage to normal tissue relative to tumor. E. Different dose fractionation schemes can result in a wider therapeutic window. 97. A 55 year old man presents with left upper quadrant abdominal discomfort and fatigue. On exam he has moderate splenomegaly and scattered petechiae on the lower extremities. Laboratory studies reveal pancytopenia. An attempt at a bone marrow aspirate was unsuccessful. If you are able obtain cells for analysis, the following would confirm the diagnosis you suspect: A. The presence of T-cell markers. B. The presence of CD33 and CD13. C. Cytochemical staining revealing resistance to Tartrate Acid Phosphatase. D. Presence of CD30 and CD15+. E. Presence of GpIIb/IIIa. Dropped 98. Which of the following lymphomas is the only one to be “graded” histopathologically? A. Diffuse Large B Cell lymphoma B. Mantle cell lymphoma C. Marginal zone lymphoma D. Follicular lymphoma E. Hodgkin’s disease. This was covered by Dr. Griffith’s lecture. Follicular lymphoma is the only type of lymphoma that is graded histologically. I’m guessing that many of you confused Staging and Grading? Grading is typically used to describe the degree of differentiation of a tumor by histologic (microscopic) examination. A Grade I tumor is typically well-differentiated. In many tumor grading schemes, Grades IV-V are undifferentiated or anaplastic. In follicular lymphoma, grading is an indication of large cell component (remember that follicular lymphomas can transform into DLBCL – a poor prognosis event). Follicular lymphomas are graded into three groups: I, II and III. Stage III has the highest large cell component and the highest likelihood of transformation. [As a reminder, STAGING refers to extent of spread of the primary tumor]. Answer True or False to the following questions (99-102): 99. Mantle cell lymphoma is associated with overexpression of Cyclin D1. A. True B. False. 26 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ 100. HIV-associated lymphomas typically include follicular lymphoma and SLL. A. True B. False 101. Adult T Cell Leukemia/Lymphoma is associated with EBV. A. True B. False 102. Marginal Zone lymphomas have an overall poor prognosis. A. True B. False 103. Which of the following is NOT an accurate statement about treatment of Follicular Lymphoma? A. Because it is an indolent disease, “watching and waiting” is an option. B. It is typically cured with standard chemotherapy agents. C. First line treatment of previously untreated patients may be combination chemotherapy (cyclophosphamide, vincristine, and prednisone) + Rituxan. D. Radioimmunotherapy with tositumomab (Bexxar) and ibritumomab tiuxetan (Zevalin) are undergoing currently undergoing evaluation for initial treatment of this disease. E. Progression to a more aggressive disease occurs at a rate of ~5% per year depending on degree of large cell component present. 104. Patients who undergo syngeneic bone marrow transplantation have: A. Increased risk of graft vs. host disease when compared with allogeneic transplant. B. Higher relapse rates when compared with allogeneic transplant. C. Have increased graft vs. leukemia effect when compared with allogeneic transplant. D. To remain on immunosuppressive therapy for life. E. None of the above. Answer True or False for Questions 105-106: 105. The possibility of long term survival after allogeneic bone marrow transplant is better in HLA-matched siblings than in matched unrelated donors (MUD). A. True B. False 106. T-cell depletion in allogeneic transplant decreases graft-vs-host disease and therefore increases survival. A. True B. False 107. Which of the following is not consistent with acute graft-vs-host disease? A. Rash Dropped B. Diarrhea C. Increased bilirubin D. Features of scleroderma E. Desquamation 27 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ Scleroderma is a feature of CHRONIC graft-versus-host disease. Desquamation may be one of the skin manifestations of severe ACUTE graft-versus-host disease. NOTE: Questions 108 and 109 are related. A 6 year old child presents with a rapidly enlarging abdominal mass and visible ascites. Mom says the child only became really sick in the last 3 weeks. The bone marrow biopsy aspirate is shown in Figure 12. Figure 12. 108. This child’s presentation and bone marrow aspirate are most consistent with a diagnosis of: A. Acute Myelogenous Leukemia (AML) B. Burkitt’s lymphoma C. Diffuse Large B cell lymphoma D. Wilm’s tumor E. Neuroblastoma 109. Which of the following is true of this disease? A. This clinical picture of a rapidly growing abdominal mass in a child is the most common presentation of this disease world-wide. B. This is an indolent, or slow-growing disease. C. Tingible-body macrophages are a prominent feature of the histopathology. D. This disease is not curable. E. This disease is a mature, peripheral T cell malignancy. 110. The therapeutic action of imatinib (Gleevec) involves inhibition of: A. Microtubule association B. Tyrosine kinase activity C. Tetrahydrofolate uptake D. DNA polymerase activity E. RNA polymerase activity 111. A common side effect resulting from treatment with either cyclophosphamide or doxorubicin would be: A. Loss of taste sensation B. Ototoxicity (ear toxicity) C. Myelosuppression D. Increased appetite E. Night blindness 28 Integrated Hematology Exam 11/21/06 Name:_______________________ID#:___________ ADDENDUM: NORMAL LABORATORY VALUES Wbc (cells/l) Hemoglobin (g/dl) 4,500-10,000 13.5-17.5 (male) 11.5-15.5 (female) Hematocrit (%) 40-52 (male) 36-48 (female) MCV (fl) 80-100 MCH (pg) 27-34 MCHC (g/dl) 20-35 (mean corpuscular Hb concentration) Platelet count 150,000 to 400,000/mm3 PT 10-12 sec aPTT 25-38 sec Creatinine (mg/dl) 0.5-1.4 Total Bilirubin (mg/dl) 0.1-1.2 Direct Bilirubin (mg/dl) 0-0.3 LDH (IU/L) 56-194 Iron (Fe) (mcg/dl) 65-150 TIBC (mcg/dl) 250-420 Ferritin (g/L) 15-200 (male) 12-150 (female) 29