Consult Request - UNM Medical Group
advertisement

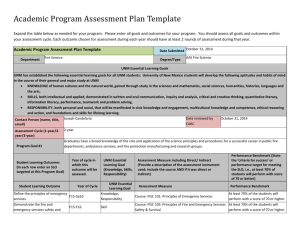
Date: _________________ EXTERNAL REFERRALS University of New Mexico Hospitals UNM Vein & Cosmetic Center (UNM Medical Group) Consult Request Thank you for your referral. UNM Vein & Cosmetic Center accepts most insurance. Fax completed form to UNM Vein & Cosmetic Center @ (505) 272-3527. Should you have any questions, please contact the UNM Vein & Cosmetic Center (UNM Medical Group) @ (505) 272-8346. Patient Name: _________________________________________________________ DOB: ______________ Patient Phone Number/s: ________________________________________________ Patient Language Preference: _____________________________________________ Referring provider/clinic: _______________________ / _______________________ Primary Care Provider: ___________________________________________________ Referring Clinic Address: _________________________________________________ Referring Clinic Phone/Fax Number:______________________/__________________ __________________________________________ (Provider Signature) Referring information checklist: □ Referral Face Sheet (with complete demographics) □ Current Medication List □ Copy of Insurance Card □ PA Requested Priority: □ ASAP □ Routine – Please call 272-8346 if you are requesting a same day appointment Please □ □ □ □ □ □ □ choose the appropriate reason for the consult: Varicose veins Spider Veins/Sclerotherapy Reconstruction after Mohs Surgery Blepharoplasty Breast Reconstruction Botox/Fillers Other: ___________________ CPT Code: _______________________________ ICD 9 Code:_________________________________ Please attach additional information that you believe would assist us in providing the best care to your patient.