1 - eCommons@Cornell
advertisement

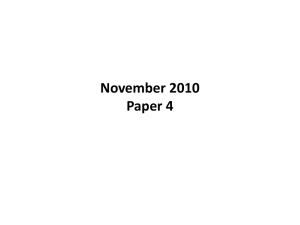
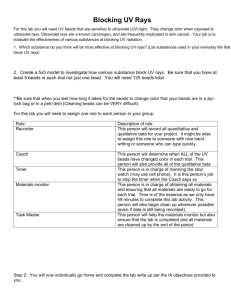
1. INTRODUCTION 1.1 Biosensor Definition and Fields of Use In recent years, the use of biosensors has been recognized as having potential in widespread analytical applications. A biosensor can be defined as “a self-contained integrated device that is capable of providing specific quantitative or semi-quantitative analytical information using a biological recognition element (biochemical receptor) which is in direct spatial contact with a transduction element.[1]” A bioanalytical sensor incorporates a biological element such as an enzyme, antibody, nucleic acid, microorganism or cell. Currently, bioanalytical sensors have been utilized in three main areas[2]: Medicine and healthcare for clinical diagnosis, pharmaceutical and drug analysis, and bacterial and viral analysis. Environment for pollution control and monitoring Quality assurance and process control for fermentation, food and drink Biosensors have many advantages over other detection methods. Use of biologically derived compounds allows specific analyte measurements with great accuracy. Unlike other bioanalytical methods such as ELISA and other immunoassays, the analyte can be measured directly and instantaneously; there is no need to wait for results from lengthy procedures that must be carried out in laboratories. By combining the receptor and transducer into one single sensor, a biosensor enables measurement of target analytes without requiring steps that uses many reagents to treat the sample. Thus, the detection method is greatly simplified. Another benefit of 1 biosensors over traditional detection methods such as immunoassays and ELISA is the highly selective, fast, simple, and continuous detection that occurs with biosensors. In fact, biosensors promise several distinct advantages to the health-care sector over conventional analytical techniques. Biosensor-based medical instruments can be used for the monitoring of patients during intensive care and surgery and diagnosing patients. Biosensors are attractive for following reasons [3,4,5]: They may be designed as inexpensive, disposable devices requiring little or no expertise for their use. They allow the quantitative detection of specific species in complex samples without the need for sample processing or purification. These features provide the opportunity for sample analysis to be performed outside hospital’s analytical laboratory to the doctor’s office and the patient’s bedside, and for self-testing in the home. The volume of sample required can be reduced from ml to μl. Results may be obtained immediately in situations where delay may be critical, for example in ICU Departments, or sensors may be implanted to allow continuous monitoring of patient status Multi-analytical devices allow quantification of several species simultaneously. One area of heath care sector that can utilize biosensors is in cell enumeration using immunophenotyping. The immunophenotyping of cell is commonly used in clinical medicine as a way to assess the patient’s condition and monitor the disease progression. 2 1.2 Immunophenotyping of Human Blood Cells The human immune system is comprised of organs and leukocytes that defend the body against disease and infection. The leukocyte family consists of polymorphonuclear neutrophils, lymphocytes, monocytes, and basophils, which function uniquely from each other. Leukocyte cell surface molecules are named systematically by assigning them a cluster of differentiation (CD) antigen number that includes any antibody that has an identical and unique reactivity pattern with different leukocyte populations. Table 1 lists some CD antigens and the cells that express them. CD antigen Cellular expression CD2 T cells, thymocytes, NK cells CD3 Thymocytes, T cells CD4 Thymocyte subsets (helper & inflammatory T cells), monocytes, macrophages CD8 Thymocyte subsets (cytotoxic T cells) CD15 neutrophils, eosinophils, monocytes CD16 neutrophils, NK cells, macrophages CD18 Leukocytes CD19 B cells CD28 T cell subsets, activated B cells CD29 Leukocytes CD30 Activated B and T cells CD34 hematopoietic precursors, capillary endothelium CD36 platelets, monocytes CD40 B cells, monocytes, dendritic cells CD45 Leukocytes CD46 hematopoietic and non-hematopoietic nucleated cells CD48 Leukocytes CD72 B cells Table 1: List of some CD antigens specific for cell types. [6] 3 Different subtypes of leukocytes can be distinguished from using the combinations of receptor proteins on the surface of the cell. For example, all leukocytes contain CD45 receptors on their surface. Lymphocytes circulate in the blood and aid in defending the body against infections and the intrusion of foreign materials. Two main classes of lymphocytes are T cells (produced from the thymus) and B cells (produced from the bone marrow). All T cells have CD3 protein on the surface membrane. Current cell enumeration techniques have used the surface markers for separation and identification. 1.3 Cell Enumeration Applications 1.3.1 Cell Enumeration for Human Immunodeficiency Virus Diagnostics 1.3.1.1 HIV Background The human immunodeficiency virus (HIV) infection can lead to Acquired Immunodeficiency Syndrome (AIDS) and ultimately to death. According to the Joint United Nations Program on HIV/AIDS (UNAIDS), approximately 37.8 million people live with HIV, and 20 million people have died from AIDS as of the year 2003 [7]. Early HIV detection allows early application of antiretroviral therapy that can prevent AIDS and prolong health. The antiretroviral therapy works by reducing the amount of virus in the body and can dramatically slow the deterioration of the immune system. For example, the government of Brazil estimates that antiretroviral treatments, that suppress activities of retrovirus such as HIV, have decreased mortality rates by 50%, morbidity rate by 60-80%, and the hospitalization of HIV positive people by 70%.[7] 4 1.3.1.2 HIV Diagnosis HIV binds to CD4 receptors on the T helper cells (CD4 cells) and then uses the lymphocyte as a host to multiply its genes. Thus with the increase in the number of HIV in the blood, more CD4 cells get infected and destroyed which leads to a significant drop in CD4 cells in the patient’s blood. In the United States, two types of techniques are used to detect HIV infections in people. One technique directly detects the HIV-RNA concentration in blood samples and the other one indirectly detects HIV level by determining the number of CD4 cells in the patient’s blood. The CD4 absolute count requires the total white blood cell count, the percentage of white cells that are lymphocytes, and the percentage of lymphocytes that express CD4. [8] An HIV infection can cause AIDS principally because of the depletion of CD4 lymphocytes. Healthy people have approximately 435 to 1500 CD4 cells per micro liter of blood [9]. Once a person is infected with HIV, the virus target CD4 cells and replicates at an exponential rate while destroying the CD4 cells. Then the immune system reaches a point where the rate of viral replication exceeds the rate of CD4 cell production. As a result, the immunologic function of the body weakens, and the body becomes more susceptible to diseases and other viral infections. Antiretroviral drugs can reduce the concentration of virus and thus stop further reduction of CD4 cells [8]. Antiretroviral therapies are initiated when the CD4 cell count is less than 350 cells per micro liter [9] or 14% of total number of lymphocytes [10]. CD4 cells bear CD3, CD4, and CD 19 receptors on the surface as well as CD 45 receptors. These receptors exist in other cell types as well, but only T helper cells have a combination of all CD3, CD4 and CD45. This characteristic of T helper 5 cells is used in the determination of the concentration of CD4 cells by flow cytometry, since the progressive depletion of CD4 cells is the chief event in pathogenesis during an infection by HIV. The absolute number of these CD4 Cells in the peripheral blood is the single most important parameter for monitoring the disease associated with HIV infection. Thus, CD4 cell enumeration is essential in three areas. First, initial CD4 counts are used to find the degree of a person’s immune deterioration. The CD4 tests are repeated to monitor a change in the CD4 count and to define a declining slope of CD4 counts as an indication of the speed of progression toward AIDS. With the help of baseline CD4 counts, patients are placed in care to start antiretroviral therapy and to define a starting point for “efficient prophylaxis against opportunistic infections.” Second, while the patient is on the antiretroviral therapy, improvements in CD4 counts indicate whether the therapy is effective. Finally, CD4 counts are used to prepare for an anticipated health care need in any one region through an epidemiological AIDS surveillance[11]. Thus, flow cytometry provides a methodology for multiparameter analysis of blood cells, at the single cell level. The analyte of major interest is the absolute CD4 count, however that number is meaningless by itself, as opposed to that the result in the context of a full complete blood count (CBC). Therefore, in addition to the absolute CD4, the CD4 percentage, along with CD3 percentage and CD3 absolute count are also reported. In fact, this lymphocyte subset analysis, entailing determination of percentages and absolute counts for CD3 (pan T), CD3/4 (T-helper), CD3/8 (T-cytotoxic/suppressor), CD16+56 (NK) and CD19 (pan-B) is performed on all submissions from patients with any 6 suspected immunodeficiency condition. Though the latter three are not reported for routine CD4 requisitions, the data is available if needed. The additional analyses are performed to facilitate internal quality control for the test.[12] 1.3.2 Other Cell Enumeration Applications Cell enumeration can be used for lymphocyte subset analysis for diagnosis and evaluation of the immunological status of a patient. Changes in the lymphocyte subsets can indicate immunological changes produced by various diseases or treatments. Helper/suppressor cell counts, including total T cell (CD3), helper T cell (CD4), suppressor cell (CD8), natural killer cells (CD16, CD56), and white blood cell and absolute lymphocyte counts, are used as a general screening in cases where there is no knowledge of the underlying cause of disease.[13] Lymphocyte subsets (CD3 and CD4 T cells and CD19 B cells) are monitored on patients undergoing bone marrow transplants with peripheral stem cell products and chemotherapy. Cell numbers can be used in evaluating these patients for disease remission, or transplant rejection. After an organ transplant, CD3 cell level is measured during immunosuppressive therapy. This therapy causes a disappearance of T cells. Thus, steady rise in the T cell demonstrates a failure to respond to therapy. Immunophenotyping of CD34 is used to determine the number of hematopoietic stem and progenitor cells. These stem cells are necessary for reconstituting the bone marrow. Bone marrow transplant patients undergo a series of procedures that enhance CD34 production, collect CD34-enriched products, destroy the diseased bone marrow and then return the CD34 enriched products back to the 7 patient.[14] More extensive cell enumeration by immunophenotyping is used to distinguish Chronic Lymphocytic Leukemia from a generalized increase of lymphocytes or to distinguish Acute Lymphoid Leukemia from Acute Myeloid Leukemia. [15] 1.4 Cell Enumeration Methods 1.4.1 Flow Cytometric Immunophenotyping Flow cytometric immunophenotyping is the golden standard for cell enumeration and has been used routinely in diagnostic analyses since its first commercialization in the 1950s.[16] Flow cytometry uses a cytometer to simultaneously and rapidly measure various physical and chemical properties of single particles or cells as they “flow in a fluid stream one by one” through a beam of light[17]. Each cell is correlated with its own characteristic scattered lights and fluorescent lights[18]. A flow cytometer consists of three main systems: a fluidic system, an optics system, and an electronics system. The fluidic system contains a flow chamber that transports particles or cells in suspension and sheath fluid in a single file. The transported particles then pass by the optics system, which has a light source (e.g., laser), filters, and a light collecting lens. Then the detector converts the collected light signals into electronic signals that can be processed and displayed as a graph on the computer screen. For cell enumeration, fluorescence detection is used in addition to side and forward scatter detection. A fluorescent probe is utilized to label other probes through covalent bonding and to indicate particular composition of the cell or to 8 directly stain the cell to analyze cell structure[19]. In the case of cell immunotyping, fluorescent probes are coupled to anti-antibodies, which bind to specific surface receptors, and distinguish sub-populations of differentiated cell types.[20] Initially, a dual-platform (two instruments) technology has been used for cell enumeration. For the measurements using dual-platform technology, the absolute lymphocyte count generated from the hematology analyzer is combined with cell count, for example CD4 T cells, from the flow cytometer to obtain a CD4 percentage of lymphocytes.[21] Using two instruments, however, increases human handling of samples and decreases accuracy. Difficulty arises in direct comparisons of hematology results between different types of instruments in different laboratories because of the time constraint in shipping blood to multiple locations.[22] Demand for accurate cell counts led to a development of a single-platform technology where the absolute numbers of lymphocyte populations as well as CD cells are obtained only by flow cytometry [23]. Single platform analysis can be done by using different color fluorochromes. Adding more fluorochromes to the analysis allows the gathering of more information, uses less sample volumes and thus results in a lower number of tubes, and requires less preparation and analysis time per patient.[19] One disadvantage of flow cytometer is the requirement of specialized equipment, such as the Beckton Dickinson FACS-Calibur or Coulter Systems cytometers. The equipment is quite expensive (at least $50,000) and each assay bears significant costs, for example the fluorochrome-conjugated antibodies can cost $20 to $30 per test [24]. 9 1.4.2. CD4 Enumeration Techniques In the case of CD4 enumeration, other diagnostic strategies that minimize the amount of specialized equipment used are available. For example, the Coulter Manual CD4 Count kit allows manual count of CD4 cells using microscopy by employing latex spheres coated with murine monoclonal antibody. Crystal violet–stained CD4+ T lymphocytes with beads attached are identified by counting in a hemocytometer.[25] The Dynabeads T4-T8 system is very similar, to the Coulter Manual CD4 Count kit. It uses antibody coated magnetic particles (Dynabeads). Here, the CD4 cells captured by the dynabeads are separated from the whole blood by a magnet, the cells are lysed and the nuclei are stained with Sternheimer-Malbin staining solution (containing crystal violet, safranin O, ammonium oxalate, and ethanol and counted. Both systems also use beads coated with another antibody, anti-CD14, to remove monocytes from CD4 T cells.[25] 1.5 Objective The objective of this project is to design a biosensor that quantifies the amount of T-lymphocytes in human blood. A microfluidic biosensor based on liposome signal generation and amplification is adapted to the detection of the T-lymphocytes using two specific sets of antibodies recognizing proteins on the surface of the cells. The project focused on the design and optimization of the device in order to produce an accurate, reliable detection system. 10 2. DESIGN 2.1 Analyte The analytes of interest are T lymphocytes in human blood. A sandwich detection approach is used in order to separate all T-lymphocytes from the remaining cells in the blood sample. Thus, the CD45 marker is used to separate the leukocytes from other cells in the blood sample. CD3 maker is used to separate the T lymphocytes for subsets of leukocytes. Overall, CD3 T cell counts can be used as positive control in CD4 enumeration for HIV detection and for monitoring immunosuppressive therapy. 2.2 Liposome-Bead Sandwich Detection Liposomes are small, spherical vesicles that spontaneously form when phospholipids molecules in aqueous solution self-assemble into hollow spheres with an aqueous cavity enclosed by a phospholipids bilayer membrane. Fluorescent dyes can be encapsulated in the liposomes for bioanalytical assay applications as has been shown in numerous applications previously [27,28,29]. Dye encapsulated liposomes are advantageous as signal generators because encapsulation of many dye molecules in one liposome allow for signal amplification leading to extremely low detection limits.. The detection method developed utilizes immunoliposomes and superparamagnetic beads that use biotin-streptavidin interactions to immobilize antiantibodies. Biotinylated anti CD45 antibodies are immobilized onto supermagnetic beads coated with streptavidin and biotinylated anti CD3 antibodies are immobilized 11 onto streptavidin-tagged liposomes. The immuno-liposomes, immuno-beads, and blood sample are incubated. During incubation, the anti-antibodies bind to the specific proteins present on the lymphocytes and produce a sandwich formation as seen in Figure 1. Figure 1: Diagram of trapped of immunobeads in the capture zone of the microfluidic device. Some immunobeads are bound to the white blood cells and subset of those for a sandwich complex as the immunoliposome bind to the T-lymphocytes. This sandwich structure is isolated from the rest of the blood sample by using a magnetic collection of the beads to the rare-earth neodymium-iron-boron magnet placed in a microfluidic channel (see chapter 3.5). Fluorescence from entrapped dye can be detected using a fluorescence microscope. 2.3 Microfluidic Device Use of microfluidics in analytical systems has increased due to its high throughput capacity and smaller sample volume requirement [30]. A microfluidic device designed previously in this laboratory has been applied to the analysis of T- 12 lymphocytes in this project. The microfluidic layout is shown in Figure 2 and will be discussed in more detail in chapter 3.5. PDMS film Glass slide Plexiglas plate screws Figure 2: Top view of assembled microfluidic sensor system with two Plexiglas housing the PDMS with channel grooves and the class slide. 8 screws are used to hold the Plexiglas plates together The biosensor is made in polydimethyl siloxane (PDMS) and packed in Plexiglas to provide connection to the outside world. The well made in the Plexiglas on top of the detection zone provides a place for the magnet. The externally placed magnet allows a way of controlling magnetic beads within the microchannel. This system allows less sample size, human handling, and time. Mixture of liposomes with reporter probes (anti CD3 antibodies), beads with capture probes (anti CD45 antibodies), and target (blood sample) are incubated prior to introduction into the microchannel. The sandwich complexes are captured on the magnet and detected by fluorescence microscope. 13 3. MATERIALS AND METHODS 3.1 Materials and Reagents All general laboratory chemicals and buffer reagents were purchased from Sigma Chemical Company, St. Louis, MO. Organic solvents were purchased from Aldrich Chemical Company, Milwaukee, WI. Lipids were obtained from Avanti Polar Lipids, Alabaster, AL. Sulforhodamine B and Streptavidin were purchased from Molecular Probes Company, Eugene, OR. Superparamagnetic beads (Dynabeads MyOne Streptavidin) were purchased from Dynal Biotech Inc., Lake Success, NY. Silicone elastomer kit Sylgard-184 containing Polydimethyl Siloxane (PDMS) prepolymer and catalyst was obtained from Dow Corning Corp., Midland, MI. The Cornell Nanofabrication Facility (CNF) provided clean room facilities, chemicals and equipment for silicon template fabrication. The Plexiglas housing was constructed in the machine shop located at the School of Chemical and Biomolecular Engineering, Cornell University. Anti-CD3 and CD45 antibodies were purchased from Biodesign International, Saco, Maine. 3.2 Immunoliposome Preparation 3.2.1 Liposome Preparation Liposomes were prepared using the reversed-phase evaporation method. Initially, the encapsulant was prepared by dissolving 150mM Sulforhodamine B (SRB) in a 0.2M HEPES with pH 7.5 and DIUF water. A vapor pressure osmometer was used to measure the osmolarity of the encapsulant. Osmolarity of the encapsulant 14 in 0.2M HEPES was 630 mmol/kg and the osmolarity of the buffer, 0.01M HEPES pH 7.5 was 365mmol/kg. 304.9g of sucrose was added to the buffer to adjust the osmolarity to be 75 mmol/kg greater than the encapsulant. 7.2μmol of diphosphatidyl palmitoylethanolamine (DPPE) was then dissolved in 2mL of 0.7% triethylamine (v/v) in chloroform by sonicating for one minute at 45°C in a round-bottom boiling flask. Then 14.3μmol of N-succinimidyl-S-acetylthioacetate (SATA) was added to the DPPE suspension, sonicated again, and placed on a shaker for 20 minutes, forming the DPPE-ATA compound. The triethylamine was removed by adding 3 mL of chloroform to the mixture and evaporating it under a vacuum in a rotary evaporator at 45°C. The lipids 40.03μmol dipalmitoyl phosphatidylcholine (DPPC), 21.0μmol dipalmitoyl phosphatidylglycerol (DPPG), 51.7μmol cholesterol and the 30.6μmol DPPE-ATA were dissolved in a mixture of 3mL chloroform, 0.5ml methanol and 3mL isopropyl ether. The lipid and organic solution mixture was sonicated in 45°C bath for 30seconds. Then 4mL of SRB encapsulant was added to the organic solution and sonicated for 4 additional minutes until the lipids were completely dissolved. Vacuum rotary evaporator was used to evaporate the excess liquid at the highest rotation speed with the vacuum 380 mbar/hPa for 30 minutes then with the vacuum 280 mbar/hPa for additional 30 minutes. The flask with thick viscous organic solvent was vortexed. Then 4mL of SRB encapsulant was added to the lipid mixture and sonicated for five minutes. The lipids spontaneously formed liposomes entrapping the SRB dye. To obtain uniform liposome size, they were extruded through 2 μm (11 times) and then 0.6μm (11 times) polycarbonate filters from Avanti Polar Lipids using the 15 Avanti mini extruder. The extrusion process was completed at a temperature between 50 to 60°C. These liposomes were purified by gel filtration using a Sephadex G50 column equilibrated with 0.01M HEPES, 0.2M sucrose, pH7.5 solution. After the liposomes were collected from the column, a measurement of the optical density of the liposomes was taken using the spectrophotometer. The spectrophotometer was blanked using the 0.01M HEPES buffer solution. 10μL of liposomes were diluted in 990μL of HEPES buffer. A plot of absorbance at 532 nm versus sample number allowed the high and medium fractions of the liposomes to be determined (Figure 3). At this wavelength and dilution level, high liposomes (tube 17-26) have an absorbance around 0.37 to 0.46 and medium liposomes (tube 11-16 and 27-30) have an absorbance of 0.18 to 0.36. The tubes after the 30th tube showed a significant increase in the signal. These tubes were not analyzed because those contained high percentage of free dye and very small percentage of liposomes. 0.5 Absorbance 0.45 0.4 0.35 0.3 0.25 0.2 0.15 0.1 0.05 0 0 10 20 30 40 Tube Number Figure 3: Absorbance of liposomes at 532 nm after purification using Sephadex G50 column. 16 The liposomes were then purified from any remaining free dye using dialysis membranes in a beaker containing 0.01M HEPES, 0.2 sucrose, pH 7.5. The dialysis membranes containing the liposomes were allowed to stir in the beaker overnight. Free dye not encapsulated by the liposomes filtered out of the dialysis membrane into the buffer solution. To determine exact lipid concentration, Bartlett assay was performed on the liposomes. 3.2.2 Bartlett Assay Bartlett assay was performed to determine the amount of phosphorus in liposomes where one mole of phosphorus is equal to one mole of phospholipids. To make the phosphorus standard, 55.8mg of potassium phosphate dibasic was dissolved in distilled deionized water in a volumetric flask. Water was added until the total volume reached 100mL and the concentration of this solution came to be 3.2 mol of phosphorus per mL The standard was diluted to 16 nmol and these solutions were treated in parallel with the samples. Fiske-SubbaRow Reagent was prepared by adding 100mg of 1-amino-2-naphthol-4-sulfonic acid to 40mL of 15% solution of sodium bisulfite while stirring for 30 minutes. The undissolved acid was filtered through Whatman filter paper and stored in the dark. 20 uL of the liposome samples were pipetted into 30 mL test tubes in triplicate. Phosphate standard were pipetted in triplicate into prelabeled test tubes: 0 nmoles (0uL), 16nmoles (5uL), 32nmoles (10μL), 64 nmoles (20μL), 128 nmoles (40μL), 256 nmoles (80uL). These test tubes were put in the oven for 15 minutes to dry the liquid 17 and then were cooled to room temperature for 5 minutes. 1mL of distilled deionized water was added to all tubes. First, the phospholipids in the liposomes are acid hydrolyzed to inorganic phosphate. This hydrolyzation was achieved by first adding 0.5mL of 10N sulfuric acid (H2SO4) and vortexed for 10 seconds. Then these tubes were placed in the oven for digestion to take place (175oC for 3 hours). And the tubes were cooled to room temperature. 0.1mL of 30% H2O2 was added to the tubes and then tubes were vortexed for 10 seconds. Test tubes were returned to the oven for 1.5 hours; afterwards the test tubes had clear solution. 4.6mL of a 0.22% ammonium molybdate was added to each tube to convert inorganic phosphate to phosphor-molybdic acid. 0.2mL of Fiske-StubbaRow reagent was added and tubes were vortexed for 10 seconds. The tubes were covered with glass marbles and placed in rack in boiling water bath for 7 minutes. The tubes were then quickly cooled in ice water bath to near room temperature. This phosphor-molybdic acid had been quantitatively reduced to a blue colored compound by amino-napththyl-sylfonic acid. The intensity of the blue color was measured using a spectrophotometer at 824nm. The intensity was compared with the calibration standards (Figure 4) to determine the phosphorus content and thus find the phospholipids concentration. 18 Absorbance @ 825 nm 0.35 0.3 y = 0.0012x + 0.0072 0.25 R2 = 0.9975 0.2 0.15 0.1 0.05 0 0 100 200 300 nmol phosphorous Figure 4: Calibration standards of the absorbance measured at 825nm for nmol phosphorous content with triplicates of 3.2μmol/mL phosphate dibasic in volumes of 0, 5, 10, 20, 40, and 80μL. The phosphorous content of the high liposomes were 103.2 nmol per 20μL of sample and of the medium liposomes were 64nmol per 20μL of sample. 3.2.3 Streptavidin Coupling DPPE-ATA, an activated lipid, was incorporated into the initial stages of liposome preparation to allow coupling of streptavidin to the liposomes. For a final mol% tag of 0.2 for streptavidin, 17.86nmol of streptavidin was allowed to react with 8.93μmol total lipids on the liposomes. Initially, streptavidin was derivatized with sulfo-SMCC. To obtain 15 equivalents of sulfo-SMCC per streptavidin molecule (268nmol sulfo-SMCC/mg streptavidin), 45.8 nmoles/μL solution of sulfo-SMCC in DMSO (5.86 μL sulfo-SMCC in DMSO/mg streptavidin) was used. This mixture was 19 incubated for 2–3 h to derivatize the amino-modified nucleotide probes with maleimide groups. The ATA groups on the liposomes were deprotected by deacetylating the acetylthioacetate groups on the surface of the liposomes, generating sulfhydryl groups. 100 equivalent of a 0.5 M hydroxylamine solution (pH 7.0 in 25mM EDTA, 0.1M HEPES: 348mg hydroxylamine HCL, 104 mg EDTA, 238mg HEPES in 10 mL deionized water) was added to the volume of liposomes. Then, for actual conjugation of the streptavidin to the liposomes, the SH-tagged liposomes and the maleimidederivatized streptavidin were mixed and allowed to react on rotating mixer for 1 hour at room temperature, then overnight at 4°C. To quench the excess sulfhydryl groups on the liposomes and the unreacted sulfo-succinimidyl groups on the sulfo- SMCC, 50 equivalents of 0.1M Nethylmaleimide (NEM) in PBS was added and mixed on rotating mixer for 4 hours at room temperature. The tagged liposomes were purified from free reporter probe by gel filtration using a Sephadex G50 column and subsequently by dialysis for overnight using a 0.01 HEPES buffer, 0.2M sucrose, pH 7.5. Liposomes were stored in the dark at 4 °C. 3.2.4 Antibody Immobilization The 10μL of streptavidin conjugated liposomes were combined with 10μL of 100μg/mL biotinylated anti CD3 antibody in 1 to 1 volume ratio. This mixture was allowed to be incubated at room temperature for 1 hour and stored in the dark at 4 °C for up to 5 days. 20 3.3 Antibody Immobilization onto Magnetic Beads The Streptavidin coupled Dynabeads MyOne coated with a monolayer of recombinant streptavidin. Each mg of Dynabeads MyOne Streptavidin binds approximately 300 pmol free biotin or 20 – 25 μg biotinylated IgG. 10mg/mL of beads are concentrated in the stock solution. The concentration of beads in the stock solution is 10 mg/mL and approximately 7-12x10^9 beads are in 1mL. Conjugation of biotinylated antibodies to streptavidin coated superparamagnetic beads was carried out following the manufacturer protocol. First, 2μL bead stock (10mg/mL) were washed two times in 1M PBS, 0.2 sucrose, pH 7 solution and resuspended in 10μL of the same buffer. 5μL anti-CD45-antibodies or 1μL anti-mouse-antibodies were added to the beads and the resultant mixture was placed on a rotator for 30 min at room temperature to allow binding. Subsequently, the beads were washed 3 times with 20μL 1M PBS, 0.2M sucrose, pH 7 solution and resuspended in the same buffer to a final volume of 20μL with bead concentration of 1μg/μL. The immunobeads were stored at 40C for up to 5 days. 3.4 Red Blood Cell Lysis The RBC lysis solution (ammonium chloride, ethylenediaminetetraacetic acid, sodium bicarbonate) was combined with RBC sample in 3:1 buffer to blood volume (30μL of buffer and 10μL of blood) and was mixed by inversion of the Eppendorf tubes. The mixture was allowed to stand for 5 minutes in room temperature to allow RBC lysis to take place. Then the Eppendorf tube was centrifuged for 20 sec at 21 14,000 rpm. The lysed supernatant was removed and the white blood cells were resuspended in 10μL of 1M PBS, 0.2M sucrose, pH 7. 3.5 Microfluidic Device Components Channels were fabricated on PDMS using a 4 inch master patterned silicone wafer with a positive surface relief. The master pattern on the silicon wafer was made using standard photolithography and dry etching technique and was provided by Dr. Natalya Zaytseva. First, a mixture of PDMS prepolymer and curing agent in a volume ratio of 7:1 was prepared and degassed under vacuum. One milliliter of this prepolymer-curing agent mixture was then poured onto the silicone template. A level surface silicone wafer was placed on top of the poured mixture. The obtained sandwich structure (silicone wafer – prepolymer curing agent – silicone wafer) was cured in an oven for two hours at 65°C. Afterwards, the assembled sandwich structure was cooled and the PDMS film with the channel grooves (a replica of the design on the silicone wafer) as shown in Figure 5 was peeled off the master. 500μm 100μm Detection zone with magnet 34,000μm Figure 5: Design and dimensions of the channel patterned onto the PDMS film. The channels are 50μL in depth with the width of the detection zone 500μm and of the winding channels 100μm. The total length of the channel network was approximately 14 cm long with from inlet to outlet length 34,000μm. The number of the straight channels in the serpentine is 40 (38 of the full length and 2 halves) 22 Final thickness of the PDMS film was ~170 m with the channel network dimensions of ~50 m in depth, ~100 and ~500 m in width of the serpentine channels and the detection zone, respectively. The total length of the channel network was 14 cm and the length from inlet to the outlet 3.4 cm. There were 40 straight channels in the serpentine with 38 full length channels and 2 half channels. The inlet (~250μm) and outlet holes were drilled into the PDMS film using a high gauge needle with a blunt end or a borer. Cross sectional and top view of the assembled microfluidic device is shown in Figure 6. Figure 6: Cross sectional view of the assembled microfluidic device. Two Plexiglas plates house the microchannels created by placing the PDMS with the glass slide. A glass cover slip was used to seal the microfluidic channels reversibly. The slip was cut out from a microscope slide and cleansed with chromic acid cleaning solution before being used in the device. A stainless steel tubing (with outer diameter of 0.51 mm and inner diameter of 0.25 mm) was glued into one of the Plexiglas plates at the locations lined up with inlet and outlet holes of the PDMS film. The Plexiglas plates had a well in the area lined up with the detection zone in the PDMS film for placement of magnet required for capturing magnetic beads. The rare-earth neodymium-iron-boron magnet obtained from Grade N40, National Imports, Inc. was 23 used. A leak proof sealing between PDMS and glass substrates was achieved by applying slight pressure by screwing the two Plexiglas plates with 6 to 8 screws. 3.6 Sample Introduction and Analysis 3.6.1 Droplet Assay In an Eppendorf tube, supermagnetic beads, blood sample, and liposomes were incubated for 30 minutes at room temperature in a shaker. After incubation, the tube was placed on the magnet for 2 minutes. The supernatant was removed by aspiration with a pipette while the tube remained on the magnet. Then the sandwich complex of liposome-T lymphocyte-bead in the tube was washed with 1M PBS, 0.2M sucrose, and pH 7 solution. Finally the sandwich complex was resuspended in 1μL buffer and placed on a microscope slide for analysis and quantification. 3.6.2 Microfluidic Assay First, continuous fluid flow through the channel network was established by applying a positive pressure at the inlet using a syringe pump obtained from KD Scientific Inc., Holliston, MA. The top of the steel tubing in the inlet hole was connected to the syringe on the pump by Tygon tubing with an inner diameter of 0.5mm. The channels were prefilled with running buffer (1M PBS, 0.2M sucrose, 0.01% Triton X) at a slow flow rate of 2μL/min to prevent bubble formation. In an Eppendorf tube, supermagnetic beads, blood sample, and liposomes were incubated for 30 minute at room temperature in a shaker. Following the incubation, the mixture was withdrawn into the tube that was connected to the syringe filled with the running 24 buffer. The end of the tube was placed back onto the inlet hole and the sample was loaded into the microfluidic channel through at a flow rate of 5μL/min. The liposomeT lymphocyte-bead complex was captured by the magnet in the detection zone. 3.6.3 Fluorescence Measurement Fluorescence of liposomes was visualized using a Leica DMLB microscope (Leica Microsystems, Wetzlar, Germany). The microscope was set up with a 10/0.25 NA long working distance objective, the appropriate filter set of 540/25 nm band pass exciter and 620/60 nm band pass emitter, and 100 W mercury illumination source. The images of beads in the detection zone were obtained with a digital CoolSnap CCD camera purchased from Photometrics, Tucson, AZ coupled to image acquisition software (Roper Scientific Inc., Tuscon, AZ). The fluorescence was quantified using Image ProExpress software (Media Cybernetics, Silver Spring, MD). 25 4. RESULTS AND DISCUSSION 4.1 Determination of Background Binding Initially, droplet testing was proposed as a way to measure the isolated sandwich complex of liposome- T lymphocyte – beads. Before the actual cell measurement, the liposomes and beads were tested for non-specific binding. Figure 7 below shows the pictures of the mixture of 1μL beads and 1μL buffer solution, 1μL liposome and 1μL buffer, 1μL liposome and 1μL streptavidin conjugated beads, and 1μL streptavidin conjugated liposome and 1μL streptavidin conjugated beads. Figure 78: CCD Image of negative control (1μL beads), positive control (1μL liposome & 1μL beads), liposome unspecifically bonded to beads, and streptavidinylated liposomes unspecifically bonded to beads. The mixture of 1μL beads and 1μL buffer was expected to have no signal and was used as negative control. The mixture of unwashed liposomes and beads (the positive signal) were expected to have the highest signal. Comparison of the liposome and streptavidin conjugated beads versus the streptavidin conjugated liposome and streptavidin conjugated beads showed that having streptavidin on both liposome and beads liposome reduced the nonspecific binding of the two. Problem with reliability came up with the droplet testing. Droplet on a microscope slide formed a meniscus that produced a thick layer of liquid with freely floating magnetic beads. Because the microscope cannot take 3 dimensional images, the thickness of the liquid created 26 layers of beads that could not be properly measured. Therefore, quantification was not possible. Thus instead of using a droplet testing, decision was made to use a microfluidic device was used to detect and isolate the liposome-sample-bead complex. 4.2 Optimization of the Microfluidic Device Operations 4.2.1 Optimization of Running Buffer Initially, 1μL of streptavidin conjugated beads were tested in the microfluidic device. Phosphate buffered saline + 0.2M sucrose solution was used as the running buffer. When the microchannel was viewed through the X10 magnification of the microscope, the beads were spread out at the neck of the channel where the 100μL width channel opened up to the 500μL width capture zone. To solve this problem, 0.01% Triton X was added to the running buffer. When tested with the new buffer, the magnetic beads all passed through the widening neck and congregate at the detection zone. 4.2.2 Optimization of Buffer Flow Rate The magnetic beads were captured on the detection zone within the microchannel by an externally positioned magnet. The distance between the magnet and the capture zone of the microfluidic channel determined the strength of the magnetic field created by the magnet. This distance was determined by the depth of the groove drilled in the Plexiglas housing and the thickness of the PDMS film. The strength of the magnetic field decreased exponentially over distance. Hence, the distance had a big influence on the flow rate; stronger magnetic field (obtained by 27 closer distance) allowed capturing of the beads at a higher flow rate. The thickness of the Plexiglas plate between the magnet and the capture zone was approximately 400um. The beads were introduced into the microchannels at a flow rate of 1μL/min. The capture zone was view through the microscope as the buffer flow rate was increased. When the flow rate reached 4μL/min, beads were pulled off from the capture zone and washed away. To increase the maximum flow rate, the Plexiglas housing was sanded to decrease the thickness. The final thickness was approximately 300um. The same test was repeated; the beads were introduced into the microchannels and the buffer flow rate was slowly increased. The beads started washing off the detection zone only when the flow rate reached 8μL/min. Because the bulky sandwich complex would not withstand the higher flow rate than just the beads could, all the tests from this point on used the flow rate of 5μL/min. 4.2.3 Optimization of Flow Time The minimum flow time that was necessary for consistent signal generation was determined. When the sample that contained the sandwich complex of liposomes – T lymphocytes – beads and residual substances of unbound liposomes, beads, and cells were introduced into the microfluidic device, a range of time was required for the beads to be immobilized on the detection zone and then the residues to be washed away from the detection zone. With the flow rate at 5μL/min and the volume of 10μL (5μL of the sample and 5μL of the buffer) introduced to the device, approximately 2 minutes would be required for all the liquid volume had passed the detection zone and 28 maximum signal would be apparent. From that point, the signal would decrease and the running buffer passes the detection zone and flushes away any unbound substance. The signal would reach a steady state value when all the possible substances are washed. The trend in the signal was observed over time to see the minimum time required for the signal to reach a constant value. Two different samples were introduced for determination of the flow time. First a sample with streptavidin immobilized beads, blood, and streptavidin immobilized liposomes were introduced to the microfluidic device. In this case, no binding should occur and the signal obtained should be considered the inherent background signal of the current device. Then a sample with 1μL immunobeads, 0.1μL blood, and 2μL immunoliposomes were used to determine the necessary flow time. In this case, a sandwich complex should be captured at the detection zone and produce a much higher signal than the first test. In both cases, the time was measured from the point after the sample was injected into the device at a flow rate of 5 L/min and washed with the running buffer at a flow rate of 5 L/min. The results were as expected, i.e. a steady state signal was obtained after about 10 minutes (which correlates to approximately 40 L of washing buffer used in order to clean the capture zone from non-bound liposomes) and the specific signal was about 3x higher than the background signal (i.e. 28.5 and 9.4, respectively) (Figure 8). From this point, all tests were run for 10 minutes before the signal was measured. 29 45 40 35 Signal 30 25 20 15 10 5 0 0 5 10 15 20 25 Time (min) Figure 8: Determination of the minimum flow time needed to wash unbound substances. Signal from sandwich complex (in pink) and 1μL liposome-1μL blood-1μL beads mixtures (in blue) were measure over time at a flow rate of 5 L/min. 4.3 Testing of the Biosensor Components 4.3.1 Negative/Positive Control To determine that the streptavidin immobilized liposomes were correctly prepared and that antibodies were properly conjugated to immunoliposomes and immunobeads, anti-mouse-antibodies were used. Anti-mouse-antibodies bind to any anti-antibodies prepared from a mouse. Anti-CD3 antibody conjugated liposomes and anti-mouse-antibody conjugated beads were prepared. The signal produced by the immunoliposome and immunobead complex should be the maximum possible intensity that would be detected and can be used as a positive control. Anti-mouseantibody conjugated beads were run without liposomes for negative control. The positive control gave the intensity of 85.0 and the negative control showed no fluorescence. 30 4.3.2 Non Specific Binding Test To understand the origin of the non-specific binding observed in the previous Section 4.1, different combinations of streptavidin immobilized beads, streptavidin immobilized liposomes, blood, lysed blood, immunobeads, and immunoliposomes were mixed and ran (Figure 9). Streptavidinylated beads and streptavidinylated liposomes produced a signal of 24.4. However, when streptavidinylated beads were mixed with immunoliposomes, the signal nearly quadrupled to 88.2. The freely floating biotinylated anti CD3 antibodies from the immunoliposome sample interacted with the streptavidin on the magnetic beads and caused a high signal that matched the positive control value from Section 4.3.1. When the beads were coupled with anti-CD45-antibodies and then mixed with the immunoliposomes, the signal decreased by 50% to 46.0. The signal could be due to the uncoupled streptavidin on the beads or the interaction between the antiantibodies CD3 and CD45. However, the beads were coupled with the antibody concentration recommended by the company for saturation and should not have any free streptavidin sites. To see if the non-specific binding was owed to unsaturated binding sites, and if the signal could be reduced, a blocking reagent (0.015% casein, 0.5% PVP, 0.25% gelatin, 1X TBS, 0.002% Tween-20) was used to treat the immunobeads prior to testing. When the treated immunobeads and immunoliposomes were captured, the signal came to be 33.0. The signal decreased by 33% from the untreated immunobeads/immunoliposome sample. Some of the background signals were from 31 the biotin on the mobile antibodies nonspecifically binding to free streptavidin on the beads, but some signal must be due to the interaction of the antibodies. From this point, all tests were run with immunobeads treated with blocking solution. 100 90 80 88.2 60 50 40 45.9 30 33.0 20 immunobeads + immunoliposomes beads + immunoliposomes 0 24.4 beads + liposomes 10 blocked immunobeads + immunoliposomes intensity 70 Figure 9: Comparison of the signal produced by beads/liposomes, beads/immunoliposomes, immunobeads/immunoliposomes, and treated immunobeads/immunoliposomes. 32 4.4 Standard Dose Response Curve For this project, exact count of the blood cell was not obtained. Instead fractions of the blood sample (1μL) were captured (Figure 10) to create the dose response curve using whole blood and lysed blood samples to understand the possible detection limit as seen in Figure 11. (a) (b) (c) (d) Figure 10: Image of the capture zone for whole blood sample. From left: (a) Positive control (antimouse antibody beads-immunoliposome), (b) assay with 100% 1μL blood, (c) assay with 10% 1μL blood, (d) assay with 1% 1μL blood Blood was diluted and used in the assays, as 100% blood sample (concentration fraction 1), 10% blood sample (concentration fraction 0.1) and 1% blood sample (concentration fraction 0.01) diluted in the same solution as the running buffer (PBS, 0.2 sucrose, 0.01% Triton X) right before testing. For a concentration fraction of 2, 2 L of 100% blood were analyzed. For both sets of analysis, a clear dose response could be observed, i.e. the signal increased with increasing blood fraction. The maximum signal obtained for whole blood with 2 L of analyte, the signal was 75.7, approximately 10% below the positive signal. This difference in signal showed that the liposome concentration was not saturated by the CD3 cells and that enough liposome concentrations were used for testing. 33 blood lysed blood positive control blocked immunobeads/immunoliposomes 90 80 70 intensity 60 50 40 30 20 10 0 0 0.5 1 1.5 2 concentration fraction Figure 11: Standard dose response curve of the lysed blood sample and whole blood sample. A positive (red) obtained from testing of anti-mouse antibody conjugated beads with immunoliposomes were drawn to show the maximum signal that can be produced by 1μL of liposomes. Non specific signal produced by blocked immunobeads/immunoliposomes (green) was graphed for comparison. However, for the lowest blood concentration fraction (0.01), the signals increased, which was assumed to be due to non-specific binding of immunoliposomes and immunobeads. Without enough cells bound to the beads, immunoliposomes had more available beads to interact with. Furthermore, in the case of lysed blood (1μL), the signal remained at all times below, whereas the signal from whole blood (1μL) remains above, the background signal discussed in Section 4.3.2. The differences in the signal were closely observed in Figure 12. 34 70 60.1 intensity 60 50 33.0 40 25.7 30 20 10 blocked immunobeads + immunoliposomes lysed blood whole blood 0 Figure 12: Comparison of the signals of whole blood sample (blue) and lysed blood sample (purple) and blocked immunobeads and immunoliposomes (beige). The signal from the test of 1μL immunobeads + 1μL whole blood + 1μL immunoliposomes was determined to be 60.1. The signal from the test of 1μL immunobeads (anti-CD45-antibody) + 1μL lysed blood + 1μL immunoliposomes was 25.71, less than half the value of the whole blood sample. The large difference in the signal strength at same concentration of T-lymphocytes in the sample suggests the possibility of background signals from the unwashed red blood cells. Because red blood cells emitted red fluorescence as SRB, the microscope could not distinguish the difference and would detect signal from both the cell and the liposomes. If the non-specific interaction was consistent with or without the presence of the blood sample, the signals obtained from testing blood samples would be higher than the signal obtained for the non specific binding. However, this was not the case; the signal from the lysed blood sample was lower than the non-specific signal 35 produced by the interaction of the blocked immunobeads and immunoliposomes without the presence of blood sample. This result suggested that the specific binding of the T-lymphocytes onto the magnetic beads reduces the nonspecific binding of the free immunoliposomes. Prior to incubation and injection into the microfluidic device, the immunoliposomes (anti-CD3-antibody labeled) were added after the immunobeads (anti-CD45-antibody labeled) and blood samples were pipette mixed. Binding of the white blood cells could be decreasing the free beads available for non-specific binding. In healthy humans there are approximately 4,500 to 10,000 white blood cells (CD45 labeled cells) per 1μL of blood. Of those white blood cells, 20-50% are lymphocytes with 800 to 2,200 T-lymphocytes per 1μL blood. According to the dose response curve, the 0.01 fraction would have T-lymphocyte count between 8-22 and 0.1 fraction with 80-220 cells. Hence, according to the dose response curve, the detection limit would be at or below the 0.1 concentration, thus 80 – 220 cells could be detected. 36 5. CONCLUSION Microfluidic biosensor using immunobeads as capture probes and immunoliposomes and reporter probes for detection and quantification of Tlymphocytes have great potential for application in the health care system. The tests performed in this study will give better direction to future testing of this biosensor for immunophenotyping. Numerous tests were accomplished to understand the efficiency and reliability of the immunoliposomes as signal probe and immunobeads as capture probe. Preliminary studies of the non-specific bindings of liposomes and magnetic beads were observed using a droplet test. However, varying thickness of the drops produced inaccurate and unreliable signals and instead a microfluidic device was used. Initially, the device was optimized for operation. Running buffer was modified to prevent sticking of the beads to the walls of the microfluidic channels. Then the optimum buffer flow time was determined to be 10 minutes to allow minimum but sufficient time for washing of unbound cells and liposomes. Following the operation modification, the biosensor components were tested. Coupling of anti-antibodies almost doubled the nonspecific binding signal of liposomes and magnetic beads from 24.4 to 45.9. Using blocking reagents to treat the immunobeads prior to combining with immunoliposomes reduced the signal by 33% to 33.02. The speculation was made that some non-specific (background) signals were due to the interaction of the anti-antibodies and not just biotinylated or streptavidinylated ends. 37 The background signal from the non-specific binding of red blood cells was decreased by lysing the whole blood sample before testing. The limit of detection of the microfluidic biosensor was determined to be at or below a whole blood fraction of 0.1, which can be correlated to 80 – 220 T-lymphocytes per L of blood sample. Variability of the results could have resulted from the instability of the blood sample. Blood samples are normally stable up to 48 hours after collected. For preliminary experimental purposes, the blood samples could not be obtained as frequently and the experiments were run on blood older than 48 hours. Further optimization of the proposed design is required including modification of sample injection method to decrease the amount of sample lost to the surface where the sample mixture is placed before withdrawn into the tubing and injected into the device, of streptavidin concentration on liposomes to decrease non-specific binding, and of working buffer used in blood and bead dilution. Fresh blood sample should be used to check the accuracy of the values and exact count of T-lymphocytes should be obtained to determine the exact limit of detection. However, the data shown here prove the principles of the micro-biosensor for T-lymphocyte detection. Success of this immunophenotyping biosensor will provide portable and cheap device with minimum human handling that can be used for Tlymphocyte enumeration. Microfluidic biosensor has great potential for testing in resource-limited settings. 38 REFERENCES 1. IUPAC – Physical Chemistry and Analytical Chemistry Division (1996) 2. Rogers, K., Gerlach, C. (1996) Environmental Biosensors: A Status Report. Environmental Science & Technology. 3. Higson, SP., Vadgama, P. (1994) Biosensors: a viable monitoring technology. Medical & Biological Engineering & Computing. Vol32(6), pp.601-609. 4. Kost, G., Hague, C. (1995) The current and future status of critical care testing and patient monitoring. American Journal of Clinical Pathology. Vol104(4 supp11), pp.2-17. 5. Turner, AP. (1994) Biosensors. Current Opinion in Biotechnology. Vol. 5(1), pp.49-53. 6. Immunology Link: http://www.immunologylink.com/CDantigen.htm. Accessed on April 20, 2005. 7. 2004 Report on the Global AIDS Epidemic : 4th Global Report (2004) Joint United Nations Programme on HIV/AIDS. p. 13. http://www.unaids.org/en/default.asp. Accessed on September 12, 2004. 8. McCloskey, T. (2001) Flow Cytometry for Evaluation and Investigation of Human Immunodeficiency Virus Infection. In: Methods in Cell Biology. New York: Academic Press. p.573. 9. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. (2004) Department of Health and Human Services Panel on Clinical Practices for Treatment of HIV Infection. pp. 1-97. http://AIDSinfo.nih.gov. Accessed on September 15, 2004. 10. Brando, B., D. Barnett, G. Janossy, F. Mandy, B. Autran, G. Rothe, B. Scarpati, G. D’Avanzo, J. D’Hautcourt, R. Lenkei, G. Schmitz, A. Kunkl, R. Chianese, S. Papa, J. Gratama. (2000) Cytofluorometric Methods for Assessing Absolute Numbers of Cell Subsets in Blood. Cytometry (Communications in Clinical Cytometry). Vol. 42, pp.327–346. 11. Janossy, G., I. Jani, B. Brandob. (2003) New Trends in Affordable CD4 T-cell Enumeration by Flow Cytometry in HIV/AIDS. Clinical and Applied Immunology Reviews. Vol. 4, pp. 91–107. 39 12. CDC. (1997) Revised guidelines for Performing CD4+ T-cell determinations in persons with human immunodeficiency virus (HIV) infection. MMWR. Vol.46(2), pp.1-29. 13. Shahghasempour, S., Gerami, M., Entezami, Z. (2001) Enumeration of Peripheral Blood Lymphocyte Subsets in a Healthy Iranian Population. Archives of Iranian Medicine Vol. 4(2), pp.80-83. http://www.ams.ac.ir/AIM/0142/shahghasem0142.html 14. Sutherland D. (1996) The ISHAGE guidelines for CD34+ cell determination by flow cytometry. J Hematotherapy. Vol.5(3), pp.213-226. 15. Kaleem, Z., Crawford, E., Pathan, M., Jasper, L. (2003) Flow cytometric analysis of acute leukemias: Diagnostic utility and critical analysis of data. Archives of Pathology & Laboratory Medicine. 16. Givan, A. (2001) The Past as Prologue. In: Flow Cytometry: First Principles Second Edition. Wiley-Liss, Inc. http://www3.interscience.wiley.com/cgibin/booktoc?ID=89011951&CRETRY=1&SRETRY=0. 17. Ormerod, M.G. (2000) Flow Cytometry, Third Edition. Oxford, Great Britain: Oxford University Press 18. Givan, A. (2004) Flow Cytometry: An Introduction. In: Flow Cytometry Protocols, Second Edition. Totowa, N.J.: Humana Press. 19. Boeck, G. (2001) Current Status of Flow Cytometry in Cell and Molecular Biology. International Review of Cytology. Vol. 204, pp. 239-298. 20. McSharry, J. (1999) Antiviral Drug Susceptibility Assays: Going With the Flow. Antiviral Research, Vol. 43(1), pp. 1-21. 21. CD4 Cell Monitoring for HIV/AIDS: Old Options, New Insights. (2001) Journal of the South African Dental Association. Vol. 56(12), pp. 602-605. 22. O’Gorman, M., J. Nicholson. (2000) Adoption of Single-Platform Technologies for Enumeration of Absolute T-Lymphocyte Subsets in Peripheral Blood. Clinical and Diagnostic Laboratory Immunology. Vol. 7(3), pp. 333–335. 23. Janossy, G., I. Jani, N. Bradley, A. Bikoue, T. Pitfield, D. Glencross. (2002) Affordable CD4 T Cell Counting by Flow Cytometry: CD45 Gating for Volumetric Analysis. Clinical and Diagnostic Laboratory Immunology. Vol. 9(5), pp. 1085–1094. 40 24. NAM/AIDSmap. (2004) Monitoring the immune system. Accessed July 2004. http://www.aidsmap.com/en/docs/A1527BEC-D49E-456D-B4026EDEA4A1B7F0.asp 25. Crowe S, Turnbull S, Oelrichs R, Dunne A. (2003) Monitoring of Human Immunodeficiency Virus Infection in Resource-Constrained Countries. Clinical Infectious Disease. Vol. 37 pp.25-35. 26. Baeumner, A.J., Cohen, R.N., Miksic, V., Min, J. (2003) RNA Biosensor for the Rapid Detection of Viable Escherichia coli in Drinking Water. Biosensors and Bioelectronics. Vol.18, pp. 405-413. 27. Esch, M.B., Baeumner, A.J., Durst, R.A. (2001) Detection of Cryptosporidium parvum Using Oligonucleotide-Tagged Liposomes in a Competitive Assay Format. Analytical Chemistry. Vol. 73, pp.3162-3167. 28. Baeumner, A.J., Schlesinger, N.A., Slutzki, N.S., Romano, J., Lee, E.M., Montagna, R.A. (2002) Biosensor for Dengue Virus Detection: Sensitive, Rapid, and Serotype Specific. Analytical Chemistry. Vol. 74(6), pp.1442-1448. 29. Kamholz A.E. (2004) Proliferation of microfluidics in literature and intellectual property. Lab on a Chip. Vol. 4(2), 16N. 41