Urinary Catheter Care
advertisement

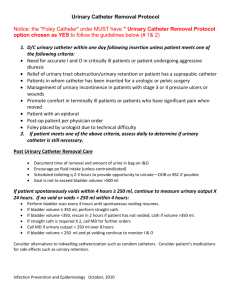
LIBERTY REGIONAL MEDICAL CENTER I. TITLE: URINARY CATHETER CARE Original Date: 04/01/1995 Effective Date: 05/10/2012 Next Review Date: 05/10/2014 DEFINITION OF POLICY: It is the policy of Liberty Regional Medical Center (LRMC) to adhere to guidelines as recommended by the Centers for Disease Control and Association for Professionals in Infection Control and Epidemiology to prevent or minimize urinary tract infections. II. PURPOSE OF POLICY: A. To provide evidence-based practice guidance for the prevention of catheter-associated urinary tract infection (CAUTI) in acute and long-term care settings. B. To maintain urinary drainage from the bladder as a continuous, unobstructed, and unidirectional flow. III. DEPARTMENTS TO WHICH THIS POLICY APPLIES: All departments within the organization and the Medical Staff via Infection Prevention Policy Manual IV. DEFINITION: Indwelling urinary catheter – A drainage tube that is inserted into the urinary bladder through the urethra, is left in place, and is connected to a closed collection system. It is also called a Foley catheter. V. PROCEDURE(S): A. Physician order is required to insert indwelling urinary catheter. B. Patient/resident and/or family will be educated on the purpose of urinary catheter and prevention of catheter-associated urinary tract infection (Attachment 4). C. Only credentialed personnel will insert urinary catheters. D. Personnel who insert urinary catheters will be required to attend yearly educational recredentialing. E. Alternatives to indwelling catheters will be considered: 1. External condom catheters for male patients without urinary retention or bladder outlet obstruction. 2. Intermittent catheterization (preferred to indwelling urethral catheter in patient with bladder emptying dysfunction). F. Urinary catheters will be inserted using sterile technique. The smallest catheter allowable for adequate urinary drainage (or the size specified by the physician) will be inserted. G. If it breaks in the sterile technique, disconnection, or leakage occur, replace the catheter and collecting system using sterile technique and sterile equipment. H. Personnel will perform hand hygiene prior to insertion, prior to and after any manipulation of catheter sites or apparatus. 1 I. Indwelling urinary catheters will be managed as a closed sterile drainage system. The following will be observed: 1. Drainage bags will not touch the floor. 2. If drainage bag has a spigot, do not allow it to touch the clean graduate container. 3. The closed drainage system will not be interrupted unless the catheter must be irrigated. J. Free flow of urine will be maintained by adherence to the following: 1. Preventing the catheter or tubing from kinking. 2. Emptying the drainage bag prior to patient/resident transport, when bag is approximately ¾ full and/or every 6 hours. 3. Maintaining the drainage below the level of the patient’s/resident’s bladder (e.g. do not put the catheter drainage bag in the bed during transport). K. Urine specimen collection from indwelling urinary catheter: 1. Under no circumstances should a urine sample be taken from the drainage bag for culture analysis after the initial insertion with immediate sampling. 2. Fresh urine specimens will be aspirated from the sampling port using aseptic technique. 3. If a CAUTI is suspected, remove the old catheter before obtaining the specimen. If indications for urinary catheterization still exist, obtain the urine specimen after replacing the old urinary catheter. L. Indwelling catheters will be properly secured after insertion to prevent movement and urethral traction. M. Long term indwelling catheters will not be changed on a routine/scheduled basis but only as needed (e.g. suspicion of urinary tract infection), unless otherwise ordered by the physician. N. Routine catheter care will be performed twice daily (morning and night), after each bowel movement, and as needed for soiling using soap and water (See Procedure for Foley Catheter Routine Care Attachment 3). This will be documented in the Nursing Progress Notes. O. Catheters will be irrigated by physician’s order only. Continuous irrigation solutions and tubing will be changed every 24 hours. Equipment for manual irrigation will be discarded after single use. P. Nursing will document the following information in the patient’s record: Indications for catheter insertion Date and time of catheter insertion Individual who inserted indwelling urinary catheter Daily assessment of need to continue indwelling urinary catheter Number of foley days(e.g. foley day 3) Date and time of catheter removal Q. Acute Care (Hospital care) 1. Indwelling Urinary Catheter Daily Assessment will be placed on the chart for physician review by night shift nursing personnel during chart checks (Attachment 1), unless for the following: a. The physician has already ordered a urinary catheter discontinuance on a designated date and time (e.g. remove Foley on post-op day 1 in the a.m.) b. The patient is determined to have a chronic indwelling urinary catheter that cannot be removed. 2. Indwelling Urinary Catheters will be removed if within 24 hours unless: a. The physician continues the order (Attachment 1). b. The physician has already ordered urinary catheter discontinuance on a designated date and time (e.g. remove Foley on post-op day 1in the a.m.). c. The patient is determined to have a chronic indwelling urinary catheter that cannot be removed. 2 d. Med-Surg Department: The Daily Monitoring Urinary Catheter Surveillance Form will be completed by unit’s charge nurse/designee and forwarded to Infection Prevention each day (Attachment 2). R. Long Term Care (Nursing Home care) Nursing will notify Long Term Care Infection Prevention Nurse of all urinary catheters. Long Term Care Infection Prevention Nurse will notify Director of Infection Prevention VI. REFERENCE(S): Gould, C, Umscheid, C., Agarwa, R., Kuntz, G., Pegues, D. and the Healthcare Infection Control Practices Advisory Committee (HICPAC). Guidelines for prevention of catheter-associated urinary tract infections 2009. Umscheid, C., Gould C., Pegues, D.A. (2008). Guidelines for preventing catheter associated urinary tract infections. Centers for Disease Control and Prevention. An APIC Guide (2008). Guide to the elimination of catheter-associated urinary tract infections (CAUTIs). Yokoe, D.S. , Mermel, L.A., Anderson, D.J., et. Al (2008). A compendium of strategies to prevent healthcare-associated infections in acute care hospitals. Infection Control and Hospital Epidemiology, 29(1):S12-S21. INI. Getting Started Kit: Prevent catheter-associated urinary tract infections. How-to-Guide. Originating Department/Committee/Team: Infection Control Committee Approval History: April 10, 2012 April 5, 2012 March 4, 2010 February 23, 2010 April 30, 2009 April 14, 2009 April 14, 2009 February 19, 2009 February 11, 2009 June 26, 2008 June 24, 2008 May 3, 2007 April 24, 2007 February 24, 2005 February 8, 2005 April 26, 2001 December 12, 2000 NCR PIC Medical Staff Policy Committee Infection Prevention and Control Committee Policy Committee Infection Prevention and Control Committee NCR PIC Policy Committee Infection Control Committee Policy Committee Infection Control Committee Policy Committee Infection Control Committee Policy Committee Infection Control Committee Policy Committee Infection Control Committee 3 Liberty Regional Medical Center Daily Urinary Catheter Assessment Date & Time Indwelling Urinary Catheter Daily Assessment Discontinue indwelling urinary catheter now Continue indwelling urinary catheter for the following reason(s): Surgical procedure with prolonged postop duration (e.g. structural repair of urethra or contiguous structures, prolonged effect of epidural anesthesia, etc…) Required immobilization due to surgery or trauma (e.g., potentially unstable thoracic or lumbar spine, multiple traumatic injuries such as pelvic fractures) Strict Intake & Output in critically ill patient (patient cannot use urinal or bedpan) Urinary obstruction (prostatic hypertrophy, clots with obstruction, etc.) Acute urinary retention and the patient cannot be intermittently catheterized Assistance in sacral or perineal wound healing with incontinent patient Patient/Resident comfort for end of life. Patient/Resident with chronic indwelling urinary catheter Physician Signature: Attachment 1 “Urinary Catheter Care” 05/10/2012 PATIENT IDENTIFICATION 4 Daily Monitoring Urinary Catheter Surveillance Form Fax to Infection Prevention Daily 408-9500 Date Shift Patient Label Patient Label Patient Label Patient Label Foley Days Indications- Circle indication or contact physician to remove Foley 1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7 Required immobilization due to surgery or trauma Strict Intake & Output in critically ill patient (pt can’t use bedpan/urinal/condom cath) Urinary obstruction Urinary retention and pat cannot be intermittently catheterized Assistance in sacral, perineal wound healing with incontinence Patient comfort for end of life Pt with chronic indwelling urinary catheter Required immobilization due to surgery or trauma Strict Intake & Output in critically ill patient (pt can’t use bedpan/urinal/condom cath) Urinary obstruction Urinary retention and pat cannot be intermittently catheterized Assistance in sacral, perineal wound healing with incontinence Patient comfort for end of life Pt with chronic indwelling urinary catheter Required immobilization due to surgery or trauma Strict Intake & Output in critically ill patient (pt can’t use bedpan/urinal/condom cath) Urinary obstruction Urinary retention and pat cannot be intermittently catheterized Assistance in sacral, perineal wound healing with incontinence Patient comfort for end of life Pt with chronic indwelling urinary catheter Required immobilization due to surgery or trauma Strict Intake & Output in critically ill patient (pt can’t use bedpan/urinal/condom cath) Urinary obstruction Urinary retention and pat cannot be intermittently catheterized Assistance in sacral, perineal wound healing with incontinence Patient comfort for end of life Pt with chronic indwelling urinary catheter Attachment 2 “Urinary Catheter Care” 05/10/2012 5 LIBERTY REGIONAL MEDICAL CENTER Procedure for Foley Catheter Routine Care The catheter-meatal junction is a significant portal of entry for bacteria into the urinary tract, potentially causing urinary tract infections. Therefore, it is most important that the perineum, catheter-meatal junction, and tubing be kept clean and free of fecal contamination. This area will be cleansed twice daily and as needed with soap and water or an acceptable perineal-cleansing product as follows: Provide patient/resident privacy. Explain to the patient/resident on what you are about to do. Call for assistance if you anticipate that the patient/resident may be uncooperative or if you need assistance positioning or turning the patient/resident. Wash hands or use alcohol hand sanitizer. Apply PPE, at minimum gloves. Obtain a basin of warm water. Wet washcloth with warm water. Apply soap or perineal cleansing product to cloth. Starting at the catheter-meatal junction, wash tubing, labia, and meatus, using friction and circular motion work outwards to the surrounding perineum. Always work from the area of least contamination to areas of more contamination and always from front to back. Repeat as needed. If gloves become grossly contaminated with feces, etc., gloves should be changed before continuing. Rinse area with clean warm water and pat dry. For uncircumcised males take special care to clean under the foreskin. After cleansing, keep the foreskin pulled down over the glans penis. Remove gloves and PPE and perform hand hygiene. Immediately document and/or report any reddened, abraded, swollen or broken skin areas to the patient’s/resident’s nurse. Reference: Centers for Disease Control and Prevention. Guideline for prevention of catheter-associated urinary tract infections. February 1, 1981. Attachment 3 “Urinary Catheter Care” 05/10/2012 6