Neuro/Musculoskeletal Assessment
advertisement

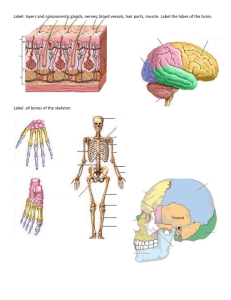
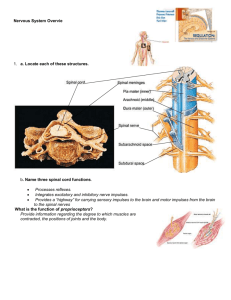
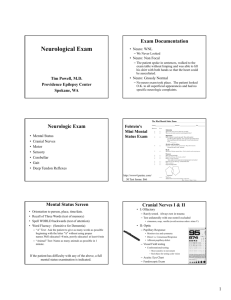
Neurological assessment 1 MENNONITE COLLEGE OF NURSING AT ILLINOIS STATE UNIVERSITY Diagnostic Reasoning for Advanced Practice Nursing 431 Neurological Assessment Quick A & P Review Central nervous system: the brain and spinal cord The Brain o 4 regions: cerebrum, diencephalon, brainstem, cerebellum o Contains interconnecting neurons (cell bodies and axons) o Gray matter: aggregations of neuronal cell bodies o White matter: neuronal axons coated with myelin The spinal cord o Extends from brainstem (medulla) to L1-L2 vertebrae o Contains motor and sensory pathways that exit and enter the cord via anterior and posterior nerve roots and spinal and peripheral nerves o 5 segments: cervical (C1-8), thoracic (T1-12), lumbar (L1-5), sacral (S1-5), coccygeal o Note: Cauda equina at L1-2, where nerve roots fan out like a horse’s tail Peripheral nervous system Cranial nerves o 12 pairs of cranial nerves plus spinal and peripheral nerves o Govern motor, sensory, and specialized functions like smell, vision, and hearing Peripheral nerves o 31 pairs of nerves that attach to the spinal cord: 8 cervical, 2 thoracic, 5 lumbar, 5 sacral, 1 coccygeal o Each nerve has an anterior (ventral) root containing motor fibers and a posterior (dorsal) root containing sensory fibers; the anterior and posterior roots merge to form a short (<5 mm) spinal nerve o Spinal nerve fibers commingle with similar fibers from other levels to form peripheral nerves o Motor and sensory pathways: descending motor and ascending sensory pathways o Dermatome: band of skin innervated by the sensory root of a single spinal nerve Common neurological complaints or symptoms Headache (see Dains chapter 18) Dizziness or vertigo (see Dains chapter 12) Generalized, proximal, or distal weakness Numbness Abnormal or loss of sensations Loss of consciousness, syncope, or near-syncope Seizures (see Bickley, pages 718-719 for types) What history indicates an increased risk? Tremors or involuntary movements Weakness Memory problems Neurological assessment 2 Health Promotion and Counseling Preventing stroke or TIA Reducing risk of peripheral neuropathy Detecting the “three Ds” – delirium, dementia, and depression In children, discuss achieved & anticipated developmental milestones The Nervous System: Key Principles Objectives o Is there a problem involving the nervous system? o Localize the problem within the nervous system o Determine the etiology o Determine appropriate diagnosis and treatment As you examine the patient, remember three important questions: o Is mental status intact? o Are right- and left-sided findings the same, or symmetric? o If findings are asymmetric or otherwise abnormal, do the causative lesions lie in the central nervous system or the peripheral nervous system? Organize your thinking into 5 categories: o mental status, speech, and language o cranial nerves o motor system o reflexes o sensory system Subjective Data: History is the most important factor in neuro assessment!!! Chief complaint HPI o Details about the symptoms o o o o o How would you describe the location of a headache when the patient points . . ? Acute or chronic in nature? Precipitating factors? Improving or worsening? Associated symptoms? Any recent travel to foreign countries? Past Medical History o Previous similar symptoms o Other medical illnesses o Previous surgeries o Pregnancy or birth illness or injury o Allergies o Current medications – when last taken (for example Parkinson’s disease, tremors, seizures, dizziness, neuropathy, etc.) Family history o Huntington’s chorea, tics, etc. Neurological assessment 3 Social history o Employment – chemical exposures o drug or alcohol intake o home life – hobbies? ROS Ask about/document handedness---Why? What are you including in the Nervous system? Objective Data; Physical Examination General Approach o Detail of exam depends on the data collected o Neuro exam can be integrated with other systems such as MSK, Behavior/Mental status. o What have you already done re: neuro? o Inspection, palpation, percussion (no auscultation) o Use head to toe approach, side-to-side (symmetry important!) Neuro exam: 5 parts 1. Mental status (and speech) 2. 3. 4. 5. Cranial nerves Motor function Reflexes Sensory function 1. Mental Status (Bickley, pages 145-157) Appearance and behavior o Level of consciousness – alert, lethargic, obtunded, stuporous, coma o Posture and motor behavior – walking, sitting, lying, comfortable, agitated, movements o Dress, grooming, hygiene o Facial expression – flat, asymmetrical o Manner, affect, relationship to people and things Speech & language o Quality, rate, volume o Articulation & Fluency Language – receptive and expressive components Dysarthrias (muscular control defect-Parkinson’s) Dysphonias (aphasias) such as Wernicke’s (fluent receptive) & Broca’s (nonfluent expressive) Aphasia testing How is this done? Mood – depressed, suicide Thoughts & perceptions – logical, relevant, organized, and coherent thoughts expressed during interview? Cognitive function o Orientation – person, place, time o Attention (Spell WORLD backwards) o Memory Short-term (minutes to days; recall of 3 words at 3 minutes) Neurological assessment 4 Long-term (months to years) Higher cognitive function o o o o Information & Vocabulary (name last 4 presidents) Calculation (simple math) Abstract thinking (explain proverb) Constructional (draw face of a clock with current time) RED FLAGS regarding mental status o Inaccurate or vague details about history o Jocularity o Change in observed grooming habits o Signs of change from previous behavior o MMSE – tool to screen for cognitive impairment not diagnose delirium or dementia 2. Cranial Nerves Sensory deficits are present when afferent fibers (A) are involved. Motor deficits are present when efferent fibers (E) are involved. o I Olfactory (A) o II Optic (A) o III Oculomotor (E) o IV Trochlear (E) o V Trigeminal (A, E) o VI Abducens (E) o VII Facial (A, E) o VIII Vestibulocochlear (Acoustic) (A) o IX Glossopharyngeal (A, E) o X Vagus (A, E) o XI Spinal Accessory (E) o XII Hypoglossal (E) Examination techniques o o o o o o o o o CNI-Olfactory; smell in each nostril separately CN II-Optic; visual acuity chart, visual field confrontation, fundoscopic CN III-Oculomotor, IV-Trochlear, VI-Abducens; PERRLA, accommodation, EOMs, convergence CN V-Trigeminal; clinch jaw, palpate temporal/masseter muscles; light touch/sharp/dull CN VI-Facial; asymmetry at rest, eyebrow raise, frown, tight closure of eyes, smile, puff cheeks CN VIII; Acoustic; bilateral Whisper test CN IX-Glossopharyngeal, CN X-Vagus; speech quality, say “Ah” CN XII-Hypoglossal; stick tongue out and move side-to-side CN XI-Spinal Accessory; shrug shoulders/turn head against resistance 3. Motor Function (trunk and limbs) Body position – shoulder height, neck position, etc. Involuntary movements – tremors, tics, fasciculations Muscle bulk – contour, symmetry, atrophy Muscle tone – hypotonia, spasticity, cogwheel rigidity o Note tone & resistance during joint ROMs Muscle Strength: How do you describe these? Neurological assessment 5 o Muscle group testing discussed in MSK o Grading 5/5 Normal Strength 4/5 Full ROM against gravity, with some effort at resistance 3/5 ROM against gravity 2/5 ROM without gravity 1/5 Trace joint or muscle contraction 0/5 No movement Coordination o Station and Gait Walk across room and back (also not arm swing) Walk heel to toe (tandem walking) If has difficulty: Romberg, hop in place, shallow knee bend, walk on toes (plantar flexion”, walk on heels, dorsiflexion) o Cerebellar Function Arms Rapid rhythmic alternating movement Point to point Legs Rapid rhythmic alternating movement Point to point 4. Reflexes Technique o Relaxed client o Limb supported o Muscle mildly stretched o Strike tendon briskly o If reflexes are symmetrically diminished or absent, use isometrics-how is this done? Grading of Reflexes o 0 Absent, no muscle contraction o 1+ Hyporeflexia o 2+ Normal o 3+ Hyperreflexia o 4+ Abnormal - strong contractions, with clonus Check these reflexes: o Biceps o Triceps o Brachioradialis o Patellar (knee) o Achilles (ankle) o Plantar response (formerly Babinski) What nerve roots do these test? 5. Sensory (dermatomes, fingers and toes) Pain & temperature (spinothalamic tract) – pinprick, tuning fork Position & vibration (posterior column) – hold side of digit, tuning fork on bone Light touch (both pathways) – cotton swab Neurological assessment 6 Discrimination o Stereognosis: object identification o Graphesthesia: number identification o Two point discrimination o Point localization o Extinction Special Maneuvers: Meningeal signs o Brudzinski’s sign (flex neck, hips/knees flex) o Kernig’s sign (flex legs at hip and knee, resistance to straightening knees bilaterally) Lumbosacral radiculopathy - straight-leg raise Examples of Nervous System notes Normal screening neurological note Mental status: alert, oriented x 3, appropriate responses in conversation. Cranial nerves: PERRLA. EOMI. Visual acuity 20/20. Whispered voice test passed. Facial strength intact. Motor: Bilateral strength 5/5 with shoulder abduction, elbow extension, wrist extension, finger abduction, hip flexion, knee flexion, ankle dorsiflexion. Casual and tandem gaits intact. Fine finger movement and finger-nose-finger intact. Sensation: Sharp/dull intact in bilateral fingers and toes. Reflexes: 2 at biceps, knees and ankles. Plantar responses flexor. Focused normal neurological examination of lower extremities note Motor: Bilateral muscle bulk and tone intact including extensor digitorum brevis, no fasciculations. Bilateral strength 5/5 in hip flexors, knee extensors and flexors, knee abductors, ankle flexors and extensors. Heel-to-shin intact. Casual, heel, toe, and tandem gaits intact. Romberg sign negative. Reflexes: 2 at knees and ankles. No clonus. Plantar responses flexor. Sensation: Bilaterally pinprick, vibratory, temperature and position sensations intact. Normal detailed neurological examination note Mental status: Alert, oriented x 3, logical and relevant responses in conversation. Recent and remote memory, intellectual ability, fund of knowledge and judgment intact on screening. Cranial nerves: Visual acuity 20/20. PERRLA. Disk margins sharp. Visual fields full. EOMI. Facial strength intact, symmetry at rest. Temporal and masseter strength intact. Whispered voice test passed. Uvula rose in the midline, gag intact. Shoulder shrug symmetric, strength 5/5. Tongue protruded midline, symmetrical movement. Motor: Good muscle bulk and tone bilaterally. Fine finger movements and finger-nose-finger intact. Strength 5/5 throughout, no pronator drift. No tremors. Casual, heel, toe, and tandem gaits intact. Romberg sign negative. Sensation: Light touch, sharp/dull, and vibratory intact bilaterally. Reflexes: 2 at biceps, triceps, brachioradialis, knees, and ankles. Plantar responses flexor.