Type 2 DM protocol
advertisement

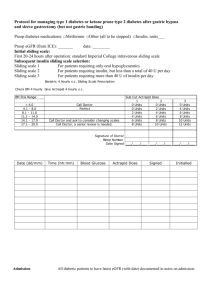
Protocol for managing type 2 diabetes after gastric bypass and sleeve gastrectomy (but not gastric banding) version 7.7.2010 Preop diabetes medications: □Metformin □Other (all to be stopped) □Insulin, units___ Preop eGFR (from ICE): _______ date: ________ Initial sliding scale selection: Sliding scale 1 For patients requiring only oral hypoglycaemics Sliding scale 2 For patients requiring insulin, but less than a total of 40 U per day Sliding scale 3 For patients requiring more than 40 U of insulin per day Bariatric 4 Hourly s.c. Sliding Scale Prescription Check BM 4 hourly. Give Actrapid 4 hourly s.c. BM Stix Range < 4.0 4.1 - 8.0 8.1 - 11.0 11.1 - 14.0 14.1 - 17.0 17.1 - 20.0 Call Doctor Perfect Call Doctor and ask to consider changing scales Call Doctor, a senior review is needed. Sub.Cut Actrapid Dose 1 2 0 Units 0 Units 0 Units 2 Units 2 Units 4 Units 4 Units 6 Units 6 Units 8 Units 8 Units 10 Units Signature of Doctor Bleep Number Date Signed ___/____/___ Date (dd/mm) Time (hh:mm) Blood Glucose Actrapid Dose ___/____/___ Signed 3 0 Units 4 Units 6 Units 8 Units 10 Units 12 Units ___/____/___ Initialled Admission All diabetic patients to have latest GFR (with date) documented in notes on admission Day of surgery/ Use Sliding Scale and make sure all oral hypoglycaemic drugs are stopped Postop. day 1 Postop. day 2 Prescribe Metformin at the same dose as on admission (which in most cases should be 1g twice daily unless poor tolerability) starting the evening 2 days after surgery, unless the latest eGFR is <60mL/min. For these patients, contact obesity physician Check if patient needs urgent referral to bariatric specialist nurse to learn to inject insulin □Referral not needed □Referral needed Referral criteria: patient both a) on postop. day 1 at 09:00 required more than 10 Units Insulin in the previous 24 h and b) does not know how to inject insulin Discharge 1. No patient to be discharged if last BM >10 mmol/L 2. If insulin use on sliding scale >10 U in last 24 h, contact senior clinician 3. All diabetic patients to text “Blood glucose mobile phone” (07970719453) with fasting glucose value for 10 days immediately after surgery. If patient does not text before 12:00, the team will contact them Metformin dosage selection: 1. All patients will be restarted on their usual metformin dose (usually metformin 1g twice daily) starting 2 days following surgery, provided that eGFR>60mL/min. Metformin will be started on the second postoperative evening (eg if operation on Tuesday then start metformin on Thursday evening). Patients who can’t tolerate metformin should be reviewed by obesity physicians/fellow/nurse specialist. 2. Metformin doses if eGFR <60 ml/min: a. eGFR 45-60 ml/min: All patients will be prescribed metformin 850mg twice daily starting 2 days after surgery. Metformin will be started on the second postoperative evening (eg if operation on Tuesday then start metformin on Thursday evening). b. eGFR 30-45 ml/min: All patients will be prescribed metformin 500mg twice daily starting 4 days after surgery. Metformin will be started on the fourth postoperative evening (eg if operation on Tuesday then start metformin on Saturday evening). c. eGFR < 30ml/min: no metformin to be given. 3. If patients can’t tolerate metformin the preferred option is to treat with Lantus s.c at night. After discharge: Daily insulin requirement will be adjusted by 2 to 4 units to achieve a fasting blood glucose of 5.6-7mmol/l. 1. At Day 10 post op clinic review a. Metformin dose at discharge will be continued. b. If FPG is >7mmol/l, pioglitazone 15mg daily will be added. Book patient into diabetes surgery clinic (DS5) to increased Pioglitazone as required to 45 mg daily, aiming to reduce the FPG to <7mmol/l and the HbA1c to <6.0%. Metformin therapy will continue. c. If FPG is >9mmol/l, insulin therapy will be instituted and book into diabetes surgery clinic (DS5) asap 2. At 3 months, all diabetic patients will be reviewed and hypoglycaemic medication adjusted in diabetes surgery clinic (DS5) 3. At 6 months, all diabetic patients will be reviewed by phone and those with HbA1c >6.5% will be brought back to the diabetes surgery clinic (DS5) for review of hypoglycaemic medication. Definitions for remission of hyperglycaemia: 1. Partial remission of hyperglycaemia is HbA1C <6.5% and fasting glucose 5.6-6.9 mmol/l of at least 1 year's duration in the absence of active pharmacologic therapy or ongoing procedures. 2. Complete remission of hyperglycameia is a HbA1C <6.0% and fasting glucose <5.6 mmol/l of at least 1 year's duration in the absence of active pharmacologic therapy or ongoing procedures.